ARTICLEPEDIATRICS Volume 138 , number 3 , September 2016 :e 20160907
Differences Between Transcutaneous and Serum Bilirubin Measurements in Black African NeonatesBolajoko O. Olusanya, FRCPCH, PhD, a Donald O. Imosemi, MBBS, FWACS, b Abieyuwa A. Emokpae, MBBS, FMCPaedc
abstractBACKGROUND AND OBJECTIVE: Transcutaneous bilirubin (TcB) correlates positively with total
serum bilirubin (TSB) across different racial populations. However, little is known
about the pattern of divergence between TcB and TSB at individual patient-level and the
relationship with TcB measuring techniques among African neonates. This study, therefore,
investigates TcB–TSB discrepancies and the contribution of 2 models of transcutaneous
bilirubinometers to the observed divergence in a black African population.
METHODS: Medical records were retrieved for late preterm and term infants with 1 to 3 pairs
of TcB and TSB measurements between December 2011 to June 2015 in Nigeria. Divergence
between TcB and TSB values for each infant was determined and the associated factors
explored with generalized estimating equations for logistic regression. Contributions
of BiliChek and JM-103 transcutaneous bilirubinometers to the divergence were further
explored through linear regression and Bland-Altman analysis.
RESULTS: Overall, 2107 TcB/TSB measurements from 1553 infants were analyzed. TSB was
overestimated by ≥2 mg/dL in 64.5%, ≥3 mg/dL in 42.7%, and ≥4 mg/dL in 25.7% of all
measurements. In contrast, TSB was underestimated by ≥2 mg/dL in 1.1%, ≥3 mg/dL in
0.5%, and ≥4 mg/dL in 0.3% of all recordings. Postnatal age, feeding mode, and type of TcB
instrument were predictive of TSB overestimation. The JM-103 was associated with greater
imprecision than BiliChek at all TSB levels.
CONCLUSIONS: BiliChek and JM-103 bilirubinometers significantly overestimate TSB in black
African neonates and may result in unnecessary or excessive treatments. Additional
development of appropriate bilirubin determination devices for this racial group, especially
in resource-limited settings, is warranted.
aCentre for Healthy Start Initiative, Ikoyi, Lagos, Nigeria; bLagos Island Maternity Hospital, Lagos, Nigeria; and cMassey Street Children’s Hospital, Lagos, Nigeria
Dr Olusanya conceived and designed the study, analyzed the data, drafted the manuscript,
and fi nalized the manuscript; Drs Imosemi and Emokpae participated in data collection and
the interpretation of the data and critically reviewed the revised manuscript; and all authors
approved the fi nal manuscript as submitted.
DOI: 10.1542/peds.2016-0907
Accepted for publication Jun 30, 2016
Address correspondence to Bolajoko O. Olusanya, FRCPCH, PhD, Centre for Healthy Start Initiative,
286A Corporation Dr, PO Box 75130 VI, Dolphin Estate, Ikoyi, Lagos, Nigeria. E-mail: bolajoko.
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2016 by the American Academy of Pediatrics
To cite: Olusanya BO, Imosemi DO, Emokpae AA. Differ-
ences Between Transcutaneous and Serum Bilirubin
Measure ments in Black African Neonates. Pediatrics.
2016;138(3):e20160907
WHAT’S KNOWN ON THIS SUBJECT: Transcutaneous
bilirubin (TcB) is highly correlated with total serum
bilirubin (TSB) across ethnic populations. TcB is a
useful screening tool or indication for treatment
in infants with severe hyperbilirubinemia where
facilities for TSB are limited or lacking.
WHAT THIS STUDY ADDS: Approximately 1 in 3 black
African neonates with hyperbilirubinemia may be
prone to TcB overestimation (≥3 mg/dL), resulting in
unnecessary treatments where confi rmatory TSB is
not readily available. Improved bilirubin measuring
devices are needed for this racial population,
especially in resource-limited settings.
by guest on May 4, 2019www.aappublications.org/newsDownloaded from

OLUSANYA et al
Studies among neonates of African-
American ancestry have so far shown
that the black race is unusually
associated with a decreased risk
of severe hyperbilirubinemia but
an increased risk of kernicterus, 1, 2
underpinned by glucose-6-phosphate
dehydrogenase (G6PD) deficiency. 3
As a high-risk population, routine,
predischarge bilirubin screening
is warranted in this racial group to
minimize the risk of kernicterus. 4
The excellent correlation between
transcutaneous bilirubin (TcB) and
total serum bilirubin (TSB) tests5, 6
has made TcB a valuable screening
tool for TSB in the management of
hyperbilirubinemia worldwide. 4, 7, 8
However, TcB tends to underestimate
TSB in whites or neonates with
light or medium skin color and
overestimate TSB in non-whites or
neonates with dark skin color.9 – 11
Such discrepancies may compromise
the effective management of infants
at risk for bilirubin encephalopathy. 12
Limited evidence exists on the
pattern and predictors of individual
TcB–TSB divergence, especially
in settings with predominantly
dark-skinned infants or limited
access to timely and reliable TSB
measurements. 13– 15 This study,
therefore, set out to determine
the prevalence and correlates of
significant TcB overestimation in a
black African population to facilitate
optimal decisions for appropriate
clinical intervention.
METHODS
This prospective, observational study
was conducted at Island Maternity
Hospital, a leading specialist
maternity hospital in Nigeria owned
by the Lagos State Government.
This 180-bed public hospital is a
referral center for over 300 private
and public hospitals in the Lagos
metropolis and its environs.
All healthy late preterm and term
neonates (gestational age ≥35 weeks
or birth weight ≥2.2 kg) delivered
between December 2011 and June
2015 with 1 to 3 pairs of TcB–TSB
measurements in the first 120
hours of life were enrolled. Only
measurements recorded before
receiving phototherapy were eligible
for analysis. All sick infants were
excluded. The study was conducted
under institutional ethical approval
from the Lagos State Health Service
Commission.
Infants of consenting mothers were
screened routinely for jaundice by
using the BiliChek transcutaneous
bilirubinometer (Philips Healthcare
North America, Monroeville, PA)
or the JM-103 transcutaneous
bilirubinometer (Draeger Medical,
Telford, PA). Measurements were
derived from the infant’s sternum
by specially trained nurse assistants.
The BiliChek was used from
December 2, 2011 to November 26,
2012 and the JM-103 was used from
November 27, 2012 to June 23, 2015.
Two units of each piece of equipment
were available to provide back-up
for maintenance. Both instruments
were used in accordance with the
manufacturers’ instructions for
quality control and calibration.
The algorithms and other technical
features of the 2 devices are well
described. 5, 6, 9 Infants whose bilirubin
levels at screening exceeded 3 mg/dL
below the recommended postnatal
age threshold for phototherapy
based on the American Academy of
Pediatrics (AAP) guidelines were
assessed for TSB within ∼1 hour.
This criterion was adopted because
of the high prevalence of G6PD
deficiency in this population. 16 TSB
measurements were performed on
capillary blood samples drawn by
heel puncture and analyzed by direct
spectrophotometry by using the
Advanced Bilirubin Stat-Analyzer
(model BR2; Advanced Instruments,
Inc, Norwood, MA).
The choice of putative predictor
variables was guided by relevant
literature, 9 – 15 and included infant’s
sex, birth weight, estimated
gestational age (in completed weeks,
based on maternal history of last
menstrual period correlated with
ultrasound scan by using Siemens
Sonoline SI-450 as documented
in the hospital records), postnatal
age at screening, maternal self-
report of ethnicity (based on the
3 most predominant tribes in
Nigeria: Hausa, Ibo, and Yoruba,
as well as others), skin color (light
brown, medium brown, or dark
brown), mode of feeding at the
time of TcB screening (formula
only, exclusive breastfeeding, or
mixed feeding), G6PD status, and
TcB model. Skin color was classified
as previously reported in this
population, 14 and recorded by the
trained nurse assistants as shown
in a color guide (Supplemental Fig
5). G6PD evaluation was based on
the fluorescent blood spot for all
infants by using methods described
by Beutler et al, 17 as previously
reported.18 Lack of fluorescence
after 10 minutes was indicative of
deficient levels.
Three levels of significant
overestimation or underestimation
were computed from the TcB–TSB
pairs: TcB–TSB ≥2 mg/dL, ≥3 mg/dL,
or ≥4 mg/dL. Because of the small
amount of TSB underestimation
by TcB, further analysis was not
considered necessary. Univariate
associations between the
predictor variables and bilirubin
overestimation (each defined as a
binary outcome) were then explored
with Pearson’s χ2. Strength of
association was estimated by odds
ratios (OR) and the corresponding
95% confidence intervals (CI) as
an approximation of the relative
risk. Statistical significance was set
at a critical level of P < .05. Factors
significantly associated with each
outcome in the univariate analysis
were entered into the respective
multivariable logistic regression
model. The generalized estimating
equation method was used for the
regression modeling to account for
2 by guest on May 4, 2019www.aappublications.org/newsDownloaded from

PEDIATRICS Volume 138 , number 3 , September 2016
repeated measurements on the same
infant. All models were adjusted
for TSB level. Plausible interaction
between TSB and each predictor
variable was also investigated.
The contributions of BiliChek and
JM-103 to TSB overestimation were
examined further with Pearson’s
correlation coefficients (r), scatter
plots, and linear regression analyses.
Because of the limitations of
Pearson’s coefficients in determining
the variability and linear correlation
between 2 continuous variables, we
explored the degree of agreement
(bias) between TcB and TSB for
each device using the Bland-Altman
method. 19 The mean bias was defined
as the mean difference between each
pair of TcB and TSB measurement
obtained from each enrolled infant.
TcB imprecision or variability
compared with TSB was defined as
2 SD from the mean difference. The
limits of agreement (LOA) of the
mean differences and their 95% CIs
were also determined. Additionally,
the discriminatory power of the
TcB devices in predicting infants
who required phototherapy was
determined by using receiver
operating curve analysis. 20 The
criteria for phototherapy were based
on the appropriate age-specific
thresholds in the AAP guidelines. 4
The interinstrument variability
in a sample of infants tested
simultaneously with BiliChek and
JM-103 was also computed. IBM SPSS
Statistics for Windows software,
version 21.0 (IBM Corporation,
Armonk, NY) was used for all
statistical analyses.
RESULTS
A total of 1553 infants with
2107 paired TcB–TSB measure-
ments were enrolled for the study.
The infants had a mean TcB of 10.04
(SD, 3.40) mg/dL and a mean TSB of
7.28 (SD, 2.66) mg/dL. TcB ranged
from 2.1 to 19.9 mg/dL, whereas TSB
ranged from 0.3 to 19.5 mg/dL.
The characteristics of the infants are
presented in Table 1. Some 54.9%
(853/1553) of the infants were
male, 5.7% (89/1551) weighed
<2.5 kg, and 9.8% (150/1533) had
a gestational age of <37 weeks. The
infants were predominantly of the
Yoruba tribe (71.2%), had light or
medium brown skin (91.6%), and
were exclusively breastfed (69.1%).
A total of 263 (16.9%) infants were
G6PD deficient.
TcB recordings in 79.1% of the
infants were with the JM-103. TSB
was overestimated by ≥2 mg/dL
in 64.5% (1358/2107), ≥3 mg/
dL in 42.7% (899/2107), and
≥4 mg/dL in 25.7% (542/2107)
of all measurements. TSB was
overestimated by ∼8 mg/dL 32 times
(19 neonates). In contrast, TSB was
underestimated by ≥2 mg/dL in
1.1% (23/2107), ≥3 mg/dL in 0.5%
(10/2107), and ≥4 mg/dL in 0.3%
(7/2107) of all measurements. Of
the 1774 (84.2%) overestimated TSB
values ≥1 mg/dL, phototherapy was
required in only 55 (3.1%) cases.
In the univariate logistic regression
analysis, 4 factors (postnatal age,
G6PD status, feeding mode, and
TcB equipment) were significantly
associated with the 3 levels of
overestimation. Ethnicity or
skin color was not significantly
associated with overestimation.
The independent predictors of
significant bilirubin overestimation
after multivariable logistic regression
are presented in Table 2. Increasing
postnatal age and use of the JM-103
were predictive of all levels of
overestimation, whereas exclusive
breastfeeding was only associated
with ≥2 mg/dL overestimation.
TSB level had a modifying effect
on feeding mode, which prompted
our adjusting all models with the
interaction term, feeding mode*TSB.
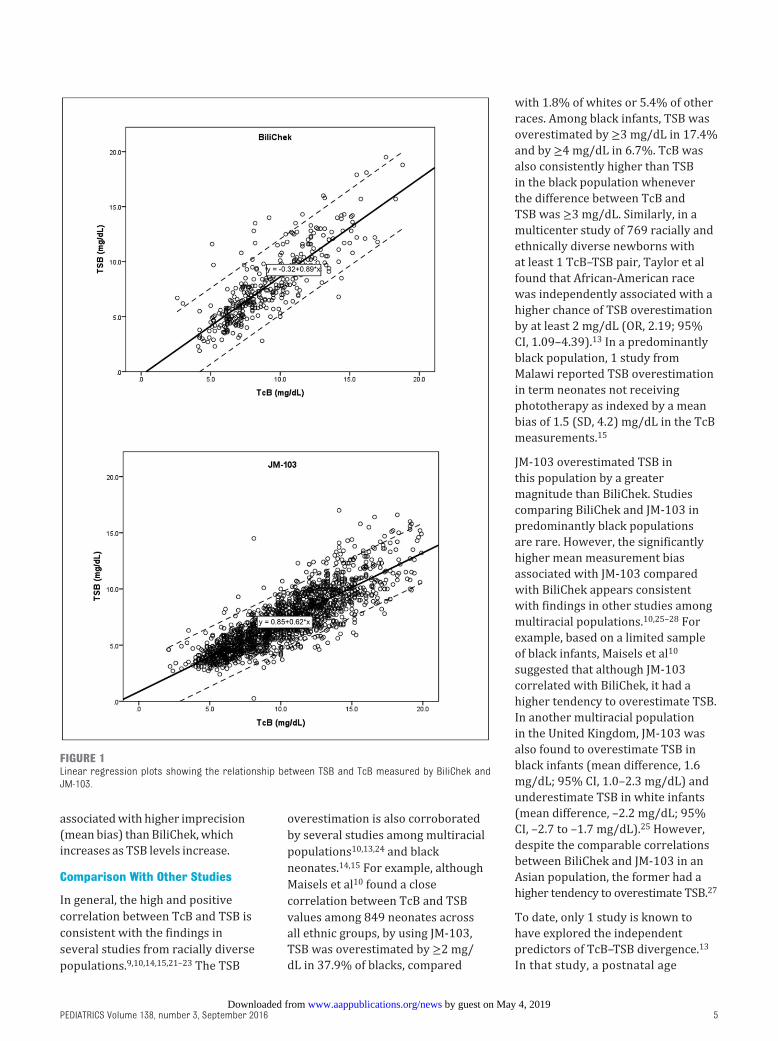
The correlation between TcB and TSB
was linear and significant for BiliChek
(Pearson’s r = 0.83, R2 = 0.69, P <
.001) or JM-103 (Pearson’s r = 0.85,
R2 = 0.72, P < .001) as presented in
Fig 1. The combined measurements
also showed significant correlation
(Pearson’s r = 0.81, R2 = 0.66,
P < .001). As shown in Fig 2, the
discriminatory power of JM-103
(area under the curve = 0.725; 95%
CI, 0.665–0.786) was slightly higher
than the value for BiliChek (area
under the curve = 0.706; 95% CI,
0.625–0.787) in predicting the need
for phototherapy. JM-103 had an
optimal combination of sensitivity
(64%) and specificity (72%) at a
cut-off of 12.1 mg/dL in detecting
infants who required phototherapy,
compared with BiliChek, which had
a sensitivity of 60% and a specificity
of 74% at a cut-off of 10.3 mg/dL.
JM-103 was associated with 100%
sensitivity for TcB values up to 4.8
mg/dL, compared with 1.6 mg/dL for
BiliChek.
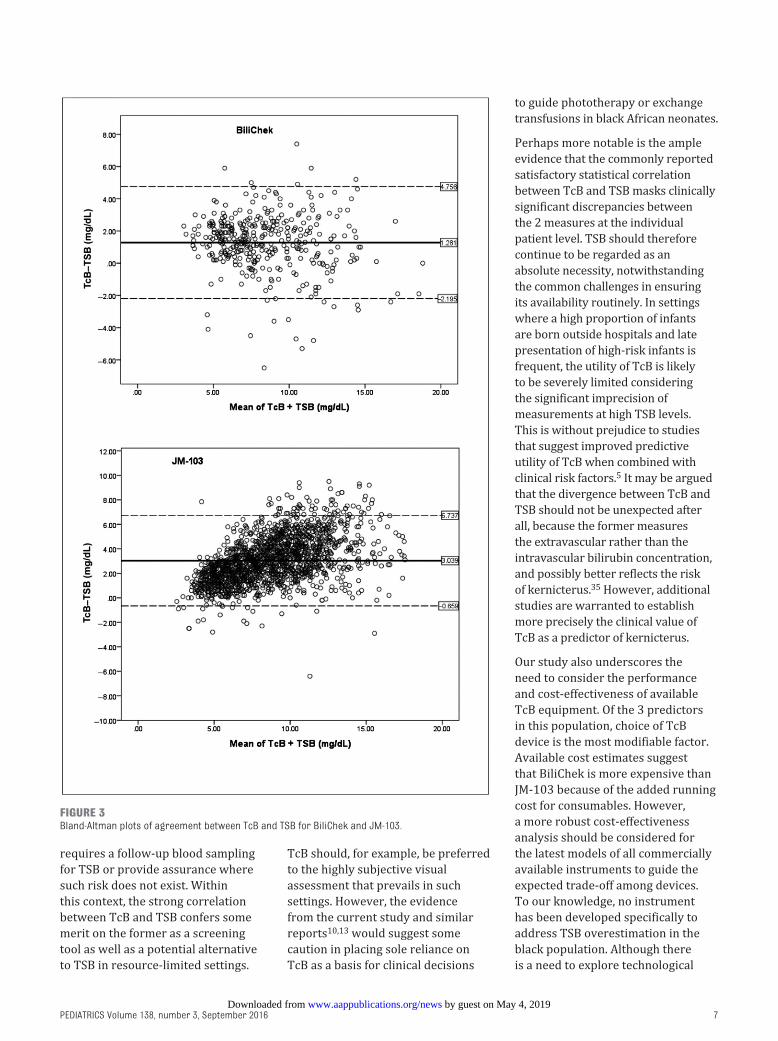
The Bland-Altman plots are
presented in Fig 3. The mean bias for
JM-103 was 3.04 (SD, 1.89) mg/dL
(95% LOA: –0.66 to 6.74 mg/dL)
compared with 1.28 (SD, 1.77) mg/dL
(95% LOA: –2.20 to 4.76 mg/dL) for
BiliChek. The pattern of mean bias
at various levels of TSB for all paired
measurements is presented in Fig 4.
The mean bias between JM-103 and
BiliChek widens as TSB increases,
with BiliChek underestimating TSB
from roughly 13.5 mg/dL. The index
of consistency based on the average
measures of intraclass correlation
between BiliChek and JM-103 in a
sample of 276 neonates was 0.818
(95% CI, 0.769–0.856), which
is indicative of a high degree of
reliability.
DISCUSSION
Principal Findings
TcB has strong positive linear
correlation with TSB regardless
of the choice of bilirubinometer.
However, TcB is likely to overestimate
TSB by at least 2 mg/dL in ∼6 out
of every 10 black African neonates
screened in the first 120 hours of
life by either BiliChek or JM-103.
3 by guest on May 4, 2019www.aappublications.org/newsDownloaded from

OLUSANYA et al
Increasing postnatal age, exclusive
breastfeeding, and type of
bilirubinometer are predictive of
significant overestimation. Ethnicity,
G6PD status, and skin color are
not significantly associated with
overestimation in this population. TSB
underestimation by both TcB devices
is also minimal. However, JM-103 is
4
TABLE 1 Profi le of Infants With Signifi cant Bilirubin Overestimation in an African Population
Factors No. of Infants Pairs of TcB–TSB Readings (n = 2107)
n = 1553 TcB–TSB ≥2 mg/dL;
n = 1358a (%)
TcB–TSB ≥3 mg/dL;
n = 899a (%)
TcB–TSB ≥4 mg/dL;
n = 542a (%)
Sex
Male 853 757 (65.1) 491 (42.2) 305 (26.2)
Female 700 601 (63.7) 408 (43.2) 237 (25.1)
Birth weight
<2.5 kg 89 83 (68.0) 58 (47.5) 36 (29.5)
≥2.5 kg 1462 1274 (64.2) 840 (42.4) 506 (25.5)
Missing data 2 1 (50.0) 1 (50.0) 0 (0)
Mean (± SD) 3.19 ± 0.50 3.17 ± 0.49 3.15 ± 0.48 3.16 ± 0.49
Gestational age
<37 wk 150 136 (70.5) 96 (49.7) 57 (29.5)
≥37 wk 1383 1208 (63.9) 792 (41.9) 476 (25.2)
Missing data 20 14 (60.9) 11 (47.8) 9 (39.1)
Mean (± SD) 38.18 ± 1.62 38.18 ± 1.71 38.16 ± 1.80 38.14 ± 1.65
Postnatal age, h
0–48 1146 710 (54.2) 384 (29.3) 194 (14.8)
48.1–96 369 583 (81.0) 462 (64.2) 313 (43.5)
96.1–120 38 65 (85.5) 53 (69.7) 35 (46.1)
Ethnicity
Yoruba 1106 981 (65.5) 656 (43.8) 404 (27.0)
Hausa 72 61 (68.5) 34 (38.2) 20 (22.5)
Igbo 198 166 (59.1) 108 (38.4) 57 (20.3)
Other 177 150 (62.8) 101 (42.3) 61 (25.5)
Skin color
Light brown 645 521 (62.0) 356 (42.3) 227 (27.0)
Medium brown 778 718 (66.1) 475 (43.7) 275 (25.3)
Dark brown 130 119 (66.5) 68 (38.0) 40 (22.3)
G6PD-defi cient
No 1290 1103 (63.9) 723 (41.9) 431 (25.0)
Yes 263 255 (67.1) 176 (46.3) 111 (29.2)
Feeding mode
Formula only 276 258 (58.4) 162 (36.7) 78 (17.6)
Exclusive breast milk 1073 902 (65.2) 594 (43.0) 364 (26.3)
Breast milk with formula 204 198 (70.2) 143 (50.7) 100 (35.5)
TcB equipment
BiliChek 325 130 (35.0) 45 (12.1) 20 (5.4)
JM-103 1228 1228 (70.7) 854 (49.2) 522 (30.1)
a n refers to number of infants.
TABLE 2 Predictors of Infants With Signifi cant Bilirubin Overestimation in an African Population After Multivariate Logistic Regression
Factors TcB–TSB ≥2 mg/dL; Adjusted OR
(95% CI)
TcB–TSB ≥3 mg/dL; Adjusted OR
(95% CI)
TcB–TSB ≥4 mg/dL; Adjusted OR
(95% CI)
Postnatal age, h
0–48 Reference Reference Reference
48.1–96 1.41 (1.16–1.66) 1.49 (1.23–1.75) 1.51 (1.20–1.81)
96.1–120 2.00 (1.32–2.68) 1.91 (1.31–2.51) 1.70 (1.10–2.30)
Feeding mode
Formula Reference Reference Reference
Exclusive breast milk 1.96 (1.18–2.74) 1.66 (0.94–2.37) 1.62 (0.71–2.53)
Breast milk with formula 1.90 (0.68–3.12) 1.80 (0.74–2.85) 1.56 (0.37–2.75)
TcB equipment
BiliChek Reference Reference Reference
JM-103 1.55 (1.28–1.81) 2.00 (1.65–2.35) 2.00 (1.51–2.49)
OR adjusted for all factors including G6PD status, TSB level, and interaction term: feeding mode*TSB. All models based on 2107 measurements from 1553 infants by using generalized
estimating equations.
by guest on May 4, 2019www.aappublications.org/newsDownloaded from
PEDIATRICS Volume 138 , number 3 , September 2016
associated with higher imprecision
(mean bias) than BiliChek, which
increases as TSB levels increase.
Comparison With Other Studies
In general, the high and positive
correlation between TcB and TSB is
consistent with the findings in
several studies from racially diverse
populations. 9, 10, 14, 15, 21 – 23 The TSB
overestimation is also corroborated
by several studies among multiracial
populations 10, 13, 24 and black
neonates. 14, 15 For example, although
Maisels et al 10 found a close
correlation between TcB and TSB
values among 849 neonates across
all ethnic groups, by using JM-103,
TSB was overestimated by ≥2 mg/
dL in 37.9% of blacks, compared
with 1.8% of whites or 5.4% of other
races. Among black infants, TSB was
overestimated by ≥3 mg/dL in 17.4%
and by ≥4 mg/dL in 6.7%. TcB was
also consistently higher than TSB
in the black population whenever
the difference between TcB and
TSB was ≥3 mg/dL. Similarly, in a
multicenter study of 769 racially and
ethnically diverse newborns with
at least 1 TcB–TSB pair, Taylor et al
found that African-American race
was independently associated with a
higher chance of TSB overestimation
by at least 2 mg/dL (OR, 2.19; 95%
CI, 1.09–4.39). 13 In a predominantly
black population, 1 study from
Malawi reported TSB overestimation
in term neonates not receiving
phototherapy as indexed by a mean
bias of 1.5 (SD, 4.2) mg/dL in the TcB
measurements.15
JM-103 overestimated TSB in
this population by a greater
magnitude than BiliChek. Studies
comparing BiliChek and JM-103 in
predominantly black populations
are rare. However, the significantly
higher mean measurement bias
associated with JM-103 compared
with BiliChek appears consistent
with findings in other studies among
multiracial populations. 10, 25 –28 For
example, based on a limited sample
of black infants, Maisels et al 10
suggested that although JM-103
correlated with BiliChek, it had a
higher tendency to overestimate TSB.
In another multiracial population
in the United Kingdom, JM-103 was
also found to overestimate TSB in
black infants (mean difference, 1.6
mg/dL; 95% CI, 1.0–2.3 mg/dL) and
underestimate TSB in white infants
(mean difference, –2.2 mg/dL; 95%
CI, –2.7 to –1.7 mg/dL). 25 However,
despite the comparable correlations
between BiliChek and JM-103 in an
Asian population, the former had a
higher tendency to overestimate TSB. 27
To date, only 1 study is known to
have explored the independent
predictors of TcB–TSB divergence. 13
In that study, a postnatal age
5
FIGURE 1Linear regression plots showing the relationship between TSB and TcB measured by BiliChek and JM-103.
by guest on May 4, 2019www.aappublications.org/newsDownloaded from

OLUSANYA et al
of <48 hours was independently
associated with TSB overestimation
by ≥2 mg/dL (OR, 0.36; 95% CI,
0.22–0.59) and ≥3 mg/dL (OR, 0.38;
95% CI, 0.20–0.72). These findings
are in agreement with our study,
which showed that a postnatal age
>48 hours was associated with
higher odds of TSB overestimation
at all levels. This may be due to
the gradual reduction in the total
blood flow through the skin and
muscle during the first 7 days of
life within the neonatal period. 29
The study by Taylor et al 13 also
showed that TcB had a tendency
to be less accurate at higher TSB
levels, regardless of the type of
bilirubinometer ( Fig 4). Other studies
among whites seem to support this
finding, 30 suggesting that it was not
race dependent. This observation
may possibly be attributable to the
dynamic processes, such as changes
in hemoglobin concentration, in the
early hours of life. 13
The association between
exclusive breastfeeding and TSB
overestimation appears to be
supported by other reports on
TcB patterns in relation to feeding
mode. 31 – 33 Itoh and colleagues, 33 for
example, proposed that increased
unconjugated bilirubin in breastfed
infants may be underpinned by
the high enterohepatic circulation
of unconjugated bilirubin from
deconjugation by β-glucuronidase of
the conjugated bilirubin in meconium.
The resultant increase in circulating
unconjugated bilirubin may therefore
be related to the observed higher
TcB/TSB discrepancy. The observed
TSB overestimation by at least ≥4
mg/dL in this population warrants
additional investigation.34
Our study also suggests that tribe
or shades of skin color in the
black race has little or no effect
on TcB performance. This is in
accordance with an earlier study that
demonstrated strong correlations
between TcB and TSB regardless of
the degree of skin pigmentation. 14
Clinical Implications of Key Findings
To optimize its utility, high TcB
levels from any instrument should
precipitate a valid concern about the
risk of severe hyperbilirubinemia or
kernicterus in the tested infant that
6
FIGURE 2Receiver operating characteristic curves for BiliChek and JM103 for predicting infants who require phototherapy based on AAP 2004 guidelines. AUC, area under the curve.
by guest on May 4, 2019www.aappublications.org/newsDownloaded from
PEDIATRICS Volume 138 , number 3 , September 2016
requires a follow-up blood sampling
for TSB or provide assurance where
such risk does not exist. Within
this context, the strong correlation
between TcB and TSB confers some
merit on the former as a screening
tool as well as a potential alternative
to TSB in resource-limited settings.
TcB should, for example, be preferred
to the highly subjective visual
assessment that prevails in such
settings. However, the evidence
from the current study and similar
reports 10, 13 would suggest some
caution in placing sole reliance on
TcB as a basis for clinical decisions
to guide phototherapy or exchange
transfusions in black African neonates.
Perhaps more notable is the ample
evidence that the commonly reported
satisfactory statistical correlation
between TcB and TSB masks clinically
significant discrepancies between
the 2 measures at the individual
patient level. TSB should therefore
continue to be regarded as an
absolute necessity, notwithstanding
the common challenges in ensuring
its availability routinely. In settings
where a high proportion of infants
are born outside hospitals and late
presentation of high-risk infants is
frequent, the utility of TcB is likely
to be severely limited considering
the significant imprecision of
measurements at high TSB levels.
This is without prejudice to studies
that suggest improved predictive
utility of TcB when combined with
clinical risk factors. 5 It may be argued
that the divergence between TcB and
TSB should not be unexpected after
all, because the former measures
the extravascular rather than the
intravascular bilirubin concentration,
and possibly better reflects the risk
of kernicterus. 35 However, additional
studies are warranted to establish
more precisely the clinical value of
TcB as a predictor of kernicterus.
Our study also underscores the
need to consider the performance
and cost-effectiveness of available
TcB equipment. Of the 3 predictors
in this population, choice of TcB
device is the most modifiable factor.
Available cost estimates suggest
that BiliChek is more expensive than
JM-103 because of the added running
cost for consumables. However,
a more robust cost-effectiveness
analysis should be considered for
the latest models of all commercially
available instruments to guide the
expected trade-off among devices.
To our knowledge, no instrument
has been developed specifically to
address TSB overestimation in the
black population. Although there
is a need to explore technological
7
FIGURE 3Bland-Altman plots of agreement between TcB and TSB for BiliChek and JM-103.
by guest on May 4, 2019www.aappublications.org/newsDownloaded from

OLUSANYA et al
improvement for TcB devices for
this racial group, efforts to develop
low-cost, point-of-care TSB devices
are currently in progress and, if
successful, hold promise for low-
and middle-income countries. 8 It
may also be helpful to consider the
development of equipment-specific
TcB nomograms in this population.
Strengths and Limitations of Study
A major strength of this study is
the large sample of exclusively
black African neonates. This is the
first study, to our knowledge, to
characterize the pattern and the risk
factors of the divergence between
TcB and TSB in this population. Unlike
previous studies, we were able to
compare the performance of 2 common
TcB equipment models. However, only
2 TcB models were evaluated, which
may restrict generalization to other
TcB instruments. It was also unclear if
the use of BiliChek for a significantly
shorter duration impacted the findings.
We could not determine the effect
of deriving TcB measurements from
the forehead compared with the
sternum. It was unclear how the
finding on skin color and ethnicity
would have been moderated by
comparison with white infants.
Additionally, this study was conducted
among inborn infants and may not
provide an accurate picture of the
pattern of divergence among outborn
infants that are frequently exposed to
hemolytic infant care products in this
population. 16 Notwithstanding, our
study has provided valuable and rare
insights to the potential limitations of
TcB as a screening tool or proxy for
TSB among black African neonates to
inform clinical decisions and additional
technological development of TcB
devices for the optimal care of infants
at risk for avoidable kernicterus.
CONCLUSIONS
TcB is noninvasive, simple to
perform, less expensive, and
has a satisfactory correlation
with TSB. However, current TcB
devices are highly sensitive only
at lower TSB levels and are more
likely to overestimate TSB with
increasing age by at least 2 mg/dL
in ∼6 out of every 10 black African
neonates and up to 9 mg/dL in
some neonates. The LOA depend
on the type of bilirubinometer
used, with JM-103 having a greater
tendency to overestimate TSB than
BiliChek. This divergence should
be recognized in the management
of infants at risk for kernicterus to
avoid unnecessary blood sampling or
excessive treatments where routine
confirmatory TSB is impracticable.
Technological advancement for
improved bilirubin determination is
warranted for this population.
ACKNOWLEDGMENTS
We thank Tina Slusher for the
provision of the bilirubinometers and
G6PD test kits used in this study. We
also thank the research team at the
Centre for Healthy Start Initiative
for assistance in data retrieval and
management.
8
ABBREVIATIONS
AAP: American Academy of
Pediatrics
CI: confidence interval
G6PD: glucose-6-phosphate
dehydrogenase
LOA: limits of agreement
OR: odds ratio
TcB: transcutaneous bilirubin
TSB: total serum bilirubin
FINANCIAL DISCLOSURE: The transcutaneous bilirubin devices used in this study were provided by Philips Healthcare North America (Monroeville, PA) and
Draeger Medical (Telford, PA). The authors have indicated they have no other fi nancial relationships relevant to this article to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential confl icts of interest to disclose.
FIGURE 4Pattern of TcB–TSB differences at various levels of TSB between BiliChek and JM-103. Data shown are mean values of TcB–TSB differences with 95% CI error bars.
by guest on May 4, 2019www.aappublications.org/newsDownloaded from

PEDIATRICS Volume 138 , number 3 , September 2016
REFERENCES
1. Watchko JF. Hyperbilirubinemia in
African American neonates: clinical
issues and current challenges.
Semin Fetal Neonatal Med.
2010;15(3):176–182
2. Wickremasinghe AC, Kuzniewicz
MW, Newman TB. Black race is
not protective against hazardous
bilirubin levels. J Pediatr.
2013;162(5):1068–1069
3. ̀Kaplan M, Herschel M, Hammerman
C, Karrison T, Hoyer JD, Stevenson
DK. Studies in hemolysis in glucose-6-
phosphate dehydrogenase-defi cient
African American neonates. Clin Chim
Acta. 2006;365(1-2):177–182
4. American Academy of Pediatrics
Subcommittee on Hyperbilirubinemia.
Management of hyperbilirubinemia
in the newborn infant 35 or more
weeks of gestation. Pediatrics.
2004;114(1):297–316
5. Engle WD, Jackson GL, Engle NG.
Transcutaneous bilirubinometry.
Semin Perinatol. 2014;38(7):438–451
6. el-Beshbishi SN, Shattuck
KE, Mohammad AA, Petersen
JR. Hyperbilirubinemia and
transcutaneous bilirubinometry. Clin
Chem. 2009;55(7):1280–1287
7. National Institute for Health and
Clinical Excellence. Jaundice in
newborn babies under 28 days
(Clinical guideline 98). Available at:
www. nice. org. uk/ CG98. Accessed
March 10, 2016
8. Olusanya BO, Ogunlesi TA, Kumar P, et
al. Management of late-preterm and
term infants with hyperbilirubinaemia
in resource-constrained settings. BMC
Pediatr. 2015;15:39
9. Bhutani VK, Gourley GR, Adler S,
Kreamer B, Dalin C, Johnson LH.
Noninvasive measurement of total
serum bilirubin in a multiracial
predischarge newborn population
to assess the risk of severe
hyperbilirubinemia. Pediatrics.
2000;106(2). Available at: www.
pediatrics. org/ cgi/ content/ full/ 106/ 2/
e17
10. Maisels MJ, Ostrea EM Jr, Touch S,
et al. Evaluation of a new transcutaneous
bilirubinometer. Pediatrics.
2004;113(6):1628–1635
11. Samiee-Zafarghandy S, Feberova J,
Williams K, Yasseen AS, Perkins SL,
Lemyre B. Infl uence of skin colour
on diagnostic accuracy of the
jaundice meter JM 103 in newborns.
Arch Dis Child Fetal Neonatal Ed.
2014;99(6):F480–F484
12. Olusanya BO, Ogunlesi TA, Slusher TM.
Why is kernicterus still a major cause
of death and disability in low-income
and middle-income countries? Arch Dis
Child. 2014;99(12):1117–1121
13. Taylor JA, Burgos AE, Flaherman V, et
al; Better Outcomes through Research
for Newborns Network. Discrepancies
between transcutaneous and serum
bilirubin measurements. Pediatrics.
2015;135(2):224–231
14. Slusher TM, Angyo IA, Bode-Thomas
F, et al. Transcutaneous bilirubin
measurements and serum total
bilirubin levels in indigenous
African infants. Pediatrics.
2004;113(6):1636–1641
15. Rylance S, Yan J, Molyneux E. Can
transcutaneous bilirubinometry
safely guide phototherapy treatment
of neonatal jaundice in Malawi?
Paediatr Int Child Health.
2014;34(2):101–107
16. Olusanya BO, Osibanjo FB, Mabogunje
CA, Slusher TM, Olowe SA. The
burden and management of neonatal
jaundice in Nigeria: a scoping review
of the literature. Niger J Clin Pract.
2016;19(1):1–17
17. Beutler E, Blume KG, Kaplan JC,
Löhr GW, Ramot B, Valentine WN.
International Committee for
Standardization in Haematology:
recommended screening test for
glucose-6-phosphate dehydrogenase
(G-6-PD) defi ciency. Br J Haematol.
1979;43(3):465–467
18. Slusher TM, Olusanya BO, Vreman
HJ, et al. A randomized trial of
phototherapy with fi ltered sunlight
in African neonates. N Engl J Med.
2015;373(12):1115–1124
19. Bland JM, Altman DG. Measuring
agreement in method comparison
studies. Stat Methods Med Res.
1999;8(2):135–160
20. Hanley JA, McNeil BJ. The meaning
and use of the area under a receiver
operating characteristic (ROC) curve.
Radiology. 1982;143(1):29–36
21. Leite M, Granato VA, Facchini FP, Marba
ST. Comparison of transcutaneous
and plasma bilirubin measurement. J
Pediatr (Rio J). 2007;83(3):283–286
22. Akahira-Azuma M, Yonemoto N,
Ganzorig B, et al. Validation of a
transcutaneous bilirubin meter in
Mongolian neonates: comparison with
total serum bilirubin. BMC Pediatr.
2013;13:151
23. Panburana J, Boonkasidach
S, Rearkyai S. Accuracy of
transcutaneous bilirubinometry
compare to total serum bilirubin
measurement. J Med Assoc Thai.
2010;93(suppl 2):S81–S86
24. Wainer S, Rabi Y, Parmar SM, Allegro
D, Lyon M. Impact of skin tone on the
performance of a transcutaneous
jaundice meter. Acta Paediatr.
2009;98(12):1909–1915
25. Thomson J, Culley V, Monfrinoli
A, Sinha A. Transcutaneous
bilirubinometers and ethnicity.
Arch Dis Child Fetal Neonatal Ed.
2008;93(6):F474
26. Raimondi F, Lama S, Landolfo F, et al.
Measuring transcutaneous bilirubin: a
comparative analysis of three devices
on a multiracial population. BMC
Pediatr. 2012;12:70
27. Sanpavat S, Nuchprayoon I.
Comparison of two transcutaneous
bilirubinometers–Minolta AirShields
Jaundice Meter JM103 and Spectrx
Bilicheck–in Thai neonates. Southeast
Asian J Trop Med Public Health.
2005;36(6):1533–1537
28. Ebbesen F, Vandborg PK, Trydal T.
Comparison of the transcutaneous
bilirubinometers BiliCheck and Minolta
JM-103 in preterm neonates. Acta
Paediatr. 2012;101(11):1128–1133
29. Wu PY, Wong WH, Guerra G, et al.
Peripheral blood fl ow in the neonate;
1. Changes in total, skin, and
muscle blood fl ow with gestational
and postnatal age. Pediatr Res.
1980;14(12):1374–1378
30. Yamauchi Y, Yamanouchi I.
Transcutaneous bilirubinometry: effect
of postnatal age. Acta Paediatr Jpn.
1991;33(5):663–667
9 by guest on May 4, 2019www.aappublications.org/newsDownloaded from

OLUSANYA et al
31. Maisels MJ, Clune S, Coleman K, et
al. The natural history of jaundice
in predominantly breastfed infants.
Pediatrics. 2014;134(2). Available at:
www. pediatrics. org/ cgi/ content/ full/
134/ 2/ e340
32. Draque CM, Sañudo A, de Araujo Peres
C, de Almeida MF. Transcutaneous
bilirubin in exclusively breastfed
healthy term newborns up to 12
days of life. Pediatrics. 2011;128(3).
Available at: www. pediatrics. org/ cgi/
content/ full/ 128/ 3/ e565
33. Itoh S, Kondo M, Kusaka T, Isobe K,
Onishi S. Differences in transcutaneous
bilirubin readings in Japanese term
infants according to feeding method.
Pediatr Int. 2001;43(1):12–15
34. Kaplan M, Herschel M, Hammerman
C, Hoyer JD, Heller GZ, Stevenson DK.
Neonatal hyperbilirubinemia in
African American males: the
importance of glucose-6-phosphate
dehydrogenase defi ciency. J Pediatr.
2006;149(1):83–88
35. Bosschaart N, Kok JH, Newsum AM,
et al. Limitations and opportunities
of transcutaneous bilirubin
measurements. Pediatrics.
2012;129(4):689–694
10 by guest on May 4, 2019www.aappublications.org/newsDownloaded from

originally published online August 30, 2016; Pediatrics Bolajoko O. Olusanya, Donald O. Imosemi and Abieyuwa A. Emokpae
Black African NeonatesDifferences Between Transcutaneous and Serum Bilirubin Measurements in
ServicesUpdated Information &
016-0907http://pediatrics.aappublications.org/content/early/2016/08/27/peds.2including high resolution figures, can be found at:
References
016-0907#BIBLhttp://pediatrics.aappublications.org/content/early/2016/08/27/peds.2This article cites 34 articles, 11 of which you can access for free at:
Subspecialty Collections
bhttp://www.aappublications.org/cgi/collection/hyperbilirubinemia_suHyperbilirubinemiasubhttp://www.aappublications.org/cgi/collection/fetus:newborn_infant_Fetus/Newborn Infantfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on May 4, 2019www.aappublications.org/newsDownloaded from

originally published online August 30, 2016; Pediatrics Bolajoko O. Olusanya, Donald O. Imosemi and Abieyuwa A. Emokpae
Black African NeonatesDifferences Between Transcutaneous and Serum Bilirubin Measurements in
http://pediatrics.aappublications.org/content/early/2016/08/27/peds.2016-0907located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://pediatrics.aappublications.org/content/suppl/2016/08/25/peds.2016-0907.DCSupplementalData Supplement at:
1073-0397. ISSN:60007. Copyright © 2016 by the American Academy of Pediatrics. All rights reserved. Print
the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on May 4, 2019www.aappublications.org/newsDownloaded from







