
Diabetes

Glucose
Required as fuel for cellular metabolism Brain’s need for glucose parallels its
demand for oxygen
Insulin
Hormone Produced by Islets of Langerhans in
pancreas Required for sugar to enter most cells Brain does not require insulin to use
sugar

Pancreas
Located in retroperitoneal space
Produces, releases– Digestive enzymes
into duodenum– Insulin, glucagon into
blood
Islets of Langerhans
Alpha cells– Glucagon– Raises blood sugar
Beta cells– Insulin– Lowers blood sugar

Diabetes Mellitus
Metabolic disease
Characterized by inadequate, absent insulin production

Type I Diabetes
No insulin production Takes insulin injections

Type II Diabetes
Inadequate insulin production Increased tissue resistance to insulin effects Controlled with
– Diet– Oral medications:
• Diabeta, Diabinese, Dymelor, Glucotrol, Micronase, Orinase, Tolinase, Glucophage
– Insulin injections as disease progresses

Problems in Diabetes

Blood Sugar Imbalance
Hyperglycemia– Diabetic ketoacidosis (DKA)– Hyperosmolar coma
Hypoglycemia

Hyperglycemia
Causes– Failure to take insulin– Overeating, eating wrong diet– Stress (fever, infection, emotional stress)
New-onset diabetics usually present with an episode of hyperglycemia

Diabetic Ketoacidosis
Usually Type I diabetic (no insulin) Blood sugar rises Kidneys try to remove excess sugar Urine production increases (polyuria) Patient becomes volume depleted
– Thirst (polydypsia)– Tachycardia– Hypotension– Dry skin, mucous membranes

Diabetic Ketoacidosis
Cells cannot burn sugar; patient experiences hunger (polyphagia)
Cells burn fat as alternative fuel Acidic ketone bodies produced Patient tries to correct acidosis; exhales CO2
Rapid, deep breathing (Kussmaul respirations) Exhaled ketone bodies produce nail-polish
remover or “fruity” breath odor

Diabetic Ketoacidosis
Volume depletion Ketone body production (ketoacidosis)

Hyperosmolar Coma
Usually Type II diabetic (inadequate insulin) Blood sugar rises Kidneys try to remove excess sugar Urine production increases (polyuria) Patient becomes volume depleted
– Thirst (polydypsia)– Tachycardia– Hypotension– Dry skin, mucous membranes

Hyperosmolar Coma
Cells continue to burn sugar Acidic ketone bodies not produced Nail-polish remover or “fruity” breath odor not
present

Hyperosmolar Coma
Severe volume depletion NO ketone body production

Hyperglycemia
Management– Support ABC’s – Treat for hypovolemic shock– Transport– When in doubt, give sugar!

Hypoglycemia
Causes– Insulin overdose– Normal insulin use without eating– Over-exercise
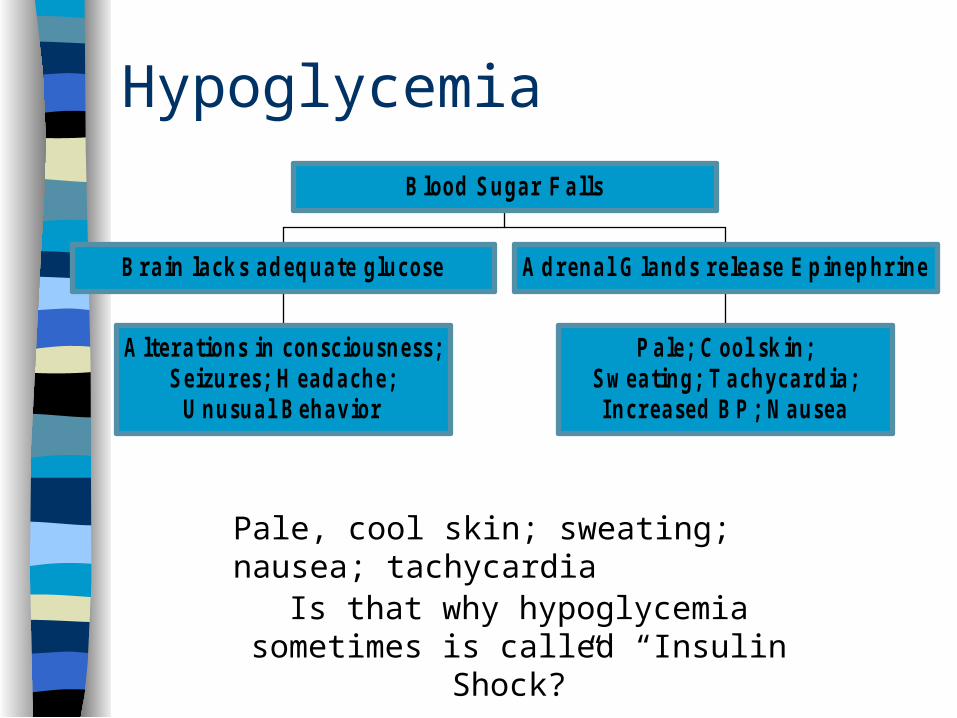
Hypoglycemia
A ltera tions in consc iousness ;S e izures; H ea d a che;
U nusua l B eha v ior
B ra in la ck s a d eq ua te g lucose
P a le ; C ool sk in;S w ea ting ; T achyca rd ia ;Increa sed B P ; N a usea
A d rena l G la nd s re lea se E p inep hr ine
B lood S ug ar F a lls
Pale, cool skin; sweating; nausea; tachycardia
Is that why hypoglycemia sometimes is called “Insulin Shock?”

Hypoglycemia
Insulin shock isn’t really shock Patient just looks “shocky” because of
epinephrine adrenals are releasing

Hypoglycemia
Can occur in non-diabetics Most common cause =
EtOH on empty stomach A patient is never, just drunk
Hypoglycemia Management
Conscious patient– Give sugar orally
Unconscious patient– Support ABC’s– Get ALS back-up for IV glucose
When in doubt, Give Sugar!
Ask All Diabetics
Have you eaten today? Have you taken your medication today? When in doubt, give Sugar!

Other Diabetes Complications
Atherosclerosis– Myocardial infarction– CVA– Peripheral vascular disease– Blindness– Renal failure

Other Diabetes Complications
Diabetic Neuropathy– Gangrene– Increased “silent” myocardial infarction risk

Silent MI
Acute MI in diabetic can present without chest pain
May resemble “flu” Manage “sick” diabetics as if critically ill
until proven otherwise







