
Direct Acting Antivirals: What are they? What is their place in HCV management?
Mark Sulkowski, MDAssociate Professor of Medicine
Johns Hopkins University School of Medicine
Limitations of PegIFN + Ribavirin (with or without protease inhibitors)
• Antiviral activity is host + virus genotype dependent – IL28B CC genotype > TC and TT
• Safety and tolerability risk outweighs treatment benefit for some individuals– “IFN unwilling and/or unable”
• Finite number of expert healthcare providers • Cost
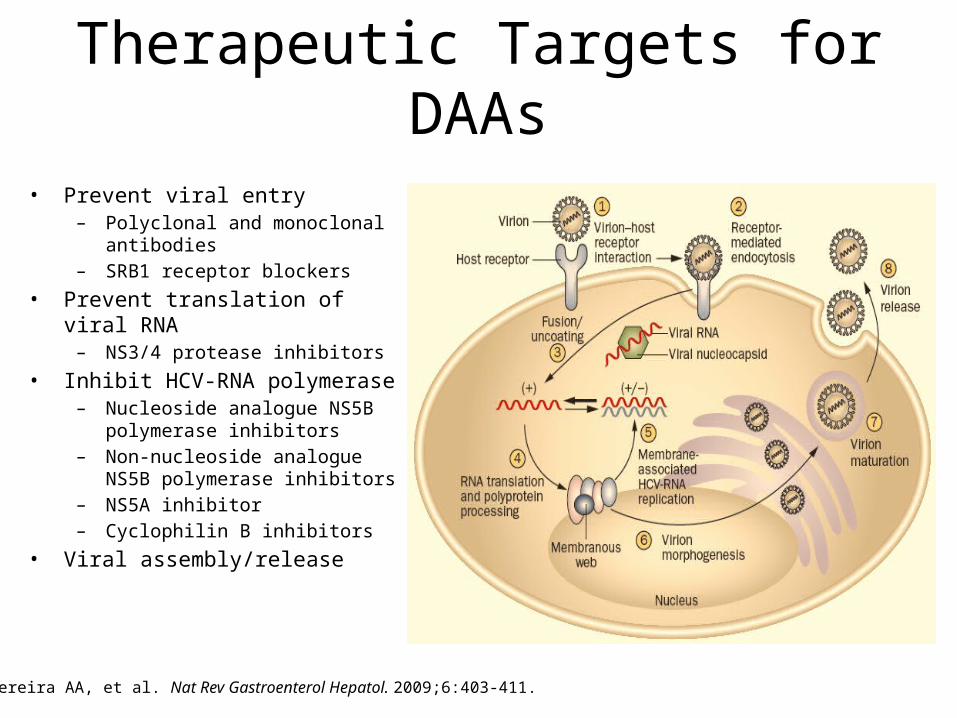
Therapeutic Targets for DAAs
Pereira AA, et al. Nat Rev Gastroenterol Hepatol. 2009;6:403-411.
• Prevent viral entry– Polyclonal and monoclonal antibodies– SRB1 receptor blockers
• Prevent translation of viral RNA– NS3/4 protease inhibitors
• Inhibit HCV-RNA polymerase– Nucleoside analogue NS5B polymerase
inhibitors– Non-nucleoside analogue NS5B
polymerase inhibitors– NS5A inhibitor– Cyclophilin B inhibitors
• Viral assembly/release

Direct Acting Antivirals for Hepatitis C
Nature Reviews Drug Discovery 10, 93-94 (February 2011) | doi:10.1038/nrd3361

New Targets
• Peginterferon lambda (PegIL-29)• Protease inhibitors • Polymerase inhibitors• NS5A inhibitors • Cyclophilin inhibitors• DAA Combinations

Peginterferon lambda + RBVVirologic response by IL28B Genotype in patients with HCV Genotypes 1, 4
0
n = 19 46 22 38 17 40 18 57 19 46 22 38 17 40 18 57
RVR cEVR
102030405060708090
100
Hatched bars: CT/TTSolid bars: CC
120 μg 180 μg 240 μg PegIFN-λ
180 μgPegIFN-α-2a
120 μg 180 μg 240 μg PegIFN-λ
180 μgPegIFN-α-2a
Perc
enta
ge o
f pati
ents
± 9
5% C
I
Zeuzem et al. EASL 2011

Changes in Hematologic Parameters Over Time and Hematology-associated PegIFN and RBV Dose Reductions
Hem
oglo
bin
(g/L
)Pl
atel
ets
(GI/
L)
T
otal
Neu
trop
hils
(G
I/L)
LLN
Study Week
LLN
150
140
130
120
0 6 8 10 122 4
300
250
200
150
0 6 8 10 122 4
54
21
3
0 6 8 10 122 4
LLN
PegIFN-λ 120 µg PegIFN-λ 180 µgPegIFN-λ 240 µg PegIFN-α-2a
PegIFN-λPegIFN
α-2a
Lab Toxicity, %120 µg(N=128)
180 µg(N=131)
240 µg(N=134)
180 µg(N=133)
Hemoglobin low 20.5 15.4 12.9 43.9
RBV dose reduction, % (due to Hb abnormality)
2.3 1.5 0.7 12.8
Neutrophils Low 0 0.8 0 15.2Platelets Low 0 0 0 14.4
PegIFN dose reduction, % (due to hematologic abnormality)
0 0 0 17.3
Zeuzem et al EASL 2011

New Targets
• Peginterferon lambda (PegIL-29)• Protease inhibitors • Polymerase inhibitors• NS5A inhibitors • Cyclophilin inhibitors• DAA Combinations

PILLAR Study: TMC435 + PegIFN/RBV
Fried et al. AASLD 2010
TMC 12/ PR24
75 mg(n=77)
TMC 24/PR24
75 mg(n=75)
TMC 12/ PR24
150 mg(n=76)
TMC 24/PR24
150 mg(n=75)
Pbo 24/PR48
(n=75)
TMC 12/ PR24
75 mg(n=78)
TMC 24/PR24
75 mg(n=73)
TMC 12/ PR24
150 mg(n=77)
TMC 24/PR24
150 mg(n=77)
Pbo 24/PR48
(n=74)
0
20
40
60
80
100
77 68 76 79
5
91 96 94 97
58
10 2016 17
11
2 1 3
11
<25 IU/mL undetectable <25 IU/mL detectable >25 IU/ml
Week 4 Week 12*** *** *** *** *** *** *** ***
PILLAR Week 24 Analysis: Proportion of Patients Achieving Virologic Response at Weeks 4 and 12
Fried MW, et al. 61st AASLD; Boston, MA; October 29 – November 2, 2010; Abst. LB-5.

PILLAR Study: Role of IL28B GenotypePILLAR Week 24 Analysis: Mean Change in HCV RNA
from Baseline According to IL28B Genotype*
Mea
n(+/
- SE)
Cha
nge
in P
lasm
a H
CV R
NA
(log 10
IU/m
L) fr
om B
asel
ine CC
CTTT
Placebo
4 8 16 240
0
-2
-4
-6
Week12 20
All TMC 435 (75 mg)
Week
0
-2
-4
-64 8 16 240 12 20
All TMC 435 (150 mg)
Week
0
-2
-4
-64 8 16 240 12 20
Fried MW, et al. 61st AASLD; Boston, MA; October 29 – November 2, 2010; Abst. LB-5.
Fried et al. AASLD 2010

SILEN-C1: BI-1335 + PegIFN/RBV with or without 3-day lead-in
eRVR SVR Relapse0
20
40
60
80
100
15
55
24
8071
9
7873
15
8883
8
PR BI1335 120 mg LIBI1335 240 mg LI BI1335 240 mg No LI
Sulkowski et al. EASL 2011

New Targets
• Peginterferon lambda (PegIL-29)• Protease inhibitors • Polymerase inhibitors• NS5A inhibitors • Cyclophilin inhibitors• DAA Combinations

Mericitabine + PegIFN/RBV for HCV genotype 1 patients
0 2 4 6 8 10 120%
20%
40%
60%
80%
100%
39%
83%62%
68%
62%
88%
62%80%
18%
49%
A: 500mg BID+ P/R 12 wk (n=80)B: 1000mg BID+ P/R 8 wk (n=81)C: 1000mg BID+ P/R 12 wk (n=82)D: 1000mg BID+ P/R 12 wk (n=81)E: P/R 48 wk (n=84)
Study Week
% P
atien
ts w
ith
viro
logi
c re
spon
se (<
15IU
mL)
*
0
*Roche COBAS® HCV Test; LLOD = 15 IU/mLITT population, n=408
Jensen DM, et al. 61st AASLD; Boston, MA; October 29 – November 2, 2010; Abst. 81.
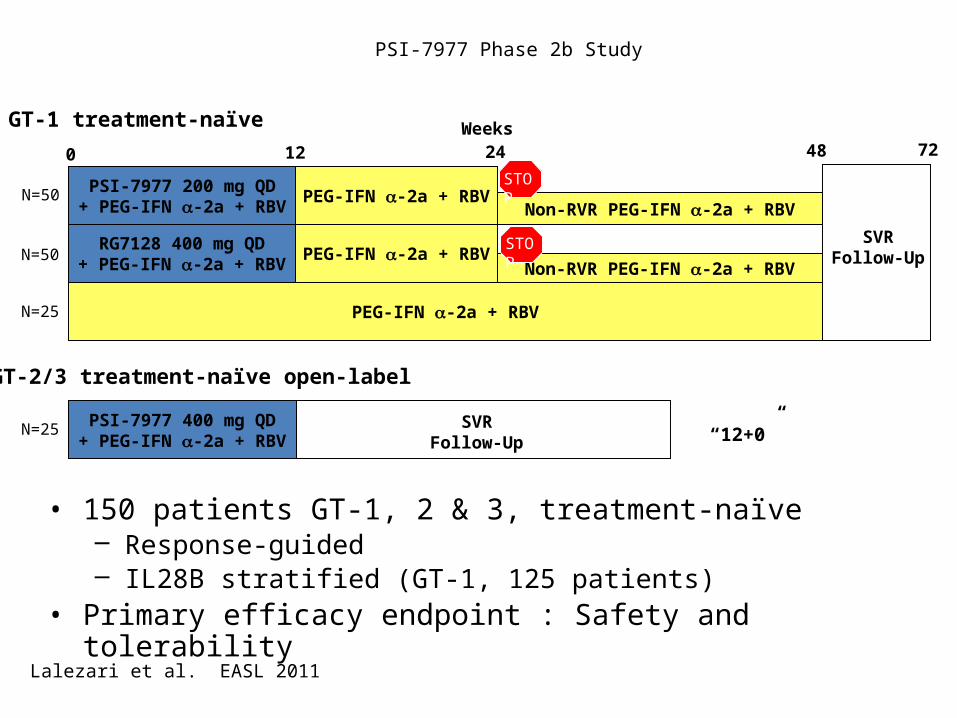
PSI-7977 Phase 2b Study
PEG-IFN -2a + RBV
RG7128 400 mg QD+ PEG-IFN -2a + RBV
PSI-7977 200 mg QD+ PEG-IFN -2a + RBV
PEG-IFN -2a + RBVNon-RVR PEG-IFN -2a + RBV
PEG-IFN -2a + RBVNon-RVR PEG-IFN -2a + RBV
0 12 24 48Weeks
SVRFollow-Up
72
STOP
STOP
• 150 patients GT-1, 2 & 3, treatment-naïve– Response-guided– IL28B stratified (GT-1, 125 patients)
• Primary efficacy endpoint : Safety and tolerability
PSI-7977 400 mg QD+ PEG-IFN -2a + RBV
SVRFollow-Up
GT-1 treatment-naïve
GT-2/3 treatment-naïve open-label
N=50
N=50
N=25
N=25 “12+0”
Lalezari et al. EASL 2011

PSI-7977 + PegIFN + RBV
Series10
20
40
60
80
100 98
19
Week 4
PSI7977 200 or 400 mg/P/RPR
• 121 patients with HCV genotype 1– 41% IL28B CC
• No viral breakthrough observed
• No safety signal detected

New Targets
• Peginterferon lambda (PegIL-29)• Protease inhibitors • Polymerase inhibitors• NS5A inhibitors • Cyclophilin inhibitors• DAA Combinations

M Gao et al. Nature 000, 1-5 (2010) doi:10.1038/nature08960
BMS-790052 Replication Complex Inhibitor:Change in HCV RNA after administration of single dose

NS5A replication complex inhibitor + PegIFN/RBV
PR (n=12) NS5A 1 mg (n=12) NS5A 10 mg (n=12) NS5A 60 mg (n=12)0
20
40
60
80
100
25
42
9283
SVR
Pol et al. EASL 2011

New Targets
• Peginterferon lambda (PegIL-29)• Protease inhibitors • Polymerase inhibitors• NS5A inhibitors • Cyclophilin inhibitors• DAA Combinations
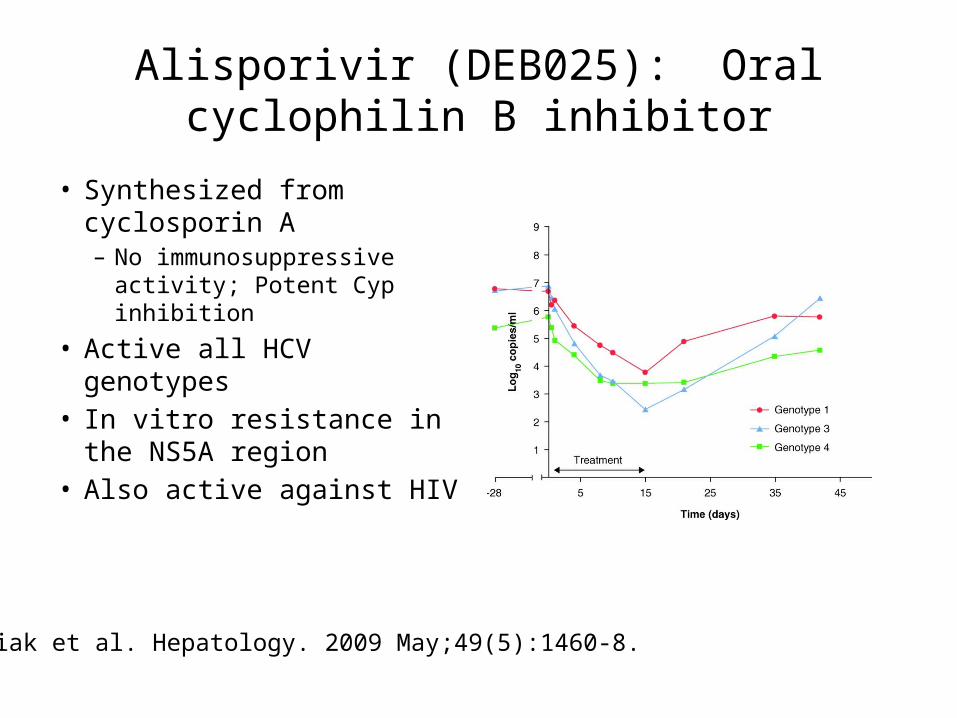
Alisporivir (DEB025): Oral cyclophilin B inhibitor
• Synthesized from cyclosporin A– No immunosuppressive
activity; Potent Cyp inhibition
• Active all HCV genotypes• In vitro resistance in the
NS5A region• Also active against HIV
Flisiak et al. Hepatology. 2009 May;49(5):1460-8.

Alisporivir + PegIFN/RBV in HCV genotype 1, treatment naïve patients
PR APV 48 wks APV 24 wks RGT0
20
40
60
80
55
76
53
69
SVR
Flisiak R et al. EASL 2011
New Targets
• Peginterferon lambda (PegIL-29)• Protease inhibitors • Polymerase inhibitors• NS5A inhibitors • Cyclophilin inhibitors• DAA Combinations

INFORM-1: RG7128 + RG7227
• 1st clinical trial to investigate the combination of DAA in the absence of interferon and ribavirin
• Assessed safety and antiviral activity of RG7128 + RG7227 x13d• Rx-naïve, null and relapser GT-1 HCV patients (N ~90)• No evidence of resistance breakthrough in any cohort
Gane et al. The Lancet 15 Oct 2010

Telaprevir + VX-222 with or with PegIFN/RBV
TLV + 222 low
TLV + 222 high
QUAD low
QUAD high
0
20
40
60
80
100
17
59
86 87
RVR
TLV + 222 low
TLV + 222 high
QUAD low
QUAD high
0
20
40
17
31
0 0
Breakthrough

SOUND C-1: PI (1335) + non-nucleoside polymerase (7127) + RBV
Day 8 Day 15 Day 22 Day 29
Group 1:7127 (400 mg TID) +
1335 + RBV(N=15)
27% 40% 67% 73%
Group 2:7127 (600 mg TID) +
1335 + RBV(N=17)
18% 82% 100% 100%
HCV RNA < 25 IU/mL, undetectable
Two genotype 1a patients in the low dose group had viral rebound during treatment
Zeuzem S., et al. 61st AASLD; Boston, MA; October 29 – November 2, 2010; Abst. LB-7.

PI + NS5A inhibitor ± PegIFN/RBV in prior null responder
0 1 2 3 4 5 6 7 8 9 10 11 120
1
2
3
4
5
6
7
8
Group A: No PegIFN/RBV, n = 11
Week
Log1
0 H
CV R
NA
↓ Indicates Initiation of PegIFN/RBV↓
↓
↓
LOQ 26 IU/mL LOD < 10 IU/mL
0 1 2 3 4 5 6 7 8 9 10 11 120
1
2
3
4
5
6
7
8
Group B: PegIFN/RBV, n =10
Week
Log1
0 H
CV R
NA
LOQ 26 IU/mL LOD < 10 IU/mL
LOQ LOD
LOQ LOD
Lok AS, et al. 61st AASLD; Boston, MA; October 29 – November 2, 2010; Abst. LB-8.

PI + NS5A inhibitor ± PegIFN/RBV in prior null responder
• No PegIFN/RBV– 4/11 patients had SVR-12 with no PegIFN/RBV
• 1a, 2/3 SVR with 1 relapse; 1b; 2/2
– 6/11 patients had breakthrough with PegIFN/RBV added 4 achieve undetectable HCV RNA (treatment ongoing)
• QUAD therapy (PegIFN/RBV)– 10/10 patients had SVR-12
Lok AS, et al. EASL; Berlin, Germany 2011

Future HCV therapies
• Multiple agents in phase 2 or later development – Effective across viral genotypes and subtypes– Different resistant variants – Improved safety and tolerability – Oral (with the exception of IFN λ)– Less frequent dosing
• Increase HCV treatment rates with IFN alfa free regimens







