
Geographic Adjusters in Medicare
Payment
Friday September 17, 2010
Douglas J. Reding, MD, MPH, FACP
Vice President & Chairperson
of Government Relations
Overview
The Medicare Payment Dilemma
Medicare Payment Inequities
Medicare Payment Adequacy
Geographic Adjustment of Practice ExpenseGeographic Adjustment of Practice Expense
The Physician Work GPCI
Forward Looking Payment System

Overview
CMS cost measurement reflects profound variation in supply-sensitive service utilization
CMS measurement tools - geographic adjustment
Obsolete
Limited in scopeLimited in scope
Imprecise
Not consistent with future health reform
CMS measurement tools must be recalibrated to future-proof Medicare reimbursement

Marshfield Clinic
at a Glance
Formed 1916
Physician led – 501(c)3
766 physicians in 86 specialties
6,450 employees
56 regional sites
374,468 unique patients/year
76K Medicare, 58K Medicaid
3,767,3003 patient encounters/yr3,767,3003 patient encounters/yr
Over $1 billion in annual revenue
Security Health Plan (170,000 Member HMO)
Division of Laboratory Medicine
Education Foundation
Research Foundation
Family Health Center (76K patients, 443K encounters annually)
Seven Dental Clinics in underserved areas
An Academic Campus of UW School of Medicine and Public Health
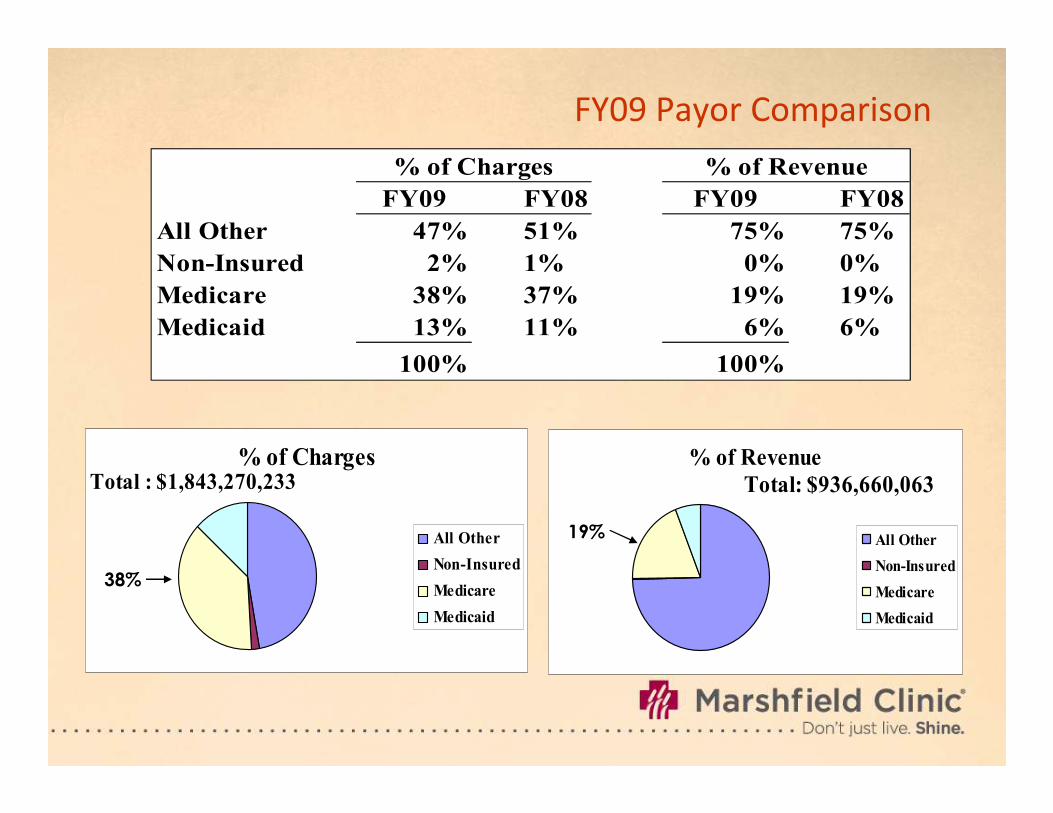
FY09 Payor Comparison
FY09 FY08 FY09 FY08
All Other 47% 51% 75% 75%
Non-Insured 2% 1% 0% 0%
Medicare 38% 37% 19% 19%
Medicaid 13% 11% 6% 6%
100% 100%
% of Revenue% of Charges
% of Charges
All Other
Non-Insured
Medicare
Medicaid
Total : $1,843,270,233% of Revenue
All Other
Non-Insured
Medicare
Medicaid
Total: $936,660,063
38%
19%

Concentration of Total Annual Medicare Expenditures
Among Beneficiaries, 2001
Percent
50
60
70
80
90
100
18.4
43.1
5
5
15
25
Beneficiar ies Expenditures
0
10
20
30
40
3.8
11.2
23.550
Source: CBO based on data from CMS.


Physician Payment
RBRVS FY 2006
●Physician Work (52.5% of fee)
●Practice Expense (43.7% of fee)
●Professional Liability Insurance (3.9% of fee)
Geographic Adjustment – 89 LocalitiesGeographic Adjustment – 89 Localities
●56 < 1.00 for work =1.0 Range 1.0– 1.079
●49 < 1.00 for PE Range 0.705 – 1.501
●62 < 1.00 for PLI Range 0.261 – 2.744
Sustainable Growth Rate (SGR)

Practice Expense Study
Composition of PE
Employee wages --Measured by proxy
Rents – Measured by Proxy
(HUD 2 BR residential Section A Housing)(HUD 2 BR residential Section A Housing)
Medical Equipment and Supplies – No geographic adjustment, purchased in national market

PE Employee Wage Proxies
Median hourly earnings of:
●Clerical Workers
●Registered Nurses
●Licensed practical nurses
●Health technologists and technicians●Health technologists and technicians
“four labor categories most commonly present in a physician’s (singular) private practice” – circa 1980

Marshfield Clinic Employee 2004 Wage Summary
Total Wages all 5138 Employees $177,347,115
●Average wage of all employees $34,516/yr
●Average wage of 3351 Proxy employees $27,262/yr$27,262/yr
●Average wage of all other 1787 employees $48,399/yr
●Wages not represented by proxies $86,490,374/$177,347,115 = 48.7%

Marshfield Clinic Employee 2009 Wage Summary
Total Wages all 4,850 Employees $235,917,877
●Average wage of all employees $48,644/yr
●Average wage of 2,563 Proxy employees $40,089/yr$40,089/yr
●Average wage of all other 2,287 employees $58,228/yr
●Wages not represented by proxies $133,191,608/$235,917,877 = 56.5%

Marshfield Clinic Employees: Distribution of Employees by Occupational
Classes, 2004 and 2009
44.3%
31.8%
34.8%
47.2%
20%
30%
40%
50%
8.5%8.7%
2.3% 1.9%
10.2% 10.4%
0%
10%
RNs LPNs Technologists Clerical Other (Non-Proxy)
2004 Employees 2009 Employees
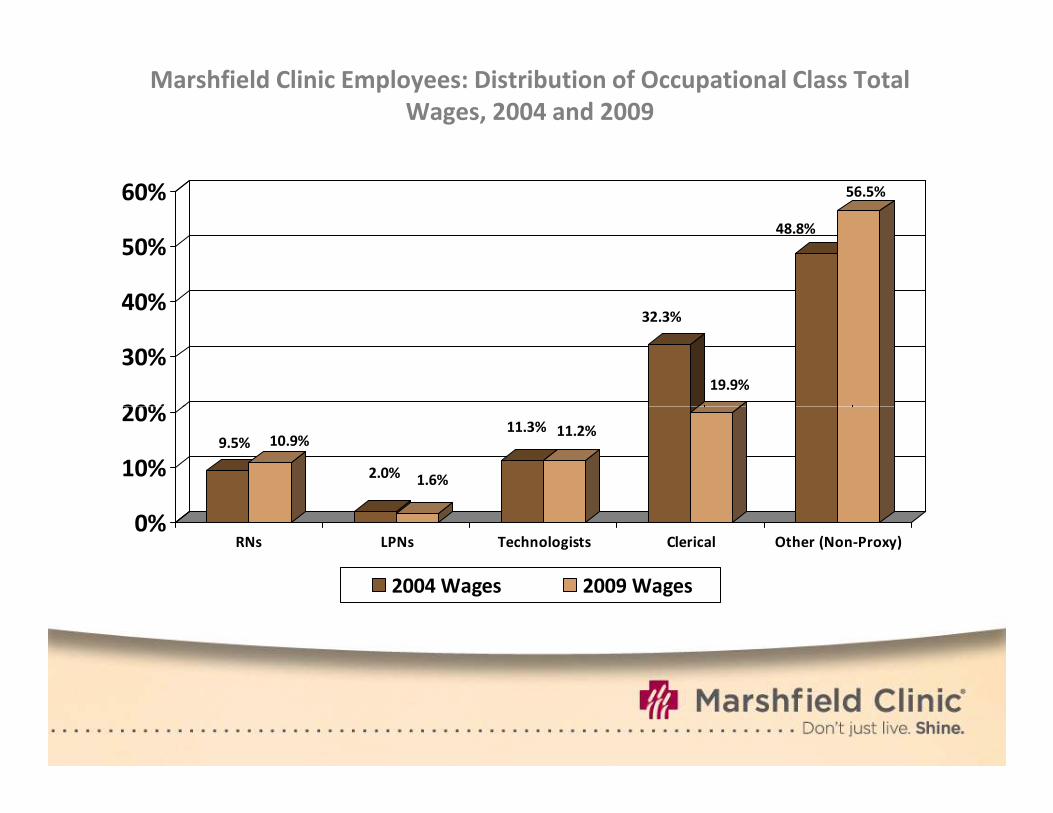
Marshfield Clinic Employees: Distribution of Occupational Class Total
Wages, 2004 and 2009
32.3%
19.9%
48.8%
56.5%
20%
30%
40%
50%
60%
9.5% 10.9%
2.0%1.6%
11.3% 11.2%
0%
10%
20%
RNs LPNs Technologists Clerical Other (Non-Proxy)
2004 Wages 2009 Wages

Practice Expense Summary
Practice organization is dynamic
● Changing non-physician labor structure is leading indicator
● Administered payment methods should reflect major changes in
practice organization and related costs
● Practice expense adjustments should reflect valid and reliable
methods
● Labor share of practice expense should reflect practice realities● Labor share of practice expense should reflect practice realities
● Increasing importance of non-traditional occupational classes
● Increasing importance of IT-related costs and therefore increasing
need to reflect these real costs either through labor-related
adjustments or alternative methods

Physician Work
• CMS defines physician work as the amount of time,
skill, and intensity a physician puts into a patient visit.
• Current payment methods adjust physician work for
local “costs” as reflected by earnings of selected non-
physician professionals. The adjustment is 25% of
these “costs.”these “costs.”
• The work adjustments for Wisconsin do not align well with market realities as reflected in our practice and in a recent study, which indicated wage premiums were evident for important physician specialties in Wisconsin.

Physician Compensation per RVU
Specialty Mean Median WI-Median Ratio WI/US
Cardiology $53.85 $51.68 $66.41 128.1
Fam Prac $42.30 $41.31 $47.01 113.8
Gastro $50.90 $46.83 $64.10 136.9
Int Med $44.36 $42.12 $48.33 114.7
OB/GYN $41.93 $40.39 $49.23 121.9
Ortho Surg $53.76 $51.71 $70.67 136.7Ortho Surg $53.76 $51.71 $70.67 136.7
Radiology $50.22 $49.51 $84.09 169.8
Surgery $44.70 $43.05 $51.47 119.6
Source: The Physician Marketplace – A Comparison of Central USA Metropolitan Areas. Merton D. Finkler Ph.D., Greater Milwaukee Business Foundation On Health, Inc., September 21, 2006

Physician Work Summary
•There is no difference between the work of physicians in different locations regardless of where the work occurs.
•Physician work should not be geographically adjusted – William Hsaio, MD, and PPRC.
• If physician work is adjusted it should reflect as directly as possible the prevailing supply and demand for physician services. Third party data are available for such adjustments.





![ADJUSTERS (N20, N26) [REP-REP-RAF1011N20-1136046] …...ADJUSTERS (N20, N26) [REP-REP-RAF1011N20-1136046] Removing and installing/r eplacing intake and exhaust camshaft adjusters (N20,](https://cdn.vdocument.in/doc/165x107/60cdcc364bfec46b2f6aa1ee/adjusters-n20-n26-rep-rep-raf1011n20-1136046-adjusters-n20-n26-rep-rep-raf1011n20-1136046.jpg)

