Governance of purchasing arrangements in Estonia
Triin Habicht Head of Department of Health System Development
Ministry of Social Affairs
OECD Joint Network on Fiscal Sustainability of Health Expenditure
4-5.02.2016 Paris

Public financial flows in health sector (1)
Source: National Health Accounts 2014
87% of total public funds is administered
by EHIF
State budget
MoSA
National Institute for
Health Development
Health Board
EHIF
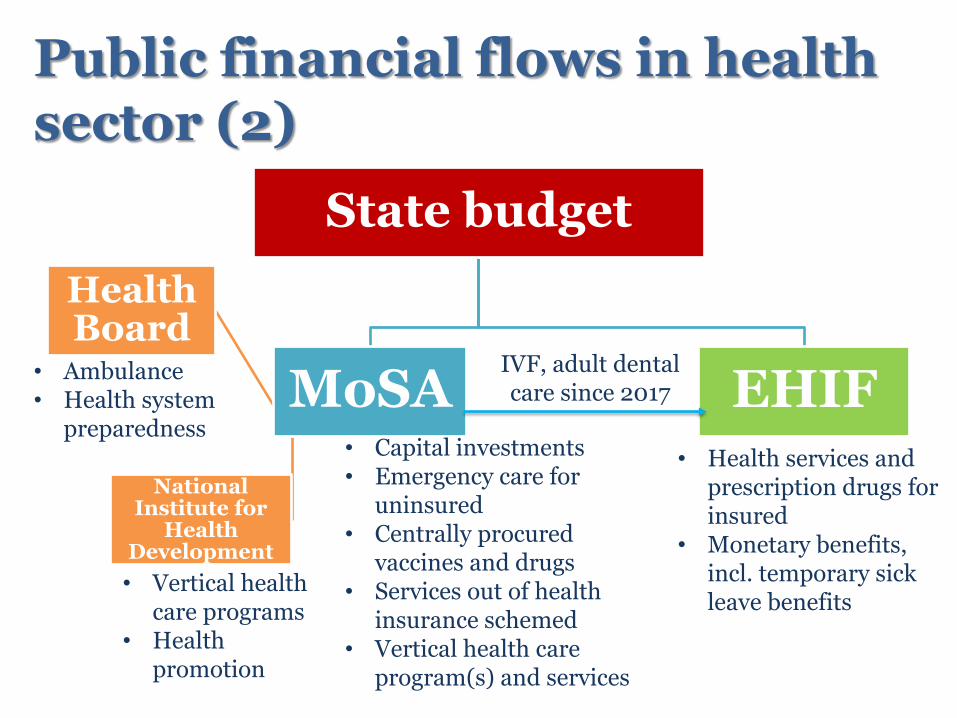
Public financial flows in health sector (2)
• Vertical health care programs
• Health promotion
• Ambulance • Health system
preparedness • Capital investments • Emergency care for
uninsured • Centrally procured
vaccines and drugs • Services out of health
insurance schemed • Vertical health care
program(s) and services
IVF, adult dental care since 2017
• Health services and prescription drugs for insured
• Monetary benefits, incl. temporary sick leave benefits

4
Evolution of the organization of health insurance
First sickness funds in 1913
Re-established regional non-competing sickness funds in 1991/92 (22 in total)
Central sickness fund to coordinate regional funds in 1994
Estonian Health Insurance Fund in 2001, Currently with 4 regional departments
5
Legal status of the EHIF
• EHIF operates as public independent legal entity – Founded in the public interest by separate act – General public service regulation does not apply to
EHIF, e.g. applies private sector labor codes
• EHIF is fully liable for its obligations with all its assets
• Tripartite supervisory board with 15 members
– 5 state (incl. Minister of Health and Labor, Minister of Finance), 5 employer and 5 beneficiaries representatives

Health Insurance Fund revenues, expenditures and reserves
Source: EHIF, www.haigekassa.ee
The puzzle of public health funds (1)
• Health insurance revenue base is explicitly determined which gives incentive to optimize within the budget and to set explicit limits on the health insurance obligations
• Additional earmarked funds to health insurance to serve political priorities (e.g. IVF, dental care program)
– Broadening revenue base has been an issue since 2005 but no changes
• Changing role of health insurance reserves
The puzzle of public health funds (2)
• Other allocations from the state budget have to compete with priorities within MoSA as well as at Government level
– Explicit areas as ambulance and emergency care for uninsured are easy to protect
– Vertical public(?) health programs are easy to confuse with health insurance
– „Fixing the problems“ money
• External sources (e.g. EU funds) still play important role
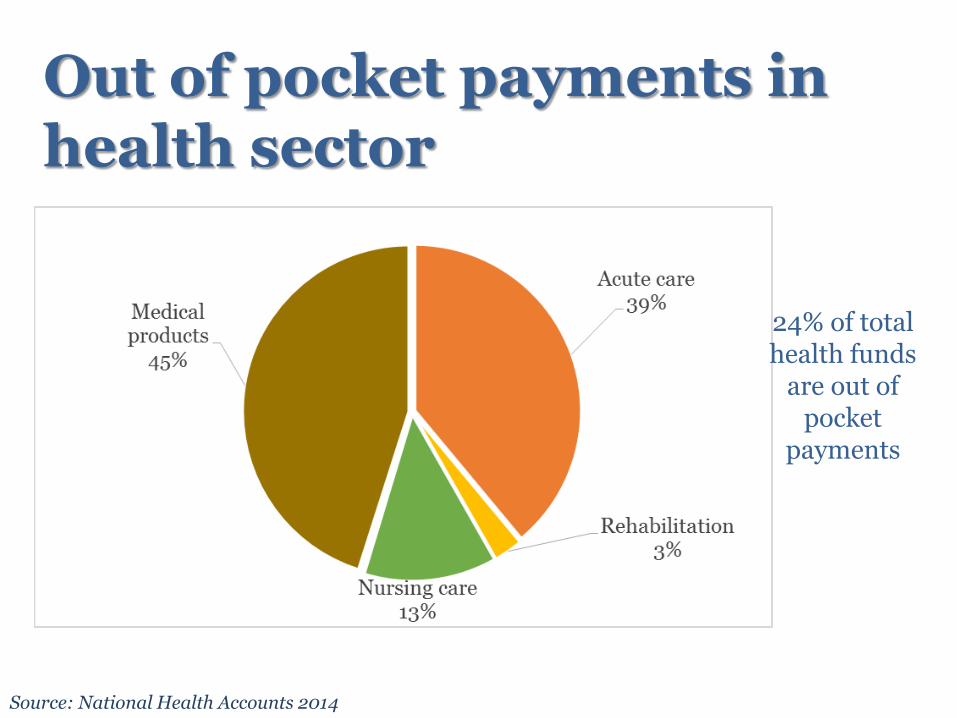
Out of pocket payments in health sector
Source: National Health Accounts 2014
24% of total health funds
are out of pocket
payments
Summing up... • Majority of public funds is pooled to the EHIF
– Stable health insurance system and strong institutional design
• Still, existing fragmentation may lead to inefficiencies
− Differences in rules and power of purchasing
− Incentives to focus on „your own piece“ but not patient needs
− Not always clear who is responsible for what
• Program based funding rises the question of ownership and sustainability
• Easy to claim that there are unfunded mandates (....but this is the only way to increase the health sector funds)
• Who governs private out of pocket expenditures?

THANK YOU FOR YOUR ATTENTION!







