
1/25/2018
1
Headache and the Contribution of Anxiety
and Mood Disorders
Randall Weeks, Ph.D.
New England Institute for Neurology & HA
Stamford, CT
HCOP
January 27, 2018
Disclosures…
Speakers’ bureau, AdBoard, Consultant…
Alder
Allergan
Pernix

1/25/2018
2
Why Study Comorbidity?
� Complicates differential diagnosis
� Could contribute to disease burden
� May affect treatment adherence
� Creates therapeutic opportunities
� Imposes therapeutic limitations
� Allows treatment of the “whole person”
Methodological Issues
� Selection bias—has to do with the deviation of results from a true value because of differences in characteristics between those selected to be investigated and those that are not studied
� Berkson’s bias (paradox)—is the non-random co-occurrence of two conditions attributed to the methodology employed
� Measurement (assessment) bias—occurs when there is systematic error arising from inaccurate measurement or classification of subjects
Methodological Issues
� Disproportionately more individuals with comorbid disorders are included in clinical samples than in community studies
� Clinic-based studies should be hypothesis generators
� Comorbidity studies are most valid when representative samples of the general population are used
Hamelsky SW, Lipton RB. Psychiatric comorbidity of migraine. Headache 2006, 46, 1327-1333.
1/25/2018
3
Methodological Issues
� Cross-sectional studies demonstrate associations (not directionality)
� Only longitudinal studies can indicate directionality to demonstrate whether one condition predisposes to another or whether the relationship is bidirectional
� Directionality has implications for clinical practice and understanding of mechanisms
Hamelsky SW, Lipton RB. Psychiatric comorbidity of migraine. Headache 2006, 46, 1327-1333.
Migraine Comorbidity Constellations
� Group 1—Defined by hypertension, hyperlipidemia, diabetes mellitus, and
hypothyroidism
� Group 2—Defined by depression, anxiety, and
fibromyalgia
� Group 3—The absence of defining comorbidities
Tietjen GE, Herial NA et al. Migraine comorbidity constellations.
Headache 2007; 47(6):857-865.
Comorbid Psychiatric Disorders
� > number predict refractory HA
� > number predict > ER visits
� > number predict > brain imaging & narcotics
� Multiaxial dx’s predict HA chronification & MOH
Guidetti V et al. Cephalalgia, 1998,18(7):455-462.
Minen MT et al. Gen Hospital Psychiatry, 2014,36(5):533-8.
Sheftell FD, Atlas SJ. Headache 2002; 42: 934-944.

1/25/2018
4
Depression
Association Between Migraine and Depression: IHS-Based Community
StudiesReference Odds Ratio
Breslau (1998)
Migraine w/ aura 4.0
Migraine w/out aura 2.2
Swartz, et al (2000) 2.3
Breslau, et al (2000) 3.5
Low NCP, Merikangas KR. The comMorbidity of migraine. CNS
Spectrums 2003;8(6):433-444.
Martin PR, et al, Behav Res Ther. 2015,73:8-18.
Depression & Migraine—International Studies
� Canada—M’s 60% more likely to dev dep/D’s 40% more likely to dev M
� Brazil—Increased OR’s moving from no M to > freq of M
� Europe—3.5% vs. 6.9% prev in no HA vs M
Mogdill G et al. Headache, 2012;52:422-32.
Goulart AC et al. Headache, 2014;54(8):1310-9.
Lampl C et al. J Headache Pain. 2016;17:59.

1/25/2018
5
Depression & Migraine (Bidirectional Relationship)
� Two year, longitudinal population based study
� Subjects with Major Depression increased the risk of migraine 3.4 fold
� Subjects with Migraine increased the risk of depression 5.8 fold
Breslau et al. Comorbidity of migraine and depression. Neurology.
2003;60:1308-1312.
Depression & Migraine (Bidirectional Relationship???)
� Shared etiology for M & Dep rather than one causing the other
� May need to look at the severity/degree of comorbid disorders (greater presence of one disorder predicts more robust presentation of the other)
Yang Y et al., Twin Res Hum Genet, 2016,49(10):1493-502.
Swartz KL et al., Arch Gen Psychiatry,2000,57(10):945-50.
Bipolar Disorder
1/25/2018
6
Bipolar Disorder?
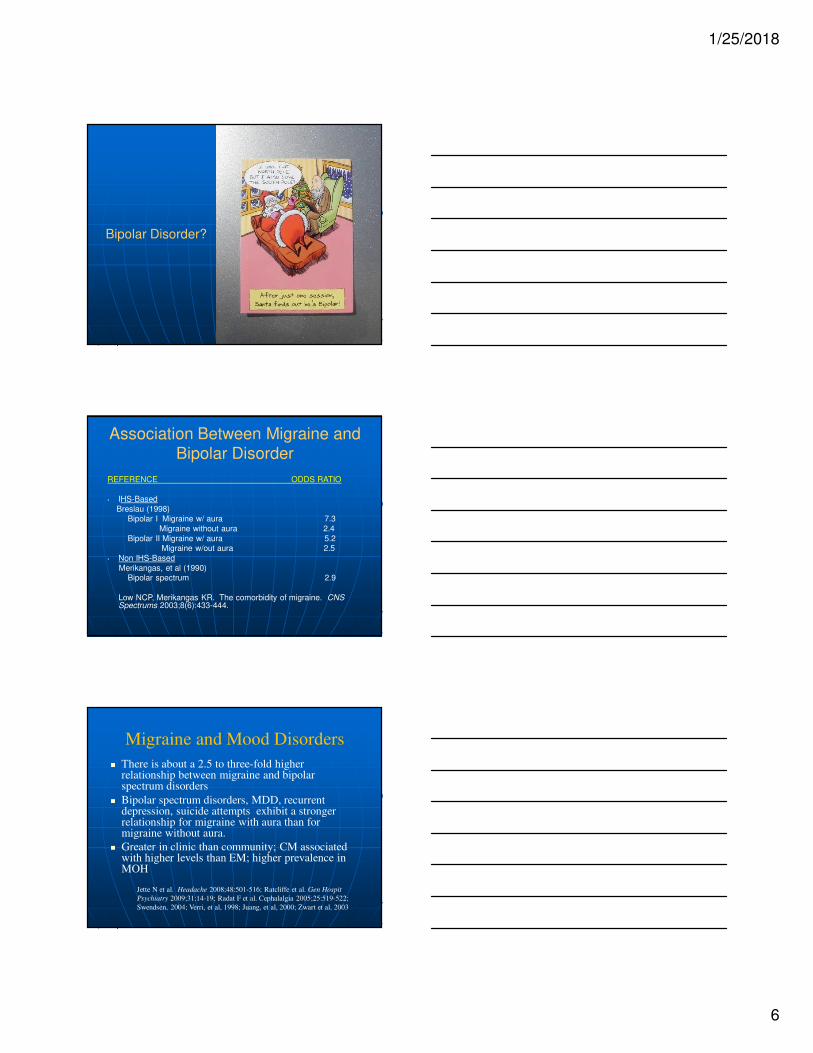
Association Between Migraine and Bipolar Disorder
REFERENCE ODDS RATIO
• IHS-Based
Breslau (1998)Bipolar I Migraine w/ aura 7.3
Migraine without aura 2.4
Bipolar II Migraine w/ aura 5.2 Migraine w/out aura 2.5
• Non IHS-Based
Merikangas, et al (1990)Bipolar spectrum 2.9
Low NCP, Merikangas KR. The comorbidity of migraine. CNS Spectrums 2003;8(6):433-444.
Migraine and Mood Disorders
� There is about a 2.5 to three-fold higher relationship between migraine and bipolar spectrum disorders
� Bipolar spectrum disorders, MDD, recurrent depression, suicide attempts exhibit a stronger relationship for migraine with aura than for migraine without aura.
� Greater in clinic than community; CM associated with higher levels than EM; higher prevalence in MOH
Jette N et al. Headache 2008;48:501-516; Ratcliffe et al. Gen Hospit
Psychiatry 2009;31:14-19; Radat F et al. Cephalalgia 2005;25:519-522;
Swendsen, 2004; Verri, et al, 1998; Juang, et al, 2000; Zwart et al, 2003

1/25/2018
7
Predictors of Bipolarity in Depressed Patients
� Psychotic symptoms� Family history of bipolar disorder� Early age of onset & high freq of depressive
episodes
� High freq of suicidal thoughts � High rates of divorce, job changes� History of erratic, impulsive behavior
� Quicker onset or improvement of symptoms� Pharmacologic-induced mania or hypomania� Hypersomnia, psychomotor retardation,
profound fatigue, overeating more common
Bowden, 2001; Judd et al, 2002; Frye et al, 2004
Anxiety
Association Between Migraine and Anxiety: Community Studies
REFERENCE ODDS RATI O______
Panic GAD OCD Phobia
Breslau (1998)
Migraine w/ aura 10.4 4.1 5.0 2.9Migraine without aura 3.0 5.5 4.8 1.8
Swartz et al (2000) 3.4 1.3 1.4
Breslau et al (2001) 3.7 Merikangas et al (1990, 1993) 3.3 5.3
McWilliams (2004) 3.9
Saunders et al (2008) 3.6Wang et al (2007) 6.6
Goulart et al (2014) 2.3 4.0
Hamelsky SW, Lipton RB (2006) 3.7
Smitherman TA et al. Headache, 2013,53:23-45.Goulert AC et al. Headache, 2014;54(8):1310-9.
Hamelsky SW & Lipton RB. Headache, 2006,46(9):1327-33.

1/25/2018
8
Comorbidity Summary
� Migraine has consistently been associated with psychiatric disorders such as depression, anxiety, and bipolar disorders
� For medical patients, treat comorbid psychiatric conditions both pharmacologically and psychologically
� For psychiatric patients, address/treat comorbid medical issues
Migraine Comorbidity
� The number of Migraine comorbities with support from population studies has increased into double digits
� Piecemeal, fragmented, and specialty driven approaches to the migraine comorbidity problem has not served the field or patients well
� Need to identify replicable “essential feature” patient subtypes
� Such subtypes could provide clues to shared pathophysiological mechanisms
Holroyd K. Disentangling the Gordion knot of migraine comorbidity. Headache 2007; 47(6):876-877.
Migraine Comorbities---
Treatment
Now what????

1/25/2018
9
Monotherapy vs. Polytheraphy
� Idea is to use one drug to treat migraine and associated conditions whenever possible (“two-fer”)
� Simpler, less cost, less AE’s, eliminate potential drug interactions
� Physicians often alter preferred choice for migraine prevention and comorbidity when both present together.
� There is risk of only treating one condition optimally.
� Physicians often sell value of “treating two conditions with one RX” more than controlling both conditions effectively.
Silberstein, Dodick, et al Headache 2007;47:585-599
Likely Will Need More than Pharmacotherapy
Learning, Conditioning, & Cognitive issues

1/25/2018
10
Biobehavioral Model
� Abandon organic/psychogenic distinction� Conditions that control chronic headache are
multidimensional involving cognitive/emotional/behavioral factors as well as biological processes
� As a headache disorder becomes more severe and chronic, faulty learning and behavior become important maintenance factors.
Psychobiological Model
As a headache disorder becomes more severe and chronic, faulty learning and behavior become important maintenance factors.
“Trait negative affectivity refers to the
predisposition to a wide range of aversive
mood states like anxiety or depresssion,
that are stable across time, independent of objective stress. Trait negative affect,
elevated in chronic headache, is related
to increased intensity of somatic symptoms”.
Watson D, Pennebaker JW. Health complaints, stress, and distress: exploring the central role of negative affectivity. PsycholRev. l989; 96: 234-254.
1/25/2018
11
Evaluate Pt’s Needs/Concerns
“The actual methods by which physicians may choose, or be forced to treat their patients is, of course, infinitely varied, as are the patients themselves. There is only one cardinal rule: one must always listen to the patient. For if migraine patients have a common and legitimate second complaint besides their migraines, it is that they have not been listened to by physicians. Looked at, investigated, drugged, charged---but not listened to.” (p. 230)
Migraine-Understanding a Common Disorder
Oliver Sacks, M.D. (1985)
Evaluate Pt’s Needs/Concerns
� The “anxious/depressed patient”
� The “co-morbid patient”
� The “angry patient”
� The “defensive patient”
� The “yes/but patient”
� The “show-me patient”
� The “‘slick’ patient”
� The “relieved patient”
Expectancy Model vs. Conditioning Model
Stewart-Williams S & Podd J. Psychological Bulletin. 2004,2:324-340.
1/25/2018
12
Cognitive Psychology
� S-R model not adequate
� Species specific
behavior
� Genetic/Organismicpredispositions
S-O-R model
Factors Thought to Contribute to Expectancy
� Biological predispositions (co-morbidities)
� Modeling
� Conditioning
� Suggestion
� Motivation
� Anxiety Reduction
Cognitive Rx

1/25/2018
13
Stimulus Organism Response
Antecedent Belief Consequence
(Behavior)
“If I don’t take the
pills, all my
headaches will
become
incapacitating.”
Julian Rotter
Internal
vs.
External
Locus of Control
1/25/2018
14
Locus of Control
Internal
� Patient is task-specific
� “Good historian”
� Action-oriented
(“I have a plan”)
� Sets realistic goals
External
� Helplessness (“fix me”)
� Fatalistic/global
� “Suffering” or “hope without action” orientation
� Looking for “magic pill”
� “Yes...but”
“Patients belonging to subgroups
believing that pain was enduring and mysterious were least likely to use
cognitive coping strategies and more
likely to catastrophize with resultant lowering of pain tolerance”.
Williams DA, Keefe FJ. Pain beliefs and the use of cognitive-
behavioral coping strategies. Pain. 1991; 46: 185-190.
Aaron Beck
� Maladaptive Patterns of Thought
� Dichotomous Reasoning
� Arbitrary Inference
� Overgeneralization
� Magnification (catastrophizing)

1/25/2018
15
Chronic pain patients (across groups)
were significantly different from healthy controls in pain-related negative self- statements, helplessness, and active coping self-statements. Improvement in therapy was associated with lessening of negative cognitions rather than strengthening of positive ones.
Flor H, Behle DJ, & Birbaumer N. Assessment of pain
related cognitions in chronic pain patients. Behav Res
Ther, 1993; 31: 63-73.
“There’s nothing
else that can be
done…I’ve tried
the meds for a
week and my HA’s
are no better…”
M. E. P. Seligman
� Concept of “Learned Helplessness”
� Laboratory analogue of depression
� Expectation of independence between behavior and
outcome (catastrophizing)

1/25/2018
16
“I should be able
to ignore my
migraines and
work each day…It
is a sign of
weakness ”
Albert Ellis
� Rational Emotive Therapy
� Irrational Beliefs & Self-statements
� Shoulds/Musts
� “Awfulizing” (catastrophizing)
“I woke up with a mild
HA this morning and
decided that I couldn’t
go to school (again)
because I was afraid it
would get worse”

1/25/2018
17
Wilbert Fordyce
Pain
vs.
Suffering
Get the diagnosis right.
Get the chemicals right.Get the behaviors right.
Get the cognitions, beliefs, & expectations
right.
Thank you for your kind attention…







