Download - External Eye Diseases New
7/29/2019 External Eye Diseases New
http://slidepdf.com/reader/full/external-eye-diseases-new 1/28
NURHAIDA DJAMIL
DEPARTEMEN ILMU KESEHATAN MATA
FAKULTAS KEDOKTERANUNIVERSITAS ISLAM SUMATERA UTARA
MEDAN
2012
March 2, 2013
NURHAIDA DJAMIL, MD
EXTERNAL EYE DISEASES 1
7/29/2019 External Eye Diseases New
http://slidepdf.com/reader/full/external-eye-diseases-new 2/28
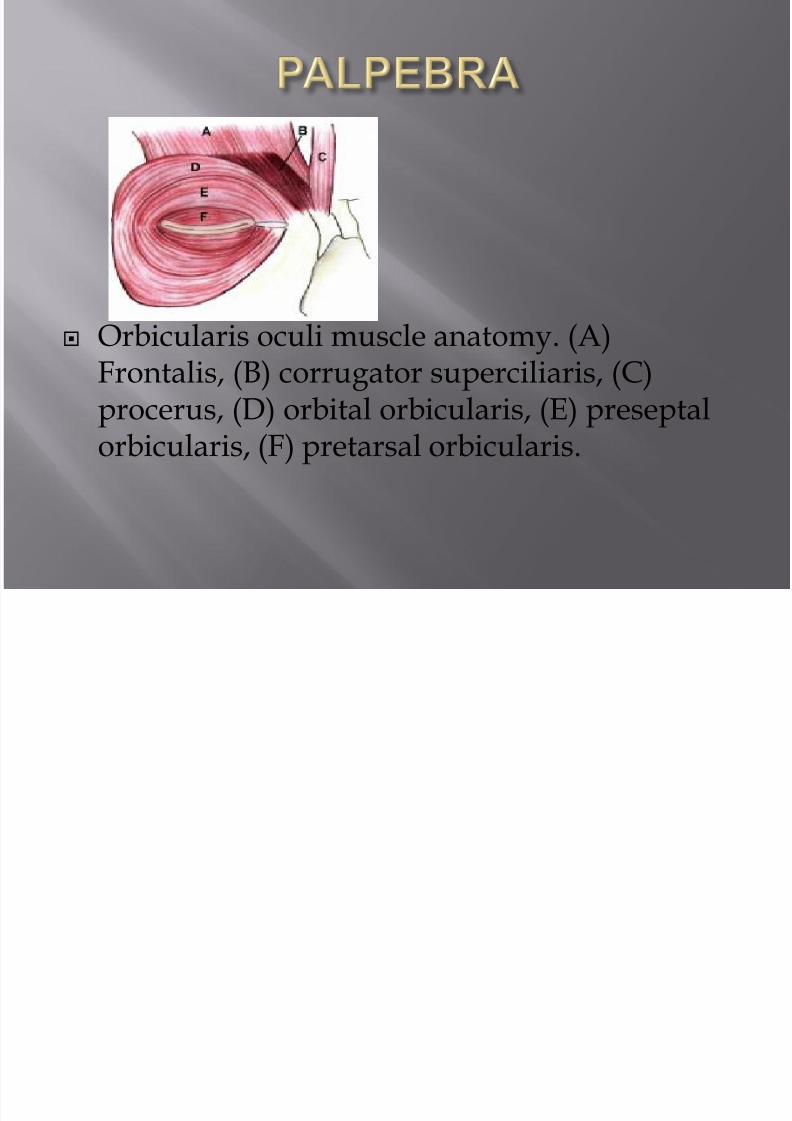
Orbicularis oculi muscle anatomy. (A)Frontalis, (B) corrugator superciliaris, (C)
procerus, (D) orbital orbicularis, (E) preseptalorbicularis, (F) pretarsal orbicularis.

7/29/2019 External Eye Diseases New
http://slidepdf.com/reader/full/external-eye-diseases-new 3/28
Hordeoulum internumIni adalah peradangan supuratif pada kelenjar meibom yang berhubungan
dengan penyumbatan saluran.
Etiology
Ini dapat terjadi sebagai infeksi staphylococcal utama kelenjar meibom atau akibatinfeksi sekunder dalam sebuah chalazion (chalazion terinfeksi).
Treatment
-Hot compresses 2-3 times
-Antibiotic eyedrops (3-4 times a day) and eye
ointment (at bed time) should be applied to
control infection.-Anti-inflammatory and analgesics relieve
pain and reduce oedema

7/29/2019 External Eye Diseases New
http://slidepdf.com/reader/full/external-eye-diseases-new 4/28
Hordeoulum eksternum
Ini adalah peradangan akut supuratif kelenjar dari Zeis atau Moll.
Treatment
-Hot compresses 2-3 times
-Antibiotic eyedrops (3-4 times a day) and eyeointment (at bed time) should be applied to
control infection.
-Anti-inflammatory and analgesics relieve
pain and reduce oedema.

7/29/2019 External Eye Diseases New
http://slidepdf.com/reader/full/external-eye-diseases-new 5/28
Chalazion
Granulomatosa kronis peradangan kelenjar meibom.
Eksisi bedah dilakukan melalui sayatan vertikal ke
dalam kelenjar tarsal
7/29/2019 External Eye Diseases New
http://slidepdf.com/reader/full/external-eye-diseases-new 6/28
Blefaritis anterior
-By chronic inflammation of bilateral palpebral
-Staphylococcus aureus, Staphylococcus epidermidis
-Symptoms: irritation, burning, itching
Blefaritis posterior palpebral inflammation due meibom glanddysfunction.
7/29/2019 External Eye Diseases New
http://slidepdf.com/reader/full/external-eye-diseases-new 7/28
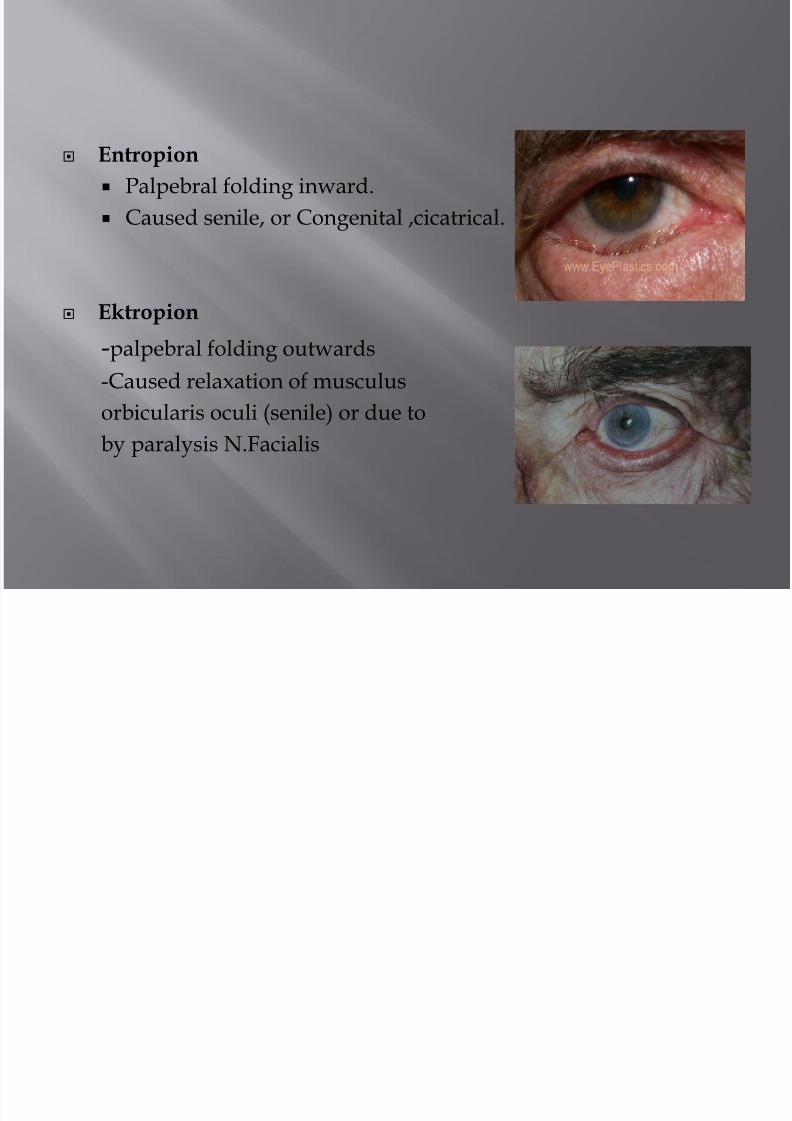
Entropion
Palpebral folding inward.
Caused senile, or Congenital ,cicatrical.
Ektropion
-palpebral folding outwards
-Caused relaxation of musculus
orbicularis oculi (senile) or due toby paralysis N.Facialis

7/29/2019 External Eye Diseases New
http://slidepdf.com/reader/full/external-eye-diseases-new 8/28
Radang konjungtiva (konjungtivitis) secara klasik didefinisikan sebagaihiperemi konjungtiva terkait dengan pelepasan yang mungkin berair,berlendir, mukopurulen atau purulen.
Etiological classification
1. Infective conjunctivitis: bacterial, chlamydial, viral,fungal, rickettsial,spirochaetal, protozoal, parasitic
2. Allergic conjunctivitis.
3. Irritative conjunctivitis.
4. Keratoconjunctivitis associated with diseases of skin and mucous
membrane.5. Traumatic conjunctivitis.
6. Keratoconjunctivitis of unknown etiology.

7/29/2019 External Eye Diseases New
http://slidepdf.com/reader/full/external-eye-diseases-new 9/28
Clinical classification
Depending upon clinical presentation, conjunctivitis can be classified as follows:
1. Acute catarrhal or mucopurulent conjunctivitis.
2. Acute purulent conjunctivitis
3. Serous conjunctivitis
4. Chronic simple conjunctivitis5. Angular conjunctivitis
6. Membranous conjunctivitis
7. Pseudomembranous conjunctivitis
8. Papillary conjunctivitis
9. Follicular conjunctivitis
10. Ophthalmia neonatorum
11. Granulomatous conjunctivitis
12. Ulcerative conjunctivitis
13. Cicatrising conjunctivitis

7/29/2019 External Eye Diseases New
http://slidepdf.com/reader/full/external-eye-diseases-new 10/28
ACUTE MUCOPURULENT CONJUNCTIVITIS
Acute mucopurulent conjunctivitis is the most common type of acutebacterial conjunctivitis. It is characterised by marked conjunctivalhyperaemia and mucopurulent discharge from the eye.
Common causative bacteria are:Staphylococcus aureus, Koch-Weeks bacillus, Pneumococcus and
Streptococcus.
Clinical course. Mucopurulent conjunctivitis
reaches its height in three to four days
Treatment
Topical antibiotics
Irrigation of conjunctival sac with sterile warm
saline once or twice a day
Dark goggles

7/29/2019 External Eye Diseases New
http://slidepdf.com/reader/full/external-eye-diseases-new 11/28
ACUTE PURULENT CONJUNCTIVITIS
The disease affects adults, predominantly males.Commonest causative organism isGonococcus; but rarely it may be Staphylococcus aureus or Pneumococcus.
Treatment
1. Systemic therapy is far more critical than the topical therapy for the infections
caused by N. gonorrhoeae and N. meningitidis. Because of the resistant strainspenicillin and tetracyline are no longer adequate as first-line treatment. Any of thefollowing regimes can be adopted :
Norfloxacin 1.2 gm orally qid for 5 days
Cefoxitim 1.0 gm or cefotaxime 500 mg. IV qid or ceftriaxone 1.0 gm IM qid, all for5 days;
2. Topical antibiotic therapy presently recommended includes ofloxacin, ciprofloxacinor tobramycin eye drops
3. Irrigation of the eyes
7/29/2019 External Eye Diseases New
http://slidepdf.com/reader/full/external-eye-diseases-new 12/28
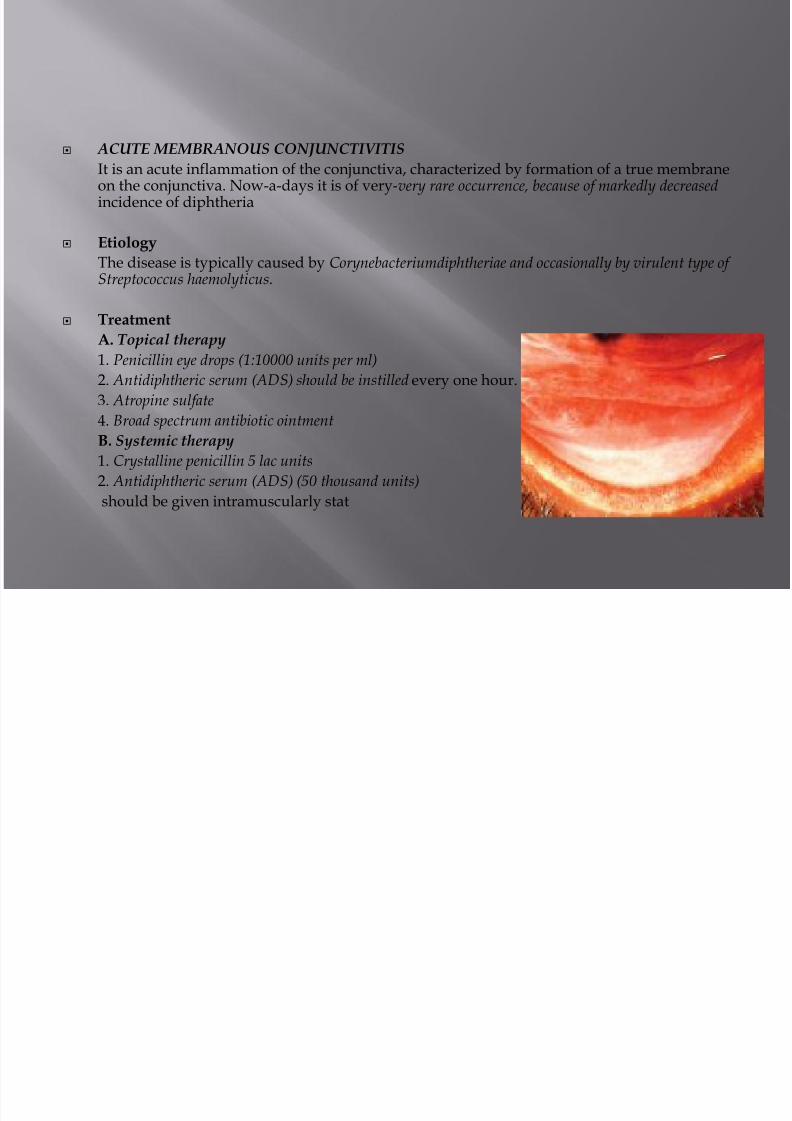
ACUTE MEMBRANOUS CONJUNCTIVITIS
It is an acute inflammation of the conjunctiva, characterized by formation of a true membraneon the conjunctiva. Now-a-days it is of very-very rare occurrence, because of markedly decreasedincidence of diphtheria
Etiology
The disease is typically caused by Corynebacteriumdiphtheriae and occasionally by virulent type of
Streptococcus haemolyticus.
Treatment
A. Topical therapy
1. Penicillin eye drops (1:10000 units per ml)
2. Antidiphtheric serum (ADS) should be instilled every one hour.
3. Atropine sulfate
4. Broad spectrum antibiotic ointment B. Systemic therapy
1. Crystalline penicillin 5 lac units
2. Antidiphtheric serum (ADS) (50 thousand units)
should be given intramuscularly stat
7/29/2019 External Eye Diseases New
http://slidepdf.com/reader/full/external-eye-diseases-new 13/28
VIRAL CONJUNCTIVITIS
Most of the viral infections tend to affect the epithelium, both of the conjunctivaand corne.
ACUTE SEROUS CONJUNCTIVITIS
Etiology. It is typically caused by a mild grade viralinfection which does not give rise to follicular response.
Clinical features. Acute serous conjunctivitis is
characterised by a minimal degree of congestion, a watery discharge and a boggyswelling of the conjunctival mucosa.
Treatment.
Usually it is self-limiting and does not need any treatment. But to avoid secondarybacterial infection, broad spectrum antibiotic eye drops may be used threetimes a day for about 7 days.

7/29/2019 External Eye Diseases New
http://slidepdf.com/reader/full/external-eye-diseases-new 14/28
Acute herpetic conjunctivitis
Acute herpetic follicular conjunctivitis is always anaccompaniment of the 'primary herpetic infection', which mainlyoccurs in small children and in adolescents.
Etiology.The disease is commonly caused by herpes simplex virus type 1and spreads by kissing or other close personal contacts. HSV type2 associated with genital infections, may also involve the eyes inadults as well as children, though rarely.

7/29/2019 External Eye Diseases New
http://slidepdf.com/reader/full/external-eye-diseases-new 15/28
VERNAL KERATOCONJUNCTIVITIS (VKC)
It is a recurrent, bilateral, interstitial, self-limiting,
allergic inflammation of the conjunctiva having
a periodic seasonal incidence.
EtiologyIt is considered a hypersensitivity reaction to some
exogenous allergen, such as grass pollens
Treatment
1. Topical steroids
2. Mast cell stabilizers such as sodium cromoglycate(2%) drops 4-5 times
3.Topical antihistaminics are also effective.
7/29/2019 External Eye Diseases New
http://slidepdf.com/reader/full/external-eye-diseases-new 16/28
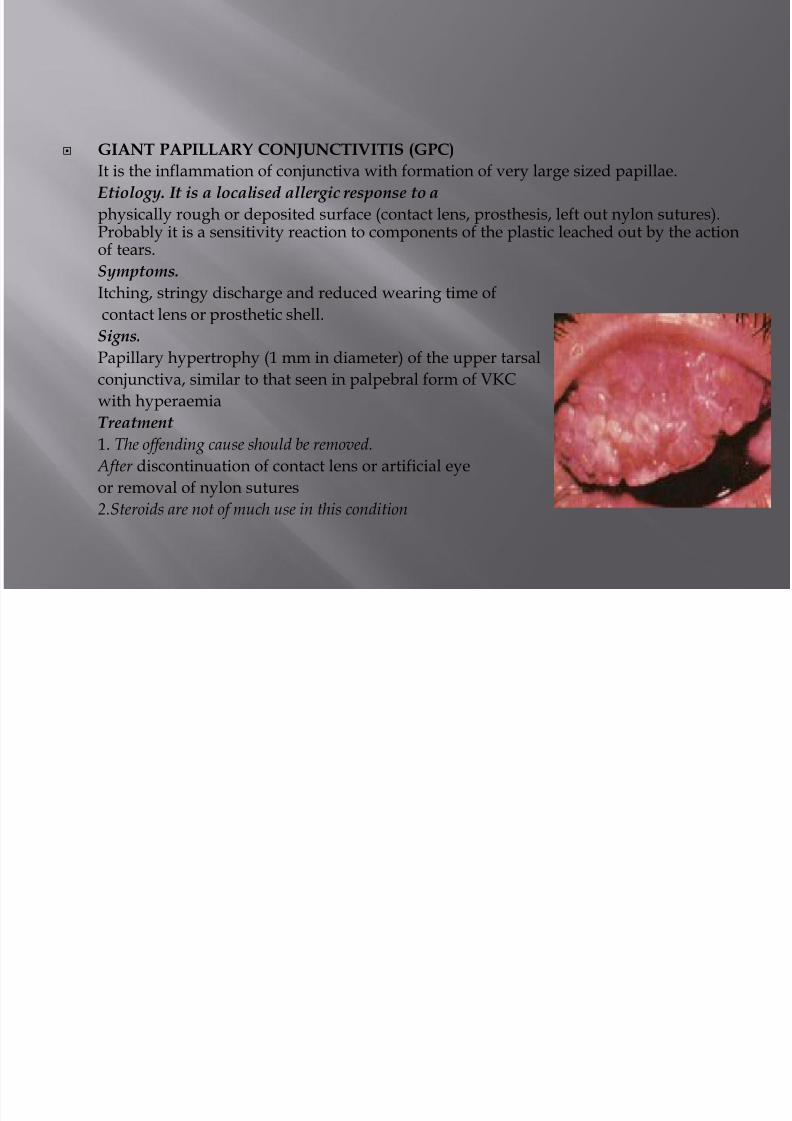
GIANT PAPILLARY CONJUNCTIVITIS (GPC)
It is the inflammation of conjunctiva with formation of very large sized papillae.
Etiology. It is a localised allergic response to a
physically rough or deposited surface (contact lens, prosthesis, left out nylon sutures).Probably it is a sensitivity reaction to components of the plastic leached out by the actionof tears.
Symptoms.Itching, stringy discharge and reduced wearing time of
contact lens or prosthetic shell.
Signs.
Papillary hypertrophy (1 mm in diameter) of the upper tarsal
conjunctiva, similar to that seen in palpebral form of VKC
with hyperaemia
Treatment
1. The offending cause should be removed.
After discontinuation of contact lens or artificial eye
or removal of nylon sutures
2.Steroids are not of much use in this condition
7/29/2019 External Eye Diseases New
http://slidepdf.com/reader/full/external-eye-diseases-new 17/28
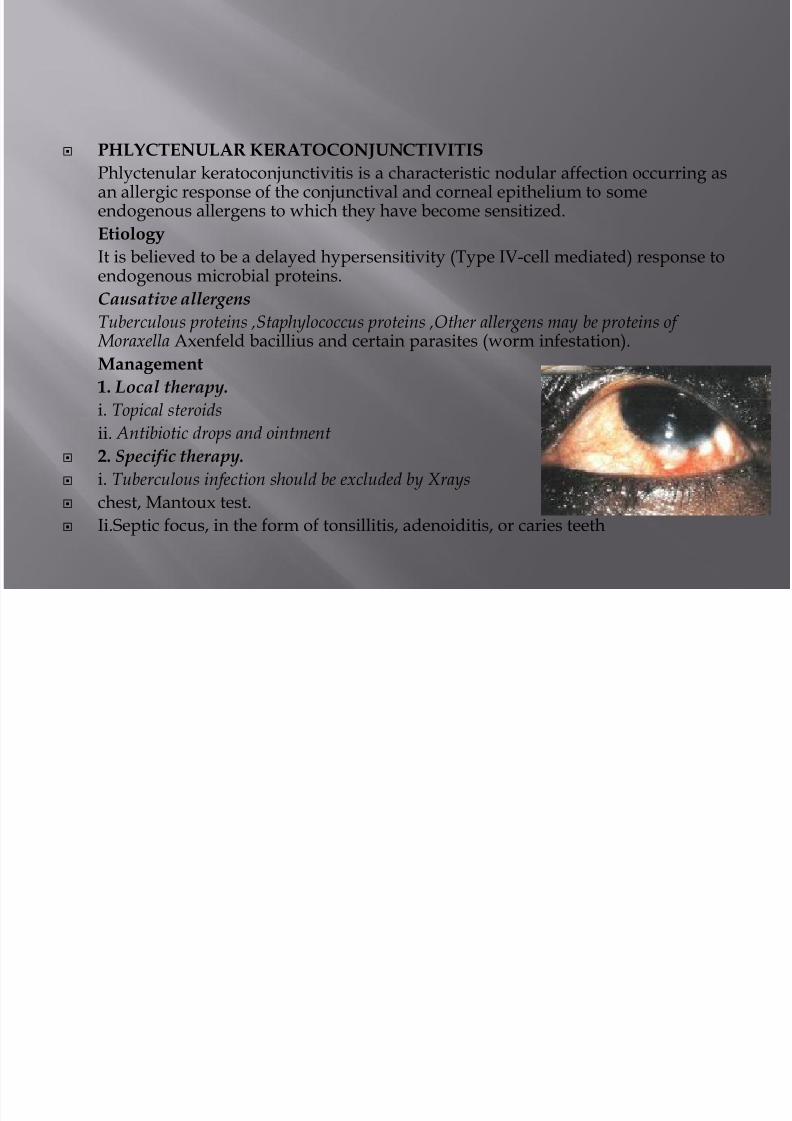
PHLYCTENULAR KERATOCONJUNCTIVITIS
Phlyctenular keratoconjunctivitis is a characteristic nodular affection occurring asan allergic response of the conjunctival and corneal epithelium to someendogenous allergens to which they have become sensitized.
Etiology
It is believed to be a delayed hypersensitivity (Type IV-cell mediated) response to
endogenous microbial proteins.Causative allergens
Tuberculous proteins ,Staphylococcus proteins ,Other allergens may be proteins of Moraxella Axenfeld bacillius and certain parasites (worm infestation).
Management
1. Local therapy.
i. Topical steroidsii. Antibiotic drops and ointment
2. Specific therapy.
i. Tuberculous infection should be excluded by Xrays
chest, Mantoux test.
Ii.Septic focus, in the form of tonsillitis, adenoiditis, or caries teeth

7/29/2019 External Eye Diseases New
http://slidepdf.com/reader/full/external-eye-diseases-new 18/28
PTERYGIUMPterygium (L. Pterygion = a wing) is a wing-shapedfold of conjunctiva encroaching upon the cornea fromeither side within the interpalpebral fissure.
Etiology.
Etiology of pterygium is not definitelyknown. But the disease is more common in people
living in hot climates
Pathology. Pathologically pterygium is a
degenerative and hyperplastic condition of
conjunctiva. The subconjunctival tissue undergoes
elastotic degeneration and proliferates as
vascularised granulation tissue under the epithelium,
which ultimately encroaches the cornea. The cornealepithelium, Bowman's layer and superficial stroma are
destroyed
Treatment.
Surgical excision is the only satisfactory treatment
7/29/2019 External Eye Diseases New
http://slidepdf.com/reader/full/external-eye-diseases-new 19/28
Etiological classification 1. Infective keratitis
(a) Bacterial
(b) Viral
(c) Fungal
(d) Chlamydial
(e) Protozoal
(f) Spirochaetal
2. Allergic keratitis
(a) Phlyctenular keratitis
(b) Vernal keratitis
(c) Atopic keratitis
3. Trophic keratitis
(a) Exposure keratitis
(b) Neuroparalytic keratitis
(c) Keratomalacia
(d) Atheromatous ulcer

7/29/2019 External Eye Diseases New
http://slidepdf.com/reader/full/external-eye-diseases-new 20/28
4. Keratitis associated with diseases of skin and
mucous membrane.
5. Keratitis associated with systemic collagen
vascular disorders.
6. Traumatic keratitis, which may be due to
mechanical trauma, chemical trauma, thermal
burns, radiations
7. Idiopathic keratitis e.g.,
(a) Mooren's corneal ulcer
(b) Superior limbic keratoconjunctivitis(c) Superficial punctate keratitis of Thygeson
7/29/2019 External Eye Diseases New
http://slidepdf.com/reader/full/external-eye-diseases-new 21/28
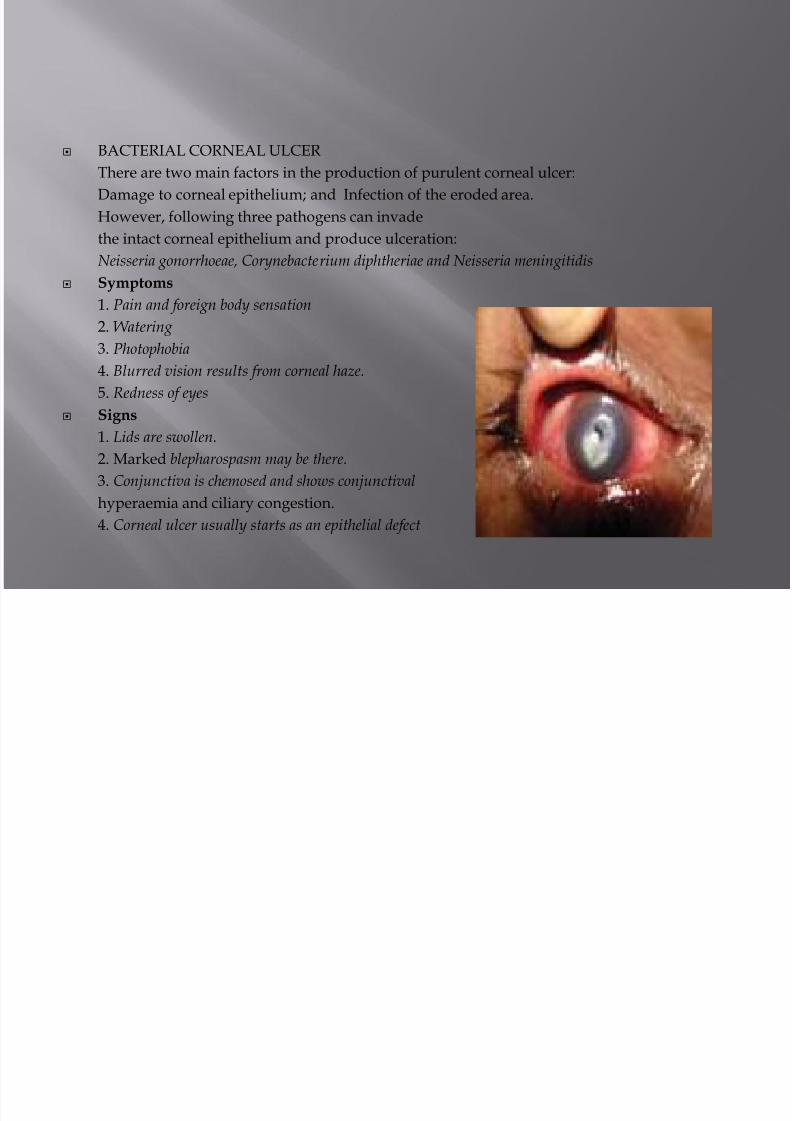
BACTERIAL CORNEAL ULCER
There are two main factors in the production of purulent corneal ulcer:
Damage to corneal epithelium; and Infection of the eroded area.
However, following three pathogens can invade
the intact corneal epithelium and produce ulceration:
Neisseria gonorrhoeae, Corynebacterium diphtheriae and Neisseria meningitidis
Symptoms
1. Pain and foreign body sensation
2. Watering
3. Photophobia
4. Blurred vision results from corneal haze.
5. Redness of eyes
Signs1. Lids are swollen.
2. Marked blepharospasm may be there.
3. Conjunctiva is chemosed and shows conjunctival
hyperaemia and ciliary congestion.
4. Corneal ulcer usually starts as an epithelial defect

7/29/2019 External Eye Diseases New
http://slidepdf.com/reader/full/external-eye-diseases-new 22/28
Treatment
Ciprofloxacin (0.3%) eye drops, or
Ofloxacin (0.3%) eye drops, or
Gatifloxacin (0.3%) eye drops

7/29/2019 External Eye Diseases New
http://slidepdf.com/reader/full/external-eye-diseases-new 23/28
HERPES SIMPLEX KERATITIS
Mode of Infection
HSV-1 infection. It is acquired by kissing or
coming in close contact with a patient suffering from herpes labialis.
HSV-II infection. It is transmitted to eyes of
neonates through infected genitalia of the mother.
7/29/2019 External Eye Diseases New
http://slidepdf.com/reader/full/external-eye-diseases-new 24/28
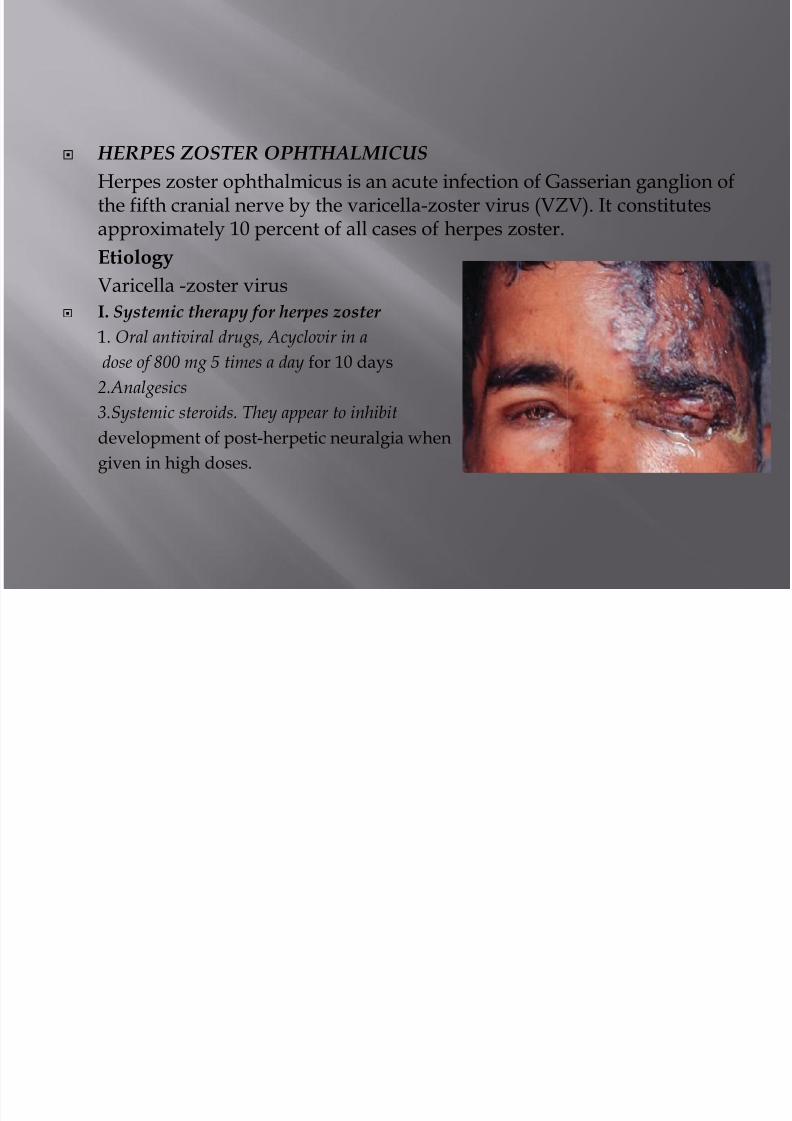
HERPES ZOSTER OPHTHALMICUS
Herpes zoster ophthalmicus is an acute infection of Gasserian ganglion ofthe fifth cranial nerve by the varicella-zoster virus (VZV). It constitutesapproximately 10 percent of all cases of herpes zoster.
Etiology
Varicella -zoster virus I. Systemic therapy for herpes zoster
1. Oral antiviral drugs, Acyclovir in a
dose of 800 mg 5 times a day for 10 days
2.Analgesics
3.Systemic steroids. They appear to inhibitdevelopment of post-herpetic neuralgia when
given in high doses.

7/29/2019 External Eye Diseases New
http://slidepdf.com/reader/full/external-eye-diseases-new 25/28
ALLERGIC KERATITIS
1. Phlyctenular keratitis
2. Vernal keratitis
3. Atopic keratitis

7/29/2019 External Eye Diseases New
http://slidepdf.com/reader/full/external-eye-diseases-new 26/28
MYCOTIC CORNEAL ULCER
The incidence of suppurative corneal ulcers caused
by fungi has increased in the recent years due to
injudicious use of antibiotics and steroids.
Etiology
corneal infections are :i. Filamentous fungi e.g., Aspergillus, Fusarium,
Alternaria, Cephalosporium, Curvularia and
Penicillium.
ii. Yeasts e.g., Candida and Cryptococcus.
(The fungi more commonly responsible for mycotic
corneal ulcers are Aspergillus (most common),
Candida and Fusarium).
7/29/2019 External Eye Diseases New
http://slidepdf.com/reader/full/external-eye-diseases-new 27/28
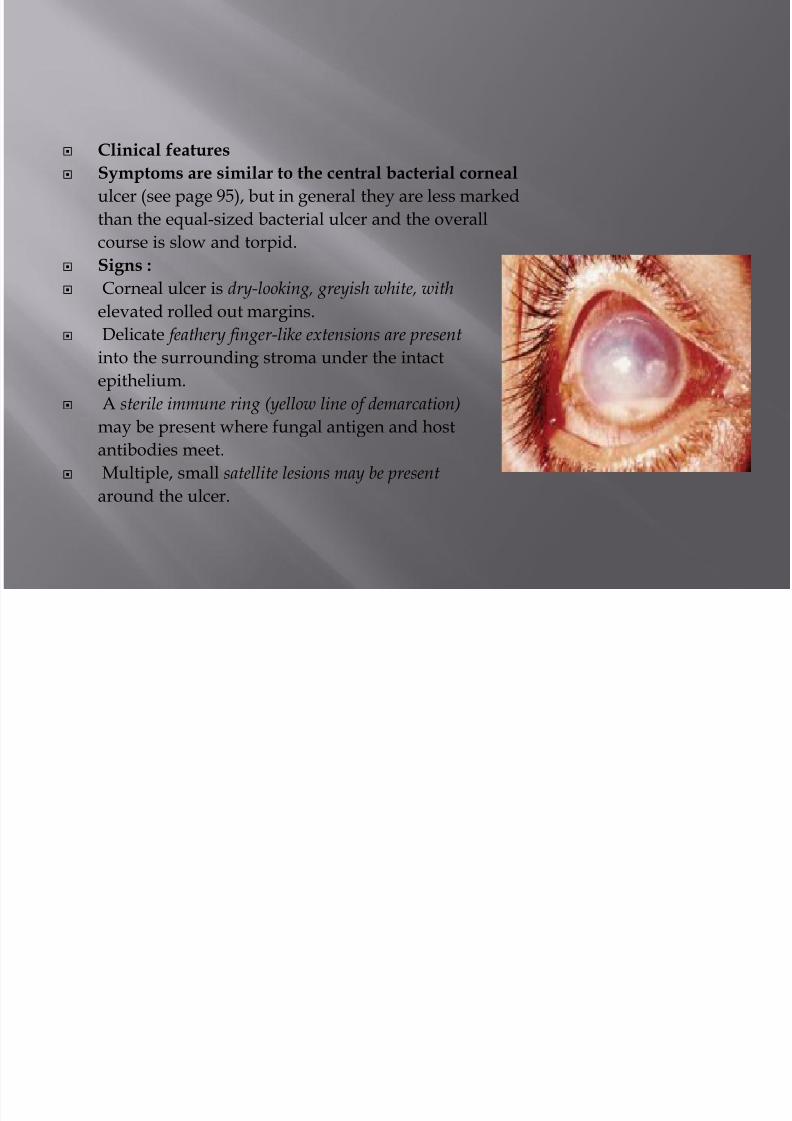
Clinical features
Symptoms are similar to the central bacterial corneal
ulcer (see page 95), but in general they are less marked
than the equal-sized bacterial ulcer and the overall
course is slow and torpid.
Signs :
Corneal ulcer is dry-looking, greyish white, with
elevated rolled out margins.
Delicate feathery finger-like extensions are present
into the surrounding stroma under the intact
epithelium.
A sterile immune ring (yellow line of demarcation)
may be present where fungal antigen and host
antibodies meet.
Multiple, small satellite lesions may be present
around the ulcer.

7/29/2019 External Eye Diseases New
http://slidepdf.com/reader/full/external-eye-diseases-new 28/28
Treatment
I. Specific treatment includes antifungal drugs:
1. Topical antifungal
Natamycin (5%) eye drops,Fluconazol (0.2%) eye drops,Nystatin (3.5%) eyeointment.
2. Systemic antifungal drugs may be required for
severe cases of fungal keratitis. Tablet
fluconazole or ketoconazole may be given for
2-3 weeks.
II. Non specific treatment. Non-specific treatment
and general measures are similar to that of bacterial
corneal ulcer (see page 98).
III. Therapeutic penetrating keratoplasty may be
required for unresponsive cases







