
Evidence-based Medicine: Treatment of Crohn’s Disease
Raymond Cross, MD, MS, AGAF Professor of Medicine Director, IBD Program
University of Maryland School of Medicine Co-Director Digestive Health Center
University of Maryland Medical Center Millie Long, MD, MPH
Assistant Professor of Medicine University of North Carolina

Disclosures
• Abbvie: Research grants, participation in advisory boards, and consulting
• Janssen: Participation in advisory boards
• Takeda: Consulting
• UCB: Consulting

Goals of Therapy
• Induce clinical remission (absence of symptoms)
• Avoid short and long term toxicity of therapy
• Maintain steroid-free remission
– Avoid repeated courses of steroids
• Enhance quality of life
• Prevent/treat complications of disease
• Achieve mucosal healing (“deep remission”)
• Decrease unnecessary health care expenditures (ER visits, hospitalizations, etc.)

Pentasa reduces CDAI compared to placebo
Clinical Gastroenterology and Hepatology 2004; 2:379-388
Copyright © 2004 American Gastroenterological Association Terms and Conditions
5-ASA Associated with Small Clinical Benefit in Crohn’s Disease

Rifaximin-extended Intestinal Release in Patients with Crohn’s Disease
43
54
62*
47
0
10
20
30
40
50
60
70
Pe
rce
nt
of
Pat
ien
ts in
Clin
ical
R
em
issi
on
Placebo 400 bid 800 bid 1200 bid
Prantera, C et al. (2012) Gastroenterology *p=0.005 compared to placebo
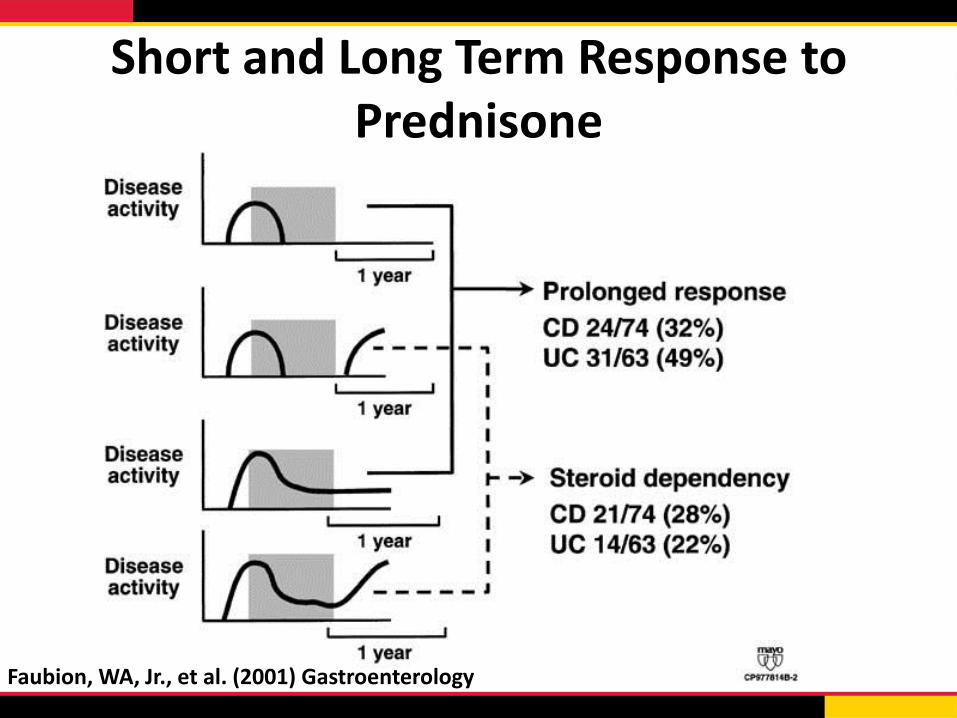
Short and Long Term Response to Prednisone
Faubion, WA, Jr., et al. (2001) Gastroenterology

ORAL BUDESONIDE IN ACTIVE
CROHN’S DISEASE

AZATHIOPRINE AS
MAINTENANCE THERAPY FOR
CROHN’S DISEASE

Early Azathioprine vs. Conventional Management
Cosnes, J, et al. (2013) Gastroenterology

Early Azathioprine in Newly Diagnosed CD
Characteristics Placebo (n=63) Azathioprine (n=68)
Steroid-free Remission at Week 76 (Primary Endpoint)
23 (37%) 30 (44%)
Patients Needing Steroids 40 (64%) 34 (50%)
Mean Days of Steroids 64+/-58 47+/-74
Development of Fistula 5 (8%) 6 (9%)
Internal Penetrating Disease 3 (5%) 4 (6%)
Perianal Fistulizing Disease 2 (3%) 2 (3%)
Patients Hospitalized 5 (8%) 11 (16%)
CD-related Surgery 1 (2%) 1 (1%)
Panés, J, et al. (2013) Gastroenterology

METHOTREXATE FOR ACTIVE
CROHN’S DISEASE

Feagan, BG, et al. (2000) N Engl J Med
Moderate-to-Severe CD: Maintenance of Remission with MTX
• Multicenter, randomized, controlled trial
• 76 steroid-dependent patients
• In remission following MTX 25 mg x 16 weeks
• Randomized to MTX 15 mg or placebo x 40 weeks
30
0 4 12 28 16 20 8 24 32 36 40
Weeks since Randomization
80
70
100
90
60
50
40
Rem
issio
n (
%)
MTX
Placebo
n=40
65%
n=36
39%

0
20
40
60
80
100
Infliximab 5 mg/kg (ACCENT I)
Certolizumab 400 mg 4-weekly (PRECiSE 2)
Adalimumab 40 mg EOW (CHARM)
Week 26–30
Long Term Maintenance of Remission in CD
N = 113 N = 113 N = 215 N = 215
Remission (CDAI<150)
N = 172 N = 172
Response (Δ100)
Reduction (≥ 70 pts and
≥ 25% in CDAI)
Pe
rce
nt
of
Pat
ien
ts
21 17 29 36 26 27
Placebo
51 52
63
39 40 48

Accent II-Fistula Response at Week 54
23 19
46
36
0
5
10
15
20
25
30
35
40
45
50
Fistula Response Complete Response
Pe
rce
nt
of
Pat
ien
ts
Placebo IFX
* *
* p<0.05
Sands, B. E., et al. (2004). N Engl J Med

Early Combined Therapy Associated with Better Short Term Results
0
10
20
30
40
50
60
70
14 26 52 78 104
Pe
rce
nt
of
pat
ien
ts
Weeks
Early combined IS group Conventional group
* * *
* p<0.05
D'Haens, G., et al. (2008). Lancet

Early Biologic Treatment Results in Higher Rates of Endoscopic Healing at 2 Years
Secondary End Point of the Top-Down/Step-Up Trial
P=0.0028
D'Haens, G., et al. (2008). Lancet 371(9613): 660-667. Baert, F., et al. (2010). Gastroenterology 138(2): 463-468; quiz e410-461.
Pati
en
ts (
%)
0
100
Step-up
80
60
40
20
Top-down
Complete Endoscopic Healing at 2 Years
30
73
Simple endoscopic score 0 Simple endoscopic score 1–9
…and these patients did better in the next 2 yrs!
Pati
en
ts I
n
Rem
issio
n (
%)
0 Remission
Off Steroids
80
60
40
20
Off Steroids, No Anti-TNF
70.8
27.3
62.5
18.2

Comparative Effectiveness Study in CD (SONIC)
Colombel, J.F., et al. N Engl J Med. 2010;362(15):1383-1395
Pati
en
ts (
%)
P=.02
P<.001
P=.06 P=.006
P=0.02
P<.001
51/170 75/169 96/169 18/109 28/93 47/107 P
ati
en
ts (
%)
30.0%
44.4%
56.8%
16.5%
30.1%
43.9%
100
0 AZA + PBO
IFX + PBO
IFX + AZA
AZA + PBO
IFX + PBO
IFX + AZA
Clinical Remission Mucosal Healing
90
80
70
60
50
40
30
20
10
100
0
90
80
70
60
50
40
30
20
10
PBO = placebo; IFX = infliximab.

0
20
40
60
80
100
0 4 8 12 16 20 24 28 32 36 40 44 48 52
Weeks
MTX Placebo
No Benefit of MTX in Addition to Steroids and IFX for CD
Feagan, B. G., et al. (2014). Gastroenterology
n= 63/group
Pati
en
ts i
n r
em
issio
n [
%]
Prednisone
taper week 0-14
Treatment failure week 14: 24% IFX/MTX, 22% IFX
Treatment failure week 50: 44% IFX/MTX, 43% IFX

Vedolizumab in CD: Second Induction Study
Clinical Remission (CDAI ≤150) at Week 10 (Secondary Endpoint)
Sands, B. E., et al. (2014). Gastroenterology 147(3): 618-627 e613.
.

GEMINI II: Vedolizumab in Crohn’s Disease Through Week 52, Maintenance ITT
Sandborn, W. J., et al. (2013). N Engl J Med 369(8): 711-721.

Ustekinumab Induction Therapy for Anti-TNF Experienced Patients (UNITI-1)
7%
20% 16%
34%
21%
38%
0%
5%
10%
15%
20%
25%
30%
35%
40%
Remission Response
Pe
rce
nt
of
Pat
ien
ts
Placebo 130 mg 6 mg/kg
Feagan, B. G., et al. (2016). N Engl J Med 375(20): 1946-1960.

Ustekinumab Induction Therapy for Treatment Refractory Patients (UNITI-2)
20%
32% 31%
47% 40%
58%
0%
10%
20%
30%
40%
50%
60%
70%
Remission Response
Pe
rce
nt
of
Pat
ien
ts
Placebo 130 mg 6 mg/kg
Feagan, B. G., et al. (2016). N Engl J Med 375(20): 1946-1960.

Clinical Remission at Week 44 after Treatment with Ustekinumab (IM-UNITI)
26%
44% 39%
57%
41%
63%
0%
10%
20%
30%
40%
50%
60%
70%
Remission (UNITI-1) Remission (UNITI-2)
Pe
rce
nt
of
Pat
ien
ts
Placebo 90 q 12 90 q 8
Feagan, B. G., et al. (2016). N Engl J Med 375(20): 1946-1960.

Use of Therapeutic Drug Levels to Guide Changes in Therapy
Response to Test
Clinical Response
P value
Detectable HACA
Increase IFX 17% P<0.004
Change Anti-TNF
92%
Subtherapeutic concentration
Increase IFX 86% P<0.016
Change Anti-TNF
33%
Afif, W., et al. (2010). Am J Gastroenterol 105(5): 1133-1139.

IFX Dosed Based on TDM vs. Clinically Based Dosing of IFX: TAXIT
66 69
0
10
20
30
40
50
60
70
80
90
100
Pe
rce
nt
of
Pat
ien
ts
Clinical and biological remission at one year
CB
LB
N=111/126 N=115/126
Vande Casteele, N., et al. (2015). Gastroenterology 148(7): 1320-1329 e1323.
29% of patients had an IFX level below 3 mcg/ml at baseline; remission rate increased from 65 to 88% (p=0.020) after one time dose optimization

IFX Reduces Post-operative Recurrence after Intestinal Resection
0
10
20
30
40
50
60
70
80
90
100
Placebo IFX
End
osc
op
ic R
ecu
rre
nce
Rat
e
Regueiro, M., et al. (2009) Gastroenterology
Endoscopic Recurrence: endoscopic scores of i2, i3, or i4

The PREVENT Trial: Trends favoring IFX were observed for fewer clinical (wk76, wk104) and endoscopic (wk76) recurrences but the primary endpoint of clinical recurrence
was not met
Prevent: Clinical Outcomes at Week 76
Regueiro, M., et al. (2016). Gastroenterology 150(7): 1568-1578

Endoscopic Surveillance After Resection is Associated with Decreased Endoscopic Recurrence
51%
33%
49%
67%
0%
10%
20%
30%
40%
50%
60%
70%
80%
Active Care (n=122) Standard Care (n=52)
Pe
rce
nt
of
Pat
ien
ts w
ith
En
do
sco
pic
Re
curr
en
ce a
t 1
8
mo
s.
Active Care (n=122) Standard Care (n=52)p=0.03
De Cruz, P., et al. (2015). Lancet 385(9976): 1406-1417.
P=0.03

AGA Clinical Pathway for CD:
Stratifying Patients by Risk for Disabling Course
Low risk Limited anatomic involvement
Age at diagnosis >30 years
Superficial ulcerations at
endoscopy
No prior surgery
Non-stricturing, non- penetrating
disease
High risk
AGA = American Gastroenterological Association. Sandborn, W.J., et al. Gastroenterology. 2014;146(1):85-95.
Extensive anatomic involvement
Deep ulcers
Age at diagnosis <30 years
Perianal disease and/or severe rectal
disease
History of prior resection
Complicated disease behavior

AGA Clinical Pathway for CD:
Initial Treatment
Low-risk patient
Ileum and/or proximal colon, none to minimal symptoms Options • Budesonide 9 mg/d with or
without AZA • Tapering course of prednisone
with or without AZA
Diffuse or left colon, none to minimal symptoms Option • Tapering course of prednisone with
or without AZA
Moderate/high-risk patient
Options • Anti-TNF monotherapy over no therapy
or thiopurine monotherapy • Anti-TNF + thiopurine over thiopurine
monotherapy or anti-TNF monotherapy • Methotrexate for patients who do not tolerate
purine analog in combination with anti-TNF
Sandborn, W.J., et al. Gastroenterology. 2014;146(1):85-95

Conclusions
• Limited role for use of antibiotics and aminosalicylates in treatment of CD
• Steroids are useful for induction of remission in CD
• Immune suppressants, particularly MTX, are effective for maintaining steroid-induced remission in CD – Little to no evidence that earlier use of these agents improves outcomes
• Anti-TNF agents are effective for treatment of luminal and perianal CD – Early combination therapy is most effective
– Outcomes can be improved with TDM
– Prevent post-operative recurrence
• Vedolizumab and ustekinumab also effective for treatment of CD – Not yet clear how to position these agents
• AGA Care Pathways available to guide selection of optimal patient for biologic treatment (not proven to improve clinical outcomes)







