
DDiirreeccttoorraattee ooff NNaattiioonnaall VVeeccttoorr BBoorrnnee DDiisseeaassee CCoonnttrrooll PPrrooggrraammmmee ((DDiirreeccttoorraattee GG..HH..SS..,, MMOOHH && FFWW,, GGoovveerrnnmmeenntt ooff IInnddiiaa))
2222,, SShhaammnnaatthh MMaarrgg,, DDeellhhii--111100 005544
22000099
Guidelines on ELIMINATION OF LYMPHATIC FILARIASIS
India
DDiissaabbiilliittyy aalllleevviiaattiioonn tthhrroouugghh hhoommee bbaasseedd mmaannaaggeemmeenntt ooff
llyymmpphhooeeddeemmaa aanndd hhoossppiittaall bbaasseeddhhyyddrroocceelleeccttoommyy
IInntteerrrruuppttiioonn ooff TTrraannssmmiissssiioonn tthhrroouugghh MMaassss DDrruugg AAddmmiinniissttrraattiioonn
wwiitthh DDEECC aanndd aallbbeennddaazzoollee
DEC
Albendazole

i
C O N T E N T S
Foreword iv
Message v
Preface
List of Acronyms
Contributors
vi
vii
viii
Chapter 1: Filariasis Control in India & Its Elimination
1 Introduction 1
2 Causative Organisms 1
3 Life Cycle of the parasite 1
4 Wolbachia Endosymbiont 2
5 Clinical Spectrum 2
6 Current status and distribution 6
7 Control of LF in India 7
8 LF Elimination strategy 7
Chapter 2: Mapping And Disease Burden Estimation
1 Mapping 9
2 Non endemic districts Organisms 10
3 Mapping based on available records for Filariasis 10
4 Disease burden estimation 12
Annex-2.1 Village-wise and Subcentre-wise compilation forms 13
Annex- 2.2 Form for interview of key informants 16
Annex- 2.3 LF patients identification card and questionnaire for line listing 17
Chapter 3: Implementation of Mass Drug Administration
1 Introduction to MDA as LF Elimination strategy 19
2 Approaches for drug administration 19
3 Dosage schedule of drugs 20
4 Preparatory activities 20
5 Pre-MDA activities at different levels 20
6 Activities during MDA 24

ii
7 Post –MDA activities 26
8 Monitoring and Evaluation 27
9 Proforma for maintaining registers at different levels 29
10 Formats for reporting at different levels 32
Annex- 3.1 Roadmap of MDA 33
Annex- 3.2 Table 1 to 13 34
Annex- 3.3 Terms of reference for State Task Force for Elimination of Lymphatic Filariasis 40
Annex- 3.4 Terms of reference for State Technical Advisory Committee for Elimination of
Lymphatic Filariasis
44
Chapter 4: Implementation of Disability Prevention & Management
1 Lymphoedema Management 46
2 Washing 47
3 Prevention & cure of entry lesions 47
4 Elevation 48
5 Exercise 48
6 Wearing proper footwear 48
7 Management of acute attack 49
8 Surgical management of Hydrocele due to Lymphatic Filariasis 51
Annex- 4.1 District wise information of state for surgical management of hydrocele cases
due to lymphatic Filariasis
55
Chapter 5: Behaviour Change Communication for Social Mobilisation for ELF
1 Need for Behaviour Change Communication (BCC) 56
2 BCC Campaign goal 56
3 BCC Objectives 56
4 BCC Strategy 57
5 Advocacy 60
6 Inter-sectoral convergence 60
7 Communication 60
8 IEC Prototypes 64
Chapter 6: Monitoring & Evaluation of Impact of Programme
1 Approach 69
2 Selection of sites (sentinel and spot check) 70
3 Collection of blood smears for microfilariaemia 71

iii
4 Entomological data collection 73
5 Important questions for monitoring & evaluation 74
Annex. 6.1 Filaria Night blood survey form 79
Chapter 7: Independent Assessment of MDA Implementation
1 Introduction 80
2 Objectives 80
3 Constitution of assessment teams 80
4 Assessment of activities 80
5 Selection process in the districts 81
6 Components to be assessed 81
7 Financial aspects 84
Annex. 7.1 Proforma for assessment of MDA compliance 85
Annex. 7.2 Compliance /Side Reaction survey 86
Annex. 7.3 Awareness and acceptance Questionnaire 87
Chapter 8: Roles & Responsibilities of Officers & staff for MDA Campaign
1 Responsibilities of National Programme Headquarters 88
2 Responsibilities of State Programme Headquarters 89
3 Responsibilities of District Co-ordination Committee 91
4 Responsibilities of District Vector Borne Diseases Officer 92
5 Responsibilities of PHC In-charge MO/Municipal Health Officer 93
6 Responsibilities of Supervisory Paramedical staff/Health workers 96
7 Responsibilities of drug administrator 97
Appendix-1 List of filaria endemic districts 99




vii
LIST OF ACRONYMS
Bm Brugia malayi
Bt Brugia timori
BCC Behaviour Change Communication
COMBI Communication for Behavioural Impact
DA Drug Administrator
DCC District Co-ordination Committee
DDC Drug Distribution Centre
DEC Diethylcarbamazine
Dte. Directorate
DVBDCO District Vector Borne Diseases Control Officer
DVBDCS District Vector Borne Diseases Control Society
Dy. Deputy
ELF Elimination of Lymphatic Filariasis
Ent. Entomology
FTD Fever Treatment Depot
GOI Government of India
ICMR Indian Council of Medical Research
IEC Information, Education and Communication
IU Implementation Unit
LF Lymphatic Filariasis
Kg Kilogram
KAP Knowledge, Attitude and Practice
Mf Microfilaria
M&F Malaria & Filaria
MDA Mass Drug Administration
Mg Milligram
MO Medical Officer
MOH&FW Ministry of Health & Family Welfare
MM Morbidity Management
NAMP National Anti Malaria Programme
NFCP National Filaria Control Programme
NFD National Filaria Day
NGO Non-Governmental Organisation
NICD National Institute of Communicable Diseases
NMEP National Malaria Eradication Programme
NVBDCP National Vector Borne Disease Control Programme
PHC Primary Health Centre
POL Petrol, Oil and Lubricants
RFT&RC Regional Filaria Training and Research Centre
SPO State Programme Officer
SVBDCS State Vector Borne Diseases Control Society
Wb Wuchereria bancrofti
Wt. Weight

viii
CONTRIBUTORS
Two workshops, one at Vector Control Research Centre and another at the Office of the
State NVBDCP, Leh were held to deliberate on this guideline and the following experts
participated and contributed in preparing this guideline.
Dr. R.K.Srivastava, Director General of Health Services, Govt. of India
Dr.G.P.S.Dhillon, Director, National Vector Borne Disease Control Programme
Dr. C.K.Rao, NPO, WHO Office, New Delhi
Dr.P.K.Srivastava, Joint Director, NVBDCP, Delhi
Dr.R.K.Das Gupta, Joint Director, NVBDCP, Delhi
Dr.V.Kumaraswamy, Officer-in-Charge, Tuberculosis Research Centre, Chennai
Dr.N.C.Appavoo, Rtd. Director of Public Health, Govt. of Tamil Nadu
Dr.Sampana, National Vector Borne Disease Control Programme
Dr.P.K.Das, former Director, VCRC, Pondicherry
Dr.K.Krishnamoorthy, Scientist F, VCRC, Pondicherry
Dr.D.S.Dakure, Special Programme Officer, Govt. of Maharastra
Dr.P.Prajapati, Special Programme Officer, Govt. of Gujarat
Dr.Shazia Waft, Regional Director, Department of Health, Govt. of Jammu and Kashmir

1
Filariasis Control in India & Its Elimination
1. INTRODUCTION
Filariasis is the common term for a group of diseases caused by parasitic nematodes belonging
to super family Filarioidea. Adult worms of these parasites live in the lymphatic system,
cutaneous tissues or body cavity of the humans and are transmitted through vectors. Filariasis
caused by nematodes that live in the human lymph system is called Lymphatic Filariasis (LF)
2. CAUSATIVE ORGANISMS
Three nematode parasites causing LF in human are Wuchereria bancrofti, Brugia malayi and
Brugia timori. Of these, only Wuchereria bancrofti and Brugia malayi are found in India. In
mainland India, Wuchereria bancrofti, transmitted by the ubiquitous vector, Culex
quinquefasciatus, has been the predominant infection contributing to 99.4% of the problem in
the country. The infection is prevalent in both urban and rural areas. The vector species breeds
preferably in dirty and polluted water.
Brugia malayi infection has been reported earlier from some rural areas in seven states
viz., Kerala, Orissa, Tamil Nadu, Andhra Pradesh, Madhya Pradesh, Assam and West Bengal.
However, its prevalence is now reportedly restricted to rural area of Kerala. Mansonia
(Mansonioides) annulifera is the principal vector while M. (M). uniformis is the secondary vector
for transmission of B. malayi infection. The breeding of these mosquitoes is associated with
aquatic plants such as Pistia stratiotes, Salvinia auriculata, Salvinia molestes, Eichhornia
speciosa, E. crassipes, etc.
Both W. bancrofti and B. malayi infections in mainland India exhibit nocturnal periodicity
of microfilariae. In 1974-75, diurnal sub-periodic W.bancrofti infection was detected among
aborigines, inhabiting Nicobar Group of Andaman & Nicobar Islands. Ochlerotatus (Finlaya)
niveus group of mosquitoes were incriminated as the vectors for this infection, formerly known
as Aedes (Finlaya) niveus.
3. LIFE CYCLE OF THE PARASITE
The adult parasite worms, male and female, live in the lymph vessels and lymph nodes by making
nest in the dilated lymphatics. The adult worms survive for about 5-8 years and sometimes for as
long as 15 years. After mating, the female worm parturates millions of microfilariae which finally
migrate to blood circulation. The sheathed microfilariae begin to appear in the blood circulation in
six months to one year after infection (prepatent period). The microfilariae remain in the arterioles
of the lungs during the day and emerge into the peripheral circulation at night (nocturnally periodic).
The periodicity of mf coincides with the biting activity of the vector. The sexual cycle of the parasite
takes place in the human host, where the adult worms ultimately die. The life cycle of the parasite
is cyclo-developmental in the vector where the parasites do not multiply.
Microfilariae, (when picked up by the mosquito during blood meal) undergo development in
mosquitoes (intermediate hosts) to form infective larvae which usually takes about 10 to 14 days.
The ingested microfilariae first shed their sheaths, penetrate the stomach wall, migrate to the
1

2
muscles of the thorax and develop there without multiplication. The slender and tiny microfilariae
(Mean length of mf in Wb 290 µ, Bm 222 µ and Bt 310 µ) transform into immobile and inactive
sausage stage (L1) larva, which has a cuticle that forms a conspicuous slender tail with specific
identification characters. The larvae grow rapidly in length and breadth after their first moult to
become L2 or pre-infective larva, which is recognised by the presence of one or two papillae at its
caudal end and by its short tail. This L2 stage moults to become L3 which is infective. It is slender
and thread like, measuring about 1500 microns in length. It is highly motile which is a unique
phenomenon used for identification (Fig.1).
When the infective mosquitoes (harbouring L3 larvae) bite, some or all of the infective
larvae escape from the proboscis and actively enter the human host through the wound made by
the mosquito bite or penetrate the skin on their own and migrate into lymphatic system. In the
lymphatic system of the infected persons, the infective larvae develop into adult male and female
worms (Fig. 2).
4. WOLBACHIA ENDOSYMBIONT
Several recent studies have demonstrated presence of Wolbachia, a bacterial endosymbionts
in the adult filarial worms and microfilaria of both W. bancrofti and B. malayi. This bacterium is
necessary for the development, viability and fertility of the adult parasite. Drug interventions
directed against Wolbachia cause deleterious effect on the survival of the adult worms.
5. CLINICAL SPECTRUM
Man is the natural host. All ages and genders are susceptible to infection. In endemic areas, the
youngest age recorded with filarial infection was infant aged 6 months. The infection increases
with age reaching a peak between 20-25 years. Disease manifestation appears in a small
proportion of infected individuals, commonly over 10 years of age. The disease spectrum of LF
ranges from the initial phase of asymptomatic microfilaraemia to the later stages of acute,
chronic and occult clinical manifestations.
Fig 1: Different stages of larvae in mosquito

3
Fig 2: Life Cycle of Filarial Parasite
5.1 Asymptomatic Parasite Carrier State
Some of the infected individuals continue to harbour the parasite for many years without any
sign and symptoms of disease. Even at this stage subclinical changes like lymph vessel dilation
and tortuosity are shown by ultrasonography and lymphoscintigraphy. Only some among these
infected asymptomatic individuals‟ progress to clinical disease in course of time.
5.2 Acute Disease
Adenolymphangitis :
o Acute dermato-adeno-lymphangitis (ADLA)
o Acute filarial lymphangitis (AFL)
Acute epididymo-orchitis and funiculitis:
Courtesy : CDC, Atlanta

4
Acute dermato-adeno-lymphangitis (ADLA): Attacks of ADLA associated with fever and chills
are the common acute manifestations for which the patients seek medical intervention. It occurs
both in early and late stages of the disease progression, it is more frequent in higher grades of
lymphoedema. The affected area, usually in the extremities is extremely painful, warm, red,
swollen and tender, the draining lymph nodes in the groin or axilla become swollen and tender.
There may be lymphangitis, lymphadenitis, cellulites or abscess. Depending upon the
precipitating factors, the frequency and duration of each episode varies. Entry of bacteria and
pathogens through the lesions of the affected parts is responsible for the acute episodes.
Acute filarial lymphangitis (AFL): At the location where adult worms die, small tender nodes
are formed either in the scrotum or along the lymphatics of the limbs. Lymph nodes may
become tender. Inflamed large lymphatics may stand out as long tender cords underneath the
skin, usually along the sides of chest or medial aspect of arm, with restriction of movement of
the affected limb. But these episodes are not associated with fever, toxaemia or evidence of
secondary bacterial infection. Rarely abscess formation may be seen at the site of dead adult
worms. This acute manifestation is directly caused by adult worms and is usually rare. This may
occur due to death of adult worn either spontaneously or by antifilarial drugs.
Acute epididymo-orchitis and funiculitis: Inflammation of structures in the scrotal sac may
result in acute epididymo-orchitis or funiculitis in bancroftian filariasis. This is characterised by
severe pain, tenderness and swelling of scrotum usually with fever and rigor. The testis,
epididymis or the spermatic cord may become swollen and extremely tender. This manifestation
is also precipitated by secondary infections.
5.3 Chronic Disease
Lymphoedema, hydrocele, elephantiasis and chyluria are the main clinical pathological
consequences of chronic bancroftian filariasis.
Involvement of Limbs
Lymphoedema of the extremities is a common chronic manifestation of LF, which on
progression leads on to elephantiasis. Lymphoedema of the limbs is graded as follows:
Grade I lymphoedema: Mostly pitting oedema; spontaneously reversible on elevation (Fig. 3).
Grade II lymphoedema: Mostly non-pitting oedema; not spontaneously reversible on elevation
(Fig-4).
Grade III lymphoedema (elephantiasis): Gross increase in volume in a grade II lymphoedema
with dermatosclerosis and papillomatous lesions (Fig. 5 & 6)
In the advanced stages of lymphoedema, the skin is thickened and thrown into folds, often with
hypertrichosis, black pigmentation, nodules, warty growth, and Intertrigo in the webs of toes
(Fig. 7) or chronic non-healing ulcers.

5
Genito-urinary Involvement
Hydrocele
Chylocele
Lymphoedema of the scrotum and penis
Lymph scrotum
Hydrocele is a common chronic manifestation of bancroftian filariasis in males (Fig. 8).
This is characterized by accumulation of fluid in the tunica vaginalis, the sac covering the testes.
The swelling gradually increases over a period of time and in long standing cases the size of the
scrotum may be enormous. Lymphoedema of the scrotum and penis may occur in bancroftian
filariasis. In some subjects, the skin of the scrotum may be covered with vesicles distended with
lymph known as „lymph scrotum‟. These patients are prone for ADLA attacks involving the skin
of genitalia.
Chronic epidiydimitis, funiculitis (inflammatory) swelling of the spermatic cord), and
lymphoedematous thickening of the scrotal skin are also genital manifestations of chronic
filariasis. These manifestations are uncommon with brugian filariasis.
Fig. 3: Grade I Lymphoedema Fig. 4: Grade II Lymphoedema
Fig. 5: Grade III Lymphoedema without nodules and warts
Fig. 6: Grade III Lymphoedema with nodules and warts

6
Other Manifestations
The other manifestation includes chyluria, hematuria, and Tropical Pulmonary Eosinophilia
(TPE) and Filarial granulomata.
Chyluria: It is defined as the excretion of chyle in the urinary tract. The basic pathophysiology is
related to blockage of the retroperitoneal lymph nodes below the cisterna chyli with consequent
reflux and flow of the intestinal lymph directly into the renal lymphatics, which may rupture and
permit flow of chyle into the urinary tract. The resultant “milky urine” contains considerable
quantities of lymph originating from the gastro-intestinal tract. The condition is usually painless
but large amounts of dietary lipids, proteins, and possibly fat soluble vitamins are excreted
leading to weight loss.
Occult filariasis and Tropical Pulmonary Eosinophilia It is the condition in which the
classical clinical manifestations are not present and where microfilariae are not found in the
blood but may be found in the tissues. Tropical Pulmonary Eosinophilia (TPE) is the classical
example of occult filariasis. TPE associated with high eosinophil counts in the peripheral blood
is an occult manifestation of both W. bancrofti and B. malayi filariasis. This syndrome is
characterized by severe cough and wheezing (specially at night), diffuse mottled pulmonary
interstitial infiltrate, peripheral blood eosinophilia > 2500 cell /ml, extreme elevation of
immunoglobin (IgE), extreme elevation of anti-filarial antibodies and dramatic clinical
improvement in response to specific anti-filarial chemotherapy with diethylcarbamazine (DEC).
6. CURRENT STATUS AND DISTRIBUTION
Global burden of lymphatic Filariasis
Lymphatic filariasis is the world's second leading cause of long-term disability. Although filariasis
does not kill, it causes debility and imposes severe social and economic burden to the affected
individuals, their families and the endemic communities. The current estimate reveals that 120
million people in 83 countries of the world are infected with lymphatic filarial parasites, and it is
estimated that more than 1.1 billion (20% of the world's population) are at risk of acquiring infection.
Over 40 million people are severely disfigured and disabled by filariasis and 76 million are
apparently normal but have hidden internal damage to lymphatic and renal systems. According to
Fig. 7: Entry lesion (candidiasis) in the web of toes in filarial leg
Fig. 8: Chronic genital manifestation on the left side of the scrotum

7
the World Health Organization, India, Indonesia, Nigeria and Bangladesh alone contribute about
70% of all the infection worldwide.
It has been estimated that approximately 5 million Disability Adjusted Life Years (DALYs)
lost annually, ranking third among the TDR diseases in terms of DALYs(Disability-adjusted life-
years), after malaria and TB. In addition, the social and psychological impact is enormous -
often destroying marriages and family relationships. Although filariasis does not kill, it causes
debility and imposes severe social and economic burden to the affected individuals, their families
and the endemic communities. Lymphatic filariasis is a major impediment to socioeconomic
development and cause and effect of poverty.
Current Status and Distribution of LF in India
The disease was recorded in India as early as 6th century B.C. by Susruta, in his book „Susruta
Samhita‟ and in 7th century A.D., Madhavakara described sign and symptoms of the disease in
his treatise „Madhava Nidhana‟, which hold good even today. In 1709, Clarke called
elephantoid legs in Cochin as „Malabar legs‟. The discovery of microfilariae (mf) in the
peripheral blood was made first by Lewis in 1872 in Kolkata City.
Indigenous lymphatic filariasis cases are reported from 20 States/UTs namely Andhra
Pradesh, Assam, Bihar, Chhattisgarh, Goa, Gujarat, Jharkhand, Karnataka, Kerala, Madhya
Pradesh, Maharashtra, Orissa, Tamil Nadu, Uttar Pradesh, West Bengal, Pondicherry,
Andaman & Nicobar Islands, Daman & Diu, Lakshadweep and Dadra & Nagar Haveli. From
these States/UTs, a total of 250 districts have been identified to be endemic for filariasis with a
population of about 500 million at risk.
The North-Western States/UTs namely Jammu & Kashmir, Himachal Pradesh, Punjab,
Haryana, Chandigarh, Rajasthan, Delhi, Uttaranchal and North-Eastern States namely Sikkim,
Arunachal Pradesh, Nagaland, Meghalaya, Mizoram, Manipur and Tripura are known to be free
from indigenously acquired filarial infection.
7. CONTROL OF LF IN INDIA
National Filaria Control Programme, launched in 1955 has operational, training and research
components. The strategies include (a) vector control (b) detection and treatment of filarial
cases and (c) delimitation of endemic areas. This is being carried out through control units, night
clinics and survey teams. This programme continues to be in place, in addition to the
programme to eliminate LF in India.
8. LF ELIMINATION STRATEGY
What is meant by Elimination of Lymphatic Filariasis?
Elimination of LF is meant that LF ceases to be a public health problem, when the number of
microfilaria carriers is less than one per cent and the children born after initiation of ELF are free
from circulating antigenaemia. Absence of antigenaemia among children is considered as
evidence for absence of transmission and new infection.
In 1997, WHO and its Member States made a commitment to eliminate Lymphatic
Filariasis (LF) as public health problem by 2020 through World Health Assembly resolution
WHA 50.29. The National Health Policy (2002) has set the goal of Elimination of Lymphatic
Filariasis in India by 2015.

8
The Govt of India constituted the
National Task Force (NTF) with Director
General of Health Services, MOH&FW as
Chairperson, DG ICMR, Director NICD,
senior officers of Health services from
states as members and Director of
NVBDCP as Member Secretary. NTF
reviews and recommends the strategy for
ELF in India.
The twin pillars of LF elimination
strategy include:
1. Transmission control – to prevent the
occurrence of new infection and
disease by administration of annual
single dose of anti filarial drug i.e.
DEC and or co-administration of
DEC+Albendazole.1
2. Disability Prevention and
Management – for those individuals
who already have the disease
Home based management – limb
hygiene for lymphoedema
Hospital based management –
surgical correction for hydrocele
Major components/functions/tasks towards
implementation strategy include:
Disease burden estimation
Mapping and stratification
Advocacy
Social mobilization
Implementation of MDA
Implementation of disability
prevention and management
Monitoring and Evaluation
Background surveillance to
prevent resurgence
Certification
1 The MDA programme will continue with DEC. Albendazole will be added when it is made available from WHO
which has agreed to supply the drug at free of cost for the LF elimination programme in India. DEC+Albendazole
administration will be included in MDA 2008 onwards.
Key advances that form the basis of the strategies for the elimination of lymphatic
filariasis
Man is the main reservoir of infection at least in India
Better understanding of the disease dynamics: o Asymptomatic carriers o Acute attacks are caused by secondary
bacterial infections o Entry lesions such as intertrigo are
responsible for the occurrence of acute attacks
o Early damage to the lymphatics o Dilation and dysfunction of lymphatics
rather than obstruction
Parasite better understanding o Parasite exhibits genetic diversity o Long patent period
Drugs o DEC and albendazole o Drugs are safe and are already in
clinical practice o Single annual dose of anti-filarial drugs
can suppress microfilaria levels for periods as long as one year
Delivery system – community based
Diagnostics – antigeneamia and antibody tests
Over 85% coverage of the population for at least 5 years could effectively interrupt transmission
MDA is operationally feasible to carry out with the available health care infrastructure with the support of community volunteers
Side effects due to the drugs are primarily in response to the killing of the parasites and can easily be managed
The key to success is community participation. Community mobilization is a key component of the elimination strategy

9
Mapping And Disease Burden Estimation
1. MAPPING
The objective of mapping areas is to identify the potential transmission areas where
intervention to be introduced.
This could be done by:
Historical records
Rapid method by key informant interview
Physical examination of the individuals by the health workers
Microfilaraemia survey
Detection of infective stage larvae in the vector
Currently the ELF is being implemented in 250 known endemic districts. These have been
chosen based on historical data on endemicity or based on reports from the states. It is
important to verify the current endemicity status of other districts especially those adjoining the
MDA districts. In MDA districts also, where the ELF is ongoing, updating of mapping will be
useful for monitoring and evaluation. Case detection is required in all the intervention districts
for providing morbidity management services.
1. 1 Historical Records
Data already available on the prevalence of microfilaraemia and or disease can be used to
identify the endemic areas. Areas qualify for the intervention includes evidence for indigenous
transmission or mf prevalence above 1%. Based on the data on prevalence of infection, the
area can be classified into (a) clearly endemic (red) (b) clearly free from infection (green) and (c)
areas with insufficient evidence (gray). Source of information, reliability of data, period or time
survey, survey methods etc. are to be considered while taking decision on the inclusion of areas
for introducing the intervention.
1.2 Key Informant Questionnaire Method
A simple questionnaire circulated to key informants such as school teachers, health workers,
Panchayat members, local medical practitioners, etc. will enable to identify high endemic areas.
Negative reporting does not necessarily mean that such areas are free from transmission of
filariasis. The sample questionnaire is given at Annex. 2.2.
1.3 Direct Physical Examination by Health Worker
In areas where the questionnaire cannot be administered or the informants are not
knowledgeable about disease prevalence, physical examination can be used as a rapid
2

10
assessment tool for lymphatic filariasis. In this approach, mobile teams of health workers visit
villages and examine adults for lymphoedema of the leg or hydrocele in males. In some
communities, the prevalence of hydrocele has offered good indirect evidence of transmission of
LF in the area.
1.4 Detection of Microfilariae in the Blood
For epidemiological screening, 20 cmm of finger-prick blood can be dried flat on a slide, stained
and examined under a microscope in accordance with the standard procedure.
Advantages of using microfilaraemia detection in finger-prick blood for initial assessment
include the general availability of materials and trained staff in many filariasis endemic districts
and the fact that positive specimens are “parasitologically confirmed”. Disadvantages include
the need to collect blood at night (between 8.30 pm and 12 midnight) and the labour-
intensiveness of preparing and examining slides.
Microscopic slides and stains will be required for baseline parasitological surveys in
sentinel surveillance sites before the first round and for subsequent years. The selection
methodology of microfilaria survey for collection of baseline data and data to assess the impact
is given in Chapter- 3.
1.5 Detection of Infective Stage Larvae (L3) in Mosquitoes
Xenomonitoring is defined as the monitoring of parasite in the vectors. By this method, vector
mosquitoes are collected and examined for the presence of parasite (dissection) or parasite
material (Polymerase Chain Reaction) using molecular technique. Presence of infective stage
larva of LF is considered as an indication of current risk of transmission. Presence of larva in the
vector indicates the presence of microfilaria carriers in the community. This is a passive method
without samples from human. These are described for better understanding to the programme
officers and assistance of research institutes can be sought for such work.
2. NON-ENDEMIC DISTRICTS
The districts, which are currently shown as non-
endemic or where there are no records, need to be
surveyed involving steps shown in flow diagram A & B:
3. MAPPING BASED ON AVAILABLE RECORDS
FOR FILARIASIS
Based on the data available till year 2006, there are
243 filaria endemic districts, which are shown in
endemicity map. Mass Drug Administration is being
implemented in these districts. However, the other
districts are being resurveyed for filaria endemicity.
The endemicity map shown in earlier years is depicted
at the end of this chapter.
Filaria Endemicity Map - 2005

11
Flow Diagram A
Flow Diagram B
Examination of all available records
Key Informant Questionnaire for occurrence of cases of Filariasis
(Elephantiasis / Hydrocele)
Occurrence of filariasis cases No case of filariasis (See Flow diagram B)
Estimation of level of endemicity
Line listing of cases (For mapping as well as for MM) Microfilaraemia Survey (as per design) (For monitoring and evaluation)
Intervention decision
(MDA & Morbidity Management)

12
4. DISEASE BURDEN ESTIMATION
Disease burden estimation is a prerequisite to:
identify areas that require intervention
prepare advocacy package to implement the intervention
plan, deliver and monitor disability alleviation and prevention strategies
monitor and evaluate intervention programmes.
4.1 Methods
The methods to assess disease burden aim at enumeration how many people are infected and
how many with disease manifestations. This can be carried out to examine historical data and/or
to carry out community surveys. Line listing is the principal method to enlist all the diseased
individuals in the given community.
4.2 line listing of filarial cases and analysis of data
Prevalence of filarial disease cases in the community should be enquired from community
heads, key informers and opinion leaders. Since lymphoedema is recognizable, the information
can easily be obtained. The reported cases are to be confirmed by visiting their houses. It is to
be enquired whether any other person in the family or in the neighbourhood also suffers from
the disease. The details are to be compiled at village/subcentre/PHC/District/State levels
including similar compilation in urban areas. This will be useful to identify high-risk areas and
more accurate estimates of disease burden could be made. Such information would be useful in
chalking out strategies for elimination of lymphatic filariasis by prioritising areas within each
district for more intensive IEC activities, morbidity management and monitoring the
effectiveness of health care delivery services on disease burden. The line listing of cases should
include the following particulars:
A patient card will be provided to the health workers to make record of persons having
manifestations of filarial such as lymphoedema, hydrocele, etc. The information should be
noted. This card should be handed over to the patient so that he can contact
CHC/PHC/Subcentre for morbidity management including hydrocelectomy.
Elimination of Lymphatic Filariasis
Patient Card
State:________________District:__________________PHC_________________
Subcentre:____________________Village:____________________
Name of the household:
Name of the patient
Address
Age
Sex
Duration of lymphoedema/ hydrocele
Other family members affected

13
On the back of the card, write some key messages on morbidity management and
prevention of filariasis.
Line listing of cases is to be recorded by the health worker in Form-1 for submission to
MO-PHC (Annex-2.1). The information will be recorded by the health workers in the village-wise
compilation register under the relevant sub-headings.
The nodal officer of districts should collect the information for rural and urban areas in
the district. The compilation should be done using the Form 2, 3 and 4 which should be
submitted to State HQ, with a copy to the Directorate of NVBDCP along with diagram and map
showing the PHCs and Subcentres where suspected cases were reported.
Annexure 2.1
Form- I
LINE LISTING OF FILARIA PATIENTS
State: _________________District:______________________________ PHC:__________________________
Sub-centre:________________________ Name of the health worker:_________________________________
Sl
.
N
o.
Name of
Patient
S
e
x
A
g
e
Name of
Head of
family &
address
Village/
Pancha-
yat
Population Disease affected part Time of
starting
of
disfigur
ement
Period
of stay
in
district
Date
of
survey
L
e
g
Hand Scr
otu
m
Bre
ast
Oth
ers
Note: Form 1 is meant for collecting basic information by the peripheral health worker / health
volunteer while Forms 2-4 are for data analysis which is to be filled by the supervisory staff with
the help of basic health workers
Form-2 ( To be compiled at PHC)
Age-wise and sex-wise classification of cases in subcentre………………..……
Age Below
2 years
2-4 5-8 9-14 15-25
26-40 41-60 60> Total No
Sex M F M F M F M F M F M F M F M F M F T
No. of
Patients
M: Male, F: Female, T: Total

14
The MO PHC will compile sub centres-wise report on Format No. 2, 3 & 4 and analyse the data
further by making a line map and diagram and forward to the district.
Example: Line list of patients:
S. No. Name of the Patient Age of
Patient (years)
Duration of
Disease (years)
Gender Village
1. Sunita 30 4 F D
2. Manoj 82 25 M A
3. Ram 60 3 M C
4. Gopal 36 4 M B
5. Shyam 30 2 M A
6. Hussain 30 5 M B
7. Meena 38 2 F B
8. Raghunath 55 3 M C
9. Pritam Singh 50 20 M D
10. Ganga 40 8 M D
11. Sangeeta 30 5 F A
12. Murti Singh 45 7 M B
13. Phool Kumari 55 20 F A
Based on the above information collected at subcentre level, the PHC-wise and District-wise
consolidated forms, map and graph will be prepared at the respective districts as indicated
below and will be sent to State Headquarters and the Dte. of NVBDCP, Delhi. The Form-1 for
line listing of patients by the health workers/health volunteer is given in Annexure 2.2. The
photo identification card for LF patient with questionnaire for line listing is given in Annexure
2.3.
Form-3 ( To be compiled at PHC)
Types of Disfigurement due to Lymphatic Filariasis in subcentre……….
Disfigurement area Leg Hand Scrotum Breast Others Total No.
No. of cases →
Form-4
Percentage of filarial patients in subcentre………….…
Name of
Village/Panchayat
Population No. of Filaria
patients
Percentage of filarial patients

15
Village C
Village B
Village A
Village D Sub-centre
MAP INDICATING VILLAGES OF FILARIA AFFECTED PATIENTS IN SUBCENTRE
A. Spot map of cases by residence
B. Age and gender-wise distribution of LF patients in subcentre_____________________
Year________
No
. o
f L
F p
ati
en
ts
M F T M F T M F T M F T M F T M F T M F T M F T M F T
Below 2
years
2-4 years 5-8 years 9-14
years
15-25
years
26-40
years
41-60
years
60+ years Total

16
Annex 2.2
INTERVIEW OF KEY INFORMANTS
Rapid Assessment of Community Burden of Disease
1. State: ……………………………………………………………
2. District: ……………………………………………………………
3. Name of village/urban area: ……………………………………………………………
4. Name of the informant: ……………………………………………………………
5. Age: ……………………………………Years
6. Sex: ………………………
7. Occupation: ………………………………………….…
8. How many years have you lived in this village/ urban area? ………. Years
9. Have you seen local inhabitants of the area with elephantiasis of the leg?
Yes No
10. How many people in the village have elephantiasis?....................................
10.1. Do you consider elephantiasis to be a health problem in this village/ urban area?
……………………………………………………………………………………...
11. Do you know of people in this village with hydrocele?
Yes No
11.1. How many people in the village have hydrocele:……………………………
11.2. Do you consider hydrocele to be a health problem in this village/urban area?
……………………………………………………………………………………...
12. Do you know of people suffering from acute attacks of filariasis?
13. Do you know about MDA in your area?
14. Have you consumed anti-filarial drugs?
15. Have you encouraged your neighbours, relatives and friends to consume the anti-filarial
drug?

17
Annex 2.3
FLASH CARD FOR LINELISTING
This card to be used by the Health Workers/volunteers visiting villages/urban areas

18
FILARIA ENDEMICITY – INDIA
1958 1969
1995
Non-Endemic districts
Unsurveyed districts
Endemic Districts with mf > 1
Endemic Districts with mf < 1
2005

19
Implementation Of Mass Drug Administration
1. INTRODUCTION TO MDA AS LF ELIMINATION STRATEGY
The concept of MDA is to approach every individual in the target community and administer
annual single dose of anti filarial drug (DEC or DEC+Albendazole). This annual dose is to be
repeated every year for a period of 5 years or more aiming at minimum 85 % actual drug
compliance.
2. APPROACHES FOR DRUG ADMINISTRATION
The following are the options for the delivery of the drugs:
House to house approach: every individual is administered with the drugs at his/her
door steps.
Booth approach: People are asked to come at predetermined place (booth) for
receiving the drug. The booths should not be located more than one kilometre walking
distance away from the community.
Group approach: Special population groups in places like schools, hospitals, offices,
industries, prisons, etc. including community aggregations like developmental projects,
market places, bus stands, railway stations, fairs, agriculture fields, etc. – are
approached for delivery of the drug.
The recommended approach based on the past experience is “supervised drug
administration by door to door visit supplemented with drug administration at booths
and groups” preferably on a single day with two-day mopping up operations, instead of
mere distribution of drug.
Drug administrator is to
administer the drug in his/her
presence (supervised administration).
It is preferred not to administer the
drug on an empty stomach. The
schools could be visited during lunch
recess or any other suitable time. The
local programme manager should
adopt suitable drug delivery strategy in
consultation with community leaders,
school teachers, managers and
supervisors of the workplaces to
achieve high drug intake. The drug
should not be left with the individual or relatives for swallowing it later.
DRUG DOSAGE SCHEDULE
Age in years
Streamlined Dose
DEC Albendazole
Dose
(mg)
Number of
100 mg
tablets
Dose
(mg)
Number of
400 mg
tablets
0-2 years 0 0 0 0
2 - 5 years 100 1 400 1
More than 5 up to
14 years
200 2 400 1
More than 14 years 300 3 400 1
3

20
3. DOSAGE SCHEDULE OF DRUGS
For operational convenience, age-wise dosage of single dose of 6 mg DEC per kg body weight,
adjusted to average weight has been streamlined. Albendazole is to be given to all the eligible
individuals as a single dose of 400 mg irrespective of age and weight. Both the recommended
doses of DEC+Albendazole are to be taken together as a single dose.
4. PREPARATORY ACTIVITIES
The activities that are necessary in implementation of Annual Mass Drug Administration can be
grouped into:
Pre-MDA (preparatory)
During MDA
Post-MDA
5. PRE-MDA ACTIVITIES AT DIFFERENT LEVELS
5.1 Projection of DEC and Albendazole Requirements
The population already enumerated every year shall
be used for calculating the drug requirement as per
the formula given below. This requirement minus the
balance of drugs (DEC and Albendazole) in hand
received from previous year will be the requirement
for the current year. The indent for the current year is
to be placed through the state programme officer and
communicated to the Directorate of NVBDCP, 22- Sham Nath Marg, Delhi-110 054. This indent
should also be accompanied with “utilization certificate” (UC) for the fund provided by NVBDCP
for ELF activities. The drugs must be received by the state at least three months before the
scheduled date of MDA.
5.1.1 Flow of Indents for Drugs
Medical Officers of PHCs and Health Officers of municipalities will prepare the requirements of
drugs and submit to the district level officers who in turn submit to state programme managers.
State programme officer will send it to the Directorate of NVBDCP, Delhi.
5.2 Advocacy and Inter-sectoral Meetings/Workshops
a. State Task Force (STF) under the chairpersonship of Minister of Health & Family Welfare of
the State and Chief Secretary as Vice-Chairperson while the other members such as Addl.
Chief Secretary, Health Secretary, Secretary (Finance), Secretary (Tribal), Secretary
(ICDS), Secretary (Social Welfare), Secretary (Irrigation), Secretary (Rural Development/
Panchayat Raj), Secretary (Agriculture), Secretary (Local Self Govt), Secretary (Industry),
Secretary (Forests), Secretary (Information), Secretary (Education), Director General of
Health Services (State)/Director of Health Services and State Programme Officer of Malaria
& Filaria (Member Secretary) will constitute the STF. The State Mission Director, NRHM
must be included as member of State Task Force. The broad Terms of Reference would be
to review the progress of implementation and impact of MDA for ELF, policy decisions and
DEC
100 mg tablets: Multiply
total population in endemic
areas by 2.5
Albendazole
400 mg tablets: Multiply
total population in endemic
areas by 1

21
modifications wherever warranted, to identify the roles & responsibilities of different
departments for successful implementation of ELF, release of sufficient funds for ELF, etc.
The first meeting of STF is to be held 120 days before MDA, the second meeting one month
before MDA and the third meeting one-and-a-half-months after MDA to review the
performance. The draft terms of Reference communicated earlier is at the end of this
chapter.
b. State Technical Advisory Committee (STAC) under the Chairpersonship of Director
General of Health Services (State) /Director of Health Services (State), while the members
such as Director of Medical Education & Research, Director of Indian System of Medicine,
Director of State Health Education Bureau, Prof. & HoD of Pharmacology, Prof & HoD of
Medicine, Prof. & HoD of PSM, Prof. & HoD of Paediatrics, Prof. & HoD of Microbiology,
Regional Director of ROH&FW, President of Indian Medical Association (State Branch) and
State Programme Officer of Malaria & Filaria or VBD (Member Secretary) will comprise of
STAC. The nodal state programme manager under NRHM must be included in STAC as
member. The broad Terms of Reference of STAC would be to review the administrative,
financial & logistics for ELF, functioning of State and District Societies, technical inputs for
ELF, morbidity management of filaria cases, capacity building, performance & impact
assessment, review the reporting system, inter-sectoral coordination, integrated vector
control measures, operational problems, etc. The first meeting of STAC is to be held 90
days before MDA, the second meeting a fortnight before MDA and the third meeting one
month after MDA to review the performance. The draft terms of Reference communicated
earlier is at the end of this chapter.
c. The instructions from the respective State Govt. State Mission Director NRHM must be
issued for nominating the District Magistrate/District Collector as the Chairperson of the
District-level Co-ordination Committee (DCC) and the district level programme officer for
Filaria/ District Medical Officer (District Vector Borne Diseases Control Officer) as Member
Secretary with other representations from public-private and NGO sector as members. The
district programme manager of NRHM must be included as member of DCC. It would be
advisable to include social sector department such as education, youth affairs, social
welfare, rural development, Panchayat, Municipal Corporation, information and
broadcasting, etc. in the DCC. Representation from professional organisations association
like SMA, CII, IMA, FICCI, ASSOCHAM, etc. may also be co-opted as members besides
NGOs. The terms of reference for this committee may also be specified stating that this
committee will oversee the implementation of MDA programme of districts and take
appropriate measures deemed fit to improve the consumption level of DEC tablets and
monitoring its impact through microfilaria survey. During the 1st meeting, the members
should be informed about the purpose of single dose mass drug administration and
requested to extend their co-operation by suitably instructing their line staff in the periphery
to co-operate in the programme. The National Filaria Day for conducting MDA throughout
the endemic districts/PHCs and the preparatory work should be discussed in the first DCC
meeting. This activity must start at least 90 days prior to the actual date of the proposed
date for MDA. Action plan for MDA should be discussed in detail besides discussions on
the achievements and problems during the MDA campaign (MDA) of previous year.

22
d. Conduct sensitisation / advocacy to all district level officials / NGOs / others: Depending on
the number of persons to be sensitised, this can be conducted either on a single day or
more than one day. What is important is that this opportunity is made use for explaining in
detail the need for everybody to swallow the tablets. Explain that DEC and Albendazole
tablets are safe drugs and there will be no side reaction practically at the recommended
dosage schedule. However, some may develop mild reaction, which is mainly due to the
effect of microfilariae getting killed in infected persons. These side effects are transitory in
nature. If any serious reactions are noted, the same must be brought to the notice of the
health department immediately. This activity must be planned within 10 days after the
1st district level co-ordination committee meeting and carried out within 60 days prior
to the actual date of MDA. Advocacy workshops may be repeated if required to
ensure optimal cooperation and active community involvement.
e. Conduct First Press meet / Media Flash / All India Radio / Doordarshan / Cable TV: Write-up
on Filariasis and its control can appear in columns of newspapers especially in local dailies,
preferably in the local language. Appeals by the prominent leaders from the community,
stressing the importance of each and everybody swallowing DEC or DEC+Albendazole
tablets should be issued. Appeals should also include that the side effects, if any, will be
mild and the programme has taken all measures to provide treatment facilities if anybody
reports about the occurrence of such reaction. District Collector may brief the media about
the MDA. This activity must begin with the first meeting of DCC and carried out 30
days prior to drug administration. (The prototype messages/writes up are annexed).
f. Organise district level training/sensitisation programme for community health officers/Deputy
Civil Surgeons/Municipal Health Officer/MO PHC, etc : The content of the training should
mainly focus on how to draw a micro-plan for their areas, how to estimate the drug
requirement, IEC materials requirement and other logistics, the side effects anticipated, the
knowledge and the drug requirement for management of these side effects, the downward
flow channel for the supply of drugs, IEC materials, and upward flow of balance quantity of
drugs and the reports. This activity should be planned for a few days depending on the
number of personnel to be trained. Normally this will be for one day at district
headquarters. The trainers will be the district level programme officers supported by the
state level programme officer, officers from Regional office for Health & FW, GOI and faculty
from medical colleges. This activity should be completed at least 45 days prior to actual date
of drug administration. This activity is to be followed by a similar training programme for the
PHC/ Municipal level medical officer and paramedical staff at PHC headquarters and towns.
Morbidity management with hands-on training should be included in all programmes. The
officers of urban areas must be included. (The copies of presentations for training are
annexed at the end).
g. Preparation of Village/Ward level micro-plan for drug administration / Inter personal
communication activities in Sub-centres, Wards, PHCs and Municipalities: This is very
important activity, which calls for the bottom up approach for planning. This micro-plan
should contain details indicating the village/street/ward, its population, schools,
dispensaries, etc. in order to determine the number of workers required for door to door drug
distribution or booths to be established. However the grouping of houses is to be done
based on the previous experience that in a single day how many families can be covered by

23
one health worker/health volunteers. Depending on terrain, location of houses whether
sparsely/thickly populated, etc., it is estimated that a health worker can cover about 50
families on a single day depending upon the density of population if all the preparatory
activities are done in advance. If the activities are started only at the time of MDA, it will be
difficult to cover 50 houses in one day and result into low compliance. This micro-plan must
be received at every PHC level at least 30 days in advance of the day of drug
administration. All the PHC-wise micro-plans so prepared should be compiled for the district.
The involvement of Village Health & Sanitation Committee is essential and the PHC MO I/c
or District authorities should issue instruction from NRHM to the representative of villages &
Health Sanitation Committees for providing full cooperation, involvement of ASHA,
Aganwadis and other volunteers in the programme for social mobilization and acceptance of
the programme by the community.
h. Conduct 2nd meeting of District level Coordination Committee to review the District Action
Plan (Manpower Assessment / Logistics- mobility / supervision, etc.) and preparedness for
launching the MDA and take appropriate measures to plug the loopholes, if any: This must
be done at least 15 days in advance of the day of drug administration.
i. Second press meet / media flash / All India Radio / Doordarshan / Cable TV / newspaper
articles: This must be done at least 15 days in advance of the day of drug administration.
Repeat the activities as explained earlier under first press meet/ media flash.
j. Organising workshop on Filariasis with special reference to MDA for private practitioners
through professional associations like IMA, IAP, etc: 15 days prior to MDA
5.3 Training of Paramedical Staff at PHC / Municipal Level
This activity should be carried out immediately after the district level training/sensitisation
programme. The venue may be fixed at PHC/Municipal level. The trainers must be the medical
officers of PHCs and Municipal Health Officers. The content of the training should also be the
same as given under district level training but the medium of training shall be the local
language. This activity must be carried out 30 days prior to drug administration.
5.4 Selection and Training of Drug Administrators
The ASHA, DDC, FTD holders, Anganwadi workers, Malaria Link Volunteers, teachers and
other social workers should preferably be deployed wherever available since these workers are
mainly local and have the confidence of the community. The drug administrator should not be a
stranger to the community. They should be imparted one day training on Do‟s and Don‟ts during
MDA. Such training and orientation of Drug Distribution is to be carried out for interpersonal
communication during their door to door visits. The drug distributors should carry household
cards and maintain them properly. Role of Drug Distributors for supervised drug intake (timing of
distribution especially whether the period would be post breakfast/lunch, etc) need to be
explained clearly. Training of Drug providers at Mandal (Block HQ)/ PHCs/ Sub-centre/ Village
level for rural areas and municipal level for urban areas must be completed 15 days prior to the
date of MDA.
5.5 IEC/BCC Activities

24
Procurement and distribution of IEC materials: The flow of IEC materials and the drug is
depicted in the following diagram. This can be modified depending on the local situation and
requirements.
State District PHC Sub-centre
Village /Ward Health & Community
Sanitation committee
Urban areas Ward
The steps explained under the Chapter “Behaviour Change Communication” are to be
followed. The activities should be started well in advance so that the IEC materials, training
guidelines and enumeration registers are made available during the training programme at each
level. It must also be ensured by discussion with the Regional Director of ROH&FW, MoH&FW,
GOI, NRHM State Mission Director, Programme Coordinator NRHM, State Programme Officer,
district level officials and medical/health officials to identify and segregate the materials that are
to be produced at each level in order to avoid duplication and distortion of messages. This
activity should be completed at least 45 days prior to the date of MDA. The prototype materials
on IEC for replication in local language by the states are annexed.
5.6 Enumeration of Households and Inhabitants in the Prescribed Household Registers
and Household Cards
The health workers along with identified drug administrator will conduct household enumeration,
update the Register and issue household cards in each village/ward during their routine visits,
prior to MDA. During their house visit, apart from recording the name, age, gender of the
members and any case of lymphoedema/hydrocele in the household, they should also explain
the following information to the community:
Need for MDA
Date/month of MDA
Consumption of drug in presence of drug administrator
Safety of the drug
The health workers will carry Flash cards with them which have also key messages on
its backside. They should also have IEC local kit for educating the community.
5.7 Microfilaria survey
Microfilaria survey is to be carried out one month before (prior to every MDA round) in identified
sentinel and random sites. The detail methodology has been described in Monitoring &
Evaluation chapter.
6. ACTIVITIES DURING MDA
6.1. Drug Administration on the Fixed Day
Supervised administration of the drug is to be adhered to the maximum extent possible by door
to door visit supplemented with other methods by the drug administrators. The National Filaria

25
Day is fixed during November when the drug is administered. To cover the absentees, mop-up
is to be carried out.
6.2. Mopping-up Operation to Enhance the Coverage Level
This should be planned for two days following the day of drug administration so that the left out
households, if any, or poorly covered areas may be taken up so as to maximize drug
consumption. Since each drug administrator is allotted 50 households covering 250 persons,
two drug administrators in the adjacent areas can form a team for mopping up operations
covering 500 population. In areas with low coverage, the supervisory staff should assist in
improving drug compliance.
6.3. Management of Side Effects of Drugs
These drugs may produce side effects in 1-2% of the treated persons. These side effects are
self limiting:
(a) Non-specific drug related reactions include headache, anorexia, nausea, abdominal
pain, vomiting, dizziness, weakness or lethargy. These symptoms begin within 1-2 hours
of taking the drug and persist for a few hours.
(b) Specific parasite related allergic reactions due to destruction of microfilariae and adult
worms include fever, local inflammations around dead worms and pruritus.
Symptomatic treatment of the reactions with antipyretics/analgesics and anti-allergic
agents should be given. The side effects also disappear spontaneously with or without
symptomatic treatment.
6.3.1. By Drug Administrators
In case of side effects, he/she should inform the health worker immediately for management.
6.3.2. By Health Workers
He/she should administer symptomatic drugs. In case of doubt, Medical Officer‟s services may
be availed including case management and referral.
6.4. Organise Rapid Response Teams for Management of Side Effects
This is an important activity. Medical teams at strategic places can be formed and the people
and the drug administrators are informed about the availability of such teams including the
phone numbers so that they report directly to these teams at times of emergency. These teams
should be in position for the period from the day of drug administration till the completion of
mopping up operations. The team should comprise of minimum one medical officer supported
by a staff nurse and a pharmacist and ambulance. The team should have an ambulance with
mobile phone and essential life saving drugs.
6.5. Supervision of the Drug Administration
On the days of drug administration and mopping-up operations, it must be supervised to ensure
that the drug is physically administered to each and every eligible individual. One supervisor
should be identified for every 5 to 10 drug administrators depending upon the terrain and

26
availability of such personnel who are also trained in dosage schedule, IEC, etc. This must be
indicated in the micro-plan itself. The supervisor should also ensure that no area/village is
omitted. He/She must also carry with him/her some quantity of drug so that if shortage with any
drug administrator is noticed during field visits, replenishment is made or diversion is made from
surplus area. The supervisors must be trained to select at least 10% of the houses in his /
her area to conduct consumption survey, side reaction survey and communication methodology
survey in these families. These surveys are to be completed within one week after the mass
drug administration. The cross-checking report by the supervisors must be submitted to the MO
PHC immediately. The supervisor will submit his visit report to PHC on the following format:
Sl.
No.
Name
of
Village
Total No.
of
houses
No. of
households
surveyed
(10%)
Number of
individuals
reported to have
consumed the
drugs
No.
reported
with side
effects
Which
communication
methodology is
most acceptable in
the area
1
2
7. POST-MDA ACTIVITIES
7.1 Organisation of Sample Survey for Assessing Drug Coverage and Consumption
Refer Chapter 7 on independent assessment
7.2 Conduct Post-MDA Review at Subcentre / PHC / Ward / Municipal Level to Highlight
the Strengths / Weaknesses in Implementation of MDA in order to Identify Village /
Street where the Drug Administration Coverage is Less and Take Appropriate
Action for Improving the Coverage
This is to be done within a period of 15 days after MDA.
7.3 Consolidation and Submission of Reports by PHC / Municipality to District
Headquarters along with Review Remarks
This is to be done within a period of 20 days after MDA.
7.4 Consolidation of PHC / Municipal Reports at District Headquarters and Review of
MDA by the 3rd Meeting of District-Level Coordination Committee and Record the
Committee‟s Observations
This is mainly done to evaluate the coverage levels and to identify the field problems which
should be recorded so that during next round, solutions must be identified to overcome the
same. This is to be done within 30 days after MDA.
7.5 Submission of Final Report to the State Programme Officer with Copy Forwarded to
the Directorate of National Vector Borne Disease Control Programme along with the
Remarks of the District Coordination Committee

27
The final report incorporating the percentage of coverage of drug consumption as per the
reports of drug administrators, consumption coverage as per sample assessment survey, the
quantity of drugs utilized, results of side reaction survey and IEC activity, including the funds
utilised and the funding sources, etc. are to be submitted within 30 days after MDA. The
proformae are given at Annex. 3.2.
8. MONITORING AND EVALUATION
Monitoring and evaluation is an integral component of any programme or campaign as there is a
need for:
demonstrating that particular intervention, medium reached and served its purpose;
obtaining guidance for programme decisions;
Determining whether improvements in health outcomes are causally linked to a given
intervention or a given behavioural change.
In other words, the knowledge of what works at each level of implementation could
provide support for continuing and improving useful interventions and discontinuing and
reallocating resources non-viable ones.
The programme or initiative can be evaluated at one or more levels: process, outcome,
impact.
8.1 Process evaluation
The main objective of process evaluation would be assessment of all programme inputs,
activities, stakeholder reactions.
8.2 Outcome evaluation
The main objective for outcome evaluation would be assessment of Campaign/Mission
approach on target behaviours.
8.3 Impact evaluation
The main objective of impact evaluation would be assessment of:
changes in mf rate
Changes in number of hydrocele cases and alleviation of suffering by monitoring
increased number of patients following foot care and reporting reduced number of
acute attacks.
8.4 Details of Concurrent and Consecutive Evaluation
1. Concurrent evaluation of the BCC campaign at each level of implementation may be
done through central/state/district observers at different levels as shown below:
Observers Level of evaluation
Central team State/District/city/town/Block/Subcentre/village
State District/city/town/Block/Subcentre/village
District Block/Town/Subcentre/village

28
This evaluation may be scheduled simultaneously with implementation of various
activities under the campaign.
2. Stakeholder interviews: Assessment of reactions, participation of inter-sectoral partner
organizations may be undertaken at each level of campaign implementation.
3. Consecutive evaluation/independent appraisal by Independent Institutions may be
scheduled after submission of the above-mentioned concurrent evaluation reports by
different observers and compilation of a comprehensive report on implementation of
various activities (independent assessment described in separate chapter).
4. Monitoring and Evaluation Indicators need to be built on:
(a) (input indicators) - Research, plans, resources, supplies, staff, etc.
(b) (output indicators) – Advocacy, Inter-sectoral collaboration, Social mobilization and
communication activities
(c) (outcome indicators) – Increased compliance; increased number of patients following
foot care (on the previous day of the survey)
8.5 Monitoring of Implementation
Monitoring of implementation is a vital element in programme management that enables us to
gauge the success of the strategy for elimination of lymphatic filariasis. Monitoring
encompasses the following functions:
i Assist programme managers at the National and State levels to achieve the
programme objectives and goals;
ii Assist programme managers to assess the current status of the programme; and
iii Assist programme managers to assess the impact of interventions

29
9. PROFORMA FOR MAINTAINING REGISTERS AT DIFFERENT LEVELS
MDA-1
Village Level
Details of Mass Drug Administration at Village
Name of Village________________ Name of Subcentre ________________
Name of PHC ________________ Round _____ Date of reporting___________
Sl
.
N
o.
Na
me
of
Hea
d of
Fam
ily
Consu
mption
of drug
in family
Age
(years)
Sex
(M/F)
No. of 100
mg DEC
tablets
administer
ed
No. of
400 mg
Albenda
zole
Tablets
administ
ered
**Code for
swallowing
the drug or
reasons for
not taking
the
drug(Use
Code i.e.T/
P/Y/S/H/A/
R/L/O)
Date of
drug
admini
stration
Reactions, if
any*** (Code)
Names of all the members of family to be entered as maintained in Family Register and
the **code for swallowing the drug in the presence of Drug Administrator or the code for
not taking the drug may be given as follows against each family member:
T= swallowed the drug in the presence of drug administrator and the code for not taking the
drug: P=Pregnant, Y=Children below two years of age, S= seriously sick, H= Handed over the
drug to the family member, A= Absent, R= Refused, L= Locked House, O= Other reasons
(Specify),
*** Code for side effects of drug: F= Fever, H= Headache, B= Body pains, N= Nausea, V=
Vomiting, O= others (specify)
Note= The balance tablets may be returned to PHC after completion of MDA (i.e. after
mopping up operations) with details of tablets received, tablets consumed and closing
balance..

30
MDA-2
PHC Level:
Details of Mass Drug Administration at PHC
Name of PHC ________________Name of District ________________
Round ______________ Date of reporting _________________
S.No. Name of
Subcentre
Total
Population
*Eligible
Population
Populatio
n
covered
in MDA
No. of tablets
supplied
No. tablets
administered
Balance of
tablets
at PHC
DEC Alb. DEC Alb. DEC Alb.
Total
Eligible Population = Total population – Population excluded from drug therapy (Children below two years age,
pregnant women and very sick persons); Alb. = Albendazole

31
MDA-3
District Level:
Details of Mass Drug Administration at District
Name of District ________________Round ______________
Date of reporting _________________
Sl.No. Name
of PHC
Total
Population
*Eligible
population
Population
covered in
MDA
No. of tablets
supplied
No. tablets
administered
Balance of
tablets at
district
DEC Alb. DEC Alb. DEC Alb.
Total
Eligible Population = Total population – Population excluded from drug therapy (Children below two years age,
pregnant women and very sick persons); Alb. =Albendazole

32
MDA-4
State Level:
District-wise Mass Drug Administration in the state
S.No. Name
of
district
Total
Population
Eligible
population
Population
covered (%)
No. of tablets
supplied
No. tablets
administered
Balance of
tablets at
district
DEC Alb. DEC Alb. DEC Alb.
Total
MDA-5
Central Level:
State-wise Programme of MDA
Sl.
No.
Name of
state/UT
No. of
MDA
districts
Total
populatio
n of MDA
districts
Eligible
population
No. of tablets
supplied
No. tablets
administered
Balance
at state
DEC Alb. DEC Alb. DEC Alb.
10. FORMATS FOR REPORTING AT DIFFERENT LEVELS
Planning and implementation of any disease control programme depends on information
support. Information is derived from data and hence the quality of information depends on how
the data are collected and the nature of the “instrument” employed in the collection procedure.
Therefore, it is essential to develop appropriate formats for data capturing. Design of the forms
to be used for recording data depends on the operational issues that need to be addressed.
The following formats will be used during the MDA campaign:
MDA1 to MDA 5 give details of MDA forms to be used at different levels for making
records starting from village/ward level to state level. The formats to be filled by the drug
administrators and he/she will submit it to health workers of his/her area. The Roadmap of MDA
activities is given at Annex. 3.1. The consolidated data formats to be submitted by the
State/District are given at Annex.3.2.
Guidelines for formation of State Task Force and State Technical Advisory Committee
are given at Annex. 3.3

33
Annex. 3.1
Roadmap for Preparatory Activities of MDA 20____
S.
No
Type of activity Period Planned
dates
Actual
dates
1 States to send indent for drugs requirement January/ 1 year before MDA
2 Conduct training for Trainers (District level Officers) 150 days prior to MDA
3 Conduct meeting of National Task Force under the
chairmanship of DGHS, Govt. of India.
120 days prior to MDA
4 Conduct State Level Task Force meeting under the
chairmanship of HFM
90 days prior to MDA
5 Conduct State Level Technical Advisory Committee
meeting under the chairmanship of DG/DHS
90 days prior to MDA
6 NVBDCP to send indent for drug requirement following
tender formalities and to procure DEC
120 days prior to MDA
7 Mapping in selected districts 120 days prior to MDA
8 Conduct 1st District coordination committee meeting 90 days prior to MDA
9 Conduct advocacy/ sensitisation workshop to district
officials/NGOs
60 days prior to MDA
10 Conduct 1st press meet/media flash 60 days in advance
11 Organise district level training for medical / health
officials
45 days in advance
12 Preparation of village/ward level micro plan 30 days prior to MDA
13 Review of micro plans at district. 15 days in advance
14 Conduct 2nd
District Coordination Committee meeting 15 days in advance
15 2nd
press meet/media flash 15 days prior to MDA
16 Complete the baseline data collection 15days prior advance
17 Conduct training to paramedical staff 30 day prior to MDA
18 Conduct training to drug providers 15 days prior to MDA
19 Carryout Inter-personal communication & update
enumeration
One week prior to MDA
20 Carry out IEC activities 45 days in advance and
continue till MDA
21 Conduct subcentre level leaders meeting 5 days prior to MDA
22 Distribute the drugs to the villages One week prior to MDA
23 Conduct workshop for medical practitioners 15 days prior to MDA
24 Drug administration day (MDA) 0 Day
25 Carry out mop up 2 Days
26 Organise supervision 0 to 2 day mopping up
operation
27 Position the rapid response teams for treating drug
reactions, if any
From day 1 to day 4 after
drug administration is over
28 Organise sample surveys to assess actual drug
compliance
Within 14 days of MDA
29 Conduct post-MDA review by subcentre / PHC /
Municipality
Within 15 days after MDA
30 Consolidate and submit to Dist. Hqrs. Within 20 days after MDA
31 Centre to conduct independent assessment on MDA Within 20 days after MDA
32 Review of the district consolidated report by District.
Coordination Committee in its 3rd Meeting
With in 25 days after MDA
33 Submission of final report on MDA by states Within 30 days after MDA.
34 Consolidation of final report at central level &
dissemination
Within 90 days after MDA

34
Annex. 3.2 Table 1: Update on the distribution of Lymphatic Filariasis: Year 200…. (To be compiled and sent by the State Programme Officer to Dte. NVBDCP, Delhi) State:_________________________ Population:___________________ Total No. of districts:_______________________ No. of disease cases: ______________________ (Lymphatic Filariasis)
Endemic District Non-endemic District Unsurveyed District
Sl. No
Name of the
district
Population Sl. No
Name of the district
Population Sl. No
Name of the district
Population
Total= Total= Total=
Note: (i) 2001 census population may be given or latest health enumeration data (ii) Year of survey may be given in parentheses after the name of district

35
Table 2: Survey of Sentinel and Spot Check Sites in MDA District: Year 20_____
Name of MDA District:___________________________________________
Separate forms are to be filled for each district and a copy to be endorsed to the Dte. NVBDCP
Date(s) of MDA:
Sl.
No.
Particulars Name of
the site
Date of
survey
Date of
MDA in
the site
No. of
Persons
Examined
No.
+ve
for Mf
Mf
Rate
(%)
No. +ve
for
Disease
Disease
Rate (%)
1 Sentinel
(Rural)
2 Sentinel
(Rural)
3 Sentinel
(Rural)
4 Sentinel
(Urban)
Sentinel sites sub Total (A)
1 Sentinel
(Rural)
2 Sentinel
(Rural)
3 Sentinel
(Rural)
4 Sentinel
(Urban)
Spot-Check Sites Sub Total (B)
Grand Total (A+B)
N.B. (i)The denominator for calculating Mf rate and Disease rate is same

36
Table 3: Mass Drug Administration (MDA) Coverage: Year 200….
Table 4: Training of Health Staff for ELF (Elimination of lymphatic filariasis) during Year 20_____
* „No. of staff sanctioned‟ (in the three columns of Table-4) should reflect the staff of Health and other sectors required to be trained for ELF ** No. of Lab. Technicians trained in LF microscopy may be reflected under MDA column. The rows under each administrative level (1, 2, 3 …) should reflect broad categories of officers/staff like state officials, district officials, medical officers, biologists, inspectors, supervisors, technicians, peripheral workers, volunteers, etc. in the respective administrative level
Name of the District
Date (s) of MDA
Total Population
of the district
Eligible Population
for MDA
No. of people receiv-ed Drug
% people received drug as
per records
% people actually
consumed drug as per field
investigation
No.
courses
organized
No. staff
sanctioned*
No.
vacant
positions
No. staff
trained
No.
courses
organized
No. staff
sanctioned*
No.
vacant
positions
No. staff
trained
No.
courses
organized
No. staff
sanctioned*
No.
vacant
positions
No. staff
trained
1.________
2.________
3.________
Total=
1.________
2.________
3.________
Total=
1.________
2.________
3.________
Total=
1.________
2.________
3.________
Total=
1.________
2.________
3.________
Total=
District level
Administrative
level
MDA Morbidity Management Both MDA & Morbidity Management
State level
CHC level
PHC level
Grand total
Lab.
Technicians **

37
Table 5: Health infrastructure available with trained health staff to manage Lymphoedema patients
during Year 20____
Name of health care
No. of centres with skilled
staff
No. of filaria patients
managed
No. of filaria hydrocele operations undertaken in the ELF
State Level
District Level
CHC Level
PHC Level
Subcentre Level
Note: The „No. of centres with skilled staff‟ should include the following: State level – State level training centres, Medical Colleges, Research institutions, etc., District level –Training centres, Medical Colleges, Research institutions, etc. , CHC/PHC & Subcentre levels–Training centres and other institutions.
Table 6: IEC/BCC Campaign for MDA: Year 20___
District: ________________________
Materials
No. Cost (in Rs.)
Activities No. Cost (in Rs.)
Banner Processions
Handbills Group Meetings
Posters Melas
Identification Cards Radio Talks
Cinema Slides Drum beating
Newspaper Adv. Mike announcements
Doordarshan Skits & Nukkad plays
All India Radio Quiz programmes in schools
Cable TV Logistics including transportation
Video quickies Interpersonal communication
Telephone canvassing Any other (specify)
Cassette player
Any other (specify)
Table 7: Serious Adverse Experiences (SAE): Year 20_____
Name of District
No. of persons with SAE
Type of Reactions
Clinical outcome
Required Hospital
Care
Remarks
1 2 3 4 T
1= Fever, 2=Nausea/Vomiting/Headache, 3=Lymphoedema, etc., 4= Others (specify), T=Total

38
Table 8: Drug Requirements
Sl. No.
Inventory Summary DEC Albendazole (400 mg) 100 mg
1 How many tablets were in stock on 01.01.20z….
2 (a) How many tablets were received since 01.01.20….
(b) From which source(s) the tablets were received
3 How many tablets were used during MDA
4 How many tablets have been destroyed since 01.01.20….
5 How many tablets have been lost/stolen or damaged since 01.01.20….
6 How many tablets balance in stock as on …………
7 Please list each batch/lot of tablets remain in stock, the number of useable tablets per batch/lot and the corresponding expiry date.
8 How many more tablets are required for the next round.
Note: Calculation of drug requirements
(i) DEC 100 mg: 2.5 x Total population. The total requirement of DEC tablets of 100 mg should be as per this formula.
(ii) The requirement under item 8 may be given after deducting the balance shown under item 6. The name, designation and consignee’s address with postal pin code and telephone No. and fax No. along with quantity may be given ( The State Programme Officer should be the consignee for drugs preferably as it facilitates the distribution of drug)
Table 9: Statement of Funds Allotted and Utilised: Year 20_____.
Central Funds Sate Funds
Funds Allotted
with dates
Funds *Utilised
with dates
Balance of Funds as
on…..
Allocated with dates
Utilised* with dates
Balance as
on ….
RD State RD State RD State
IEC
Training
Other activity (specify)
Total
Give the list of organisations as the footnote to whom the funds were disbursed
Table 10: Line Listing of Filaria patients
Leg Hands Scrotum Breast Others
Time of
starting of
disfigurement
Period of
stay in
the
district
Date of
survey
Disease affected part
Sl.No
Name
of
patient
Name
of Head of
family &
address
VillagePopul
ation
Panc
hayatAge Sex

39
Table 11: Consolidated district report on Lymphoedema Morbidity Management and Hydrocele cases: 2004 to 2007
(The annual New Capture Format is adopted for 4 years)
District:__________________
Sl. No. Details 2004 2005 2006 2007
1 No. of LF cases line listed
2 No. of LF cases trained during this month for MM
3 Balance to be trained
4 No. trained LF cases following MM
5 No. of hydrocele cases line listed
6 No. ineligible for surgery
7 No. of hydrocele cases operated
8 Balance to be operated
Table 12: Details of DCC Meetings in 20____
Designation of Members Date of First DCC Meeting
Date of Second DCC Meeting
Date of Third DCC meeting
Table 13: Proposal for withdrawal of MDA if qualified
Sl. No.
Name of District Sample size as per ELF
Guidelines
No. of MDA Rounds
completed
Proposed dates of Assessment of mf
among 3000 children

40
Annex.3.3 DRAFT
TERMS OF REFERENCE FOR STATE TASK FORCE FOR ELIMINATION OF LYMPHATIC FILARIASIS
1. Need for State Task Force (STF)
In view of expansion of Mass Drug Administration (MDA) covering all the Lymphatic Filariasis
endemic districts in the state, it is necessary to review the programme to record its
achievements & drawbacks in the preceding year(s) in respect of financial, administrative and
technical components, which will enable the state to rationalize the inputs so that there would be
better implementation of the programme within the available resources effectively in the
succeeding years and to consolidate the achievements accrued by the cost-effective strategy.
2. Constitution of STF
The following members will constitute the STF
1. Minister of Health &FW - Chairperson
2. Chief Secretary - Vice Chairperson
3. Addl. Chief Secretary - Member
4. Health Secretary - Member
5. NRHM State Mission Director - Member
6. Secretary (Finance) - Member
7. Secretary (Tribal) - Member
8. Secretary (ICDS) - Member
9. Secretary (Social Welfare) - Member
10. Secretary (Irrigation) - Member
11. Secretary (Rural Development/ Panchayat Raj) - Member
12. Secretary (Agriculture) - Member
13. Secretary (Local Health Govt.) - Member
14. Secretary (Industry) - Member
15. Secretary (Forest) - Member
16. Secretary (Information) - Member
17. Secretary (Education) - Member
18. Director General of Health Services (State)/
Director of Health Services - Member
19. Regional Director (H&FW), Govt. of India - Member
20. State Programme Coordinator, NRHM - Member
21. State Programme Officer (Mal. & Fil. or VBD) - Member Secretary
(In the state where different programme officers are looking different vector borne
diseases such as Malaria, Filaria, Kala-azar, JE, Dengue and Chikungunya, all should
be invited)
Where the designated post mentioned above does not exist, the senior-most administrative
head of the concerned department will participate in the STF. The State Task Force can co-opt

41
members from the relevant public & private sectors including NGOs, CBOs, FBOs, Women-self
help groups, Youth Clubs etc. who are to be involved in intersectoral coordination.
3. Terms of Reference
The proposed Terms of Reference are:
To Review:
(i) Progress of Implementation: To review the progress and impact of MDA for
elimination of lymphatic filariasis in the state.
(ii) Policy Decisions: To suggest modifications for effective implementation in the state
policy decisions, wherever warranted, to resolve programme/policy issues of
administrative, financial and technical nature as and when required.
(iii) To spell responsibilities of various departments for their contribution and the
concerned departments should convey these responsibilities to ground level staff.
(iv) Budget: To decide/recommend/ensure the release of sufficient funds up to the
peripheral levels for elimination of lymphatic filariasis and reflect the same in the state
budget.
(v) Any other relevant matter pertaining to the programme
4. Frequency of STF Meetings
The STF may hold the first meeting 120 days before the proposed date of MDA and the second
meeting one month before MDA. The third meeting may be held one-and-a-half months after
MDA to review the performance. The recommendations made in each STF meeting will be
communicated to all the members with a copy endorsed to the Ministry of Health & Family
Welfare (GOI), Directorate General of Health Services (GOI) and Directorate of NVBDCP within
15 days of holding the meeting.
5. Follow-up Action of STF Recommendations
The Action Taken Report is to be submitted to Member-Secretary by the concerned
departments within a fortnight after receipt of STF recommendations or as per the time indicated
in the specific recommendation(s).
6. Background Material on ELF to be made available to STF Members along with the
meeting notice.
The background material listed under below may be provided to all the members so that they
get apprised about the salient aspects of the programme.
6.1 Strategy for the Elimination of Lymphatic Filariasis in India
The strategy being adopted by the country for ELF i.e. MDA for interruption of transmission and
morbidity management for disability alleviation may be described with the
modifications/innovations made in the state and the updated report need to be presented to STF
members.

42
6.2 Goal and Objectives
6.2.1 National Health Policy (2002) Goal:
To eliminate lymphatic filariasis from India by the year 2015.
6.2.2 Objectives:
(i) To reduce and eliminate transmission of LF by Mass Drug Administration of anti
filarial drugs (Diethycarbamazine Citrate (DEC) or DEC+Albendazole)
(ii) To reduce and prevent morbidity in affected persons
The goal and objectives will be achieved through the existing health services with
improved health care delivery system and enhanced activities by involving the NGOs, private
and public sectors. IEC for integrated vector borne diseases control approach will be
implemented through intersectoral cooperation and coordination.
6.3 Basic Principle of Strategy for the Single Dose Mass Drug Administration
(i) Interruption of disease transmission and
(ii) Treatment of problems associated with lymphoedema (disability prevention and
control)
During a large-scale treatment programme, the key to success is the ability of the
peripheral (village/subcentre) level team involved in MDA to communicate effectively with the
community. Once the mutual confidence is built-up, the communication with people becomes
easy and the treatment objectives and nature of possible reactions would be explained to them.
The success of the strategy also depends on the speed of control measures put forth in order to
prevent parasite becoming re-established within a stipulated period of time.
6.4 Mass Drug Administration
The Operational Guidelines for ELF has reiterated that in MDA, DEC is given to almost
everyone in the community except children under 2 years, pregnant women and very sick
patients. Everyone may be considered to be more or less equally exposed to the infection.
The single annual dose mass therapy with DEC tablets has been found to possess the
following advantages:
(i) It avoids the cost of a mass blood examination.
(ii) All members of the community receive treatment, nobody feels left out and compliance
is, therefore, enhanced
(iii) It is as effective as 12-day therapy for public health measure.
(iv) It has lesser side effects thus enhancing public compliance.
(v) It involves decreased delivery cost.
(vi) It does not require complex management infrastructure.
(vii) It can be integrated into the existing primary health care system for delivery and
compliance.

43
(viii) Single dose mass treatment annually in combination with other techniques had either
eliminated or markedly reduced the transmission of lymphatic filariasis in some
countries.
6.5 Side Effects of DEC
DEC is a safe drug, which has been in use in India for more than 50 years. However, DEC may
produce side reactions in a small proportion of population especially among those harbouring
infection (microfilaria in circulating blood), who are usually symptom less (apparently healthy).
The drug reactions may be of two kinds:
(a) Those due to drug itself (Pharmacological toxicity): Headache, anorexia, nausea,
abdominal pain, vomiting, dizziness, weakness or lethargy. These symptoms begin
within 1-2 hours of taking the drug and persist for a few hours.
(b) Those due to allergic reactions due to destruction of microfilaria and adult worms
(attributable to filaricidal action): fever, local inflammations around dead worms, pruritus.
These reactions are transitory and subside within two days which can be treated with
symptomatic therapy.
6.6 National Filaria Day (NFD)
Mass Drug Administration is to be observed on a single day as National Filaria Day. Besides
free drug distribution, there are additional inputs in the form of IEC, POL expenses, training,
monitoring and evaluation of the project. All the endemic States/UTs may observe NFD on a
commonly accepted day after mutual consultations and prior approval of Govt. of India.
6.7 MDA Data of the Preceding Year (s)
The Member-Secretary with the inputs may monitor MDA data of the preceding year(s) and
circulate to all the members at least a fortnight before the meeting along with meeting notice.
The information may be provided with relevant write-up.
The Member Secretary should also brief on the progress made in hydrocele operations
and target for ensuing years. In addition, the report should also include the demonstration and
publicizing the home based morbidity management for lymphoedema management and the
number of patients practicing it.

44
Annex.3.4
DRAFT
TERMS OF REFERENCE FOR STATE TECHNICAL ADVISORY COMMITTEE FOR
ELIMINATION OF LYMPHATIC FILARIASIS
1. Need for State Technical Advisory Committee (STAC)
In view of expansion of Mass Drug Administration (MDA) covering all the Lymphatic Filariasis
endemic districts in the state, it is necessary to review the programme to record its
achievements & drawbacks in the preceding year(s) in respect of technical, operational and
administrative components, which will enable the state and district programme managers to
augment the most feasible and cost-effective strategy so that there would be better
implementation of the programme within the available resources effectively in the succeeding
years and to consolidate the achievements by cost-effective measures.
2. Constitution of STAC
The following members will constitute the STAC:
1. Director General/Director of Health Services (State) Chairperson
2. Director of Medical Education & Research - Member
3. Director of Indian System of Medicine - Member
4. Director, State Health Education Bureau - Member
5. Prof. & HOD Pharmacology - Member
6. Prof. & HOD Medicine - Member
7. Prof. & HOD PSM - Member
8. Prof. & HOD Pediatrics - Member
9. Prof. & HOD Pharmacology - Member
10. Regional Director (H&FW), GoI - Member
11. President, Indian Medical Association, State Branch - Member
12. Nodal State Programme Manager (NRHM) - Member
13. State Programme Officer (Mal & Fil or VBD) - Member-Secretary
(In the state where different programme officers are looking different vector borne
diseases such as Malaria, Filaria, Kala-azar, JE, Dengue and Chikungunya, all should be
invited)
(The Director General of Health Services of the state will chair the STAC where such a post
exists and DHS will be a member while in other states, the DHS will chair the STAC. The State
TAC can co-opt other expert members representing organizations like ICMR, Medical Colleges,
mother NGOs, FBOs, CBOs, women - self help groups, youth club, etc).
3. Terms of Reference
The proposed Terms of Reference are:
(i) Review
(a) the administrative, financial and logistics for ELF at various levels,
(b) the functioning of the State and District Vector Borne Diseases Control Programme
Societies.

45
(c) to provide technical inputs for the effective implementation of elimination of
lymphatic filariasis and management of cases with filariasis
(ii) Capacity Building
(a) Review the technical guidelines and training material available and if any
modification is required need to be communicated to Dte. of NVBDCP, Delhi
(b) Training load & services i.e. training programmes organized or to be organized for
various categories of personnel – target (total personnel to be trained in the state in
respect of various categories separately) – achievement against each target.
(c) Capacity for organizing skill based training involving, Trainers at State and District
levels, MO-PHC, Paramedical Staff, Block Extension Educators (BEEs), Drug
Distributors, health volunteers, laboratory technicians, etc. – Review of quality of
training and developing of core trainers.
(iii) Logistics Assess the availability of DEC (to be supplied by GOI) and remedial drugs
and deployment of Rapid Response Teams to manage side effects of DEC.
(iv) Review the performance of the programme on drug compliance and methods to
improve actual compliance >85%.
(v) Assess the impact of MDA on microfilaria rate as per guidelines of ELF.
(vi) Assess the performance of morbidity management of lymphoedema cases and
review the augmentation of hydrocelectomies by the identified CHCs and Hospitals as
well as organization of special camps.
(vii) Review the MIS contents, frequency and methodology of reporting.
(viii) Review intersectoral coordination and review the efforts undertaken towards
IEC/Social mobilization and Public-private partnership
(ix) Review integrated vector control measures including personal prophylactic
measures, insecticide treated mosquito nets, larvivorous fish and environment and
minor engineering measures.
(x) Review the nature and extent of operational problems affecting the programme, as
well as financial and staffing constraints affecting drug compliance.
(xi) Any other relevant matter pertaining to MDA
4. Frequency of STAC Meetings
The STAC may hold the first meeting 90 days before MDA and the second meeting a fortnight
before MDA. The third meeting may be held one month after MDA to review the performance.
The recommendations made in each STAC meeting will be communicated to all the members
with a copy endorsed to Directorate of NVBDCP within 10 days of holding the meeting.
5. Follow-up Action of STAC Recommendations
The Action Taken Report is to be submitted to Member-Secretary by the concerned
departments within a fortnight after receipt of STAC recommendations.
6. Background Material: As given under STF may be provided to all the members so that
they get apprised about the salient aspects of the programme.

46
Implementation Of Disability Prevention & Management
In order to gain confidence of the community on MDA, the patients with filarial lymphoedema
and hydrocele have also to be taken care of. Under ELF programme, the two activities namely
management of filarial lymphoedema and management of hydrocele have to be emphasized.
Effective, simple and cheap techniques have now been available to minimize the suffering
caused by the acute and chronic manifestations of the disease. The management of filarial
lymphoedema and disability prevention can be achieved through cost-effective home-based
management and the hydrocele can be operated through the available standard surgical
methods.
1. LYMPHOEDEMA MANAGEMENT
Filaria patients with damaged lymphatic vessels often have more bacteria on the skin than
usual. The large number of bacteria on the skin, multiple skin lesions, slow lymph fluid
movement and the reduced ability of the lymph nodes to filter the bacteria cause inflammation
characteristic of an acute attack. Repeated bacterial infections precipitate frequent acute
attacks, which further damage the tiny lymphatic vessels in the skin, reducing their ability to
drain fluid. This vicious cycle continues, aggravating the condition of the patient.
The lymphoedema management involves the following components:
Washing,
Prevention and cure of entry lesions,
Elevation of the foot,
Exercise,
Wearing proper footwear,
Management of acute attacks.
1995
Detection and Management of lymphoedema has to be a continuous process need to be carried out throughout the year by the paramedical staff, closely monitored by the Medical Officers.
For prevention of disability, all the cases should be enlisted by the paramedical staff through the prescribed format following the standard guidelines for line listing as given in Chapter -2.
These lists should also be linked to the CHCs / Taluk hospital for surgical intervention of hydrocele.
4

47
5. WASHING
Good hygiene and treatment of entry lesions are important measures for managing
lymphoedema. The patients should be encouraged to practise skin care and hygiene.
2.1. Supplies needed: (i) Clean water at room temperature, (ii) Soap (least expensive soap
without perfume is usually the best), (iii) Basin, (iv) Chair or Stool, (v) Towel, (vi) Footwear
within easy reach.
2.2. Check skin for: (i) Entry lesions, including very small lesions between the toes that can
hardly be seen, (ii) Entry lesions between the toes may cause itching. Scratching can further
damage the skin and can provoke an acute attack; tell patients to avoid scratching, (iii) Toe nails
should be trimmed in such a way that the skin is not injured. Do not try to clean under the nails
with sharp objects as these can cause entry lesions.
It is important to check the skin every time the leg is washed because entry lesions allow
bacteria to enter the skin and this will cause acute attacks. If entry lesions are found, they
should be cleaned carefully.
2.3. Wash the leg: (i). Wet the leg with clean water at
room temperature. Do not use hot water to wash the
leg, (ii). Begin soaping at the highest point of swelling
(usually around the knee), (iii). Wash down the leg
towards the foot, (iv). Gently clean between all skin folds
and between the toes, preferably using a small cloth or
cotton swab, and paying particular attention to the entry
lesions. Brushes should not be used as they can
damage the skin, (v). Rinse with clean water, (vi).
Repeat this careful washing until the rinse water is clean,
(vii). Wash the other leg in the same way, even if it looks
normal.
2.4. Dry the skin: (i). Pat the area lightly with a clean
towel. Do not rub hard because this can cause damage
to the skin, (ii) Carefully dry between the toes and
between skin folds using a small cloth, gauze or cotton
swab. Wet areas between the toes, skin folds and entry
lesions promote bacterial and fungal growth leading to
frequent acute attacks.
3. PREVENTION AND CURE OF ENTRY LESIONS
3.1. Entry lesions are common in patients with lymphoedema and are most frequently found
between the toes and deep skin folds and around the toe nails. Entry lesions, such as wounds,
can also be found on the surface of the skin. Both fungi and bacteria can cause entry lesions.
Fungal infections frequently damage the skin and create entry lesions, especially between the
toes, and may cause itching. The entry lesions allow bacteria to enter the body through the skin
and this can cause acute attacks. Fungi and bacteria can cause bad odour.
Washing and drying should be done daily ideally both morning and at night
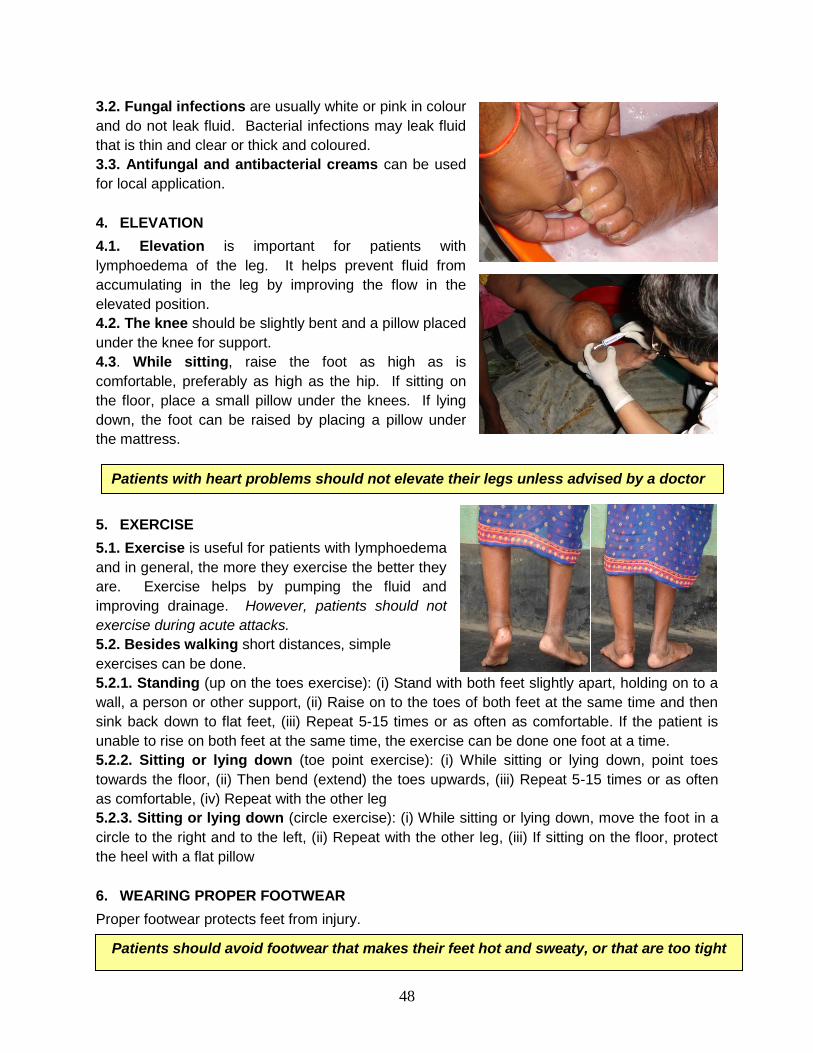
48
3.2. Fungal infections are usually white or pink in colour
and do not leak fluid. Bacterial infections may leak fluid
that is thin and clear or thick and coloured.
3.3. Antifungal and antibacterial creams can be used
for local application.
4. ELEVATION
4.1. Elevation is important for patients with
lymphoedema of the leg. It helps prevent fluid from
accumulating in the leg by improving the flow in the
elevated position.
4.2. The knee should be slightly bent and a pillow placed
under the knee for support.
4.3. While sitting, raise the foot as high as is
comfortable, preferably as high as the hip. If sitting on
the floor, place a small pillow under the knees. If lying
down, the foot can be raised by placing a pillow under
the mattress.
5. EXERCISE
5.1. Exercise is useful for patients with lymphoedema
and in general, the more they exercise the better they
are. Exercise helps by pumping the fluid and
improving drainage. However, patients should not
exercise during acute attacks.
5.2. Besides walking short distances, simple
exercises can be done.
5.2.1. Standing (up on the toes exercise): (i) Stand with both feet slightly apart, holding on to a
wall, a person or other support, (ii) Raise on to the toes of both feet at the same time and then
sink back down to flat feet, (iii) Repeat 5-15 times or as often as comfortable. If the patient is
unable to rise on both feet at the same time, the exercise can be done one foot at a time.
5.2.2. Sitting or lying down (toe point exercise): (i) While sitting or lying down, point toes
towards the floor, (ii) Then bend (extend) the toes upwards, (iii) Repeat 5-15 times or as often
as comfortable, (iv) Repeat with the other leg
5.2.3. Sitting or lying down (circle exercise): (i) While sitting or lying down, move the foot in a
circle to the right and to the left, (ii) Repeat with the other leg, (iii) If sitting on the floor, protect
the heel with a flat pillow
6. WEARING PROPER FOOTWEAR
Proper footwear protects feet from injury.
Patients should avoid footwear that makes their feet hot and sweaty, or that are too tight
Patients with heart problems should not elevate their legs unless advised by a doctor

49
7. MANAGEMENT OF AN ACUTE ATTACK
The reduction in the frequency of the acute attacks is an indication that the patient‟s condition is
improving. An acute attack is painful. The patient may complain of fever, nausea, headache and
soreness of the lymph glands. Most patients can easily care for their acute attack. The patient
should rest and elevate the leg comfortably as much as possible at home.
The following simple procedures can alleviate the symptoms;
1. A cloth soaked in water and placed around the leg can relieve pain. The leg can be
soaked in bucket of cold water.
2. The leg should be washed with soap and clean water but more gently and carefully.
3. After drying, antiseptic can be applied to the skin and medicated cream.
4. The patient should drink plenty of water
5. Paracetamol can be taken for fever every six hours until the fever lessens.
6. Oral antibiotics can shorten the attack and are recommended.
Patients, with any of the signs listed here, should be seen by a doctor: (i) Very high fever,
confusion, headache, drowsiness or vomiting, (ii) Fever, shaking, chills, or pain in the leg that
does not respond to treatment within 24 hours, (iii) Splitting of the skin because of rapid
increase in the size of the leg, (iv) Pus in the area affected by the acute attack.
The lymphoedema of lower limb is classified into three grades as given below:
Grade I lymphoedema: mostly pitting oedema; spontaneously reversible on elevation.
Grade II lymphoedema: mostly non-pitting oedema; not spontaneously reversible on elevation.
Grade III lymphoedema (elephantiasis): gross increase in volume in a Grade II
lymphoedema, with dermatosclerosis and papillomatous lesions.
The consolidated data formats to be submitted by the District are given below:
No exercise during an acute attack as, such exercise will be painful. Cold compress
will help the patient.

50
Proforma: MM- 1
Report on the monthly village-wise / ward-wise lymphoedema Morbidity Management
Report for the Month of_________________
Name of the Sub-centre/Ward:_____________PHC/ Municipality__________________
Details Name of the village / ward Number
1 2 3 4 5 6 7 8 9 Total
No. of LE cases
line-listed
No. of LE cases
trained during this
month for MM
Balance to be
trained
No. trained LE
cases following
MM
Note: The report has to be submitted by the Paramedical staff to MO PHC / MHO before 7th of
every month
LE= Lymphoedema, MM=Morbidity Management
Proforma: MM- 2
Report on the monthly Subcentre-wise / Ward-wise lymphoedema Morbidity Management
Report for the Month of ___________________
Name of the PHC / Municipality________________________________
Details Name of the Sub-centre / Ward number
1 2 3 4 5 6 7 8 9 Total
No. of LE cases
line-.listed
No. of LE cases
trained during this
month for MM
Balance to be
trained
No. trained LE
cases following MM
Note: The report has to be submitted by MO PHC / MHO the District Health Authorities.

51
Proforma: MM- 2a
Report on the monthly PHC-wise / Municipality-wise lymphoedema Morbidity
Management
Report for the Month of:____________________
Name of the District:
Details
Name of the PHC / Municipality
1 2 3 4 5 6 7 8 9 total
No. of LE cases line-listed
No. of LE cases trained during this month for MM
Balance to be trained
No. trained LE cases following MM
Note: The report has to be submitted by the District Health Authorities to State Directorate with
copy marked to NVBDC.
8. SURGICAL MANAGEMENT OF HYDROCELE DUE TO LYMPHATIC FILARIASIS
Hydrocele is one of the commonest manifestations seen in the endemic districts. Surgical
management of hydrocele not only gives great relief to the patients but also augments
community compliance for success of ELF in the country.
The first level peripheral health centres (PHCs) will be able to diagnose cases needing
surgical intervention, while most of the second level health centres (CHCs) have facilities for
undertaking hydrocelectomy. WHO brought out a publication on „Surgical Approaches to make
Urogenital Manifestations of Lymphatic Filariasis‟ with algorithm for management of scrotal
swellings, assessment of needs for conducting hydrocelectomy, etc., which is available on WHO
website.
The prevalence of hydrocele manifestations under each CHC is to be obtained and the
cases are to be line listed and a time schedule is to be prepared for augmenting surgical
facilities, training of surgeons, wherever needed and undertaking hydrocelectomy operations.
Besides CHCs, the private sector including NGOs are also to be involved for promoting the
surgical intervention for management of hydroceles. The calendar of activities with pragmatic
targets and the minimum financial inputs are to be worked out so that the Govt. of India and the
State Govt. may be able to consider for allocation of funds for this specific activity. The
hydrocelectomy has to be carried out through camps in the institutes like CHCs / Taluk
Hospitals / District Hospitals where the trained manpower and facilities are available. The
consolidated data formats to be submitted by the State/District are given below and Annex.4.1.

52
Proforma: MM- 3
Report on the monthly village-wise / ward-wise Hydrocele cases
Report for the Month of _________________
Name of the sub-centre/Ward:________________ PHC/ Municipality________________
Details Name of the village / ward Number
1 2 3 4 5 6 7 8 9 Tot
No. of
Hydrocele
cases line-listed
No. ineligible
for surgery
No. of
hydrocele
cases operated
Balance to be
operated
Note: The report has to be submitted by the Paramedical staff to MO PHC / MHO before 7th of
every month
Proforma: MM- 4
Report on the monthly PHC-wise / ward-wise Hydrocele cases
Report for the Month of _________________
Name of the PHC / Municipality:______________________________
Details Name of the PHC / Municipality
1 2 3 4 5 6 7 8 9 Total
No. of Hydrocele
cases line-listed
No. ineligible for
surgery
No. of hydrocele
cases operated
Balance to be
operated
Note: The report has to be submitted by the PHC / MHO to the District Health Authorities.

53
Proforma: MM- 5
Report on the monthly PHC-wise / Municipality-wise Hydrocele cases
Report for the Month of _______________________
Name of the District :_______________________
Details Name of the PHC / Municipality
1 2 3 4 5 6 7 8 9 Total
No. of Hydrocele
cases line-listed
No. ineligible for
surgery
No. of hydrocele
cases operated
Balance to be
operated
To be submitted by District Health Authorities to State Programme Officer with a
copy to NVBDC
Proforma: MM- 6
CHC / TALUK (THS) / DISTRICT HOSPITALS (DH) INFORMATION FOR SURGICAL
FACILITIES FOR HYDROCELE CASES
Report for the Month of:_____________________________
S.No. Name of the Hospital with
surgical facilities
No. of surgeons
trained
No. of surgeons
to be trained
Note: The report has to be submitted by the MO in-charge of CHCs / Municipal Hospitals/ THs /
DHs to District Health Authorities

54
Proforma: MM- 6a
CHC / TALUK (THS) / DISTRICT HOSPITALS (DH) INFORMATION FOR SURGICAL
FACILITIES FOR HYDROCELE CASES
Report For The Month of: ___________________
Name of the District : ____________________
S.No.
No. of CHCs
with surgical
facilities
No. of THs
DHs with
surgical
facilities
No. of
surgeons in
CHCs/
THs/DHs
No. of
surgeons
trained
No. of
surgeons to
be trained
Note: The report has to be submitted by the District Health Authorities to State Programme
officer with a copy marked to NVBDC
Proforma: MM- 7
DISTRICT-WISE INFORMATION FOR SURGICAL MANAGEMENT OF HYDROCELE CASES
DUE TO LYMPHATIC FILARIASIS
S.No. Name of
district
No. Hospitals
(including CHCs)
with Surgical
facilities
No. of
surgeo
ns
trained
No. of
surgeons
to be
trained
No.
hydrocelectomy
conducted
Note: The report has to be submitted by the State Programme Officer to the NVBDC

55
Annex. 4.1
DISTRICT-WISE INFORMATION OF STATE FOR SURGICAL MANAGEMENT OF
HYDROCELE CASES DUE TO LYMPHATIC FILARIASIS
S.No. Name of
district Population
No. of
PHC
No. of
CHCs
No. of CHCs
with surgical
facilities
No. of
surgeons in
CHCs
S.No.
Name
of
district
No. of
hydrocele
operations
conducted
per annum
in district
No. of surgeons
trained on
hydrocelectomy
at Dist.
Hospital/CHCs
No. of surgeons
requiring
training on
hydrocelectomy
Dist. Hospital
having facilities
for conducting
training for
hydrocelectomy

56
Behaviour Change Communication For Social Mobilization For ELF
1. NEED FOR BEHAVIOUR CHANGE COMMUNICATION (BCC)
Lymphatic Filariasis is a major public health problem in India. Filariasis causes irreversible
chronic manifestations, which results in social stigmatization, disability and immense economic
loss. In order to control this disabling disease, India is committed to achieve elimination of
lymphatic filariasis by year 2015 as reflected in the National Health Policy of India in the year
2002. In order to achieve the said National Health Policy Goal, a strategy for the elimination of
lymphatic filariasis has been in operation since year 2004. Since then, an Annual National
Filaria Day has been observed which includes Mass Drug Administration (MDA) with DEC
(diethylcarbamazine citrate) tablets in recommended dosage and morbidity management for
alleviation of the sufferings of the patients. However, in this drive, advocacy, inter-sectoral
convergence and social mobilization are extremely important to achieve the desired level of
compliance in the community and regular care of lymphoedema/hydrocele in patients. Co-
administration of DEC+Albendazole has been recommended by the National Task Force in its
meeting in 2006.
Information, Education and Communication (IEC) activities are oriented towards
increasing awareness among target communities/groups regarding MDA and encourage their
participation involving primarily development/distribution of IEC materials and undertaking
activities for disseminating information.
Behavior Change Communication (BCC) is a process of learning that empowers people
to take rational and informed decisions through appropriate knowledge; inculcates necessary
skills and optimism; facilitates and stimulates pertinent action through changed mindsets and
modified behaviour.
The process of BCC involves linkages between advocacy, inter-sectoral collaboration and
communication efforts at individual, family and societal levels thereby removing barriers that
restrict people from acting, developing enabling environments complemented by requisite
service delivery.
2. BCC CAMPAIGN GOAL
Integrated accelerated action through Behaviour Change Communication and delivery of
services for informed decision-making, initiation of individual and social change towards
elimination of Lymphatic Filariasis by 2015.
3. BCC OBJECTIVES
The specific objectives are as under:
Enhance awareness regarding source and transmission risk reduction, treatment,
availability of services at different levels.
Promote attitudinal and value changes among target audiences leading to informed
decisions, modified behaviour, desirable practices at individual and societal level.
5

57
Stimulate increased and sustained demand for quality prevention and care services and
optimal utilization of available health care services.
Build support for the programme across inter-sectoral partner organizations, influential
sectors of society (corporate sector, political representatives, social activists, media, civil
society organizations, etc.) and health care service providers and elicit commitment for
action.
Ensure availability of services.
4. BCC STRATEGY
The BCC campaign is to be undertaken across all levels of programme implementation up to
village for individual and social change. For ELF, the campaign needs to focus on:
Improvement of drugs consumption during the annual Mass Drug Administration at a
level of 85% or more in all endemic areas and sustain similar levels during subsequent
rounds for at least 5 to 7 years, unless the mf rate comes down to less than 1% and
absence of indigenous transmission.
Improvement in practicing home based morbidity management by the lymphodema
patients.
4.1 Important Aspects of BCC Campaign
4.1.1 Catalysts
The process of individual and social change starts with a catalyst/stimulus that may be external
or internal to the community. A catalyst represents the trigger that initiates dialogue about a
specific issue of concern to the community. Potential catalysts could include internal stimulus
(e.g. debility in a person), change agents e.g. National Govt Programmes/community
volunteers, Non-Governmental Organizations (NGOs)/Faith Based Organizations
(FBOs)/Community Based Organizations (CBOs)/Local Self-Government, Private health care
service providers, School children/Teachers, Opinion leaders, Policy makers, Elected
representatives, Media, innovation and availability of new technology (e.g. new drugs), policies
(e.g. legislations), mass media campaigns (e.g. messages designed to change individual
behaviour or promote collective action).
4.1.2 Role of Private Sectors
The private health sector represents a substantial resource, especially in urban areas. Private
medical practitioners can also be motivated through the professional organizations. These
organizations can also identify areas in which the support of private physicians could best be
utilised in mass drug administration and in morbidity (disability) management.
The private sector, industrial houses and private educational institutions are also
important groups for organizing mass treatment campaigns for their employees. Large
industries provide health services to their employees and their families and sometimes also
provide health services to the Industrial Township or rural area where they are located. An
inventory of private establishments will enhance planning for drug distribution.
Education department and social welfare departments can be potential partners in BCC
activities. Messages can be disseminated through students and anganwadi workers.

58
4.1.3 Role of NGOs, CBOs, FBOs, Panchayats and Village Health Sanitation Committees
Non-Governmental Organizations (NGOs), Community Based Organisations CBOs), Faith
Based Organisations (FBOs) and village health sanitation committees can play an important
role in LF elimination. These organisations should be invited to discussions when the annual
strategic plan is prepared, so that they can identify areas of interest for their participation, which
could be incorporated in the national plan. A list of NGOs, CBOs, and FBOs with the possible
areas of partnership should be prepared. The possible areas of partnership for an active role of
these include social mobilization towards MDA and disability prevention and management.
4.2 Community Dialogue
Social change is most likely to be sustainable if the individuals and communities most affected
own the process and content of communication. Community Dialogue as a sequential process
or a series of steps can take place within the community, some of them simultaneously, which
would lead to the solution of a shared problem. All steps however, may or may not happen in a
specific context or case. Broadly, the steps of community dialogue are:
a. Recognition of a problem: As a result of a catalyst, someone in the community
becomes aware of the problem and starts a discussion among them. For example, an
individual [Health Worker/ASHA/Fever Treatment Depot (FTD)/Drug Distribution Centre
(DDC)] or a group (NGO/FBO/CBO) discovers and discusses about LF in the area.
b. Identification and involvement of leaders and stakeholders: The problem is
discussed with family members and/or elders in the community. A health worker or an
opinion leader (Opinion leader/Religious leader/Multipurpose Health Worker
(MPW)/ASHA/Anganwadi worker/teacher/doctor) may be consulted and members of the
community may get together to meet informally to discuss the problem.
c. Clarification of perceptions: Discussions may lead to identifying causes for the
problem. Dialogue is necessary to create a common understanding. Only after
perceptions are clarified and different points of view rectified, the process moves forward
regarding how the problem needs to be solved.
d. Expression of individual and shared needs: A key element that community
programmes need to keep in mind is the involvement of individuals who are the most
disadvantaged in the community. Not everyone will experience the problem with the
same degree of severity. For example, better-off families with access to quality health
care may not face regular health problem or the threat of LF and therefore, may not
perceive it to be a problem for their individual families.
e. Vision of the Future: This represents an ideal picture of how a community wants to see
itself in the future with respect to a problem. It is important that all groups in the
community share this vision.
f. Assessment of Current Status: This tells the community where they stand in relation
to the problem today. Quantification of the problem gives an understanding of the size of
the problem. For example, number of LF cases. Qualitative assessment is also
necessary to understand the nature of the problem. For example, is there a remedy for
LF? What, how and why? Such assessment is important to set goals for action and
determine whether any progress is taking place.

59
g. Setting Objectives: Goal setting is the next step. All individuals/community must know
the goal and also its achievability, which creates high level of group motivation – a must
for people to take sufficient action to solve the problem.
h. Options for Action: The kinds of action to be taken to accomplish a health objective
with which everyone has agreed need to be defined. This implies identification of
resources both inside and outside the community as well as persons or groups that can
carry them out. Getting a consensus on action can lead to conflict between interest
groups or lack of commitment on the part of some groups. The leadership needs to
explore options and evaluate them from the standpoint of conflict occurrence and their
resolution.
i. Consensus on Action: Once a plan is at hand, a new process of getting consensus
among the community needs to take place. The more the community participates and
sees the proposed actions as theirs, the more likely they will take action.
j. Action Plan: A specific timetable for each activity needs to be developed that will help
the community to have clear deadlines and determine who does what and when certain
activities need to be taken to accomplish the desired goals.
4.3 Collective Action
The Collective Action involves the process of effectively executing the action plan and the
evaluation of its outcomes. The key action steps include:
a. Assignment of Responsibilities: To convert a plan into action, specific people must
take responsibility to accomplish specific tasks within specified time-period. Leaders
must ask volunteers or else assign tasks to individuals/community subgroups. It may be
necessary to create community task forces focused on specific goals.
b. Mobilization of Organizations: Existing organizations within and outside the
community could be involved to help. For example, community volunteers, civil society
organizations, schools. Communication through different media is an invaluable
resource for mobilizing community support and activity.
c. Implementation: This includes actual implementation and monitoring of the activities.
d. Outcomes: This refers to the actual results the community has been able to achieve
given the resources, organization and mobilization process specified by the action plan
and then carried out.
e. Participatory Evaluation: Comparison of outcomes with the shared vision and original
objectives is an important part of the process. For purposes of group motivation and
reward, it is important that most of the community participates in the evaluation of
process, so that lessons about what worked and why, could be shared throughout the
community. The four-pronged BCC strategies for ELF are Advocacy, Inter-sectoral convergence, Programme communication (IEC), Monitoring & Evaluation. Advocacy, social mobilization and programme communication initiatives begin with baseline situation analysis/research/identification of target (service takers, service providers) that identifies the levels of current knowledge, attitudes, beliefs, practices, points of resistance, barriers for

60
individual and collective action; approaches to improve same and motivate the target group; effective media options, type of communication, potentials for community participation and inter-sectoral collaboration in addition to ways for scaling up service provision. Regular monitoring and evaluation need to be in place for mid-course corrections.
5. ADVOCACY
Advocacy aims at developing enabling environment by
educating the political leaders, elected representatives,
planners, organized sectors, professional bodies, media for
building support, eliciting commitment and motivating them to
be advocates for a particular social development objective;
for instance, prevention and control of malaria and other
vector borne diseases. Thus, priorities are defined,
appropriate policies are framed, sufficient resources are
allocated and directions are provided to the implementers
thereby facilitating availability and accessibility of resources
to community.
6. INTER-SECTORAL CONVERGENCE
Inter-sectoral convergence is a planned process of
bringing together all inter-sectoral partners and the
community to determine felt needs and raise awareness of
and demand for certain intervention/s. Inter-sectoral
collaboration is extremely important, as there is a need for
propagating that the onus of implementation and acceptance
of programme interventions should be shared. This initiative is an integral part of commencing
„community dialogue‟ and „collective action‟. This would provide uniformity in diagnosis,
treatment and monitoring through a wider programme base and to maximize access to
appropriate and locally suited measures. Such collaboration is also expected to initiate effective
and sustained action towards community mobilization and initiation of behaviour change.
7. COMMUNICATION
Programme communication through different media (mass media, inter-personal
communication) for:
a. strengthening knowledge, beliefs, values, attitudes, confidence,
b. strengthening enabling environment,
c. strengthening reinforcement of knowledge, action through family, peers, teachers,
employers, health service providers, community leaders, etc.
Approaches
Implementing BCC through focused localized on-ground initiatives with supportive
umbrella campaign. That is, decentralizing to ensure local relevance and wide reach of
information. The Centre will provide leadership and develop core messages for mass

61
media and advocacy events. The states and districts need to base their specific
strategies on the core framework and messages, but encourage local adaptation and
innovation to reach target groups with appropriate communication tools.
Tackling issues at a local level and providing support for ELF initiatives in each region.
For example, customized solutions need to be created and provided for dealing with
local level problems related to MDA and morbidity management. The media route would
be focused local media options using the local language and idiom.
Providing a steady flow of information through appropriate media mix.
Focusing communication on key issues and community participation.
Publicizing achievements and success stories.
Sustaining a positive message in front of key audiences.
Countering negative publicity.
Promoting media responsibility through, for example, intensive campaign that would
feature "hot spot" prior to MDA. An interface to make information accessible, organize
and unify existing resources, establish links to partner organizations, create a forum for
partners and allies to exchange ideas, and constitute a rapid response mechanism to
broadcast/telecast problems and correct false rumors.
Identifying and engaging journalists/media persons covering social sector at different
levels of programme implementation.
Keeping in mind cultural and gender sensitivity while developing and delivering
messages. Addressing specific issues like stigma in case of Lymphatic Filariasis.
Targeting women and children as critical audience.
Ensuring continuity, which is critical. There is a need to be present continually as a
reminder.
Assigning higher weights before MDA.
Incorporating messages into the story line of popular soaps/serials.
In addition to building partnerships with civil society organizations and others, involving
professional advertising agencies, who understand the local social and cultural context.
Carrying out research.
Carrying out monitoring and evaluation
In general, the following structure is to be followed:
People Based Media:
Folk Media: Puppet Shows, Song & Drama, Street Play
Other Media: Road show, Rallies, Exhibitions, Human Chain,
Outreach activities: Peer Education, Group Discussion, Role play
Media Mass media Other media
Print News Papers, Magazine Posters, Stickers, Handbills, Hoardings
Electronic Television, Radio Video. Audio, Cinema Slides

62
Focused Localized on Ground Campaign through:
o Interpersonal Communication (IPC)
- Interpersonal communication works best when there is one-on-one contact
between the health worker and/or health communicator/health educator and the
person whose behaviour is sought to be changed to adopt new knowledge, life
skills and practices to ensure the welfare of their families and children.
- One-on-one contact facilitates comprehension of new concepts and
demonstration of new practices. Over a period of time, if done consistently, this
method can result in adoption of new practices on a sustainable basis.
- The tool kit for interpersonal communication includes aids that enable the
communicator/health worker to easily demonstrate any concept through visual
aids like manuals, demonstration devices such as role plays as well as such
materials as:
Flip Books, Flash cards: To be used by volunteers, health workers to counsel
audiences during home visits.
Stickers: For distribution among school children, shops, and other places to
remind people about the core themes on prevention and control of vector
borne diseases.
Badge, signboards with logo: For identification of those associated with the
MDA campaign, such as volunteers and other health workers,
Bag with logo: For volunteers/health workers to carry IPC material during
door to door visits.
Calendars: To promote the anti-malaria messages among influencers,
panchayat members, etc. with the key periods highlighted.
Mailers, gate folders and wall charts/logo stickers: For civil society
organizations, doctors, school teachers, chemists, DDCs/FTDs, community
volunteers.
Illustrated booklets (predominantly visual) with stories on prevention and
control of vector borne diseases especially for children.
o Folk performances: The folk performances are important on account of reach,
credibility, persuasiveness, ability to adapt performances to the message as well as
costs. The focus and venue of the show are to be selected with care, keeping in
mind the socio-cultural environment of the area and target audience.
- Scripts of the plays/shows should be sensitive to community, religious and social
norms.
- Troupes that are known to the audience of the region should be engaged.
- Training of the performers is a key aspect of communication through folk media.
Workshops have to be organized to sensitize them to the nature of the

63
messages, preferably through role play. Interactive sessions are necessary so as
to weave the messages into compelling and entertaining scripts.
- There should be element of interaction between audience and performers. The
performer should elicit feedback from the audience to involve them and also
gauge their level of interest and retain attention. Sometimes dummy performers
are present in the audience and at the appropriate moment, he/she may be
included in the play. Since the show is set in a village ambience and since the
performers are familiar with the rural setup, it lends a lot of credibility to the
messages being disseminated. In this way, the audience trusts the performers to
the extent that they are willing to take their advice on the product/service being
advertised. The scripts can be designed to explore every issue of concern like
prevention as well as curative steps.
- Successful performances are those whose scripts are flexible and open to on the
spot improvisations, to suit local dialects, tastes and preferences.
o ‘Melas’ and ‘Haats/Bazaars’
- Melas and Haats/Bazaars are prominent features of rural life. While
Haats/Bazaars refer to periodic markets held for trading, melas are usually more
for either religious or exhibition purpose. Both of these offer large audiences in a
short span of time, who are open and more receptive to information as they are
in a leisure mode.
- Haats/Bazaars are usually held once a week, while some others are held once in
two weeks. They are the focal centres of the economic, social and cultural life of
villagers.
- Melas are held periodically. Over 25,000 melas are held annually. However,
almost 80% are held for a day in conjunction with a festival and may have limited
importance in terms of information dissemination. However, many others last for
a week or more. The media Action plan therefore, needs to be drawn
accordingly.
- During these events, miking and live demonstration of morbidity management
could be arranged.
For localized campaign, emphasis may be given on: Socio-cultural, economic
characteristics of the target audience; local language, culture, costumes; featuring local
stories, anecdotes and people.
Miking and intensive interpersonal communication: Wherever feasible mobile
mike announcements shall be made with crisp messages on cause of disease,
benefits of MDA, consumption of drug by all the eligible population, date and timing
of MDA, location of booth and timing, etc. The miking shall be done one day before
and on the day of MDA. Additionally, intensive interpersonal communication should
be encouraged through community at the village level. Information should be given
on MDA, booth, side reactions.

64
NATIONAL FILARIA DAY : 11 NOVEMBER, 2006
OUR RESOLVE – FREEDOM FROM FILARIASIS
We will take single dose of DEC tablets on National Filaria Day - 11 November, 2006
to save ourselves from Filaria and ensure a healthy and happy future.
Filaria parasite is transmitted by the mosquitoes breeding in polluted water.
We shall avoid water collection in and around houses
and protect ourselves from mosquito bites by using insecticide treated bed nets.
Poster 2
Directorate of National Vector Borne Disease Control Programme,
Directorate General of Health Services, MOH&FW, Govt. of India 3
VARIOUS IEC PROTOTYPES
Directorate of National Vector Borne Disease Control Programme, Directorate General of Health Services, MOH&FW, Govt. of India
Our area is affected by Filaria. We will take single dose of DEC tablets on National Filaria Day - 11 November, 2006
to save ourselves from Filaria and ensure a healthy and happy fu ture.
Filaria parasite is transmitted by the mosquitoes breeding in po lluted water. We shall avoid water collection in and around houses
and protect ourselves from mosquito bites by using insecticide t reated bed nets.
NATIONAL FILARIA DAY: 11 NOVEMBER, 2006
Poster 1
OUR RESOLVE – FREEDOM FROM FILARIASIS
2

65
If you have lymphoedema/
elephantiasis these are the simple
things you should do:
Wash your legs and skin folds with
soap & water
Dry it with clean cloth.
Put anti bacterial or anti fungal
ointment locally, if required.
Keep your leg(s) in raised position
while sitting or sleeping.
Exercise anytime, anywhere
convenient. Raise your toes up and
down, rotate your foot from the ankle
clockwise and anticlockwise.
Walking is a good exercise.
Please Note:
Don‟t do the exercise if you have
high fever and acute infection as it
will be painful.
If you are a heart patient consult
your doctor before doing the
exercise and elevating your feet.
For more information visit your
nearest health centre
Wash your leg daily with
water and soap
Dry your leg with Clean cloth
Do exercise by rising up & down on toes
MORBIDITY MANAGEMENTELIMINATION
OF
LYMPHATIC FILARIASIS
OUR RESOLVE
FREEDOM FROM FILARIASIS
DIRECTORATE OF NATIONAL VECTOR
BORNE DISEASE CONTROL PROGRAMME
22,SHAMNATH MARG
DELHI – 110 054
MASS DRUG
ADMINISTRATION
ON
NATIONAL FILARIA DAY
11th November, 2006
Gateway Folder 1
63

66
What is Lymphatic Filariasis?
•Lymphatic Filariasis is a mosquito
borne parasitic disease commonly
known as Elephantiasis or Haathi Paon.
•The Parasite is thread like worm which
lives in lymphatic. The infection causes
lymph damage and dysfunction.
How is it spread?
•It is spread through mosquito bites.
•The adult worms produce millions of
baby worms (microfilariae), into blood
stream of affected person.
•While taking blood meal, mosquitoes
pick up microfilarae and transmit to
healthy persons.
What is symptom of Filariasis?
•Periodic fever or no symptoms are
recognized during initial period of
infection.
•Fever recurs after many years of
infection and.
•The frequency of acute attacks of fever
and pain, swelling of legs increase over
the years, leading to elephantiasis if
proper morbidity management is not
practiced.
What is Mass Drug Administration (MDA)?
MDA with annual single dose of
Diethylcarbamazine citrate (DEC) tablets is
recommended for elimination of lymphatic
filariasis in the affected areas.
Who should take DEC tablets?
Everyone living in filariasis affected area,
even if apparently healthy should take a
single dose of DEC tablets.
However, the following groups should not be
given the medicine :
•Children below two years of age,
•Pregnant women, &
•Seriously ill persons.
How often DEC tablets are to be taken?
DEC tablets are to be taken once a year
during Mass Drug Administration campaign
for 5-7 years consecutively.
DEC tablet should be taken as indicated
below:
2-5 years 1 tablet of 100 mg
6-14 years 2 tablets of 100 mg
15 years & above 3 tablets of 100 mg
Where DEC tablets would be available?
DEC tablets will be distributed free of
cost by health workers or volunteers
through house to house visits and
booths/camps at schools, work places,
health facilities, town centers, etc. during
MDA campaign on National Filaria Day
on November 11 2006.
How to take the DEC tablets?
DEC tablets should be taken with a glass
of water. DEC TABLETS SHOULD NOT
BE TAKEN ON EMPTY STOMACH.
Are there any side effects from the
medicine?
Persons having microfilaria in their blood,
may experience body ache, vomiting,
headache, dizziness, fever, rash,
itchiness after intake of DEC due to its
killing effect on microfilaria. These
symptoms are temporary and usually
disappear within a day. In case, the
symptoms persist, health worker/ health
centre should be immediately contacted.
Why should DEC tablets be taken on
National Filaria Day?
To ensure healthy future free from
filariasis for the children and community,
annual single dose of DEC tablets should
be taken for 5-7 consecutive years.
National Filaria Day
MASS DRUG ADMINISTRATION
64

67
FILARIA MESSAGES
vkvks feydj gkFkh ikWao ls ik,Wa NqVdkjkA Mh-bZ-lh- nok [kkdj rqe nks lkFk gekjkAA Mh-bZ-lh- nok dk ns[kks tknwA Qkbysfj;k ij ikvks dkcwAA Mh-bZ-lh- nok [kkus ls ikvks funkuA ojuk gkFkh ikWao ls rqe gks tkvksxs ijs’kkuAA gkFkh ikWao ls ikvks NqVdkjkA Mh-bZ-lh- nok [kkdj nks lkFk gekjkAA Mh-bZ-lh- nok [kkvks] ;g gS ukjk gekjkA rHkh rks gkFkh ikWao ls rqe ikvksxs NqVdkjkAA Mh-bZ-lh- nok [kkuk lHkhA gkFkh ikWao ls cpksxs rHkhAA gkFkh ikWao ls lcdks gS cpkuk ;g /;; gS gekjkA Mh-bZ-lh- nok [kkdj rqe+ gedks nks lgkjkAA ---------------------------------- lquks jss HkkbZ;ksa] lquks jh lf[k;ksa] Qkbysfj;k ls cpks vc rqeA Mh-bZ-lh- nok ds ns[kks xq.kAA mYVh] fljnnZ] cq[kkj ijs’kkuh lrk,WA vk’kk rqe lcdks ;g crkyk,WAA bl ijs’kkuh ls er ?kcjkukA Mh-bZ-lh- nok [kkrs tkukAA lf[k;ksa lquks&lqukss rqe ,d dgkuh gkFkh ikWao ij vc fot; gS ikuh Mh-bZ-lh- nok tks [kk yks rqe LoLFk 'kjhj ikvksxs rqeAA gkFk ls gkFk feykrs pyks Mh-bZ-lh- nok f[kykrs pyksAA ojuk gkFkh ikWao ls rqe gksxs ijs’kkuA fQj u ikvksxs dksbZ funkuAA ----------------------- lf[k;ksa lquks&lqukss rqe ,d dgkuh gkFkh ikWao ij vc fot; gS ikuh Mh-bZ-lh- nok tks fu;fer [kk;sxk iwjk thou LoLFk og jgs ik;sxkAA tks tks Mh-bZ-lh- nok fu;fer [kkrk gSA ogh iw.kZ mipkj ikrk gSAA ge vxzsath esa Qkbsysfj;k o fganh esa gkFkh ikWao dgrs gSAA bl ds bykt esa tks Mh-bZ-lh nok [kkrs gS] oks fujksx gksdj psSu ls th ikrs gSAA Mh-bZ-lh nok [kkrs tkvks gekjk lkFk fuHkkrs tkvks vkl&ikl dksbZ ejht gks rks vkdj ges crykvks mlds uothou ds fy, Mh-bZ-lh nok ysdj tkvks fu;e iwoZd mldks f[kykvks] mlds 'kjhj dks LoLFk cukvksA Hkkjr ljdkj us QkbZysfj;k@gkFkh ikWao dks tM+ ls feVkus dh dle [kkbZ gSA cpko gsrq Mh-bZ-lh nok vkidks LoLFk j[kus gsrq cukbZ gSAA
HkkbZ;ksa ftlus&ftlus Hkh ;g nok [kkbZ mlus gh fujksxh dk;k ikbZ gSAA eq¶r Mh-bZ-lh- feysxh rqedks [kkyh isV [kkuk er bldks ikWap lky ls uhps dks nsa ,d xksyh N% ls pkSng [kk¡, nks xksyh] vkSj iUnzg ds Åij dh ¿VksyhÀ rhu xksyh [kkuk getksyhAA ?kj&?kj ck¡Vs eq¶r nok [kkvks bls rks u ikvks lt+k fodykxark ls cpus ds fy, djks lksp fopkj Qkbysfj;k dh chekjh ds gS dbZ mipkj% ikuh lkcqu ls djks /kqykbZ fQj lkQ diM+s ls iksasN ysuk HkkbZ djuk FkksM+k rqe O;k;ke rc ikvksxs cgqr vkjke iSj Åij mBk dj j[kks izfrfnu nok ysi yxkdj j[kks QVs ?kko dks er [kqtykvks laØe.k dks nwj Hkxkvks lans’k ;g Hkh QSykuk gekjk Mh-bZ-lh- djss Qkbysfj;k NqVdkjkAA gks vxj rqe LoLFk js HkbZ;k Qkbysfj;k ds ijthoh dh nwj djks js NbZ;k jkr esa [kwu dh tkWap vo’; djok,A rHkh rks lc Qkbysfj;k ls eqfDr ik,AA vxj Mh-bZ-lh- dk lsou djksxs lHkh vkus okys oa’kksa dks Qkbysfj;k ls eqDr j[kksxs rHkh HkkbZ cfgu lquks js ckck lcdks ;g lans’k lqukuk Mh-bZ-lh- xksyh lHkh dks f[kykuk vkSj Qkbysfj;k ls eqfDr ikuk vkSjr enZ lquks js lHkh Mh-bZ-lh- dh xksyh [kkuk rqe lHkh ojuk ns[kksxs nq"ifj.kke gkFkh ikWa¡¡o gksus ij :d tk,xsa lc dke dkSM+h c<+s rks oa’k Fke tk, vkSj fcuk 'kknh fcfV;k nq[k ik, gkFk ls gkFk feykrs pyks Mh-bZ-lh- dh xksyh f[kykrs pyks Mh-bZ-lh- nok [kk ys HkbZ;k QkbZysfj;k dh nwj j[kks rqe NbZ;k¡

68
mYVh isVnnZ feryh lrk, MkDVj rqedks vf/kd le>k, Mh-bZ-lh- ds lsou ls dhM+s ejrs gSa rHkh ;g y{.k fn[krs gSa rki nks fnu ls vf/kd gks tkuk tkWap dsUnz rqe tYnh tkuk vkSj fcYdqy u rqe ?kcjkuk D;ksafd Qkbysfj;k ls NqVdkjk tks gS ikuk {kf.kd tfVyrk esa Q¡l tkvks rqe fpfdRlh; lqfo/kk ikvksxs rqe ?kj&?kj ckWVs eq¶r nokbZ bls vo’; [kk ysuk HkkbZ rki vxj u de gks ik,a
MkDVj ikl rqjUr gh tk,a vkSj rfud u ?kcjk,a Qkbysfj;k jksdFkke esa lg;ksx c<ka, LokLF; dehZ }kjk iwNs tkus okys iz’u% D;k vkids vkl&iM+ksl esa fdlh ds gkFk&ik¡o esa QksVks tSlh lwtu gS\ D;k fdlh dks bl izdkj dh lwtu esa nnZ gksrk gS\ D;k fdlh iq:"k ds dkSM+h ¼Qksrs½ lwts gSa\ D;k fdlh O;fDr ds lwts vaxksa esa ykyiu gS ;k ckj&ckj cq[kkj vkrk gSA

69
Monitoring & Evaluation Of Impact Of Programme
Monitoring and Evaluation of the programme is an inbuilt component of the programme to
assess the impact of the programme as well as to take evidence based decision to withdraw
MDA. Epidemiological evaluation focusing on the infection will be useful. For epidemiological
evaluation, parasitological surveys in human population before and after the intervention
covering certain proportion of population have to be carried out in selected villages / wards.
Distribution of filariasis is known to be clustered and therefore selection of villages for impact
assessment should cover representative samples from different clusters within a given district.
Sentinel sites (fixed) and random sites (spot-check) are to be selected as per the guidelines
given below:
The decision to stop MDA should be based not just on the number of MDA rounds
completed but on careful monitoring and strong evidence for cessation of transmission. The
objective of MDA is to interrupt transmission by reducing the level of microfilaraemia in infected
individuals to such an extent that the potential for transmission is reduced to levels where no
new transmission could occur.
1. APPROACH
Impact evaluation to verify absence of transmission can be done by assessing the infection in
children who are born after the introduction of intervention. Before examining this, the reduction
in mf prevalence can be verified and when it reaches below 1% prevalence, absence of
transmission can be checked. The steps involved in epidemiological evaluation include:
Step 1: Collect baseline data from sentinel sites (three villages and one ward) with equal
number of spot check sites
Step 2: Repeat microfilaraemia survey in the sentinel sites prior to subsequent round of MDA
and in equal number of spot check sites selected newly every survey.
Step 3: Before fifth round of MDA screen all children in the age class 2-4 years for antigenaemia
in addition to community mf survey covering the sample size as given in Step-5 & 6.
Step 4: If mf prevalence in sentinel and spot check sites reaches below 1% and antigenaemia
testing of children shows no positive, sample 5-10 additional sites of presumed high risk
for continued transmission. Repeat mf survey at community level and antigenaemia
survey among children 2-4 years old covering the sample size as given in Step-5 & 6.
Step 5: If mf prevalence shows below 1% and no antigenaemia prevalence among children,
select 30 clusters (village/ward) randomly in the district and examine 10 children in the
age class 2-4 years for antigenaemia.
6

70
Step 6: If none of the 300 children show positive for antigenaemia, then screen 3000 school
entrants (5 year old children) by Lot Quality Assurance Survey method. The survey has
to be continued till antigenaemia positive is detected or reach the target of 3000 children,
When none of the 3000 children show positive for antigenaemia, the MDA can be stopped.
2. SELECTION OF SITES [SENTINEL (FIXED) AND SPOT-CHECK (RANDOM)]
2.1 Sentinel (Fixed) Sites
Make a list of all PHCs in the district
Select 3 PHCs with the highest number of lymphoedema and hydrocele cases detected
during morbidity survey.
Select one subcentre each from the above three PHCs with the highest number of
cases.
Select one village each from the 3 subcentres with highest number of lymphoedema and
hydrocele cases.
In urban areas, select one municipality with highest number of lymphoedema and
hydrocele and select one ward from the selected municipality.
The 3 villages and one ward selected above will be the sentinel sites (fixed) for 5 years
or as long as MDA is implemented.
2.2 Spot-check (Random) Sites
Select 3 PHCs randomly from the list of PHCs irrespective of number of lymphoedema
and hydrocele cases.
Select one subcentre randomly from each of the 3 PHCs.
Select one village each from the three subcentres on a random basis.
For urban areas, select one municipality from which select one ward randomly.
Rounds of MDA
1 2 3 4 5
Mf and entomological surveys every year before subsequent rounds of MDA
Impact evaluation in Sentinel and Spot check sites
Mf prevalence & entomological survey (baseline)

71
The 3 villages and 1 ward selected randomly are spot check sites, which are to be changed
every year following the above method.
3. COLLECTION OF BLOOD SMEARS FOR MICROFILARAEMIA
Select the sites with more than 500 population so as to enable to collect at least 500 blood
smears and thus a minimum 4,000 blood smears from 4 sentinel and 4 random sites should be
collected.
3.1 Inform Community At Large and Seek their Cooperation
Visit the selected villages a few days before the date fixed for collection of blood smears.
Identify key village leaders and extension workers of other government departments
working in the village or volunteers such as ASHA/DDC/FTD or Anganwadi worker or
local NGOs and inform them about the purpose of the blood smear collection and the
date and time of the next visit. Seek their cooperation in informing the community and in
the collection of the blood smears.
Visit the identified patients with lymphoedema and hydrocele in the village and inform
them about morbidity management and hydrocelectomy.
Make arrangements for night halt in the village.
3.2 Collection of Blood Smears
Collect blood smears between 8.30 pm and 12 midnight.
Cover all households in the village / ward so that a minimum of 500 blood smears are
collected.
Cover all the individuals in the household, except children under two years of age.
REMEMBER
Blood smears should be collected in the night after 8.30 p.m. Seek community
participation by informing them in advance.
Blood smears can be collected by laboratory technicians from NFCP survey teams
and NFCP control units and other paramedical personnel.
Make necessary arrangements to transport the slides to the laboratory next
morning. If blood smears are made by laboratory technicians, these can be fixed
and stained in the field and examined in the laboratory after return of the survey
team.
Make a time schedule and ensure adequate supply of the items needed for the
preparation of the blood smears well in time.
3000 or more blood smears from the rural areas and 1000 or more blood smears
from the urban areas are expected from each district, every year before MDA.
60 to 80 man-hours will be required for the staining and examination of these
smears at the rate of 75 slides per person per day i.e. one technician will need
nearly two weeks to examine these smears. The period can be shortened by
assigning more technicians.

72
Record the name, age and address of the person in a register in serial order with a serial
number (Annex 6.1). The number should be noted on the slide. If there is more than one
team working in the village, prefix A or B or C….. to the slide number of each team. If the
survey is conducted in a village for more than one night, the slide number for the
subsequent nights will be given serially after the last slide number of the preceding night
blood smear (for example if Team A collects 52 blood smears on the first night, the slide
numbers will be A1, A2,…..A52 and the second night blood survey slides of the same
team will start from A53, A54, …. and so on)
Make sure that the smear is dried flat before putting the slide in the slide box.
3.3 Instruction for Examination of Blood Smears
The blood smears should be dehaemoglobinised within 24 hours of collection and fixed in acid-
alcohol (2 parts of con. HCl + 98 parts of methyl alcohol). If there is delay in
dehaemoglobinisation of blood smears, the blood smears may get auto-fixed and microscopic
examination will be difficult in the detection of mf. The dehaemoglobinised blood smears are
stained in JBB-1 for 40-60 seconds, washed in distilled water or buffer, dried and examined
under low power of compound microscope. The entire blood smear is to be examined
systematically from one end to the other end. The species of mf is confirmed under oil
immersion lens. The details are given in the Training Manual for LF Microscopists developed by
NVBDCP
3.4 Calculation of Parasitological Indices
No. of slides +ve for mf
Microfilaria rate (%): x 100
Total number of slides examined
Total number of microfilariae
Average mf density:
(Mean no. mf. /20 l blood) No. of +ve blood smears
No. of persons +ve for disease
Disease Rate (%): x 100
Total number of persons examined
Record the names and addresses of patients of lymphoedema and hydrocele for follow-
up regarding morbidity management and hydrocelectomy in case of the latter, if required.
3.5 Cross-checking of Blood Smears
All positive slides should be sent to the office of the Regional Director of Health and
Family Welfare for cross checking.
10% of the negative slides should be sent to the state level laboratory, which will send
2% of these slides to the office of the Regional Director of Health and Family Welfare
and examine the remaining 8%.

73
Form for Filaria night blood survey is given in Annex 6.1 and compilation of data for sentinel
and random (spot check) sites is given at Annex 4 of Chapter 4.
Microfilaria of Wuchereria bancrofti seen under Compound Microscope
Sh: Sheath, C.S.: Cephalic Space, N.R.: Nerve Ring, Ex.P.: Excretory Pore, Ex. C.:Excretory Cell, I.K.:
Innenkorper, G.C. I & G.C. 2-4: G Cells (so-called “genital cells”), A.P.: Anal Pore, R.B.C.: Red Blood Cells,
Neut.: Neutrophil, Eos.:Eosinophil, Lymph: Lymphocytes
4. ENTOMOLOGICAL DATA COLLECTION
From each sentinel and spot-check site, entomological data collection should be made from 10
catching stations spending 15 minutes in each catching station using flash light and aspirator
tube in the early morning between 6 a.m. and 10 a.m. All the female Culex quinquefasciatus
shall be dissected to find out the filarial infection. The following entomological parameters are to
be calculated for each selected village/ward.
From each site, minimum three collections at an interval of 10 days shall be carried out
before each round of MDA

74
4.1 Calculation of Entomological Indices:
No. of female C.quinquefasciatus collected
Ten Man-hour Vector density: X 10
No. of man-hours spent for mosquito collection
No. of mosquitoes +ve for any stage (L1/L2/L3 stages) of the parasite
Infection rate(%): X 100
No. of female vector mosquitoes dissected
No. of mosquitoes +ve for infective larvae (L3)
Infectivity rate: X 100
No. of female vector mosquitoes dissected
No. of infective larvae (L3) found
Mean number of L3/ infective mosquito:
No. of infective mosquitoes
L1: Stage 1 larva or sausage stage larva
L2: Stage 2 larva or pre-infective stage larva
L3: Stage 3 larva or infective stage larva
5. IMPORTANT QUESTIONS FOR MONITORING & EVALUATION
5.1 What is Implementation Unit (IU)?
It is an administrative unit in a country for which decision has been made to administer drugs to
entire population. In India, the Implementation Unit is a district. However, if some districts are
showing different ecogeography and some part is suspected to be free from LF, it should be
surveyed for LF cases followed by mf survey before it is brought under MDA or excluded from
MDA.
5.2 What should be monitored?
The selective monitoring of a few critical aspects of the programme is generally sufficient and
cost effective. While assessing interruption of transmission, it is most important to consider the
following aspects:
i The number of people who have ingested the drugs; and
ii The impact of MDA on prevalence of microfilaraemia
5.3 What information is required on LF status in IU?
The State Programme managers should categorize IUs into one of the three categories
described below:
i Endemic (Red): IUs where the average native population has an infection (mf)
rate of 1% or more;

75
ii Non-endemic (Green): IUs where either the ecological situation is not conducive
to transmission, e.g. altitude above 1600 meters, dry arid area, or where previous
surveys have indicated an infection (mf) rate below 1%; and
iii Uncertain (Grey): IUs where the LF status is still undetermined and where further
surveys are required to assess the infection rate.
5.4 How to assess the endemicity of LF in the IU?
Assessment of endemicity requires two steps:
i Assess how widespread the disease in the IU. This can be ascertained through
reviewing:
a. historical data;
b. unpublished and published data on filariasis;
c. report of medical and health services at the district level
d. hospital record on hydrocelectomy; and
e. the existence and use of local names for the terms like hydrocele and
lymphoedema
f. the review would make it possible to distinguish those areas in which LF is
likely to be endemic and which require further investigation.
ii Microfilaraemia survey by taking night blood slides from the targeted population.
5.5 What do you understand by the population at risk in the IU?
The area where indigenous transmission of microfilaria is established is known as filaria
endemic and the population living in the area is at risk. When MDA was launched in 2004, the
district as a whole was taken as the implementation unit for MDA. Any new district or part of
district if suspected to be filaria endemic, the night blood microfilaraemia surveys are to be
conducted and if Mf prevalence rate is found >1%, it should be considered for MDA and the
population covered under area of IU should be considered as population at risk. If part of
district is considered as population at risk, there should be significant data to prove other area
as non-endemic.
5.6 What is eligible population in the IU for MDA?
The entire population above two years of age is eligible population for MDA. However pregnant
women and severely ill persons should be excluded from the programme of MDA besides
children below 2 years of age.
5.7 What are impact monitoring indicators of MDA on microfilaraemia?
For effective monitoring of impact, the following need to be considered:
i Choice of diagnosis tool; and
ii Sampling and frequency of measurement
A number of diagnostic tools are currently available for monitoring the impact of MDA.
They are as follows:
i Night blood films for microfilaraemia;

76
ii Wuchereria bancrofti antigen detection tests that can be done any time of the day;
iii Filaria antibody detection tests; and
iv Polymerase Chain Reaction (PCR) techniques in humans and mosquitoes for
detection of filarial infection.
The night blood films for microfilaraemia and the antigen detection test have been standardized
and are currently recommended for use in the programme globally. The other diagnostic tests
are still being standardized and assessed for their interpretation in the field.
5.8 What are the limitations of the antigen detection tests?
i The antigen test is currently available only for W.bancrofti only.
ii It measures the presence of adult worm antigen; therefore, it can be a useful tool
to identify IUs with filarial infection in the community during the initial assessment
phase.
iii It is not very effective for measuring the impact of MDA on microfilaraemia as the
test may still be positive despite a significant reduction in levels of
microfilaraemia.
iv However, it can also be used to look for new infection in children born after the
start of MDA.
Keeping in view of limitations of antigen detection tests, the standard night blood film
examination remains the recommended diagnostic tool to assess the impact of MDA on
microfilaraemia.
5.9 How frequently the impact monitoring should be carried out?
It should be carried out before each round of MDA for examining the trend. However, it would be
sufficient to carry out before first, third and fifth rounds of MDA, then every two years to make
decision to withdraw MDA. Ideally when the frequency of health event is measured, it should be
representative of the geographical area. The ideal sample size for measuring microfilaraemia
levels of 1% or less, with a reasonable margin of error, would require testing of large number of
individuals. The alternative way of assessing the impact of MDA is through sentinel sites. Since
these sites are known to health workers responsible for implementing MDA in the area, bias
could occur. To avoid this, spot check sites need to be identified.
5.10 How many sentinel and spot check sites are needed for each implementation unit?
As per operational guidelines, 4 sentinel sites (three villages from rural areas and 1 ward from
urban area) should be identified on the basis of prevalence of higher number of disease cases
from each IU which will remain fixed for the IU till the goal of MDA is achieved. Similarly 4 spot
check sites (three villages from rural areas and 1 ward from urban area) should be identified
randomly irrespective of prevalence of disease cases from each area. Each site should have
population over 500 and if it is less than that the neighbouring area or hamlets may be included.
The national guidelines should be followed for the national programme to have
uniform monitoring.

77
5.11 How useful are sentinel sites in measurement of prevalence of lymphoedema and
hydrocele?
The presence of clinical cases of lymphoedema and hydrocele should be recorded in all sentinel
sites. Apart from assessing the trend in prevalence of lymphoedema and hydrocele in the
sentinel sites over the period of programme implementation, this information would also give an
indication of the disease burden in the IU. The prevalence of clinical signs in a given IU can be
calculated as indicated below in the example:
Sl.
No.
IU
(name)
Sentinel
site
No. of
individuals
examined
No. of
Lymph-
oedema
cases
Prevalence
%
No. of
males
examined
No. of
hydrocele
cases
Prevalence
%
The clinical signs are only surveyed in sentinel sites.
5.12 What are the criteria for stopping MDA?
It has also been briefly described in the beginning of this chapter. The following steps are
considered in deciding when to stop MDA:
Step (i):
Test all age groups in the sentinel sites and spot check sites for mf prevalence and mf
density, before first round, third and fifth round of MDA. Before fifth round of MDA, test
the children aged 2-4 years for antigenaemia with ICT cards.
If mf prevalence rate in the sentinel and spot check sites is below 1% and no child
aged 2-4 years is positive for antigenaemia using ICT cards, the criteria have been
met and so proceed to Step (ii) after completing 5th round. But if the criteria have not
been met, continue MDA and repeat Step (i) before round 7.
Step (ii):
Select 5-10 additional sites presumed to present a high risk of continued transmission.
If mf prevalence rate in all these sites sties is below 1% and no child aged 2-4 years is
positive for antigenaemia using ICT cards, the criteria have been met and so proceed
to Step (iii), following 5th round of MDA. But if criteria have not been met, continue
MDA and repeat step (i) before 7th round.
Step (iii):
Conduct a small community ICT survey of 300 children of 2-4 years of age in 30 high
risk areas; 30 cluster Lot quality Assurance Sampling ( LQAS). From each cluster,
sample 10 children at random. If no positive found, proceed to step (iv). If any positive
is found, continue MDA and repeat Step (i) before round 7th.
Step (iv):
o Conduct a large community ICT survey of 3000 school entrants using LQAS. Has any
true positive been found? If yes, repeat Step (i). If no, stop further round.

78
5.13 What is Lot Quality Assurance Sampling?
It is a sampling technique in which a sample of 30 clusters of 10 children each is chosen from
the highest risk areas. In the individuals cluster, one household in chosen at random and the
oldest child in the appropriate age range is selected from that household (or from next
household if there are no children in the first) and tested using ICT. If the selected child is
absent from the household, the second oldest child is selected, but note is taken of the
absentees. In case the proportion of absentees becomes high enough to warrant revisiting
households or necessitates some other procedure to minimize absentees bias, successive
households are selected unless 10 children in the appropriate age range have been tested. The
selection of only one household is proposed here to minimize the known effect of clustering in
families.
Conduct LQAS of ICT positivity of 3000 school children entrants covering the entire
implementation area or areas being assessed. If no true positive case is found, stop MDA. If
true positives are found, conduct 5th and 6th rounds and repeat the LQAS school survey as
described above before 7th round. If no true positives are found, stop MDA.
Flow chart showing the scheme of monitoring and evaluation
at IU / sub-district level (adapted from WHO M&E guidelines)
Sample
sentinel and
spot sites for
mf prevalence
and Ag status
Find < 1% mf
prevalence
AND no ICT
positive child
of 2-4 yrs old
Step 1
Continue MDA
Step 2
NO
Find < 1% mf
prevalence
AND no ICT
positive child
of 2-4 yrs old
Sample 5-10
additional sites
of presumed
high risk for
continued
transmission
Conduct 30
cluster- LQA-
CS ICT survey
of 300 children
2-4 yrs old in
high risk area
Step 3
Conduct large
community
LQA ICT
survey of 3000
school entrants
Find NO
positives
Step 4
Find NO
positives
STOP MDA
YES YES YES
NO YES
NO NO

79
Annex 6.1
FILARIA NIGHT BLOOD SURVEY FORM
PHC:__________________________ Village:_________________________
Date of screening:__________________
Sl.
No
.
Name of
Person
Name of
Head of
Household
Door
number
Age Sex Disease affected part Time of
starting of
disfigure-
ment
Period of
stay in
district
Blood smear
Leg Hands Scrotum Breast Others
Id No.
Result
(Mf
count)
1
2
3
4
5
6
7
8
9
Date of examination of blood smear:
Signature
(Name of the technician)

80
Independent Assessment Of MDA Implementation
1. INTRODUCTION
Monitoring of implementation is an inbuilt component of the programme (13 capture formats
given in Chapter 3). It has been observed in the past that actual drug consumption was lower
than the reported coverage by peripheral health workers/volunteers. As per the norm, the drugs
are to be consumed by the eligible population in the presence of drug administrators but on
many occasions, the drug was handed over to the family members for consumption later on. It
has been observed that a substantial proportion of community members do not consume the
drug. Therefore, it is important that the mid-term assessment shall be conducted by
independent team members who are not directly connected with MDA programme in the
selected area. The assessment shall be completed within 2 to 3 weeks of MDA so that the
community will be able to recall the events without memory lapse. Assessment of programme
implementation will be useful to make mid-term corrections as well as strengthening the
ongoing programme. All the MDA districts are included for the assessment.
2. OBJECTIVES
(i) To review the progress of activities of single dose DEC mass administration in the
selected districts.
(ii) To make independent assessment of the programme implementation with respect to
process and outcome indicators.
(iii) To recommend mid-course corrections and suggest necessary steps for further course
of action.
3. CONSTITUTION OF ASSESSMENT TEAMS
Team should be identified from the medical colleges/ research institutes like Malaria Research Centre, other ICMR institutions not directly connected to MDA.
A three member independent Assessment Team will be constituted for the selected endemic State/UT by Directorate of NVBDCP for Mid Term Appraisal of MDA from the identified institutions.
4. ASSESSMENT OF ACTIVITIES
(iv) Central level (NVBDCP/NICD/ICMR) regarding logistics, funds, trainers‟ training, etc
(v) Regional level (ROH&FW) regarding training, co-ordination for MDA activities
7

81
(vi) State level (20 States/UTs/) Macro planning, training of district level officers through
Medical Colleges, advocacy, flow of funds & supplies, etc.
(vii) Medical Colleges: Training of District level officers, advocacy, monitoring of side
effects of drugs in selected districts, selection of sentinel and random sites for
baseline/impact data, independent assessment.
(viii) District level (all MDA districts in each State/UT) planning, funds and logistics flow,
training, DCC activities, implementation, supervision, rapid response teams and
assessment
(ix) PHC level (3 PHCs in each selected district) planning, logistics, training,
implementation and supervision
(x) Urban level (one ward of the identified town) planning, logistics, training,
implementation and supervision
(xi) Peripheral level (A cluster of 30 households in one village in each of the 3 selected
subcentres and one ward in a town)
5. SELECTION PROCESS IN THE DISTRICTS
Four clusters (each cluster having 30 households) are to be selected comprising urban and rural
areas.
Classify the PHC low, medium and high on the basis of drug distribution coverage
From each category, select one PHC at random
From each PHC, select one village at random
Select one ward from medium coverage town
Select 30 household cluster in each village/ward
From each cluster of 30 households, information pertaining to all inmates of the
household to be collected.
On an average, 30 households may contain 150 or more inmates. The four cluster survey may
indicate information for 600 or more household members.
However, in the districts where the urban population is more than the rural population, the
distribution of the four clusters may be modified according to the proportion of urban to rural
population. For example, in Pondicherry, the urban population is about 60% and hence two
urban clusters and two rural clusters are to be selected. If the urban population in any UT is
100%, all the sites are to be selected in urban areas only.
6. COMPONENTS TO BE ASSESSED
6.1 Intra and Intersectoral Coordination
The qualitative, quantitative and frequency of intra and intersectoral coordination will be
assessed at central, state and districts, selected PHCs and villages/wards.
(i) Central Level
(ii) State Level

82
(iii) District Level
(iv) PHC Level (selected PHCs)
(v) Village/ward level (selected villages/wards)
6.2 Training
The training in respect of adequacy regarding number of participants and timing before MDA
may be assessed at the following levels:
(i) Trainers‟ Training imparted to Medical College Faculty and State officers by the Dte. of NVBDCP or any other organisation
(ii) MO PHC Training
(iii) Health Workers‟/Health Volunteers‟ Training
(iv) Lab Technicians‟ Training on LF Microscopy
(v) Drug Distributors‟ Training
6.3 Process Indicators
(i) Action Plans at State, District and PHC levels
The preparation and implementation of detailed action plans at different levels may be
assessed.
(ii) Epidemiological indices from Sentinel and Spot-check Villages/Ward
(a) Selection of sentinel and spot-check sites (b) Sample size and method of survey as per the guidelines (c) Epidemiological indices: Mf rate, Mf density, Disease rate and Entomological
(wherever available).
(iii) Line listing of lymphoedema/hydrocele cases
(a) Whether all the villages and towns covered in the survey
(a) Number of PHCs with population having indigenous LF cases
(b) Number of PHCs with population not having indigenous LF cases
(iv) Logistics of Drugs
(a) Demand of DEC and Albendazole as per population norm
(b) Supply and distribution of drugs in time and space
(c) Balance of drugs available at PHC, district and state levels after completion of MDA
(d) Physical verification of drugs on quality and shelf life
(e) Procedure followed for Quality Assurance of drugs
(v) IEC and social mobilisation
(a) Types and quantity of IEC materials distributed in the district

83
(b) Whether IEC material was printed in local language
(c) Advertisements in local press and other media
(d) Posters, banners, folders, handbills, etc. used in the programme.
(e) Whether interpersonal communication at village level has been adequately followed
(f) Group meetings in time and space
(g) Advocacy at different levels
(h) Any other innovative IEC programme (Specify)
6.4 Impact Indicators
The impact indicators are collected by the personnel involved in the collection of
baseline/impact data as described in Chapter-3. The impact assessment will be carried out in
the districts where baseline data was collected before taking up MDA. The impact indicators
cover the following parameters:
6.4.1. Epidemiological
Parasitological
Mf rate
Mf density
Disease rate (specify the rate of lymphoedema, hydrocele, etc.)
Entomological
Mosquito density
Infection rate
Infectivity rate
Mean number of L3/ infective larvae per infective mosquito
6.4.2. Operational
Social mobilization
Changes incorporated in IEC for treatment seeking behaviour of community for enhanced
consumption rate of DEC tablets.
Coverage and Compliance
The actual drug compliance is determined by interviewing about 600 family members in
each district following the sampling technique as indicated at point No. 5 as against the reported
coverage in the drug registers. The information is to be elicited in such a manner that the
community members will give the information without any apprehension / hesitation.
Management of Side Effects of Drugs:
(a) Whether community was made aware of transitory side effects especially among
infected persons
(b) Whether the side effects were properly recorded
(c) Whether symptomatic treatment was provided to individuals reporting side effects

84
(d) Proportion of mild and serious side effects, if any
(e) Whether serious side effects were immediately referred to the PHC for remedial
measures
Morbidity Management
(a) Community awareness on morbidity management methods
(b) Number of cases observing simple methods of foot hygiene in the villages under mid-
term assessment
(c) Impact of morbidity management
(d) Facilities for hydrocelectomy in the selected CHC areas/District Hqrs. and if so, the
number of hydrocelectomy operations conducted during the preceding 12 months
7. FINANCIAL ASPECTS
The Central funds received by the State/UT or the Societies for ELF from MOH&FW, Dte. of
NVBDCP and ROH&FW, timely release of these funds to the districts and judicial utilization of
funds by the districts will be assessed. The funds provided by the State/UT from their own
budget in cash and kind as well as inputs by public/private sector and NGOs, etc. are also be
covered.
7.1 Submission of Mid-Term Assessment Report
The assessment will have to be completed within 4 days in each district and the assessment
report along with recommendations fulfilling the objectives shall be submitted to the Dte. of
NVBDCP within 10 days after the completion of field visit.
The sample questionnaire for householders to assess drug compliance is given at
Annex.7.1

85
Annex 7.1
PROFORMA FOR ASSESSMENT OF MDA COMPLIANCE Record examination: Name:________________________________________
Village Sub-
centre PHC District
Name of Head of Family
Name of individual interviewed Age /Sex
No. of persons in the family Age in years
Sex
No. of DEC tablets (100 mg) given to each person
No. of Albendazole tablets given to person
The questionnaire should be highly discreet for extracting information on drug compliance. The Drug Administrator’s household register may be collected from PHC and carried to the village/ward for cross-checking the entries. The names of the family members and their age should be checked. The first request to the householder shall be: Interview of the householder: (ii) Physical verification of tablets: Please show me the anti-filarial tablets given to you by
the drug administrator.
(iii) Defaulters: (a).Why did the particular person (name the defaulter) not take the drugs? (b)
Did you persuade the defaulter to take drugs? (C) Did you help the drug administrator for drug compliance in your village or mohalla?
(iv) Drug Administrator: Do you have any reservations on drug administrator? If yes, please
specify. Did you swallow the tablets in the presence of Drug administrator? If no, why? Did the drug administrator explain to you about ELF and the details of transmission?
(v) Side Effects: Did you experience any side effect of drugs? If yes, did you get remedial
drug? Did you receive treatment for any ailment before experiencing side effects of drugs? (vi) IEC: When did you first hear about MDA and from whom? Did you read or see any
banner, poster, newspaper advertisement, handbill, mike announcement, drama, street play, etc. on MDA? If yes, which is the most effective one?
(a) Disease Cases: Do anyone of your family member or neighbour or person in your
village suffer from LF disease? If yes, name them? (b) Do you consult a qualified physician? If no, what are the reasons? (c) Record any other relevant information on MDA
Name & Signature of Investigator Date
No of 100 mg DEC given No. of DEC tablets recovered from the house
No of persons taken full dose Number taken partial dose No. not taken DEC
No of 400 mg Alb. given No. of Albendazole tablets recovered from the house
No of persons taken full dose Number taken partial dose No. not taken Alb.

86
Annex 7.2
District:------------------------------------ PHC:---------------------------------------- Village:-------------------------------------------------- Street: ------------------------------------
Date of drug distribution:.................... Date of survey:………………………. Collected by:………………..…………………...…………………….. Door No. ……………………………………….
Number of tablets recovered: Big………...….Small……….…….
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23
Big Small Big Small
1
2
3
4
5
6
7
8
9
¹Details of side reaction
Tre
atm
en
t
(G/P
)
If No, Reason for not
swallowing Type
1
Afte
r food
Dura
tion
(In d
ays)
COMPLIANCE/SIDE REACTION (ACTIVE) SURVEY
No.of tablets
Tre
atm
en
t
for o
ther
ailm
en
t
Sl.
No.Name Age
Sex
M/F
Received tablets
Codes: Headache (1); Fever (2); Dizziness (3); Fatigue (4); Nausea (5); Vomiting (6); Diarrhea (7); Abdominal pain (8);
Joint/muscle pain (9); Swelling of limb (10); Swelling of nodes/scrotum (11); Rash (12); Scrotal reaction (13); Presence of nodules (14).
Respo
nd
en
t
Y / N
No. tablets
Sid
e re
actio
n Y
/N
Details of side reaction
Passing
worms in
stool Y/N
If yes fro
m
who
m
In p
resen
ce
Sw
allo
wed Y
/N
If swallowedDid DD
Pers
ua
de
Expla
in

87
Annex: 7.3
Drug administrator:
Examine the family register:
How many tablets
Received/distributed/balance Verify the family register:
Received or not
Number of tablets received against each member
Correct dose
Interview with the household member (for self and other family members)
Did you receive
How many
Get back the balance drugs to confirm whether they consumed (partial/selective) or not
Side effects
Partial
Over/under dose
IEC – source of information
Awareness and acceptance (only head / responsible person of the family)
Name:
What is the source of information on MDA (list)?
1
2
3
4
5
6
Which is / are the most effective one(s) in the order ot priority?
1
2
3
4
5
Did any one suffer from LF disease?
Self:
Family member:
Community member (number, M/F)
Do you have any reservation about the drug distributor?
If yes specify:
Who in your opinion to be given the responsibility of DD?

88
Roles and Responsibilities Of Officers And Staff For MDA Campaign
The roles and responsibilities of different categories of officers and staff at various levels viz.
National Programme Headquarters, State Programme Headquarters, District Headquarters,
PHC/Town, Sub-centre and village/ward are given below. The duties are mentioned as general
guidelines, which may be adapted to rules and regulations of Govt. /Local Body.
1. RESPONSIBILITIES OF NATIONAL PROGRAMME HEADQUARTERS (DIRECTORATE
OF NATIONAL VECTOR BORNE DISEASE CONTROL PROGRAMME)
i Organising meeting of National level steering committee, National Task Force and
National Technical Advisory Committee. Constituting Expert Group for formulating
guidelines on various aspects of ELF and prepare national strategic plan for ELF.
ii Preparatory national workshop with involvement of State Programme Officers, NVBDCP,
NICD, ICMR and LF Experts and review meetings.
iii Technical guidance, monitoring and independent evaluation of ELF.
iv Formulating budget proposal for appropriate central funds for implementation of ELF in
the endemic states.
v Procurement of DEC and Albendazole and supply to endemic states/UTs.
vi Preparation/Updating of operational manual on ELF and circulation to all the endemic
states/UTs/Medical colleges.
vii Develop training modules/Learning Units on relevant aspects of ELF and develop a
national plan for training of manpower in ELF.
viii Develop prototypes on IEC with the help of media agencies and media experts and
circulate to the states/UTs for printing in local language.
ix Undertake advocacy for decision makers at national and state/regional levels.
x Plan operational research with the help of NICD, ICMR and other research institutions.
xi Monitor, assess and evaluate the programme on process and impact indicators regularly
to issue guidelines for corrective measures wherever warranted.
xii Identify teams consisting of physician, pharmacologists, epidemiologists and social
scientists for investigation in the field in the event of any report of adverse reactions.
xiii Collaborate with WHO, international/bilateral agencies, private & public sectors, NGOs,
other ministries, etc. on ELF and co-ordinate ELF activities between the states through
ROH&FWs and officers of Dte. of NVBDCP.
8

89
2. RESPONSIBILITIES OF STATE PROGRAMME HEADQUARTERS
The Nodal officer for Elimination of Lymphatic Filariasis of the State Health Deptt. has to
supervise the entire work of ELF in the State.
i. He will organize the drug procurement for the next round of MDA even before the MDA
dates are announced (usually in January)
a. Calculate the number of tablets required using the formula for DEC 100 mg tablets:
population updated based on the last available census x 2.5 Add 10% for unlisted
members of the community and for Albendazole 400 mg tablets: Population x 1and
10% for unlisted members of community.
b. Send the request for tablets under the PIP to Director NVBDCP, Delhi
c. When the drugs are received, store them at Headquarters or any other identified
stores till the date of MDA is announced.
d. Arrange to check the quality of drug & inform to centre about the result.
e. Arrange to distribute the drug to the peripheral areas sufficiently early before the
MDA
ii. Process for the release of funds for the ELF activities including MDA Programme from
State health Society to the District health Society to make the funds available to the
District programme officers and PHC medical officer and at grass roots.
iii. Start training activities as soon as the proposal has been approved and funds
sanctioned.
a. Prepare a training calendar for MOs, Paramedical staff and drug administrators
b. Conduct training for MOs at a venue convenient to the participants
c. At the end of the training, participants will be expected to be familiar with the basis
of the programme, their responsibilities and to develop further training at the
periphery for the paramedical staff, drug administrators and inform the community
leaders.
iv. Organize a STF meeting and STAC meeting as per schedule.
v. Issue instructions and ensure to Organize DCC meetings as per schedule
vi. Organize inter-sectoral meeting as per schedule
vii. Start BCC activities as soon as the funds are realized.
a. Choose the IEC channel that is most effective in the community (from the following
options – miking, street plays, skits and dramas, banners (cloth or digital),
hoardings, advertisements in local print media, TV spots in local cable network, All
India Radio and Doordarshan, slides in cinema theatres, pamphlets and leaflets).
Use celebrity endorsement for the programme wherever possible.
b. Follow the financial guidelines.
c. Ensure .that all IEC materials are distributed and displayed in the sites already
chosen well ahead of the MDA date and also ensure their proper dismantling and
return to Hqrs. for subsequent use and accountability.
viii. Start the mapping activities 120 days prior to MDA date.
ix. Choose the fixed sentinel sites

90
a. Choose 3 PHCs with highest number of disease cases.
b. Choose 3 subcentres with highest number of disease cases from among these
PHCs
c. Choose a village highest number of disease cases from each of these subcentres.
d. Choose an urban ward with the highest number of disease cases.
Chose the random (Spot-check) sites
a. Choose any 3 PHCs irrespective of disease status
b. Choose 3 subcentres within these PHCs irrespective of disease status
c. Choose any village from each of these subcentres irrespective of disease status.
d. Choose any urban ward at random irrespective of disease status.
x. Arrange to collect at least 500 smears from each of these sites (total 4000 or more
slides).
xi. The community should be made aware of this activity soliciting their cooperation using
village leaders‟ meetings and other BCC methods.
xii. Depute lab staff to conduct the night surveys and arrange for their examination at the
headquarters. Calculate the mf rate for each sentinel site. This is essential to
determine the success of the programme and should be completed well before the
MDA date. It will also serve as a benchmark for selecting BCC activities with particular
emphasis on vulnerable pockets.
xiii. Organize an entomological survey along with blood smear survey, which shall be
made from 10 catching stations each with 15 minutes catch wherever feasible.
xiv. One week prior to the MDA, dispatch the drugs as per demand raised by the PHC
Medical Officers.
xv. Starting one week before the MDA, step up the publicity for the MDA by increasing the
BCC activities.
xvi. On the NFD, ensure that you are fully available for the MDA activities. Visit as many
sites as possible to oversee the MDA activities
a. Identify problems faced by the PHC Medical Officer on that day
b. Redress the problem to the best of your ability
c. Assess the response of the public and evaluate the availability of drugs in the
community and their reactions
d. Identify and remedy bottlenecks and redress them
e. Handle the media using standard guidelines
f. Ensure that the PHC is prepared for managing side reactions till the end of the
mopping up day
g. Ensure that the RRT is available and inform the PHC medical officer of the
arrangements made and provide contact information.
h. Set up an information cell preferably with a help-line to handle queries from the
public, professionals and the media.

91
xvii. Collect the reports for the day including a) No. of people covered b) No. of drug
distributors c) Frequency and intensity of side reactions d) Any admission to PHCs or
state Govt hospitals e) other relevant information
xviii. Transmit the reports to Dte. of NVBDCP on the same day by fax.
xix. Supervise the mopping up operations on the second and third day using the same
modus operandi.
xx. Submit the final report on MDA activities (NFD) to Dte. of NVBDCP on the 4th day.
xxi. Organize sample surveys to assess actual drug compliance by utilizing the services
of designated institutes within 2-3 weeks after MDA (since recall may not be reliable
beyond this point.
xxii. Collect the information on unused drugs from the respective PHCs for consolidation
at headquarters within a month after completion of 30 days.
xxiii. File your report with Dte. of NVBDCP before the end of 30 days after the MDA.
xxiv. Collect all relevant vouchers and expenditure statements from the PHCs.
xxv. Collect all relevant vouchers and expenditure statements from the Headquarters.
xxvi. Submit a consolidated statement of expenditure as per guidelines to the Dte. of
NVBDCP.
xxvii. Arrange for dispatching the statement of expenditure (SoE) and utilization certificate
to the Dte. of NVBDCP. Unless the UC is submitted, subsequent release of funds will
not be possible.
xxviii. Convene post-MDA DCC meeting to review the activities of the MDA.
3. RESPONSIBILITIES OF DISTRICT CO-ORDINATION COMMITTEE
i. The DCC is responsible for developing plan of action and implementation of all
aspects of ELF in the district
ii. During the 1st meeting, all district level officers of different sectors and local NGOs
are apprised about the purpose of single dose MDA. They are requested to extend
their co-operation by suitably instructing their subordinates down the line to co-
operate in the programme.
iii. The National Filaria Day, mutually decided by Ministry oh Health and Family Welfare,
Govt. of India and Govt. of endemic states/UTs, is observed for conducting MDA in
the endemic district and the preparatory work will be discussed in this meeting. This
activity must start at least 90 days prior to the proposed date for MDA, usually 11th
November.
iv. The 2nd and 3rd meetings of DCC are conducted as per schedule to review the
implementation of MDA.
v. Following every DCC meeting, media-flash/press meet is conducted to disseminate
the message for community cooperation and participation in ELF.
vi. The funds allotted to the districts are judiciously utilised with proper maintenance of
records.

92
4. RESPONSIBLITIES OF DISTRICT VECTOR BORNE DISEASES OFFICER
vii. He/She is responsible for implementation of all ELF activities in the district in
accordance with the directives given by the SPO and DCC.
viii. He should act as member secretary of DCC and convene the meeting under
chairmanship of District Magistrate/District Collector and communicate the minutes to
SPO and Dte. of NVBDCP. He should get the data compiled and summit timely
reports to SPO and Dte. of NVBDCP, Delhi.
ix. He shall be responsible for the programme planning, implementation and monitoring,
watch the progress, assess the results of sentinel and spot check sites from time to
time and make necessary changes in the pattern of organization and methods that
may be found necessary for achieving maximum compliance for MDA in consultation
with SPO and DCC.
x. Ensure that the implementation of ELF in all the selected areas in the district and the
funds earmarked by the state and centre for ELF are judiciously utilised for ELF. He
should ensure timely submission of Utilization Certificates
xi. He should take appropriate measures deemed fit to improve the drug consumption
level.
xii. He will have close supervision and co-ordination of the activities of different
agencies. He will also coordinate with local branch of the professional bodies like
IMA local branch in order to obtain support for MDA from the medical fraternity,
hospitals, clinics, nursing homes, private practitioners, etc.
xiii. He will get the IEC material including folders on foot hygiene distributed to all the
PHCs well in advance of MDA. He will get that multimedia messages are
disseminated throughout the district collaborating with AIR, TV, cable, local press,
posters, hand bills, group meetings, etc.
xiv. He will ensure that all the concerned PHC officials are given training on ELF who in
turn will train the personnel down in the line.
xv. He will get the mapping done in the identified areas as per schedule and demarcate
the priority areas for MDA and make sure that baseline information and selection of
sentinel/spot check sites are undertaken.
xvi. He will place indent with the State Health Directorate as per schedule for supply of
DEC+Albendazole tablets/other drugs and IEC material after taking into account the
closing balance of drug(s) from the preceding round of MDA. He will ensure that
adequate quantities of drugs are stocked in all the peripheral centres for
symptomatic treatment of side effects of anti-filarial drugs wherever reported.
xvii. He will make frequent visits for on-the-spot technical guidance, seek public co-
operation by meeting prominent people and remove administrative and technical
bottlenecks in the smooth implementation of the programme.
xviii. He will get that the personnel of neighbouring PHCs independently evaluate MDA in
the PHC when the microfilaraemia/antigenaemia reaches below 1%.

93
5. RESPONSIBILITIES OF THE PHC IN-CHARGE MEDICAL OFFICER/MUNICIPAL
HEALTH OFFICER
For MDA Programme:
i. He is the key person for the success of MDA programme.
ii. Determine the number of persons to be treated in the PHC area.
a. Obtain the population size from the family registers
b. Subtract the ineligible population (children less than 2 years, pregnant women and
critically ill patients)
c. Calculate the number of tablets required using the age as the criterion
d. Place an indent with the Programme Manager (NVBDCP) fro the issue of the drugs
well in advance of the MDA date
iii. After attending the training programme organized by the programme manager at HQ,
prepare the training calendar for a) paramedical staff b) drug administrators
iv. Convene a meeting of the village leaders to inform them about the programme
v. Ensure receipt of all registers, flash cards, IEC materials, etc. well in advance.
vi. Arrange to receive the funds earmarked for paramedical staff, training activities, drug
administrators‟ activities including remuneration, and also for management of
lymphoedema cases.
vii. Conduct the training for paramedical staff separately emphasizing their roles and need
to motivate the community and ensure complete participation as per training manual.
Identify drug administrators in the community. Select from NGOs, NSS volunteers and
other local agencies involved in community development activities.
viii. Identify one drug administrator for every 250 population or 50 households to be
covered
ix. Organize training for drug administrators at least a week before the NFD as per
training manual.
x. Prepare a plan for the drug administration process identifying the areas to be covered
by individual drug administrators who would have also a health staff to advise and
assist in the drug administration process. Where possible appoint a supervisory staff to
monitor the activities.
xi. Arrange for the receipt of the drugs from the HQ at least a week prior to NFD and store
them in a cool dark place (use a dark plastic cover as DEC is photosensitive)
xii. Organize a lymphoedema management camp in the PHC using the services of the
filarial field staff. This is preferably done between 7 and 15 days before the MDA.
a. Collect list of lymphoedema patients in the PHC area

94
b. Assemble them at the PHC and demonstrate the techniques of foot hygiene and
preventive foot care.
xiii. Plan of action for the NFD
a. Map the area to be covered under the MDA
b. Appoint the persons to distribute the drugs as per plan
c. Issue the drugs to the drug administrators along with the covers
d. Ensure that the registers are taken to the field for listing the details
e. Instruct the supervisory staff about their roles
f. Should go to the area on NFDs and assess the progress of the drug administration,
identify problems and suggest solutions.
g. Ensure that the network for identifying and managing the side reactions is robust
and functioning
h. Meet the public to assess their response and address their concerns.
i. Collect and consolidate the data at the end of the day for onward transmission to
the state programme manager
j. Submit the reports for the day including a) No. of people covered, b) No. of drug
administrators, c) Frequency and intensity of side reactions, d) Any admission to
PHCs or state Govt hospitals e) other relevant information
k. Prepare for the mopping up operations for the next 2 days
l. Identify refusals and try to convince them to take the drugs
m. Arrange for submitting the necessary vouchers and unspent balance to the state
programme officer within a week of the NFD
For Morbidity Management:
i. Assess the number of copies of the flash cards, forms for enumeration and line listing
of the clinical lymphatic filariasis cases.
ii. Train the Health workers / Volunteers for identifying and grading the lymphatic filariasis
cases in the implementation areas.
iii. Train the Health workers / Volunteers on all components of home based morbidity
management procedures.
iv. Attend on all cases of ADLA episodes for effective management and advocating for
prevention of further episodes.
v. Ensure the documentation of line listing for completeness and forward the
consolidated reports on standard formats.

95
vi. Be fully in-charge of the implementation area and will be held responsible for all
activities in his/her area.
vii. Must acquaint with all aspects of ELF work assigned. For implementing the campaign,
get familiarized with the area and know the epidemiology of LF in the area by means of
available data.
viii. Will have to see that the scheduled programme approved by the SPO and DCC is
carried out correctly by the staff of the area. Indeed, he should set-up a code of work
to the other members of the team. Strict discipline is essential for carrying out the
scheduled work.
ix. In addition to the familiarity with the technical details of ELF work, he should also
familiarize with the standing orders of the State Government, recruitment rules for
volunteers, maintenance of accounts, etc.
x. Well in advance, he must determine the number of sub-divisions in the Implementation
Unit and the number of supervisory staff and health workers/volunteers in each sub-
centre/ village/ ward, taking into account the local conditions in respect of
concentration of houses, accessibility by road, the type of local terrain, etc.
xi. He is fully responsible for Inter-sectoral partners- identification and their involvement in
effective implementation of the MDA campaign.
xii. Training of the drug administrators is one of the most important aspects and he has to
organize the training in local language.
xiii. He has to arrange distribution of drug to all the drug administrators well in time and
collect back balance of drug after mopping up operations.
xiv. It would be his endeavour to know all the staff personally and inspire sufficient
confidence in them as a leader to facilitate team-work.
xv. He must ensure that all the Senior Supervisory staffs carry pocket notebooks in which
MDA work is maintained and that should be available for inspection in the field by
inspecting officers.
xvi. Draw up a clear schedule for maintenance of records and impress upon each
subordinate staffs that these returns are permanent records and should be very
carefully prepared and submitted on the due dates after careful scrutiny to the district
programme manager.
xvii. He should visit the filed area frequently for on-the-spot technical guidance, seeking
public co-operation by meeting prominent people and remove administrative and
technical bottlenecks for the smooth implementation of the programme.
xviii. He has to attend without fail the serious side effects cases as soon as the staffs report
to him.
xix. He is fully responsible for ensuring 85% actual drug compliance of target population
and monitoring of adverse / side reactions.

96
xx. He is responsible for imparting training for screening of the population for identifying
established cases of lymphatic filariasis and implementing morbidity management
packages.
xxi. He is fully responsible for the management of funds provided for the campaign.
6. RESPONSIBILITIES OF THE SUPERVISORY PARAMEDICAL STAFF/ HEALTH
WORKERS
For MDA Programme:
i. Get thoroughly acquainted with the area allotted.
ii. Prepare the maps of the sector and sub-sectors showing the households, schools,
factories, etc.
iii. Identify the Drug Administrators (DAs) from the implementation areas following the
guidelines.
iv. Considering the density of the population, transit facilities, distribute the work to the
DAs in such a way that the responsibility of each one of them could be pinned down.
v. As far as possible, supervise each one of them from time to time while on work.
vi. Collect the remaining drugs from the DAs and return them to MO in-charge.
vii. Collect the information on all the cases of side effects of drugs on day-to-day basis.
viii. Coordinate with the MO so that all the cases with side effects are attended within 24
hours of the reporting.
ix. Perform the duties of DA as and when decided by the MO in-charge.
x. Prepare for mopping up operations to achieve more than 85% actual drug intake (i.e.
drugs to be swallowed in the presence of DA).
For Morbidity Management:
i. Collect the required number of flash cards and enumeration forms for line listing of
lymphatic filariasis cases.
ii. While carrying out door-to-door enumeration for MDA, enquire for at least the most
common clinical manifestations of lymphatic filariasis.
iii. Record all cases on the standard formats.
iv. Inform the MOs immediately if you identify any ADLA cases in the field.
v. Follow-up the patients with ADLA to ensure for the compliance of treatment.
a. He is mainly responsible for the implementation of MDA and Morbidity Management
programmes in his area.
b. He should know the entire households of the implementation areas.

97
c. He is link between the Medical Officers and the drug administrators and success of
MDA and prevention of disability will largely depend on his efficiency and integrity.
d. He is responsible for coordinating the work of drug administrators.
e. He is directly responsible for the coverage and the effective management of side
reactions.
7. RESPONSIBILITIES OF DRUG ADMINISTRATOR
For MDA:
Drug administrator could be the health worker/ASHA/FTDs/DDCs/MLVs or Anganwadi worker
or any other health functionary or health volunteer who shall be imparted training by MO-PHC
on MDA and morbidity management.
i. From the health worker, find out the locality and households in the community allotted to
him for drug administration
ii. Try to locate the fifty households allotted
iii. Find out from health worker the date and venue of training on drug administration
programme
iv. Attend the training programme; get all doubts on mass treatment programme clarified by
the Medical Officer.
For Morbidity Management:
a. Take the flash cards personally for identifying filariasis cases in the community.
b. Showing the flash cards to the family members, enquire for filarial disease
manifestations among any of the family members.
c. Enlist the cases and report to the supervisor.
d. Inform the participants about the home based morbidity management and its uses.
Three visits to households
Make at least three visits to the 50 households allocated to mobilize the people to participate in
treatment and administer the drugs.
Make the first visit to the 50 households 10 days prior to the day of drug administration.
Carry the census register for 50 households and Drug administrators‟ Gate-folder. Verify the
household members using census register. Using the Gate-folder, explain in all the 50
households about the drug administration programme. Inform clearly about the date and time of
drug administration. Clarify people‟s doubts about the mass treatment.
He is the most important person in filariasis elimination programme. His active participation and administration of drugs to all the eligible community members is absolutely essential to eliminate one of the most dreadful diseases and make India
free from lymphatic filariasis.

98
Make the second visit to the same 50 households three days prior to the day of drug
administration. Using Gate folder, explain further about the programme. Emphasize that (i)
chronic disease conditions are irreversible which persist life long (ii) chronic disease inflicts
severe social and economic problems (iii) prevention of disease is easy and simple (iv)
prevention requires only one treatment per year (v) it yields further benefits in terms of
clearance of intestinal worms and make entire family healthy. Again, announce the date and
time of drug administration. Request all the household members to be at home on drug
administration day and take part in treatment. Clarify peoples‟ doubts.
Make third visit to administer drugs. Identify each household member with the help of
census register. After verifying the age, administer the drugs directly to each and every
household member according to the standard dosage schedule. Mark against the name in
census register administration of drugs. Those who are not willing to receive and consume the
tablets, try to explain the preventive value, benefits and safety of treatment, convince them and
administer the drugs. Complete drug administration in all 50 households.
After 3-4 hours, once again visit all the 50 households, verify those who have not received
and consumed the drug. Ask them to consume the drug. Identify those who were not available
earlier and administer the drugs to them. Monitor for side effects, if any.
Management of side effects
Try to be around the 50 households until late evening and monitor if anybody is affected with
side effects. Refer those who developed side effects to the health worker for palliative
treatment. Ensure that they are properly taken care off, and do not allow the situation to spark of
any rumour.
Records and left over drugs
Return the completed records i.e. the census register with drug administration details and left
over drugs to the health worker. Inform him / her if you have had any serious problems during
drug administration.
Programme support
Your efforts to administer the drugs to the community are supported by extensive education
campaign through national and local TV, Newspapers, Radio, posters and pamphlets.
Drug administration next year
Note down all the important points you feel as necessary for your more effective participation in
the programme next year.

99
Sl. No. LF endemic district Sl. No. LF endemic district Sl. No. LF endemic district Sl. No.LF endemic
districtSl. No. LF endemic district Sl. No. LF endemic district Sl. No. LF endemic district
1 Chittoor 16 Katihar 4 Navsari 10 Thrissur 8 Gajapati 12 Chandauli 1 24-Parganas North
2 East Godavari 17 Khagaria 5 Porbandar 11 Trivandrum 9 Ganjam 13 Chitrakoot 2 24-Parganas South
3 Guntur 18 Kishanganj 6 Rajkot 10 Jagatsinghpur 14 Deoria 3 Bankura
4 Karimnagar 19 Lakhisarai 7 Surat 1 Chatrapur 11 Jajpur 15 Etawah 4 Bardwan
5 Krishna 20 Madhepura 8 Valsad 2 Chindwara 12 Jharsuguda 16 Faizabad 5 Birbhum
6 Mahboobnagar 21 Madhubani 3 Damoh 13 Kendrapara 17 Farrukhabad 6 Cooch-Behar
7 Medak 22 Munger 1 Bokaro 4 Datia 14 Khurda 18 Fatehpur 7 Maldah
8 Nalgonda 23 Muzzaffarpur 2 Chatra 5 Katni 15 Koraput 19 Gazipur 8 Midhnapur East
9 Nellore 24 Nalanda 3 Deogarh 6 Panna 16 Malkangiri 20 Gonda 9 Midhnapur West
10 Nizamabad 25 Nawada 4 Dhanbad 7 Rewa 17 Nawarangpur 21 Gorakhpur 10 Mushidabad
11 Prakasham 26 Patna 5 Dumka 8 Sagar 18 Nayagarh 22 Hamirpur 11 Nadia
12 Rangareddy 27 Purnea 6 East Singhbum 9 Satna 19 Nuapada 23 Hardoi 12 Purulia
13 Srikakulam 28 Rohtas 7 Garhwa 10 Tikamgarh 20 Puri 24 Jalaun
14 Visakhapatnam 29 Saharsa 8 Giridih 11 Umaria 25 Jaunpur 1 Pondicherry
15 Vizianagaram 30 Samastipur 9 Godda 1 Chennai 26 Kannauj
16 West Godavari 31 Saran 10 Gumla 1 Akola 2 Cuddalore 27 Kanpur Dehat 1 Andaman & Nicobar
32 Sheikhpura 11 Hazaribagh 2 Amravati 3 Kanchipuram + Saidapet 28 Kanpur nagar
1 Dibrugarh 33 Sheohar 12 Lohardaga 3 Bhandara 4 Kanyakumari 29 Kaushambi 1 Daman & Diu
2 Darrang 34 Sitamarhi 13 Ranchi 4 Chandrapur 5 Nagapattinam 30 Kheri
3 Dhemaji 35 Siwan 14 Sehebganj 5 Gadchiroli 6 Perambalur 31 Kushinagar 1 D & Nagar Haveli
4 Dhuburi 36 Supaul 15 West Singhbum 6 Gondia 7 Pudukottai +Aranthangi 32 Lucknow
5 Kamrup 37 Vaishali 7 Jalgaon 8 Thanjavur 33 Maharajganj 1 Lakshadweep
6 Nalbari 38 West Champaran 1 Bagalkot 8 Latur 9 Thiruvallur + Poonamallee 34 Mahoba 243
district
Total
7 Sibsagar 2 Bidar 9 Nagpur 10 Thiruvannamalai + Cheyyar 35 Mau
1 Bilaspur 3 Bijapur 10 Nanded 11 Thiruvarur 36 Mirzapur
1 Arraha 2 Dhamtari 4 D.Kannada 11 Nandurbar 12 Trichy 37 Pilibhit
2 Arwal 3 Durg 5 Gulbarga 12 Osmanabad 13 Vellore +Thiruppattur 38 Pratapgarh
3 Aurangabad 4 Janjgir 6 Raichur 13 Sindhudurg 14 Villupuram + Kallakurichi 39 Raibareli
4 Banka 5 Jashpur 7 U.Kannada 14 Solapur 40 Rampur
5 Begusarai 6 Mahasamund 8 Udipi 15 Thane 1 Allahabad 41 Sant Kabir nagar
6 Bhagalpur 7 Raigarh 16 Wardha 2 Ambedkarnagar 42 Sant Ravidas nagar
7 Bhojpur 8 Raipur 1 Alappuzha 17 Yawatmal 3 Auraiya 43 Shahjahanpur
8 Buxar 9 Surguja 2 Ernakulam 4 Azamgarh 44 Shravasti
9 Darbhanga 3 Kannur 1 Angul 5 Baerilly 45 Siddharthnaar
10 East Champaran 1 North Goa 4 Kasargod 2 Balasore 6 Ballia 46 Sitapur
11 Gaya 2 South Goa 5 Kollam 3 Bhadrak 7 Balrampur 47 Sonbhadra
12 Gopalganj 6 Kottayam 4 Boudh 8 Banda 48 Sultanpur
13 Jahanabad 1 Amreli 7 Kozhikode 5 Cuttack 9 Barabanki 49 Unnao
14 Jamui 2 Jamnagar 8 Mallapuram 6 Deogarh 10 Basti 50 Varanasi
15 Kaimur 3 Junagarh 9 Palakkad 7 Dhenkenal 11 Bherich
Lakshadweep
List of filaria endemic districts
Bihar
West Bengal
Pondicherry
A & N Islands
Daman & Diu
Gujarat OrissaKerala
Madhya Pradesh
Maharashtra
D & Nagar Haveli
Uttar Pradesh
Tamil Nadu
Chattisgarh
Goa
Gujarat
Kerala
Orissa
Uttar Pradesh
Karnataka
Andhra Pradesh
Assam
Bihar
Jharkhand
Appendix 1







