REPORT ON THE MIDTERM EVALUATION OF THE HEALTH LEADERSHIP, MANAGEMENT
AND GOVERNANCE TRAINING PROJECT IN ZIMBABWE
Health Leadership, Management and Governance
Project
2010-2016
University of Zimbabwe
Department of Community Medicine
i
This project has been supported by the President’s Emergency Plan for AIDS Relief (PEPFAR) through The Centers for Disease Control and Prevention under the terms of Cooperative Agreement Number 1U2GPS003002-03.
ii
Table of Contents Table of Contents ............................................................................................... ii
Abbreviations ...................................................................................................... 1
Evaluation Teams ................................................................................................ 2
Acknowledgements.............................................................................................. 3
Executive Summary ............................................................................................ 4
CHAPTER 1 ....................................................................................................... 12
1.1 Background ....................................................................................................................................... 12
1.2 The overall Goal of the Project ......................................................................................................... 13
Long Term Objectives....................................................................................................................... 13
Short Term Objectives ..................................................................................................................... 13
1.3 Introduction ...................................................................................................................................... 14
1.3.1 Purpose of Evaluation ................................................................................................................ 14
1.3.2 Objectives of the evaluation ...................................................................................................... 14
1.4 Framework for Evaluation ................................................................................................................ 15
1.5 Specific Evaluation Objectives .......................................................................................................... 15
1.5.1 Level 1: Satisfaction with Training ............................................................................................. 15
1.5.2 Level 2: Measuring Transfer of Learning .................................................................................... 16
1.5.3 Level 3— Change of behaviour after training ............................................................................ 16
1.5.4 Level 4—Results ......................................................................................................................... 16
1.6 Overview of Primary Stakeholders ................................................................................................... 16
1.7 Participatory Evaluation .................................................................................................................... 17
2.1 Methodology ..................................................................................................................................... 18
2.1.1evaluation Design ........................................................................................................................ 18
2.1 .2 Target Population ...................................................................................................................... 18
2.2 Sampling Procedure .......................................................................................................................... 19
2.2.1 Evaluation Questions ................................................................................................................. 19
2.3 Data Collection .................................................................................................................................. 20
Pre and Post test ............................................................................................................................... 20
Field Survey ........................................................................................................................................ 20
Level 3— Change of behaviour after training .......................................................................... 20
iii
2.4 Location ............................................................................................................................................. 22
2.6 Data Management ............................................................................................................................ 22
CHAPTER 3 ....................................................................................................... 25
3.0 Results of the Evaluation by Kirkpatrick’s Levels of Evaluation ........................................................ 25
3.1 District Health Executive Findings ..................................................................................................... 25
3.2 Reaction Per Five Modules ............................................................................................................... 26
3.3 Reactions To Four Modules .............................................................................................................. 27
3.4 Evaluating Reaction ........................................................................................................................... 27
3.5 Characteristics /Reaction .................................................................................................................. 29
3.7 Change of behavior after training ....................................................................................... 33
3.8 Knowledge Rating Before And After Training ................................................................................... 37
3.8.1 Application Of Knowledge And Skills From The LMG Training .................................................. 39
3.9 Self-Evaluation Perception And Attitudes......................................................................................... 41
3.10 Application Of Knowledge To Routine Practice ............................................................................. 43
CHAPTER 4 ....................................................................................................... 51
4.1 Qualitative Evaluation For DHEs ....................................................................................................... 51
4.2 Conducting FGDs ............................................................................................................................... 51
4.3 Transcription and Analysis ................................................................................................................ 52
Phase 5: Methods of Analysis .................................................................................................... 53
Table 16 Description of the FGD Sample ................................................................................................ 53
4.5 Results Of FGDs ................................................................................................................................. 54
Working as DHE Teams ................................................................................................................ 54
Disciplinary and Grievance Procedures ................................................................................ 56
Decision making process ............................................................................................................. 57
5.1 Provincial Health Executive Level Evaluation.................................................................................... 66
5.3 Educational Qualifications ................................................................................................................ 69
5.4 Provincial Health Executive Level Evaluation Results ....................................................................... 70
CHAPTER 6 ....................................................................................................... 75
6.1 Provincial Hospitals Evaluation ......................................................................................................... 75
Evaluation of PHMT in Health Leadership, Management and Governance
Project .............................................................................................................................................. 75
6.2 Designation Of Respondents- Provincial Hospitals Management Teams ......................................... 75
iv
6.3 Provincial Hospitals Management Teams Results .......................................................................... 77
CHAPTER 7 ....................................................................................................... 81
7.1 Stakeholder Perspectives .................................................................................................................. 81
7.2 Dr L Mbengeranwa- Executive Chairman- Health Service Board ...................................................... 82
7.3 Brigadier-General Dr G. Gwinji: Permanent Secretary MOHCC ........................................................ 82
7.4 CDC Perspective- Dr P Kilmarx .......................................................................................................... 83
7.5 Director Human Resources- Ms J Mudyara ...................................................................................... 83
7.6 The Executive Director Health Services Board – Ms. R.R. Kaseke ................................................... 84
7.7 Dr G. Sikipa, Technical Advisor from MSH ........................................................................................ 85
7.8 National Level Perspectives/ Administration ................................................................................... 85
7.9 Provincial Medical Directors Perspectives ........................................................................................ 89
7.10 Case Studies- Districts ..................................................................................................................... 89
Lupane District ................................................................................................................................ 93
CHAPTER 8 ....................................................................................................... 97
8.1 Discussions ........................................................................................................................................ 97
8.2 Recommendations ............................................................................................................................ 98
Recommendations ............................................................................................................................. 98
8.3 Lessons Learnt ................................................................................................................................... 99
v
Table 1 level of measurement .................................................................................................................... 15
Table 2 Questions aligned to the three levels of Kirkpatrick’s Training evaluation model ........................ 17
Table 3 Related study designs for each level of the model ........................................................................ 18
Table 4: Tools administered for the LMGP midterm evaluation ................................................................ 21
Table 5: Study sites Provinces and Districts ............................................................................................... 22
Table 6 Characteristics of the sample for pre and post training assessment ............................................. 29
Table 7 Demographics pretest/posttest scores .......................................................................................... 30
Table 8 Gender/scores ................................................................................... Error! Bookmark not defined.
Table 9 Profession /pretest and posttest scores ........................................... Error! Bookmark not defined.
Table 10 Level of Education pretest/post test scores .................................... Error! Bookmark not defined.
Table 11 Years of work experience ................................................................ Error! Bookmark not defined.
Table 12: distribution of districts visited during the survey ....................................................................... 34
Table 13: DHE tool distribution by province .................................................. Error! Bookmark not defined.
Table 14.Qualifications of interviewed DHE members ............................................................................... 35
Table 15: DHE professional qualification ....................................................... Error! Bookmark not defined.
Table 16: Years of experience in current position ......................................... Error! Bookmark not defined.
Table 17: Age distribution of DHE members ................................................. Error! Bookmark not defined.
Table 18: HLMG activities by DHE members .............................................................................................. 36
Table 19: Self Evaluating of knowledge before and after training ............................................................. 37
Table 20 Summarizing self-rating scores on knowledge before and after training .................................... 38
Table 22 Mean DHE performance scores before and after training ........................................................... 40
Table 23 Perceptual Analysis (% response rate to each item given for each score) .................................. 41
Table 24 Frequency of Application and practice ........................................................................................ 43
Table 25 Mean DHE performance scores before and after training ........................................................... 44
vi
Table 27: FGD Participants ............................................................................. Error! Bookmark not defined.
Table 28: Provinces and Sample- PHE ......................................................................................................... 66
Table 30: Designation Of Respondents-PHE .................................................. Error! Bookmark not defined.
TABLE 31: Duration in Present Position -PHE ............................................................................................. 69
TABLE 32: PHE Perception of DHE Performance after LMG training ........................................... 72
TABLE 33: Designations for Provincial Hospitals Interviews ....................................................................... 75
TABLE 34: Educational attainment and Work Experience Provincial Hospitals Interviews ...................... 76
TABLE 35: Self-assessment of your knowledge and skills application Provincial Hospitals
Interviews.................................................................................................................................................... 77
Table 36: Rating of hospital performance .................................................................................................. 78
Table 36a: Rating of hospital performance................................................................................................. 79
Table:37 Ministry of Health and Child Care Vehicle Returns of 2010 ...................................................... 86
Table:38 Ministry of Health and Child Care Vehicle Returns of 2014 ........... Error! Bookmark not defined.
1
Abbreviations ANC Antenatal Care
DCM Department of Community Medicine
DEHO District Environmental Health Officer
DHE District Health Executive
DHT District Health Team
DMO District Medical Officer
DNO District Nursing Officer
CEO Chief Executive Officer
CHS College of Health Sciences
HMIS Health Management Information System
HPA Health Professional Authority
HR Human Resources
HRH Human Resources for Health
HRHD Human Resources for Health Development
HRHIS Human Resources for Health Information System
HRM Human Resources Management
HSR Health Services Regulations
HSB Health Service Board
MDGs Millennium Development Goals
MOHCC Ministry of Health and Child Care
NGO Non-Governmental Organization
NUST National University of Science and Technology
PHC Primary Health Care
PMD Provincial Medical Director
PSC Public Service Commission
PHE Provincial health executive
PHT Provincial Health Team
PMD Provincial Medical Director
RHC Rural Health Centre
UZ University of Zimbabwe
WHO World Health Organization
2
Evaluation Teams
Team 1 Northern Provinces
Name Organization Designation
Professor S.Rusakaniko University of Zimbabwe Principal Investigator
Brighton Muzavazi UZ DCM Leadership
Project
M&E Officer
Balbina Mguni UZ DCM Leadership
Project
Finance and
Administration
Officer
E.Mposha Health Services Board Human Resources
Officer
R. Deka MoHCC Human Resources
Officer
Team 2 Southern Provinces
Dr J.Chideme-.Maradzika UZ DCM Leadership
Project
Lecturer
HLMG Project
Director
Andrew Chimatira UZ DCM Leadership
Project
Project Officer
Witness Chekumanyara UZ DCM Leadership
Project
Finance Manager
Vasco Chikwasha UZDCM Biostatistician Lecturer Consultant
Comfort Mwendamberi Ministry of Health and
Child Care
HRO
Rufaro Chikanya Health Services Board HRO-Training
3
Acknowledgements The Evaluation Team is grateful to all institutions and individuals who contributed in
various ways towards the success of the evaluation exercise. Our special thanks go to
the Provincial Medical Directors in all the eight Provinces in Zimbabwe, District Health
Executive Members in the selected districts and the Provincial Hospital Management
Teams. It is with pleasure that we note the invaluable contributions of Ministry of
Health and Child Care members for their readiness and zest in contributing both
programmatic and operational assistance in enabling the evaluation team to do the
work with relative ease.
The MOHCC is appreciated for providing policy direction and guidance during the
proposal preparation and for participating in the evaluation process as part of the data
collection teams. We acknowledge Centers for Disease Control and Prevention the
activity manager Ms Zwashe Bangani for the financial and technical support for this
evaluation without which the evaluation would not have been possible.
4
Executive Summary Background:
The Leadership Management and Governance Project under DCM is a partnership
among the MOHCC, HSB and the University of Zimbabwe that is assisting the MOHCC
to strengthen manpower capacity through health leadership, management and
governance training. The content of training is based on the roles and functions of the
District Health Executives and these include management processes and procedures,
good governance, use of health information for planning, application of health services
regulations and accountability in use of health resources including the capacity to
work with partners and the community in health care delivery.
Purpose
A midterm evaluation of the HLMG training was carried out. The main purpose of the
mid-term evaluation was to assess the process and outcomes of implementing the
health leadership, management and governance training programme in terms of
efficiency, relevance, acceptability and sustainability.
Methods:
Kirkpatrick’s model of evaluation (reaction, learning, behaviour and impact) was used to
develop a framework for evaluating HLMG training.
Reaction
A onetime group series design was used for this level on each DHE group that went
through training. A questionnaire was used to assess the reaction of participants’ in
terms of how the delegates felt about the training as a whole in terms of content,
objectives, duration of training, competency of facilitators, venue and other logistics
related to the training programme. Reaction was measured using Likert scales on
parameters such as satisfaction, relevancy, adequacy, applicability and acceptability.
Learning
A Pre and posttest design was used to assess learning. A questionnaire based on the
expected competencies was used to collect data from each group of participants before

5
and after training. The purpose was to assess whether there was an increase in
knowledge - before and after.
Application /behavior
A cross sectional survey was used to evaluate this level. A questionnaire based on the
competencies covered during training was used to assess application of knowledge
gained during training into practice. Additionally the project developed 8 custom
indicators to track the application of knowledge into practice. These indicators were
developed in line with the content that was covered during the training as well as
considering the expectations and responsibilities of the trained DHE members.
Custom indicators were collected on a quarterly basis and results compared with the
baseline to assess if there are any changes in terms of DHE performances after two
and half years.
Results:
Reaction
A total of 237 DHE participants responded to this level of evaluation. The sample was
made up of 39.7% females and 60.3% males. 95% of the participants indicated that
the module on the National Health Care Strategy is relevant to their day to day duties
and 87% agreed that the information provided to them on this module is adequate
while 90% said they are able to apply what they have learnt during the training when
performing their duties. Time given for each topic was thought of as inadequate since
they preferred more time to grasp important information which was in most cases
quite new for the participants. Over 90% of participants indicated that they were
comfortable with the delivery methods used during training. Relevance was rated as
very good by 98%. Usefulness was rated as excellent by 95% of participants.
Learning
Data was collected from 235 participants for assessing pre and post-test knowledge
levels. The mean score for pretest was 38.1% (SD 13.3) and the median 38% IQR
(30%-48%). Post training scores were mean=75.8 % (SD 10.0), median=76%, IQR
(69%-86%)
Post test scores were significantly higher than pre-test scores (p<0.001). There was
statistical significance between males (mean=36.6%, SD=13.3%) and females
(mean=40.3%, SD=13.3%) on pretest scores p = 0.037. No statistical significance was
6
observed between males (mean=76.2% SD=10.2%) and females (mean=75.0%,
SD=9.8%) at post testing implying an overall positive knowledge gain for the whole
group from the training. Multiple comparison test indicates a significant difference in
pre-test scores between Nurses (mean=44.6%, SD=11.9%) and Accountants
(mean=34.5%, SD=10.3%) (p=0.018), between Nurses (mean=44.6%, SD=11.9%) and
Medical doctors (mean=33.0%, SD=16.7%) (p=0.018) and between Nurses
(mean=44.6%, SD=11.9%) and Pharmacy Managers (mean=34.4%, SD=11.1%)
(p=0.017), with nurses scoring significantly higher. However, in the post-test scores
there was no significant difference between professions. ANOVA test indicates a
significant difference in pre-test scores by years in present position. Those with 6-10
years in present position scored significantly higher (mean=41.8%, SD=9.8%) than
those with less than one year (mean=32.5%, SD=15.9%) (p=0.022), and those with
more than 10 years scored significantly higher (mean=41.6%, SD=15.9%) than those
with less than 1 year (mean=32.5%, SD=15.9%) (p=0.036).
Application of knowledge/behaviour
A total of 105 DHE members were interviewed in the cross sectional survey.
Matabeleland South had the highest number of trained DHE members who were
interviewed (17.1%) compared to Manicaland where only 7.6% were interviewed. A
total of 60.8% were males, whilst 39.2% were females. Positive attitudes were also
noted on procurement where responses disagreed with the statement that
procurement should be done by one person to reduce confusion at 83.5%.
There is an obvious difference in scores for before and after training on all the
assessed topics as indicated by statistically significance levels of p > 0.001 except for
procurement which has a p = 0.009.
Conducting outbreak investigations showed a statistically significant difference as a
result of training as seen by a p = <0.001.The scoring on this aspect increased two fold
after training (2.8) against (4.4) indicating a clear improvement in conducting outbreak
investigation in the DHE performance. There was a significant change in asset
management and control after the training p < 0.001. Working as teams p<
0.001.There was significant improvement in DHE performance in all the areas trained
in timely and accurate reporting p=0.002. DHE Coordination of activities was
7
statistically significant at p value 0.001. Attitudes for working as a team have shifted
towards the positive. Positive rating of team work statements are ranging from a high
of 89.4%, 81.0% Positive attitudes were also noted on procurement where responses
disagreed with the statement that procurement should be done by one person to
reduce confusion at 83.5%
Provincial Health Executive
A total of 18 PHE members were interviewed as part of the cross sectional survey in
the six Provinces. The highest number being in Mashonaland East where 5
respondents were interviewed. Performance of DHEs was rated as significantly
improved in all modules (p<0.005). PHEs noted that DHEs had improved in
coordination of activities, asset management and outbreak investigation.
Regarding the PHEs opinion on the DHE training, (93%) of the participants agreed
that the DHE training in HLMG has strengthened the performance of the DHE in all
their roles and functions.
Provincial Hospital Management Teams
A total of 24 interviews were conducted at Provincial Hospitals as part of the cross
sectional survey. A total of 24 Provincial Hospital Executives were interviewed from the
8 Provincial Hospitals and these were composed of 45.8% females and 54.2% males.
The majority of the hospital executive teams were in the age group 25 -40 years.
The mean scores are highest on teamwork 3.96 and asset management 3.92 against
the lowest mean score of 3.52 quality control. The hospitals had already received
training on quality control hence the no difference in before and after mean scores.
Regarding the PHEs opinion on the DHE training, (93%) of the participants agreed that
the DHE training by the HLMG has strengthened the performance of the DHE.
Conclusions
Relevance
The HLMG training curriculum was developed from the required competencies which
are in turn linked to the day to day roles and functions of District, Provincial and
Hospital Health Executives thus training was relevant to the needs of these managers.
Effectiveness
The immediate results from this evaluation of the training showed that the HLMG
training provided the necessary leadership, management and governance knowledge
8
and skills to the District Health Executives, Provincial Health Executives and
Provincial Hospital Teams. Scores for posttest show a definite increase in knowledge
across all groups showing that learning did take place and was not influenced by the
same factors at pre-testing level. There was an obvious increase in knowledge and
skills for management and governance for health managers at district, provincial and
provincial hospital teams as shown by the rating for before and after training.
Efficiency
The HLMG training has provided an essential function in terms of induction of health
managers. Newly appointed health managers now understand the health services
regulations and the understanding has strengthened their performance for quality
health care service provision.
There was also evidence that health managers were now applying what they had learnt
during HLMG training. Impact has been made in terms of working as teams,
organizing and holding of planning meetings for better collaboration among
programme managers. Impact has been observed in the improvement of accountability
and planning for resources, budgeting procurement and submitting returns to the
national level. Health managers are now aware that they have to use evidence for
planning and evaluation of activities in order to account for any differences before and
after public health activities. Our training provided much needed skills required by
DHE for managing district public health activities.
Sustainability
a) Some districts have collaborated with partners after gaining skills for engaging
partners from the HLMG training. The interaction with partners has provided
additional resources which have in turn translated into improved quality in
health care delivery and a sustained approach to health development in private
partner participation.
a) The HLMG Project has trained teams of facilitators from HSB, MOHCC, UZ,
ZIPAM and ZACH to conduct training National, Provincial and District level
Managers. These facilitators are providing continuity in the HLMG training of
newly appointed health managers at each level. The DHEs are using the skills
obtained from the HLMG training to strengthen other programmes such as the
RBF and /HTF these programmes are being supported by DHEs through
9
training of health center committees in leadership, management and
governance as these group participate in the RBF and HTF initiatives. The
DHEs have also extended training in HLMG among health workers at clinics
and rural hospitals during District Health Team meetings, monthly meetings for
nurses and EHTs.
b) The HLMG project has maintained an inbuilt mechanism for continuation of
training through the provision of summer and winter schools as a way of
continuity. Newly appointed health mangers can participate in these short
courses so as to get an orientation on their roles and functions as health
managers
Noted Good practice in the LMG project
a) Development of training curriculae for all levels of health managers
The HLMG project has developed a number of curricula for health executives for
each level of National Health Care System within the MOHCC. These curricula
have catered for the District Health Executives, Provincial Health Executives,
Provincial Hospital Management Team and City Health Executives. This
approach has been consider as good practice since these modules have been
shared among all the organizations involved in leadership, management and
governance training. All the Health Executives trained in this project were
provided with CDs containing all the modules covered during training.
b) The HLMG project has formed a task force composed of the Ministry of Health
and Child Care Health Services Board, Centers for Disease Control and
Prevention, Management Sciences for Health and the University of Zimbabwe.
The task force has facilitated the smooth implementation of all the training
activities. Consensus through the task force committee has speeded up decision
making and contributed towards success of the HLMG training.
c) The HLMG project provided partial support to trained districts in order to
encourage the holding of quarterly DHT meetings. This support was considered
as crucial in the development of coordination of health related activities at
district level.
10
d) Partial support was provided to the Provincial Health Executive so as to enable
them to provide supportive supervision, mentorship and on job training to the
DHE members to ensure quality health care service delivery.
e) Partial support was provided to the provinces to enable them to conduct their
Provincial Health Team(PHT) meetings which are crucial in coordinating district
activities
f) The HLMG project trained health managers as teams. This approach was well
appreciated by the participants since they realized that every public health
manager has a lot to contribute towards the vision, missions and objectives of
the MOHCC.
Recommendations
a) In-service training for health managers should continue to be competency
based using the already developed modules so as to ensure success, relevance
and usefulness in the strengthening of the health care systems.
b) Province hospitals and districts to have a an orientation programme that helps
new health managers to understand the health system management processes
and the health service regulations so that they can perform their duties in
response to the MOHCC priorities
c) Methods such as group work and cases studies were found to be very conducive
for learning in future such methods should be used in order to enhance adult
learning
d) DCM in collaboration with MOHCC and HSB can work together to develop a
pre-deployment training for health managers to prepare them for new
appointments as health managers at provincial and district level
e) HLMG issues should be included in the training curricula of health workers since the
participants considered the subject as essential for all health mangers as an important
part that prepares them for their roles and functions.
f) There was concern that there should be a continued follow up and mentorship of
trained managers on regular basis.
g) HLMG Training should be made a requirement for promotion to management positions.

11
h) The MOHCC to support the identification of further funding for HLMG training in
Zimbabwe in collaboration with interested partners. HLMG should continue to be
supported financially since this evaluation is indicating the need to for in- service
training and pre-deployment training to cater for the high attrition in the MOHCC and
also to cater for other partners that are involved in public health initiatives.
i) DCM LMGP to train trainers of trainers for each province in leadership
management and governance as a sustainable strategy for ensuring
quality in health care delivery and the training to emphasis the concept
of working as teams since the participants rated this module very highly
and field work follow up has also indicated that the module on working
as teams was most favourable and the skills are being applied in the
health teams day to day work
KEY WORDS: Kirkpatrick’s model, Health Systems Strengthening, Competency based training
and Evaluation
12
CHAPTER 1
1.1 Background The Ministry of Health and Child Care remains committed to the vision of ensuring the
highest possible level of health and quality of life for all citizens of Zimbabwe. This will
be attained through the combined efforts of individuals, communities, organizations
and the government, which will allow them to participate fully in the socio-economic
development of the country. Over the last decade the government of Zimbabwe`s
economy has declined due to various challenges. The declining economy has impacted
negatively on the health sector and this has in turn reduced the ability of the MOHCC
to deliver health care.
To achieve the attainment of the highest level of care provision, the Ministry of Health
and Child Care has developed the National Health Strategy which has thirty three
areas for action and implementation over the next five years (NHS 2009). One of the
key aspects of the strategy is Health System Strengthening which requires adequate
resources and an appropriate enabling environment as critical prerequisites for the
successful scaling up of health care delivery. Health System Strengthening requires
six pillars namely:
a) Provision of adequate, skilled and well remunerated Human Resources for
Health. (Through halting and reversing brain drain, recruiting, training and
retaining qualified health staff, Increase productivity and professionalism of health
worker)
b) ) Continuous supply of medicines and medical supplies:
c) ) Provision of functional Equipment:
d) ) Provision of Transport:
e) ) ensuring a sustainable and predictable Financial Base:
f) ) There will also be need to address the issues of leadership and governance
at all levels, disease surveillance and health information for decision making
including strengthening coordination of health sector players.
13
The areas identified in the NHS go beyond the boundaries of the health sector and are
thus the Ministry of Health has actively pursued the opportunity to develop private
and other public partnerships in order to response comprehensively to the health
needs of the nation. The HLMGP under DCM is one of such partnerships that is
assisting the MOHCC to strengthen the district health systems focusing on Pillar 1
and Pillar 6 specifically through the training of District Health Executives (DHE) as
indicated in the National Health Strategy.: “Health management has weakened as
a result of high attrition rates of experienced health service and programme
managers. This has an impact on supervision and monitoring and is evidenced
by reduced quality of service provision. ”Page 9 NHS 2009 .The DCMLMGP has
been running for a year and is now in its second year and has trained
1.2 The overall Goal of the Project To strengthen the public health manpower capacity that will contribute to quality
patient care and to well-planned and managed public health programmes for total
health improvement in the nation.
Long Term Objectives
1. Effective leadership in health planning, program implementation and patient
care in public sector In Zimbabwe.
2. Implementation of the MOHCC National Human Resources for Health (HRH)
policy at all levels of the public health sector delivery system.
3. Development and implementation of National Leadership training and
mentorship program.
Short Term Objectives
1. To revise and implement a national leadership curriculum in the first year of
the cooperative agreement.
2. To roll out the newly developed HRH policy document, at national and
provincial levels. in the first year and rolled out to all 62 districts by the end of
the fifth year of the cooperative agreement.
3. To train at least 500 health workers successfully in health leadership,
management and governance.
4. To conduct at least 124 District strategic planning and review meetings and at
least twenty provincial strategic planning and review meetings per year.
14
1.3 Introduction The Leadership, Management and Governance Training programme now at its half-life
stage carried out a midterm evaluation to self-introspect. Having trained all the DHE,
PHMT in all provincial hospitals it was time to assess whether the programme was
moving in line with its envisaged objectives and contributing to improved health care
services.
1.3.1 Purpose of Evaluation
The main purpose of the mid-term evaluation was to assess the process and impact of
implementation of the leadership management and governance training programme in
terms of efficiency, relevance, acceptability and sustainability of the LMG training. The
mid-term evaluation was based on the Kirkpatrick’s model of training evaluation The
model includes assessment of training based on four levels of training outcomes:
knowledge gained, attitude change, and application of knowledge gained and impact
on health. The evaluation only focused on the three levels since the fourth level
requires a long time to realize.
1.3.2 Objectives of the evaluation
1. To assess the knowledge levels on the principles and frameworks on health
leadership, management and governance provided during the training for DHE
conducted between 01 October 2010 to August 2013
2. To assess the values and attitude on HLMG related to the application of
principles covered in the DHE training.
3. To identify the practices of DHEs in place as a result of the HLMG training
conducted between 01st October 2010 to August 2013
4. To assess on how the Health Services Regulations training conducted between
01 October to August 2013 has influenced the application of health services
regulations in the workplace.
5. To compile success stories, best practices and challenges faced by DHEs in
implementing what they have learnt.
6. To assess the progress made regarding district supervision and support by the
PHE.
15
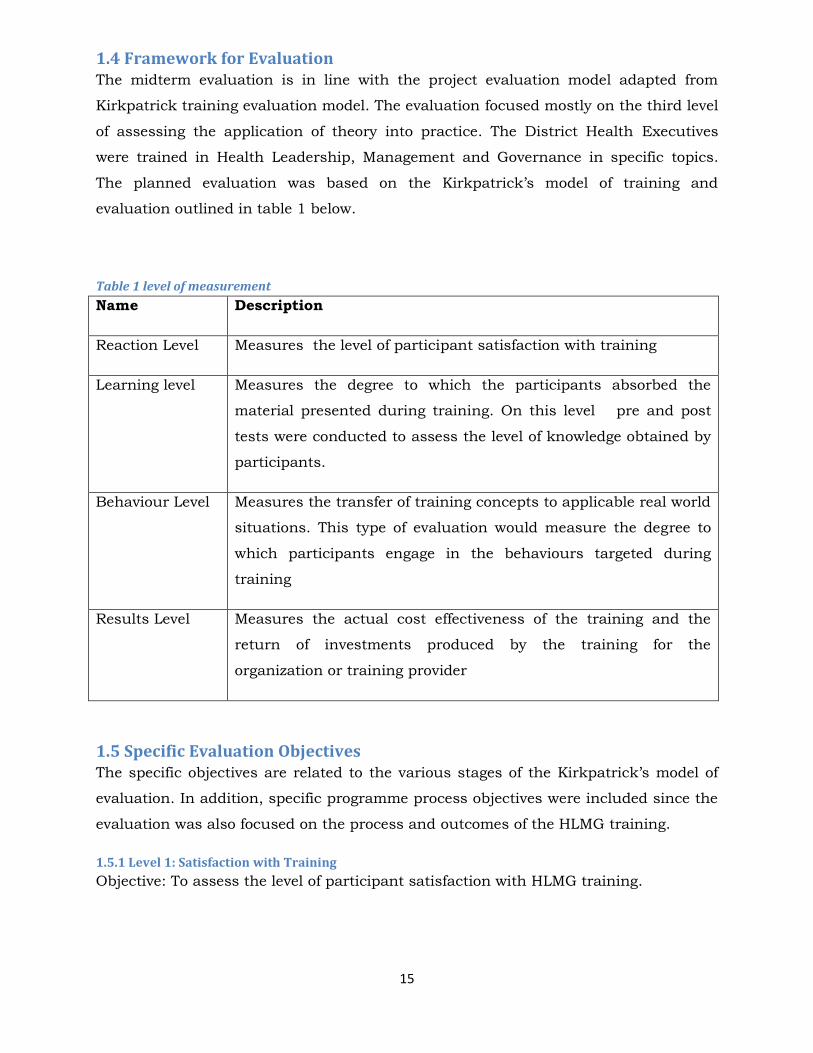
1.4 Framework for Evaluation The midterm evaluation is in line with the project evaluation model adapted from
Kirkpatrick training evaluation model. The evaluation focused mostly on the third level
of assessing the application of theory into practice. The District Health Executives
were trained in Health Leadership, Management and Governance in specific topics.
The planned evaluation was based on the Kirkpatrick’s model of training and
evaluation outlined in table 1 below.
Table 1 level of measurement
Name Description
Reaction Level Measures the level of participant satisfaction with training
Learning level Measures the degree to which the participants absorbed the
material presented during training. On this level pre and post
tests were conducted to assess the level of knowledge obtained by
participants.
Behaviour Level Measures the transfer of training concepts to applicable real world
situations. This type of evaluation would measure the degree to
which participants engage in the behaviours targeted during
training
Results Level Measures the actual cost effectiveness of the training and the
return of investments produced by the training for the
organization or training provider
1.5 Specific Evaluation Objectives The specific objectives are related to the various stages of the Kirkpatrick’s model of
evaluation. In addition, specific programme process objectives were included since the
evaluation was also focused on the process and outcomes of the HLMG training.
1.5.1 Level 1: Satisfaction with Training
Objective: To assess the level of participant satisfaction with HLMG training.
16
1.5.2 Level 2: Measuring Transfer of Learning
Objective: To assess if the participant absorbed the information presented during
HLMG training.
1.5.3 Level 3— Change of behaviour after training
Objective: To assess the level of application of HLMG ideas gained from the DHE
training
To assess if there are any changes in behaviour after the HLMG training.
To assess the degree to which trained health managers are engaging in the
behaviours targeted during HLMG training (e.g. holding meetings regularly
working as a team utilizing health information for planning)
To identify if the training is contributing towards an increase in discrete skills
and techniques for leadership management and governance.
To assess if there has been improved performance by DHEs and PHMTs that
have undergone the HLMG training.
1.5.4 Level 4—Results
Objectives: To identify if the HLMG training have contributed to the overall
organizational objective
Intermediate outcome of training may include the following aspects:
Improved quality of work, higher productivity, reduction in turnover.
reduction in scrap rate (i.e., less wasted resources), improved quality of work
life, improved human relations (e.g., improved vertical and horizontal
communication, Lower absenteeism, higher worker morale, greater job
satisfaction
The evaluation did not include the fourth level of the Kirkpatrick’s model which is an
improvement in the community’s quality of life and ultimately the reduction in
morbidity and mortality.
1.6 Overview of Primary Stakeholders The study sought to address the information needs of all the stakeholders involved in
the LMGP that include CDC , , MOHCC, HSB , (MSH) and other UN organizations and
17
NGOs that have an interest in leadership, management and governance training of
health workers. The stakeholders were to be engaged to contribute to the development
of the evaluation process from the beginning to the finalization of findings of the
evaluation.
1.7 Participatory Evaluation The evaluation study incorporated the concept of participatory evaluation. This was
done in order to empower the trained DHE members to analyze, appreciate and to
solve any problems that may hinder the adoption of recommended management
practices in a health care setting. (Jackson and Kassam 1999).The evaluation team
comprised of all sectors HSB, MOHCC Human resource department all PMD offices,
HSB and CDC. The participants from the training were given a chance to describe
their experience in terms of knowledge gained and the practices they now engage in.
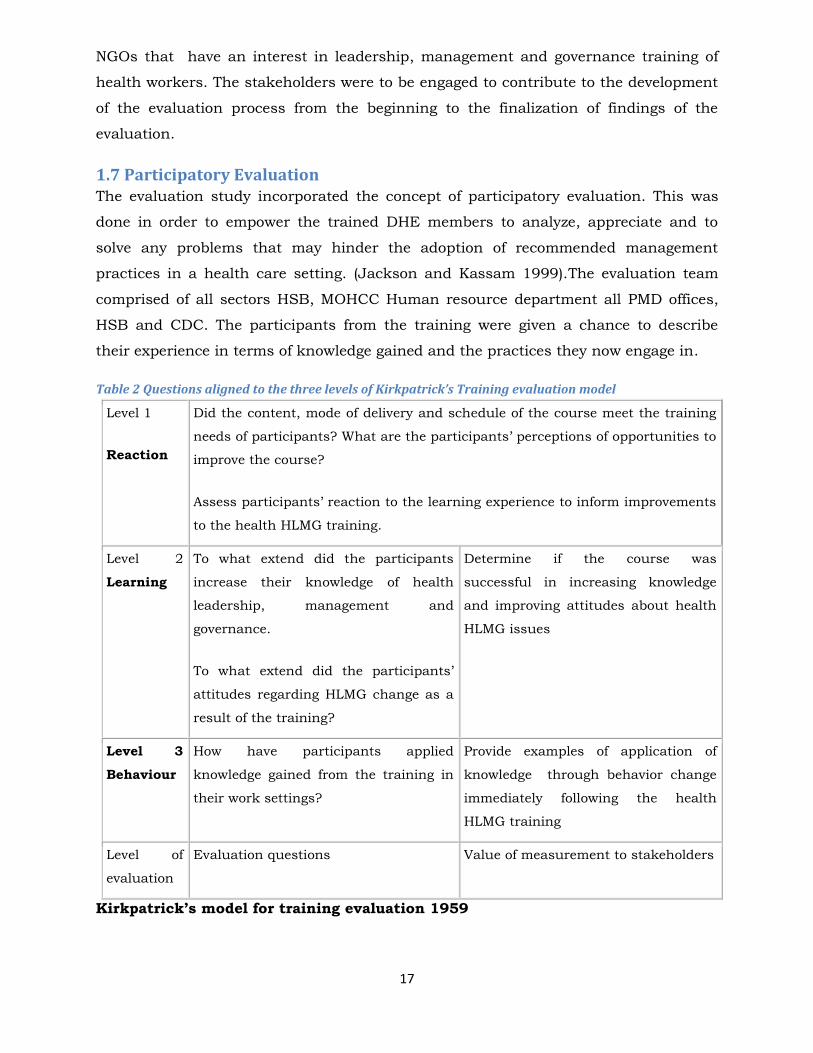
Table 2 Questions aligned to the three levels of Kirkpatrick’s Training evaluation model
Level 1
Reaction
Did the content, mode of delivery and schedule of the course meet the training
needs of participants? What are the participants’ perceptions of opportunities to
improve the course?
Assess participants’ reaction to the learning experience to inform improvements
to the health HLMG training.
Level 2
Learning
To what extend did the participants
increase their knowledge of health
leadership, management and
governance.
To what extend did the participants’
attitudes regarding HLMG change as a
result of the training?
Determine if the course was
successful in increasing knowledge
and improving attitudes about health
HLMG issues
Level 3
Behaviour
How have participants applied
knowledge gained from the training in
their work settings?
Provide examples of application of
knowledge through behavior change
immediately following the health
HLMG training
Level of
evaluation
Evaluation questions Value of measurement to stakeholders
Kirkpatrick’s model for training evaluation 1959
18
CHAPTER 2
2.1 Methodology
2.1.1evaluation Design
The study designs were applied as appropriate for each level of outcome being
evaluated as described under each section. A mixture of study designs were employed
for this evaluation. Kirkpatrick’s model of training and evaluation was used for this
evaluation since the model formed the format of the training. Overall a cross sectional
survey was used as an overall design. However other study designs were nested within
the cross sectional survey framework in order to capture specific issues and to suit the
level of evaluation and the specific outcomes accordingly in relationship to
Kirkpatrick’s model of training and evaluation as illustrated in table 3 below.
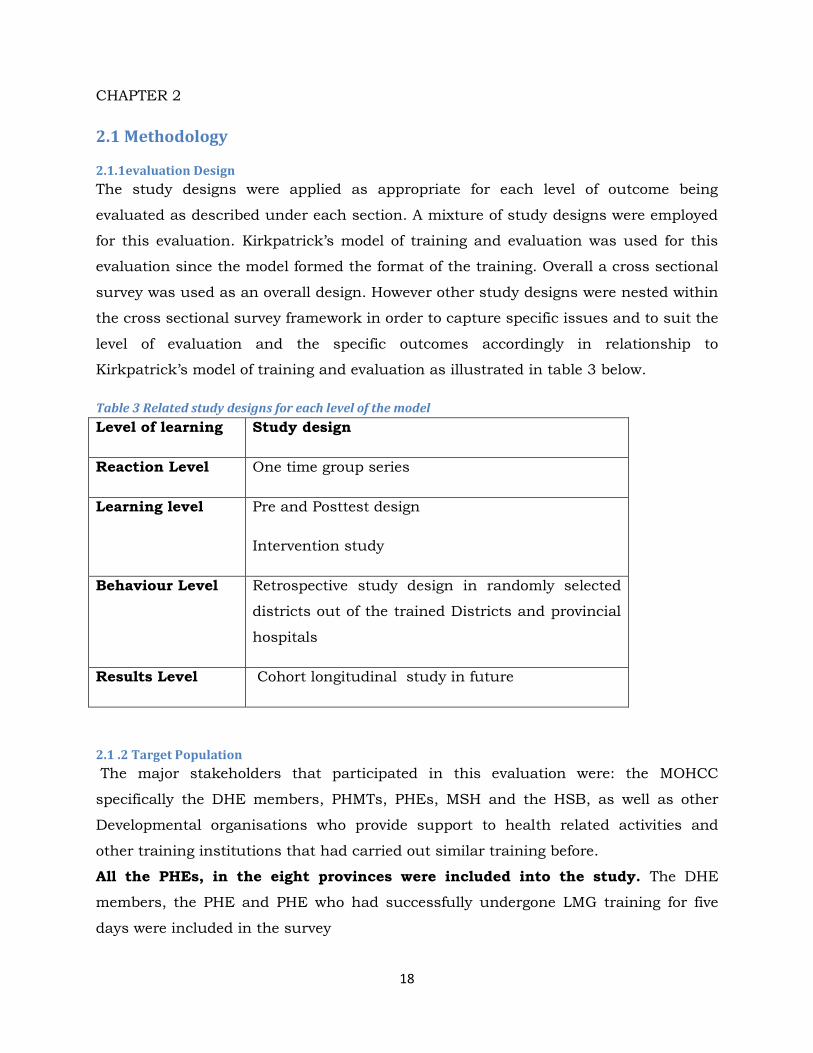
Table 3 Related study designs for each level of the model
Level of learning Study design
Reaction Level One time group series
Learning level Pre and Posttest design
Intervention study
Behaviour Level Retrospective study design in randomly selected
districts out of the trained Districts and provincial
hospitals
Results Level Cohort longitudinal study in future
2.1 .2 Target Population
The major stakeholders that participated in this evaluation were: the MOHCC
specifically the DHE members, PHMTs, PHEs, MSH and the HSB, as well as other
Developmental organisations who provide support to health related activities and
other training institutions that had carried out similar training before.
All the PHEs, in the eight provinces were included into the study. The DHE
members, the PHE and PHE who had successfully undergone LMG training for five
days were included in the survey
19
The project targeted all DHE members in the 61 districts, facilitators in the DHE
training, PMDs, programme managers in the MOHCC and those in the Private sector
and Non-Governmental organization who have interacted and supported HLMG
training over the three years.
2.2 Sampling Procedure Manicaland, Mashonaland East, Mashonaland Central, Mashonaland West, Masvingo
Matabeleland North and Matabeleland South were selected into the study.
Convenience sampling was used to identify the respondents who are all members of
the DHE and PHE who were found present on the day of the evaluation.
Development of the questionnaires
The questionnaires were developed using Kirkpatrick’s model of training evaluation.
The following questionnaires were developed:
a) Pre and posttest questionnaire
b) Workshop evaluation questionnaire
c) Custom indicator questionnaire field follow up
d) Midterm survey questionnaire based on the modules covered
e) Focus group discussion guide
Pretesting the Survey Instruments
The data collection instruments were designed for each of the three categories of
respondents, namely DHE, PHE and PHMT members. The draft questionnaires
were pre tested with the Seke DHE for user friendliness which was later not
included in the survey. The technical content was pre-tested within the DCM to
ensure that the questions were understandable and relevant to the study
objectives.
2.2.1 Evaluation Questions
Did the content, mode of delivery and schedule of the HLMG training meet the
training needs of participants?
What are participants` perceptions of opportunities to improve the course?
To what extent did participants’ increase their knowledge on health leadership,
management and governance principles as a result of the training?
To what extent did participant’s attitudes towards health leadership,
management and governance change as a result of the training?

20
How have participants applied knowledge gained from the training in their work
as DHEs
2.3 Data Collection Reaction- Workshop Evaluation
Participants were given questionnaires to fill in at the end of each training session of
five days. Questions in this level included how participant’s felt about the learning
process including aspects such as the organization of learning process, time allocated
to the modules, ability of the facilitators ,relevance of subject covered, adequacy of
time , , accommodation ,food and general ambiance of the venue.
Pre and Post test
Data collection involved the administration of pre and post test before participants
began the training and post test upon completion of training. The pre test included
demographic information to establish a baseline for knowledge and attitudes relevant
to content in each of the moduels in the HLMG training. The post test included the
same information on satisfaction with content mode of delivery and schedule as well
as an opprtunity to provide examples of application of knowledge gained in a work
setting.
Field Survey
The midterm evaluation survey involved carrying out interviews and focus group
discussions with the selected respondents. Interviewer and self administered
questionnaires were used to collect data. In cases where respondents were available
the data collectors would administer the questionnaires but where the respondents
were not available, the questionnaires were left for the respondents to complete . The
evaluation teams would then come back on a later date to collect the completed
questionnaires. Focus group discussions were held in each of the district visited.
Level 3— Change of behaviour after training
To assess if there are any changes in behaviour after the LMG training
21
To assess the degree to which trained health managers are engaged in the
behaviours targeted during HLMG training (e.g. holding meetings regularly
working as a team utilizing health information for planning)
To identify if the training is contributing towards an increase in discrete skills
and techniques for health leadership, management and governance to assess if
there has been improved performance by DHEs and PHMTs that have
undergone the training
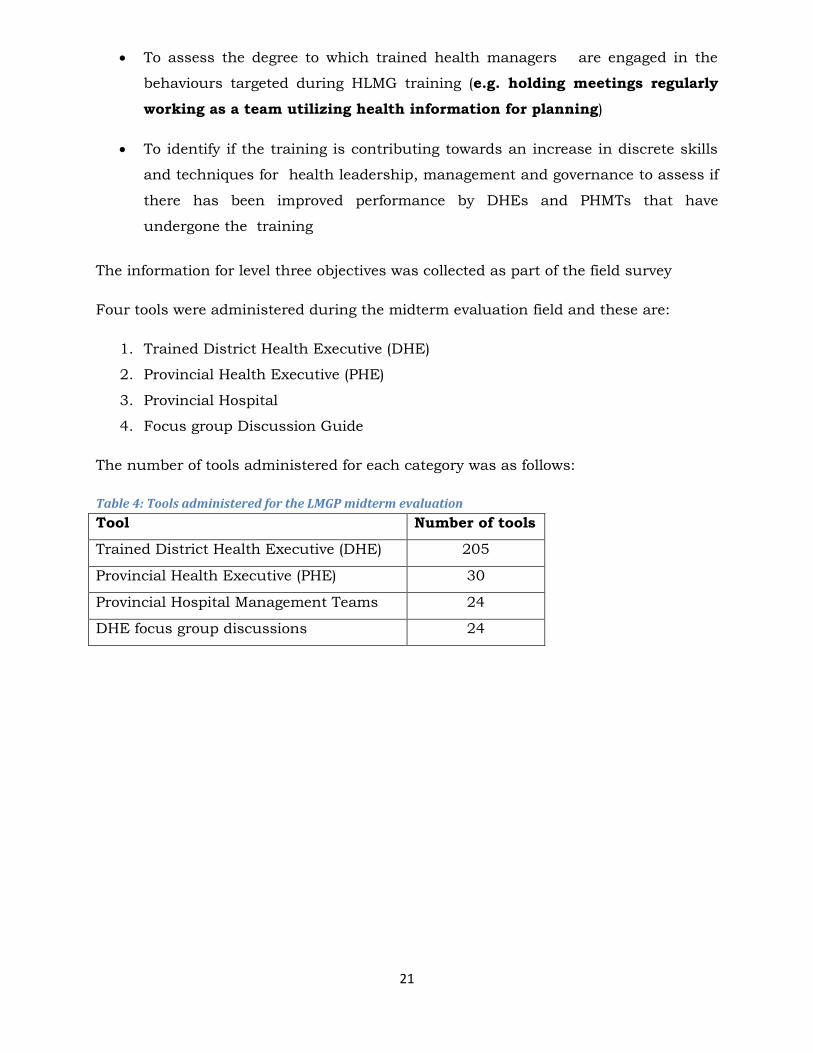
The information for level three objectives was collected as part of the field survey
Four tools were administered during the midterm evaluation field and these are:
1. Trained District Health Executive (DHE)
2. Provincial Health Executive (PHE)
3. Provincial Hospital
4. Focus group Discussion Guide
The number of tools administered for each category was as follows:
Table 4: Tools administered for the LMGP midterm evaluation
Tool Number of tools
Trained District Health Executive (DHE) 205
Provincial Health Executive (PHE) 30
Provincial Hospital Management Teams 24
DHE focus group discussions 24
22
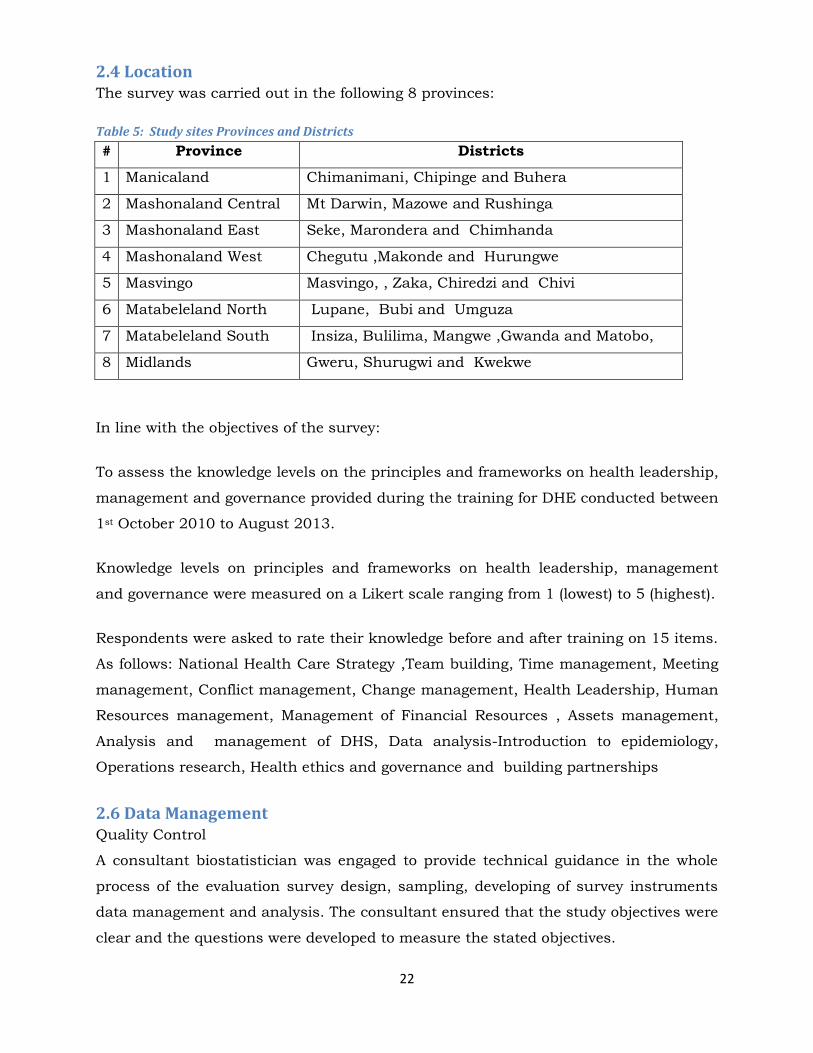
2.4 Location The survey was carried out in the following 8 provinces:
Table 5: Study sites Provinces and Districts
# Province Districts
1 Manicaland Chimanimani, Chipinge and Buhera
2 Mashonaland Central Mt Darwin, Mazowe and Rushinga
3 Mashonaland East Seke, Marondera and Chimhanda
4 Mashonaland West Chegutu ,Makonde and Hurungwe
5 Masvingo Masvingo, , Zaka, Chiredzi and Chivi
6 Matabeleland North Lupane, Bubi and Umguza
7 Matabeleland South Insiza, Bulilima, Mangwe ,Gwanda and Matobo,
8 Midlands Gweru, Shurugwi and Kwekwe
In line with the objectives of the survey:
To assess the knowledge levels on the principles and frameworks on health leadership,
management and governance provided during the training for DHE conducted between
1st October 2010 to August 2013.
Knowledge levels on principles and frameworks on health leadership, management
and governance were measured on a Likert scale ranging from 1 (lowest) to 5 (highest).
Respondents were asked to rate their knowledge before and after training on 15 items.
As follows: National Health Care Strategy ,Team building, Time management, Meeting
management, Conflict management, Change management, Health Leadership, Human
Resources management, Management of Financial Resources , Assets management,
Analysis and management of DHS, Data analysis-Introduction to epidemiology,
Operations research, Health ethics and governance and building partnerships
2.6 Data Management Quality Control
A consultant biostatistician was engaged to provide technical guidance in the whole
process of the evaluation survey design, sampling, developing of survey instruments
data management and analysis. The consultant ensured that the study objectives were
clear and the questions were developed to measure the stated objectives.
23
During the data collection process completion of the questionnaires was ensured
through random checks of completed questionnaires. The completed questionnaires
were collected at the end of each day by the team leaders and put in a secure place.
Data management commenced during field work. Data quality control took place
during the data collection process. Questionnaires that were self-completed by the
respondents were also checked for completeness and any incomplete questionnaires
had to be completed by engaging the responsible respondents during rescheduled
where necessary and possible.
Data entry
A data base was created in Epi Info 3.5.1 for each questionnaire to ensure that data
would be captured immediately during and after the survey.
After the survey all questionnaires were sorted into the categories and were prepared
ready for entry into the Epi Info data bases.
Two data entry clerks were trained to enter the data. After the training data entry
commenced with each data entry clerk entering different questionnaires. Data entry
quality checks were done randomly by selecting 10% of the entered questionnaires
and verify accuracy and completeness.
After completing data entry, data was transferred from Epi Info to Stata 13 for
cleaning and analysis in line with the objectives of the survey. The cleaned data was
archived on USB and is stored securely by the project team.
24
EVALUATION (DHE)
FINDINGS
25
CHAPTER 3
3.0 Results of the Evaluation by Kirkpatrick’s Levels of Evaluation
3.1 District Health Executive Findings
Level 1 Reaction
This first level of Kirkpatrick`s training evaluation model measures how the delegates
felt about the training or learning experience.The purpose of these questions were to
identify how the participants viewed the whole process and organization of the
workshop, status of the venue, the adequacy of time allocated to each module
,workshop programming and the effectiveness of training delivered. The questionnaire
consisted of questions on reaction evaluation on how the participants felt about the
learning experience. Other aspects of the assessment included how the participants
felt about the venue, meals and logistics arrangements and the overall coordination of
the training. The reaction to the training was assessed at each of the training
workshops held for the 61 DHEs. Data is based on 237 participants since this level of
assessment was not done for the initial four workshops. The data presentation below
provides information on the results of this assessment.
26
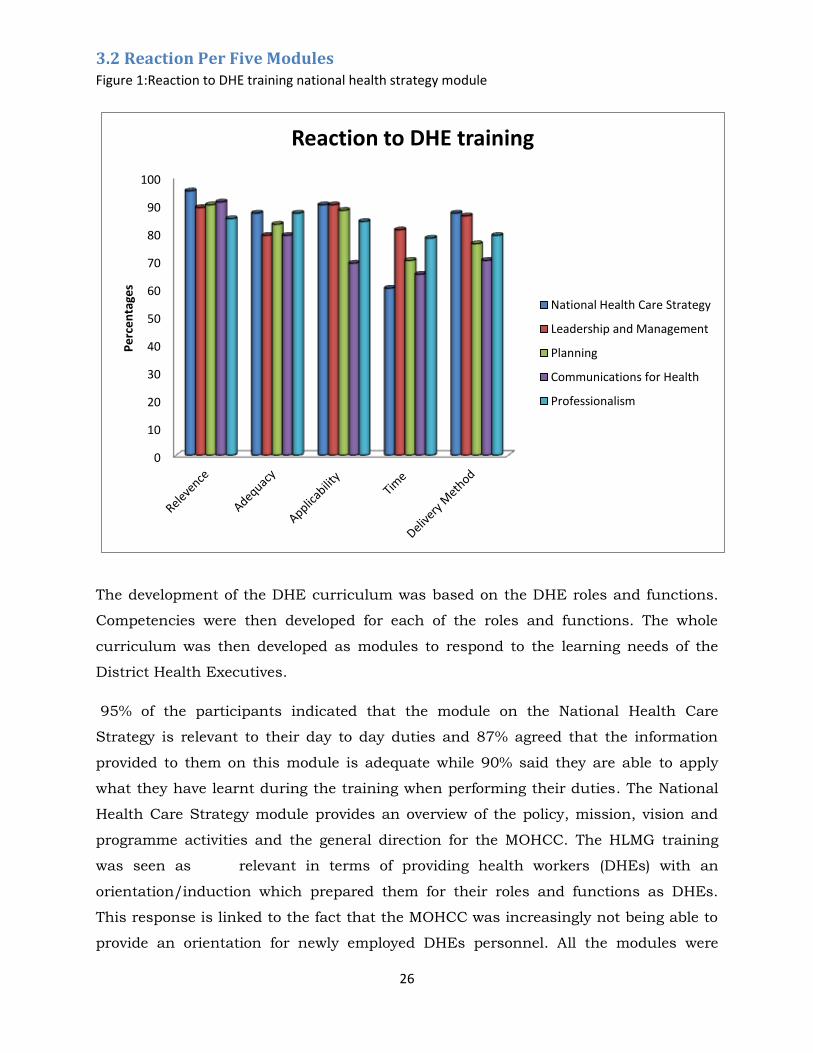
3.2 Reaction Per Five Modules Figure 1:Reaction to DHE training national health strategy module
0
10
20
30
40
50
60
70
80
90
100
Pe
rce
nta
ges
Reaction to DHE training
National Health Care Strategy
Leadership and Management
Planning
Communications for Health
Professionalism
The development of the DHE curriculum was based on the DHE roles and functions.
Competencies were then developed for each of the roles and functions. The whole
curriculum was then developed as modules to respond to the learning needs of the
District Health Executives.
95% of the participants indicated that the module on the National Health Care
Strategy is relevant to their day to day duties and 87% agreed that the information
provided to them on this module is adequate while 90% said they are able to apply
what they have learnt during the training when performing their duties. The National
Health Care Strategy module provides an overview of the policy, mission, vision and
programme activities and the general direction for the MOHCC. The HLMG training
was seen as relevant in terms of providing health workers (DHEs) with an
orientation/induction which prepared them for their roles and functions as DHEs.
This response is linked to the fact that the MOHCC was increasingly not being able to
provide an orientation for newly employed DHEs personnel. All the modules were
27
relevant to the work being done by the DHE as highlighted by 90% of the participants.
Time given for each topic was thought of as inadequate since participants preferred
more time to grasp important information which was in most cases quite new for the
them as shown by figure 1 above. The delivery methods used included lectures,
plenary session, group discussions, group work, role plays and District projects. Most
of the participants were comfortable with the delivery methods as indicated in the
figure 1 above.
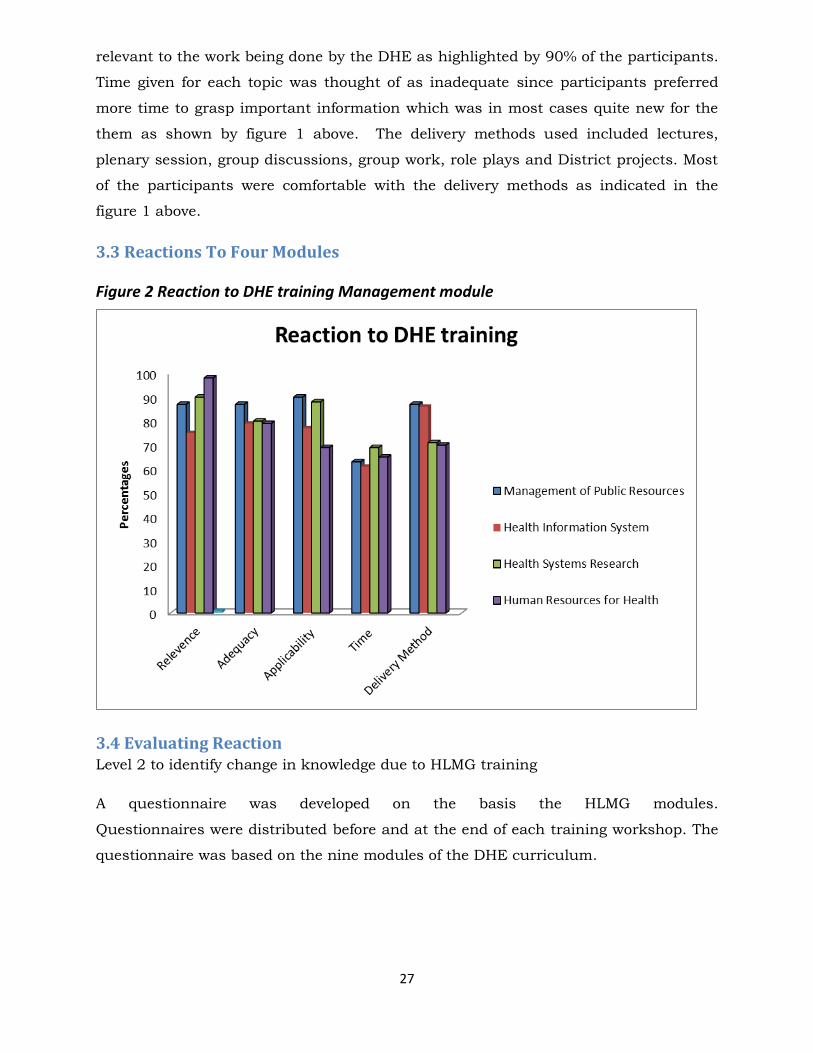
3.3 Reactions To Four Modules
Figure 2 Reaction to DHE training Management module
3.4 Evaluating Reaction Level 2 to identify change in knowledge due to HLMG training
A questionnaire was developed on the basis the HLMG modules.
Questionnaires were distributed before and at the end of each training workshop. The
questionnaire was based on the nine modules of the DHE curriculum.
28
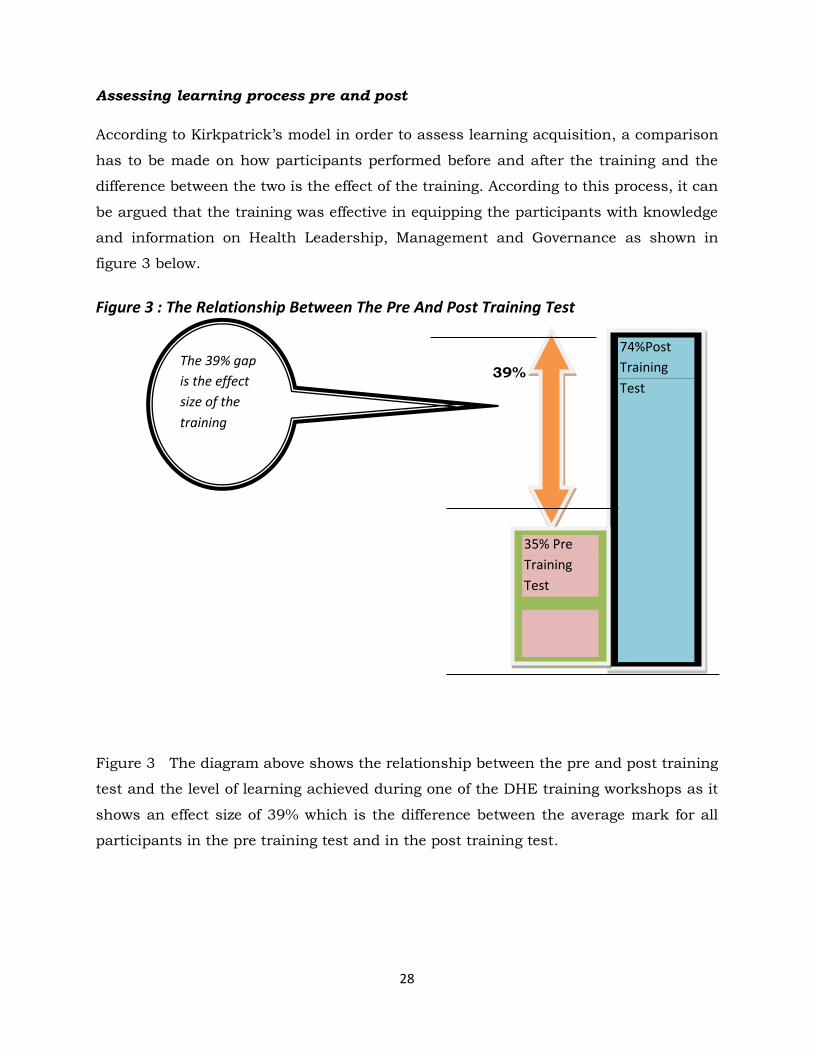
Assessing learning process pre and post
According to Kirkpatrick’s model in order to assess learning acquisition, a comparison
has to be made on how participants performed before and after the training and the
difference between the two is the effect of the training. According to this process, it can
be argued that the training was effective in equipping the participants with knowledge
and information on Health Leadership, Management and Governance as shown in
figure 3 below.
Figure 3 : The Relationship Between The Pre And Post Training Test
39%
Figure 3 The diagram above shows the relationship between the pre and post training
test and the level of learning achieved during one of the DHE training workshops as it
shows an effect size of 39% which is the difference between the average mark for all
participants in the pre training test and in the post training test.
74%Post
Training
Test
The 39% gap
is the effect
size of the
training
35% Pre
Training
Test
29
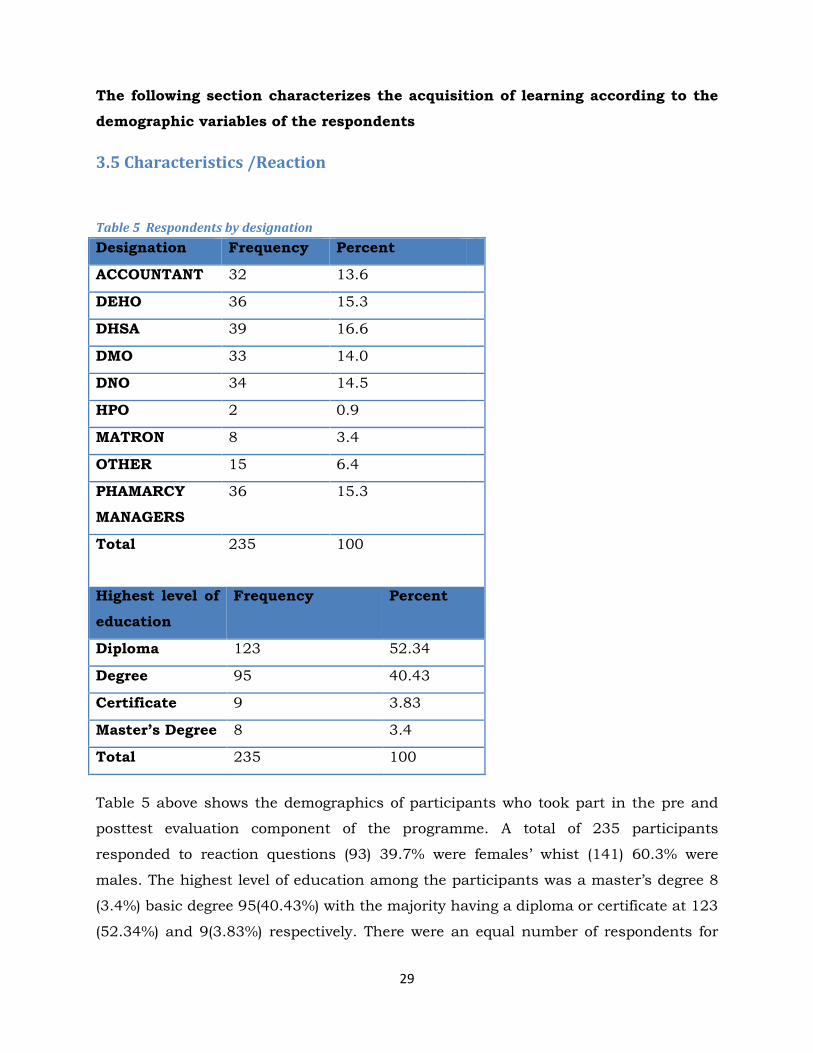
The following section characterizes the acquisition of learning according to the
demographic variables of the respondents
3.5 Characteristics /Reaction
Table 5 Respondents by designation
Designation Frequency Percent
ACCOUNTANT 32 13.6
DEHO 36 15.3
DHSA 39 16.6
DMO 33 14.0
DNO 34 14.5
HPO 2 0.9
MATRON 8 3.4
OTHER 15 6.4
PHAMARCY
MANAGERS
36 15.3
Total 235 100
Highest level of
education
Frequency Percent
Diploma 123 52.34
Degree 95 40.43
Certificate 9 3.83
Master’s Degree 8 3.4
Total 235 100
Table 5 above shows the demographics of participants who took part in the pre and
posttest evaluation component of the programme. A total of 235 participants
responded to reaction questions (93) 39.7% were females’ whist (141) 60.3% were
males. The highest level of education among the participants was a master’s degree 8
(3.4%) basic degree 95(40.43%) with the majority having a diploma or certificate at 123
(52.34%) and 9(3.83%) respectively. There were an equal number of respondents for
30
most categories of the DHE team and a few in the categories of matron, nutritionists
and health promotion officers since these are co-opted members of the DHEs in some
districts.
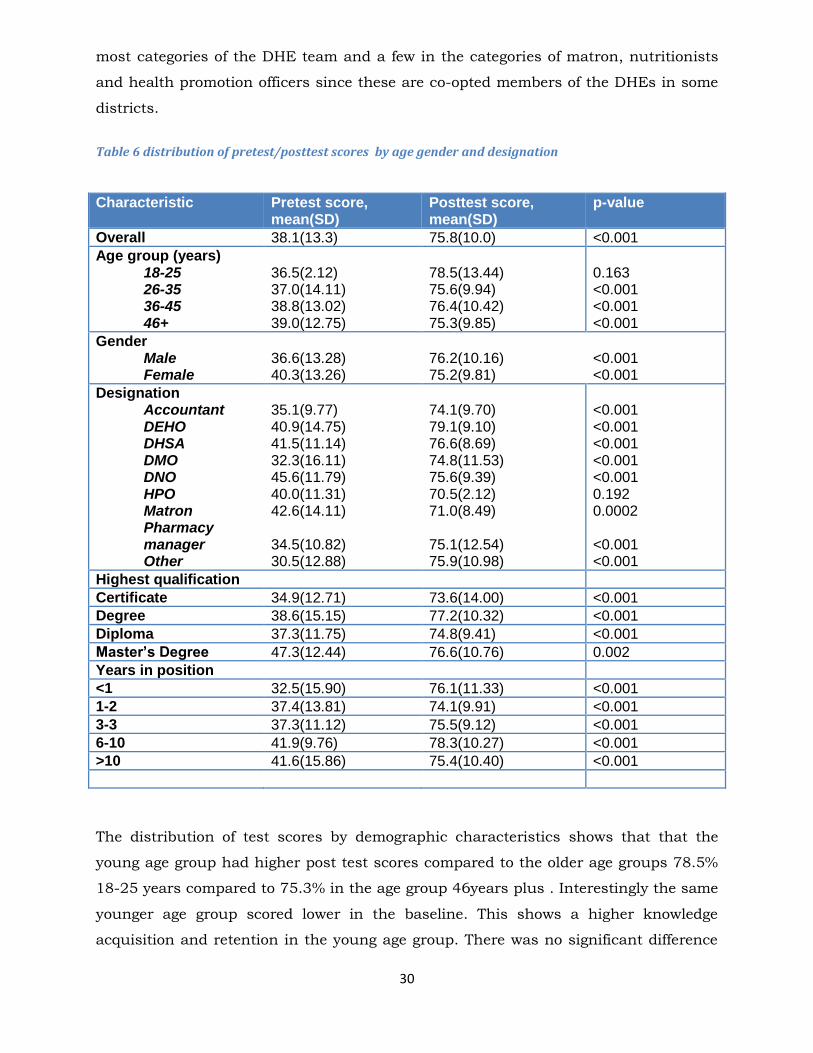
Table 6 distribution of pretest/posttest scores by age gender and designation
Characteristic Pretest score, mean(SD)
Posttest score, mean(SD)
p-value
Overall 38.1(13.3) 75.8(10.0) <0.001
Age group (years) 18-25 26-35 36-45 46+
36.5(2.12) 37.0(14.11) 38.8(13.02) 39.0(12.75)
78.5(13.44) 75.6(9.94) 76.4(10.42) 75.3(9.85)
0.163 <0.001 <0.001 <0.001
Gender Male Female
36.6(13.28) 40.3(13.26)
76.2(10.16) 75.2(9.81)
<0.001 <0.001
Designation Accountant DEHO DHSA DMO DNO HPO Matron Pharmacy manager Other
35.1(9.77) 40.9(14.75) 41.5(11.14) 32.3(16.11) 45.6(11.79) 40.0(11.31) 42.6(14.11) 34.5(10.82) 30.5(12.88)
74.1(9.70) 79.1(9.10) 76.6(8.69) 74.8(11.53) 75.6(9.39) 70.5(2.12) 71.0(8.49) 75.1(12.54) 75.9(10.98)
<0.001 <0.001 <0.001 <0.001 <0.001 0.192 0.0002 <0.001 <0.001
Highest qualification
Certificate 34.9(12.71) 73.6(14.00) <0.001
Degree 38.6(15.15) 77.2(10.32) <0.001
Diploma 37.3(11.75) 74.8(9.41) <0.001
Master’s Degree 47.3(12.44) 76.6(10.76) 0.002
Years in position
<1 32.5(15.90) 76.1(11.33) <0.001
1-2 37.4(13.81) 74.1(9.91) <0.001
3-3 37.3(11.12) 75.5(9.12) <0.001
6-10 41.9(9.76) 78.3(10.27) <0.001
>10 41.6(15.86) 75.4(10.40) <0.001
The distribution of test scores by demographic characteristics shows that that the
young age group had higher post test scores compared to the older age groups 78.5%
18-25 years compared to 75.3% in the age group 46years plus . Interestingly the same
younger age group scored lower in the baseline. This shows a higher knowledge
acquisition and retention in the young age group. There was no significant difference
31
in pre-test scores by age (p=0.750), and also no significant difference in post-test
scores by age (p=0.9001). Regarding designation the District Environmental Health
Officers (DEHO) scored higher on posttest 79.2 highest against 71.0 for matrons and
70.5 % for HPOs although this group were also not fully represented as the other
designations. ANOVA test shows a significant difference in pre-test scores by
designation (p<0.001). Significant differences were noted between DNOs and
Accountants (p=0.032), DNOs and DMOs (p=0.001), DNOs and Pharmacy managers
(p=0.011) and DNOs and others (p=0.006). DNOs scored significantly higher than each
of these groups. In the post test scores no significant differences were noted by
designation.
Overall, Post-test scores were significantly higher compared to pre-test scores
(p<0.001).Scores by gender, scores show that the male scored lower at baseline and
subsequently scored higher on posttest after an educational input 76.2 for males
against 75.2 for females. Females scored significantly higher than males in the pre-
test (though the scores were all low), p=0.037. In the post test there was no significant
difference between males and females (p=0.383)
There was no significant difference in pre-test and post-test scores by educational
attainment. However the respondents with a master’s degree scored higher at both
pretest 47.3% compared to those with a certificate who scored 34.9%. Post test results
show that those with a basic degree and master’s degree scored higher than other
groups 77.2% for degreed and 76.6% for master’s degree
The mean scores according to work experience ANOVA test indicates a significant
difference in pre-test scores by years in present position. Those with 6-10 years in
present position scored significantly higher than those with less than one year
(p=0.022), than those with more than 10 years scored significantly higher than those
with less than 1 year (p=0.036). There was no significant difference by years of work
experience. There is no doubt that health professionals that are more experienced do
acquire some background knowledge of how the health care system is run and the
requirements thereof.

32
6. Analysis On Pretest Scores
A total of 355 DHEs from 61 districts responded to the pre and post-test
questionnaires during the five day health leadership, management and governance
training workshops. Data was collected from 235 participants. Kirkpatrick’s model of
evaluation (reaction, learning, behaviour and results) was used to develop a
framework for assessing training outcomes. A questionnaire based on the expected
competencies was used to collect data from the participants before and after training.
Measurement was based on whether there was an increase in knowledge - before
and after.
The sample was made up of 39.7% females and 60.3% males and these comprised of
medical doctors, nurses, health services administrators, environmental health officers,
health promotion officers, pharmacists, accountants and nutritionists. 92.77% of the
sample had either obtained a diploma or degree as a basic qualification in their
respective professions and 3.4% had undergone post graduate training. 75% had 3-6
years of work experience. 41.7 % were in the age group 26-35 years.
Learning focused on pre and post- test scores. The mean score for pretest was 38.1
(SD 13.3) .Post scores were 75.8 % (SD 10.0) Post test scores were significantly higher
than pre-test scores (p<0.001). There was statistical significance between males and
females on pretest scores p value 0.037.No statistical significance was observed
between male and female at post testing implying an overall positive knowledge gain
for the whole group from the training. Multiple comparison test indicates a significant
difference in pre-test scores between Nurses and Accountants (p=0.018), between
Nurses and medical doctors (p=0.018) and between Nurses and Pharmacy managers
(p=0.017), with nurses scoring significantly higher. However, in the post-test scores
there was no significant difference between Professions although the environmental
health officers tended to score higher in their posttest scores. ANOVA test indicates a
significant difference in pre-test scores by years in present position Those with 6-10
years in present position scored significantly higher than those with less than one year
(p=0.022), than those with more than 10 years scored significantly higher than those
with less than 1 year (p=0.036).
33
Conclusions for Level 2
Scores for posttest show a definite increase in knowledge across all groups showing
that learning did take place and was not influenced by the same factors at pre-testing
level. Overly the training had an effect size of 39% which is the difference between the
average mark for all participants in the pre training test and in the post training test.
The younger age group tended to score higher in their posttest scores showing that the
younger health professionals may need to be provided with in-service training
constantly so that they easily acquire relevant information to ensure professional
practice. Being female was related to high pretest scores .This could be due to the fact
that more female health professionals are in place and they also tend to have more
experience in the same position. Educational level plays a significant role in the
additional acquisition of knowledge as evidenced by the fact that those with a basic
degree and master’s degree scored higher than other groups. Respondent with more
years of experience in the workplace had higher posttest scores indicating the
influence of experience in the learning process. There is no doubt that health
professionals that are more experienced do acquire some background knowledge of how
the health care system is run and what they need to know to better deliver quality
services. In service training should be competency based so as to ensure success,
relevance and usefulness in the strengthening of the health care systems. Our training
provided much needed skills required by DHE for managing district public health
activities. The content of our training was based on the roles and functions of the
DHEs thus making it very relevant to their day to day activities.
3.7 Change of behavior after training
This section presents results on the assessment of the knowledge and attitudes of
DHEs in terms of the HLMG knowledge gained and the cognition of how DHEs
perceive themselves to be applying the knowledge gained in their day to day functions.
The assessment was based on the modules covered during HLMG training.
Level 3— Change of behavior after training
To assess if there are any changes in behavior after the HLMG training.
To assess the degree to which trained health managers are engaged in the
behaviours targeted during HLMG training (e.g. holding meetings regularly working as
a team utilizing health information for planning)
34
To identify if the training is contributing towards an increase in discrete skills and
techniques for leadership management and governance
In order to assess the level 3 on the Kirkpatrick’s model interviews were conducted
with DHE members in the selected districts
Overall mean score for these 16 items was 30% (SD=7.3%). These questions were
asked in the negative. The scores were reversed so that the scores are measured in the
positive sense and the overall mean perception score was 90.5% (SD=7.3%).
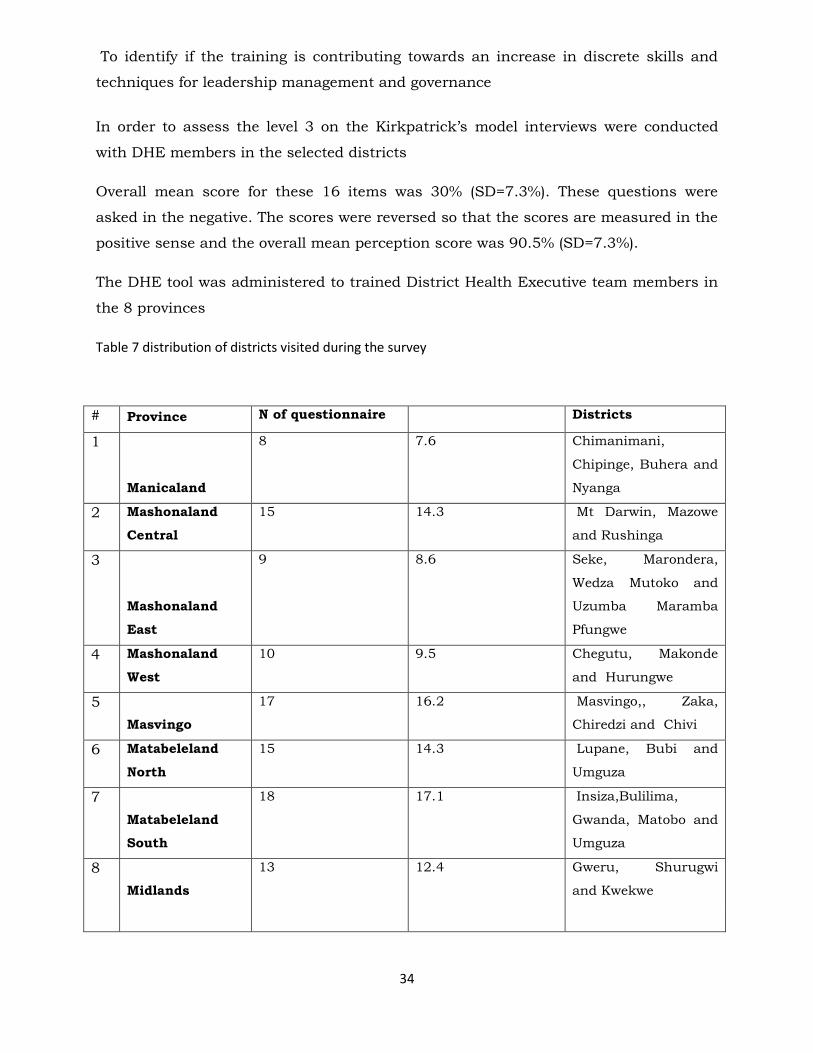
The DHE tool was administered to trained District Health Executive team members in
the 8 provinces
Table 7 distribution of districts visited during the survey
# Province N of questionnaire Districts
1
Manicaland
8 7.6 Chimanimani,
Chipinge, Buhera and
Nyanga
2 Mashonaland
Central
15 14.3 Mt Darwin, Mazowe
and Rushinga
3
Mashonaland
East
9 8.6 Seke, Marondera,
Wedza Mutoko and
Uzumba Maramba
Pfungwe
4 Mashonaland
West
10 9.5 Chegutu, Makonde
and Hurungwe
5
Masvingo
17 16.2 Masvingo,, Zaka,
Chiredzi and Chivi
6 Matabeleland
North
15 14.3 Lupane, Bubi and
Umguza
7
Matabeleland
South
18 17.1 Insiza,Bulilima,
Gwanda, Matobo and
Umguza
8
Midlands
13 12.4 Gweru, Shurugwi
and Kwekwe
35
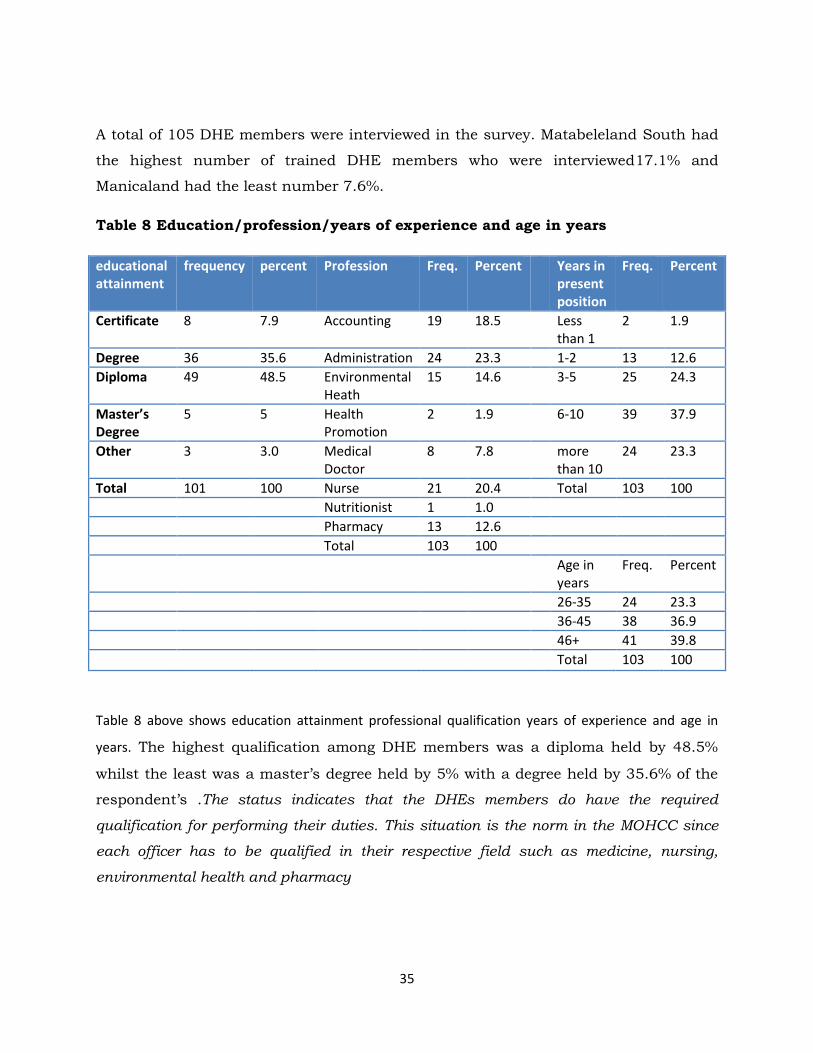
A total of 105 DHE members were interviewed in the survey. Matabeleland South had
the highest number of trained DHE members who were interviewed17.1% and
Manicaland had the least number 7.6%.
Table 8 Education/profession/years of experience and age in years
educational attainment
frequency percent Profession Freq. Percent Years in present position
Freq. Percent
Certificate 8 7.9 Accounting 19 18.5 Less than 1
2 1.9
Degree 36 35.6 Administration 24 23.3 1-2 13 12.6
Diploma 49 48.5 Environmental Heath
15 14.6 3-5 25 24.3
Master’s Degree
5 5 Health Promotion
2 1.9 6-10 39 37.9
Other 3 3.0 Medical Doctor
8 7.8 more than 10
24 23.3
Total 101 100 Nurse 21 20.4 Total 103 100
Nutritionist 1 1.0
Pharmacy 13 12.6
Total 103 100
Age in years
Freq. Percent
26-35 24 23.3
36-45 38 36.9
46+ 41 39.8
Total 103 100
Table 8 above shows education attainment professional qualification years of experience and age in
years. The highest qualification among DHE members was a diploma held by 48.5%
whilst the least was a master’s degree held by 5% with a degree held by 35.6% of the
respondent’s .The status indicates that the DHEs members do have the required
qualification for performing their duties. This situation is the norm in the MOHCC since
each officer has to be qualified in their respective field such as medicine, nursing,
environmental health and pharmacy
36
The findings indicate that the majority of respondents were in administration 41.8%
(23.3%, 18.5%) Two respondents did not specify their professions. 14.6% were
environmental health officers
It is pleasing to note that more respondents have been in position for more than 3
years with the majority 37.9% having been in position for more than five years with
more than ten years for a good 23.3% of the respondents. Two respondents did not
specify their durations in their current positions. More years in one place is obviously
of advantage for an organization since stability is in built where people have more
experience .Institutional memory can be passed on and new cadres are reassured of
mentorship and guidance.
The majority of respondents were in the age group 36-46+ years. The older age group
formed 77% in total .The older age group also indicates stability in an organization since
the young age groups tend to be very mobile thus upsetting the status quo and functions
of an organization
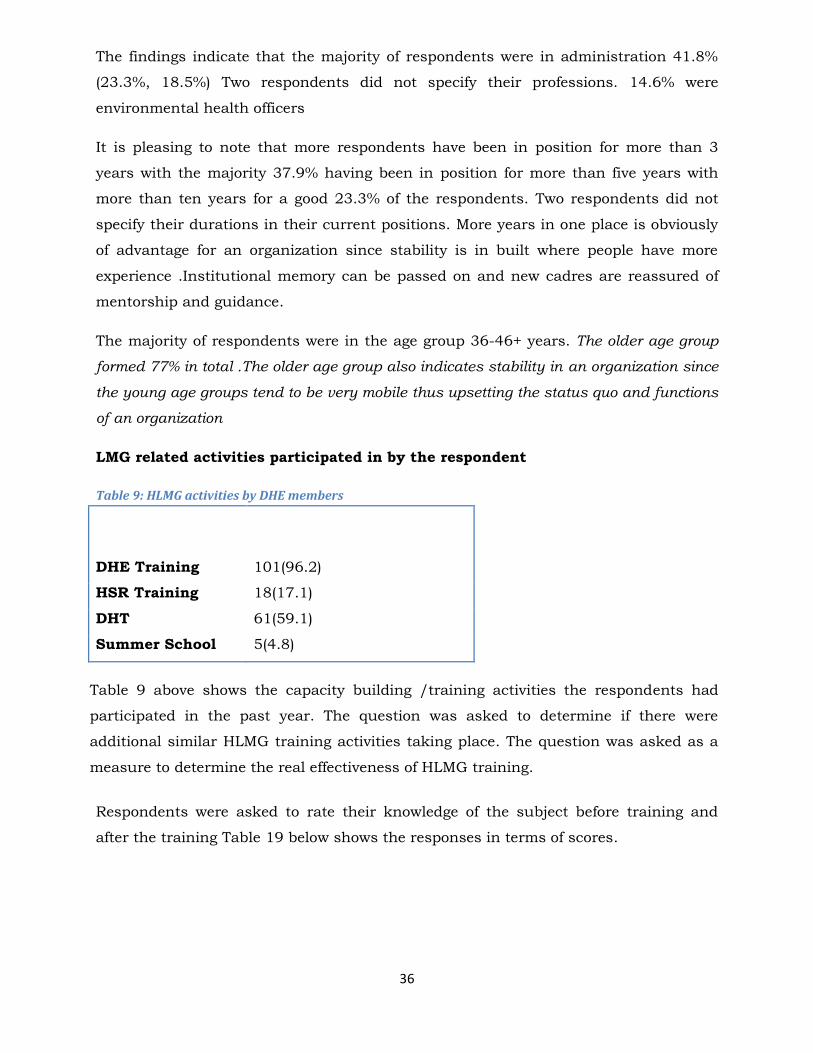
LMG related activities participated in by the respondent
Table 9: HLMG activities by DHE members
Activity Number of respondents, n
(%)
DHE Training 101(96.2)
HSR Training 18(17.1)
DHT 61(59.1)
Summer School 5(4.8)
Table 9 above shows the capacity building /training activities the respondents had
participated in the past year. The question was asked to determine if there were
additional similar HLMG training activities taking place. The question was asked as a
measure to determine the real effectiveness of HLMG training.
Respondents were asked to rate their knowledge of the subject before training and
after the training Table 19 below shows the responses in terms of scores.
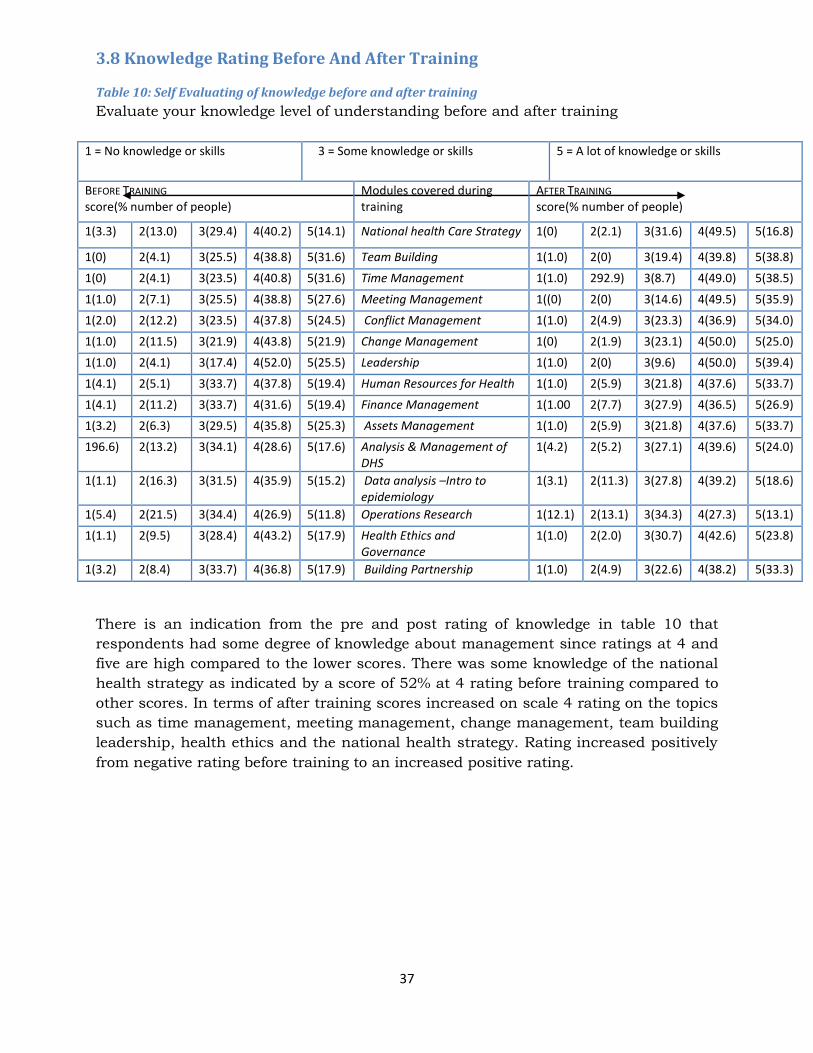
37
3.8 Knowledge Rating Before And After Training
Table 10: Self Evaluating of knowledge before and after training
Evaluate your knowledge level of understanding before and after training
1 = No knowledge or skills 3 = Some knowledge or skills 5 = A lot of knowledge or skills
BEFORE TRAINING score(% number of people)
Modules covered during training
AFTER TRAINING score(% number of people)
1(3.3) 2(13.0) 3(29.4) 4(40.2) 5(14.1) National health Care Strategy 1(0) 2(2.1) 3(31.6) 4(49.5) 5(16.8)
1(0) 2(4.1) 3(25.5) 4(38.8) 5(31.6) Team Building 1(1.0) 2(0) 3(19.4) 4(39.8) 5(38.8)
1(0) 2(4.1) 3(23.5) 4(40.8) 5(31.6) Time Management 1(1.0) 292.9) 3(8.7) 4(49.0) 5(38.5)
1(1.0) 2(7.1) 3(25.5) 4(38.8) 5(27.6) Meeting Management 1((0) 2(0) 3(14.6) 4(49.5) 5(35.9)
1(2.0) 2(12.2) 3(23.5) 4(37.8) 5(24.5) Conflict Management 1(1.0) 2(4.9) 3(23.3) 4(36.9) 5(34.0)
1(1.0) 2(11.5) 3(21.9) 4(43.8) 5(21.9) Change Management 1(0) 2(1.9) 3(23.1) 4(50.0) 5(25.0)
1(1.0) 2(4.1) 3(17.4) 4(52.0) 5(25.5) Leadership 1(1.0) 2(0) 3(9.6) 4(50.0) 5(39.4)
1(4.1) 2(5.1) 3(33.7) 4(37.8) 5(19.4) Human Resources for Health 1(1.0) 2(5.9) 3(21.8) 4(37.6) 5(33.7)
1(4.1) 2(11.2) 3(33.7) 4(31.6) 5(19.4) Finance Management 1(1.00 2(7.7) 3(27.9) 4(36.5) 5(26.9)
1(3.2) 2(6.3) 3(29.5) 4(35.8) 5(25.3) Assets Management 1(1.0) 2(5.9) 3(21.8) 4(37.6) 5(33.7)
196.6) 2(13.2) 3(34.1) 4(28.6) 5(17.6) Analysis & Management of DHS
1(4.2) 2(5.2) 3(27.1) 4(39.6) 5(24.0)
1(1.1) 2(16.3) 3(31.5) 4(35.9) 5(15.2) Data analysis –Intro to epidemiology
1(3.1) 2(11.3) 3(27.8) 4(39.2) 5(18.6)
1(5.4) 2(21.5) 3(34.4) 4(26.9) 5(11.8) Operations Research 1(12.1) 2(13.1) 3(34.3) 4(27.3) 5(13.1)
1(1.1) 2(9.5) 3(28.4) 4(43.2) 5(17.9) Health Ethics and Governance
1(1.0) 2(2.0) 3(30.7) 4(42.6) 5(23.8)
1(3.2) 2(8.4) 3(33.7) 4(36.8) 5(17.9) Building Partnership 1(1.0) 2(4.9) 3(22.6) 4(38.2) 5(33.3)
There is an indication from the pre and post rating of knowledge in table 10 that
respondents had some degree of knowledge about management since ratings at 4 and
five are high compared to the lower scores. There was some knowledge of the national
health strategy as indicated by a score of 52% at 4 rating before training compared to
other scores. In terms of after training scores increased on scale 4 rating on the topics
such as time management, meeting management, change management, team building
leadership, health ethics and the national health strategy. Rating increased positively
from negative rating before training to an increased positive rating.
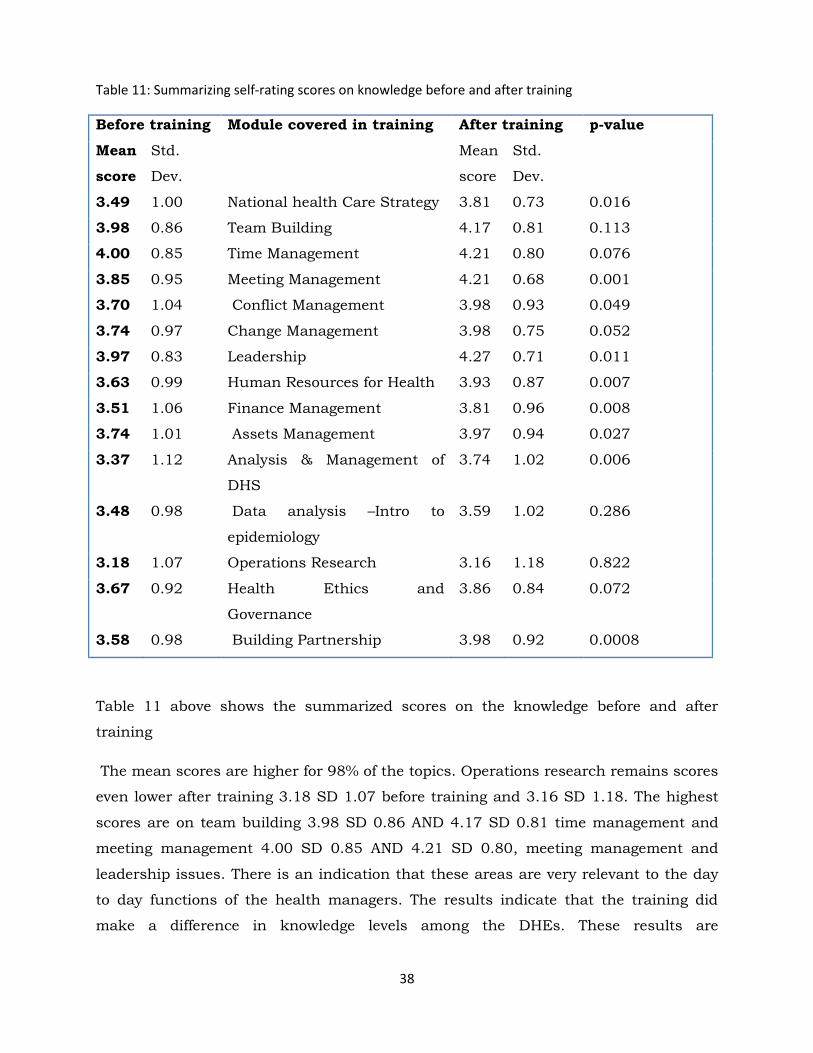
38
Table 11: Summarizing self-rating scores on knowledge before and after training
Before training Module covered in training After training p-value
Mean
score
Std.
Dev.
Mean
score
Std.
Dev.
3.49 1.00 National health Care Strategy 3.81 0.73 0.016
3.98 0.86 Team Building 4.17 0.81 0.113
4.00 0.85 Time Management 4.21 0.80 0.076
3.85 0.95 Meeting Management 4.21 0.68 0.001
3.70 1.04 Conflict Management 3.98 0.93 0.049
3.74 0.97 Change Management 3.98 0.75 0.052
3.97 0.83 Leadership 4.27 0.71 0.011
3.63 0.99 Human Resources for Health 3.93 0.87 0.007
3.51 1.06 Finance Management 3.81 0.96 0.008
3.74 1.01 Assets Management 3.97 0.94 0.027
3.37 1.12 Analysis & Management of
DHS
3.74 1.02 0.006
3.48 0.98 Data analysis –Intro to
epidemiology
3.59 1.02 0.286
3.18 1.07 Operations Research 3.16 1.18 0.822
3.67 0.92 Health Ethics and
Governance
3.86 0.84 0.072
3.58 0.98 Building Partnership 3.98 0.92 0.0008
Table 11 above shows the summarized scores on the knowledge before and after
training
The mean scores are higher for 98% of the topics. Operations research remains scores
even lower after training 3.18 SD 1.07 before training and 3.16 SD 1.18. The highest
scores are on team building 3.98 SD 0.86 AND 4.17 SD 0.81 time management and
meeting management 4.00 SD 0.85 AND 4.21 SD 0.80, meeting management and
leadership issues. There is an indication that these areas are very relevant to the day
to day functions of the health managers. The results indicate that the training did
make a difference in knowledge levels among the DHEs. These results are

39
corroborated by our findings on the pre and post test scores. It is pleasing to note that
the evaluation asked respondents to rate themselves close to a year after training
whereas the pre and posttest took place during the HLMG training.
3.8.1 Application Of Knowledge And Skills From The LMG Training
A question was asked in which DHE members were asked to score the difference in
performance in terms of before and after the training. The area of improvement was
based on the modules covered during training from which the HLMP developed custom
indicators for monitoring the training. The scores are presented below in table 21
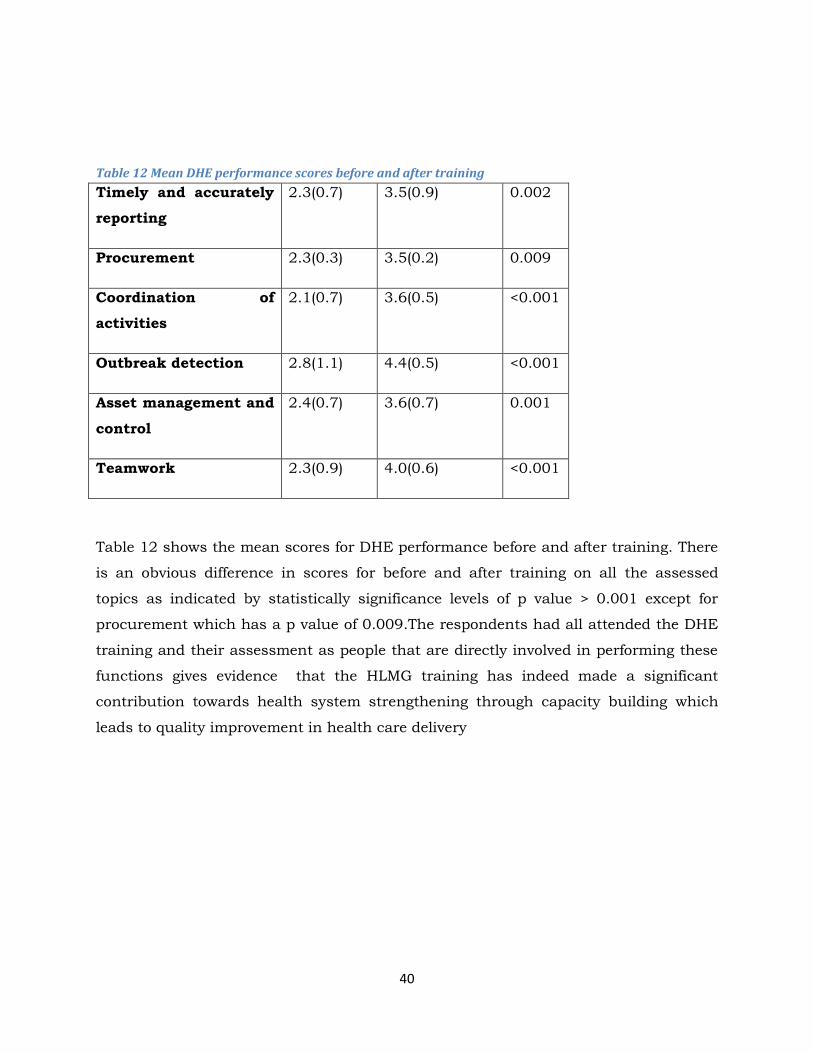
40
Table 12 Mean DHE performance scores before and after training
Timely and accurately
reporting
2.3(0.7) 3.5(0.9) 0.002
Procurement 2.3(0.3) 3.5(0.2) 0.009
Coordination of
activities
2.1(0.7) 3.6(0.5) <0.001
Outbreak detection 2.8(1.1) 4.4(0.5) <0.001
Asset management and
control
2.4(0.7) 3.6(0.7) 0.001
Teamwork 2.3(0.9) 4.0(0.6) <0.001
Table 12 shows the mean scores for DHE performance before and after training. There
is an obvious difference in scores for before and after training on all the assessed
topics as indicated by statistically significance levels of p value > 0.001 except for
procurement which has a p value of 0.009.The respondents had all attended the DHE
training and their assessment as people that are directly involved in performing these
functions gives evidence that the HLMG training has indeed made a significant
contribution towards health system strengthening through capacity building which
leads to quality improvement in health care delivery
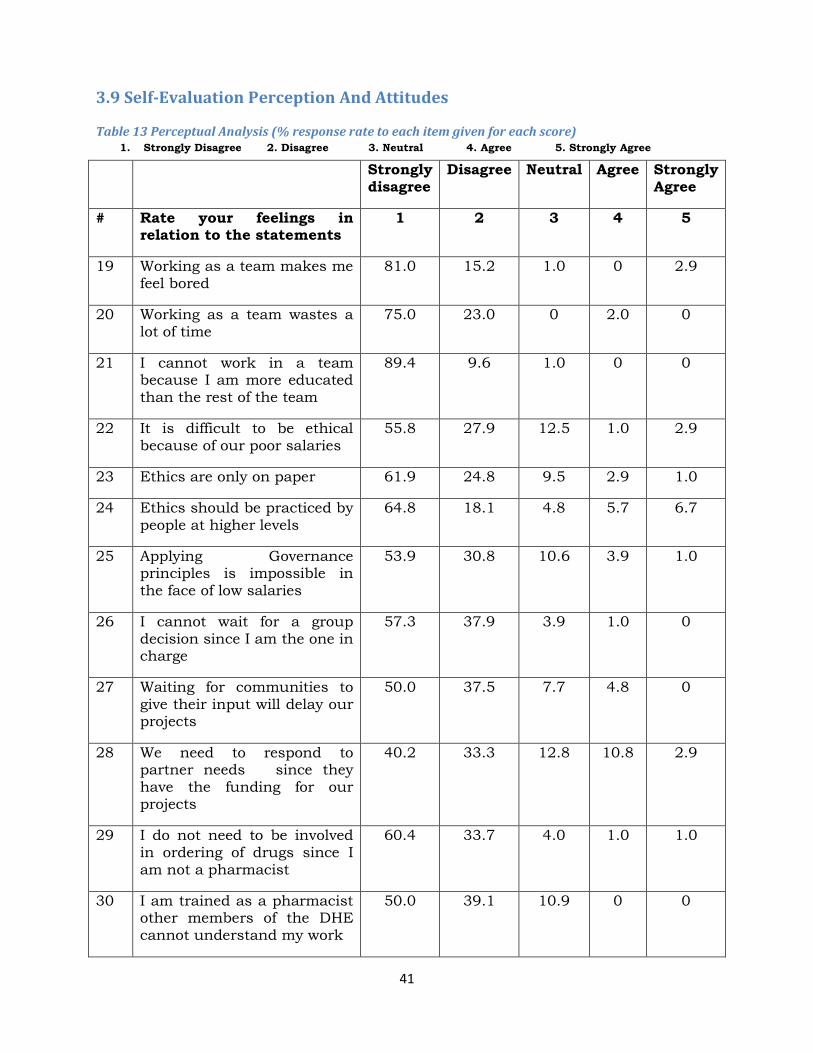
41
3.9 Self-Evaluation Perception And Attitudes
Table 13 Perceptual Analysis (% response rate to each item given for each score) 1. Strongly Disagree 2. Disagree 3. Neutral 4. Agree 5. Strongly Agree
Strongly disagree
Disagree Neutral Agree Strongly Agree
# Rate your feelings in relation to the statements
1 2 3 4 5
19 Working as a team makes me feel bored
81.0 15.2 1.0 0 2.9
20 Working as a team wastes a lot of time
75.0 23.0 0 2.0 0
21 I cannot work in a team because I am more educated than the rest of the team
89.4 9.6 1.0 0 0
22 It is difficult to be ethical because of our poor salaries
55.8 27.9 12.5 1.0 2.9
23 Ethics are only on paper 61.9 24.8 9.5 2.9 1.0
24 Ethics should be practiced by people at higher levels
64.8 18.1 4.8 5.7 6.7
25 Applying Governance principles is impossible in the face of low salaries
53.9 30.8 10.6 3.9 1.0
26 I cannot wait for a group decision since I am the one in charge
57.3 37.9 3.9 1.0 0
27 Waiting for communities to give their input will delay our projects
50.0 37.5 7.7 4.8 0
28 We need to respond to partner needs since they have the funding for our projects
40.2 33.3 12.8 10.8 2.9
29 I do not need to be involved in ordering of drugs since I am not a pharmacist
60.4 33.7 4.0 1.0 1.0
30 I am trained as a pharmacist other members of the DHE cannot understand my work
50.0 39.1 10.9 0 0
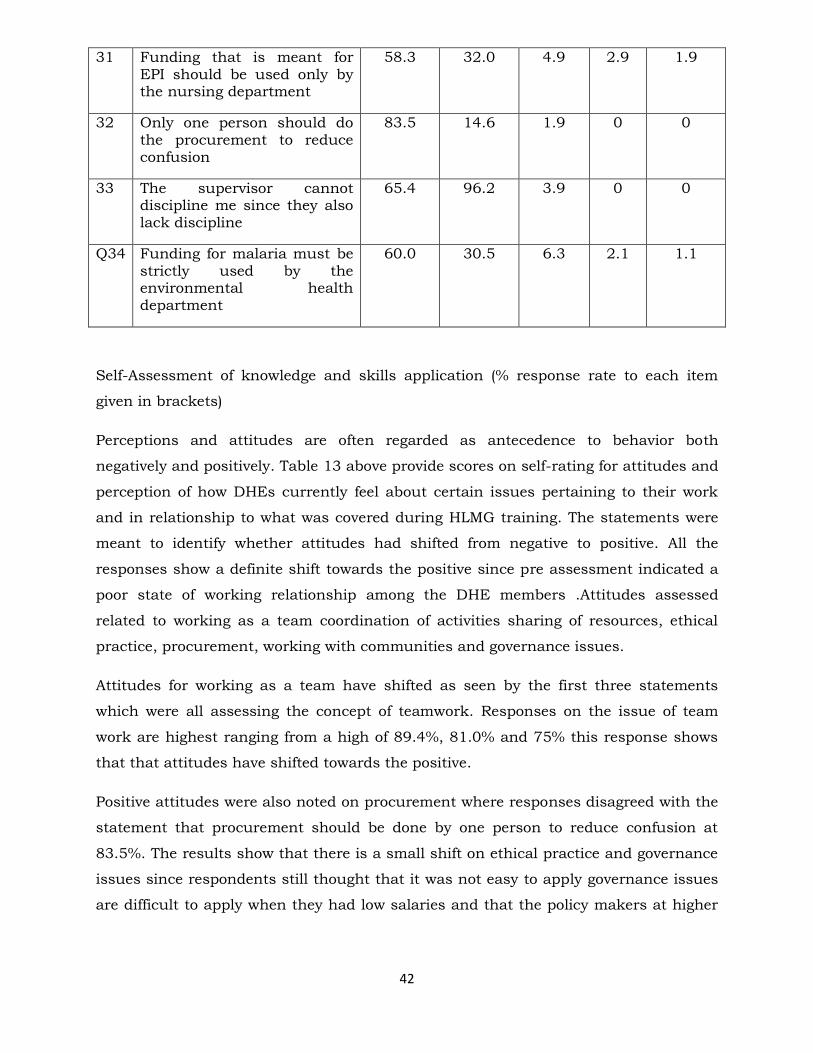
42
31 Funding that is meant for EPI should be used only by the nursing department
58.3 32.0 4.9 2.9 1.9
32 Only one person should do the procurement to reduce confusion
83.5 14.6 1.9 0 0
33 The supervisor cannot discipline me since they also lack discipline
65.4 96.2 3.9 0 0
Q34 Funding for malaria must be strictly used by the environmental health department
60.0 30.5 6.3 2.1 1.1
Self-Assessment of knowledge and skills application (% response rate to each item
given in brackets)
Perceptions and attitudes are often regarded as antecedence to behavior both
negatively and positively. Table 13 above provide scores on self-rating for attitudes and
perception of how DHEs currently feel about certain issues pertaining to their work
and in relationship to what was covered during HLMG training. The statements were
meant to identify whether attitudes had shifted from negative to positive. All the
responses show a definite shift towards the positive since pre assessment indicated a
poor state of working relationship among the DHE members .Attitudes assessed
related to working as a team coordination of activities sharing of resources, ethical
practice, procurement, working with communities and governance issues.
Attitudes for working as a team have shifted as seen by the first three statements
which were all assessing the concept of teamwork. Responses on the issue of team
work are highest ranging from a high of 89.4%, 81.0% and 75% this response shows
that that attitudes have shifted towards the positive.
Positive attitudes were also noted on procurement where responses disagreed with the
statement that procurement should be done by one person to reduce confusion at
83.5%. The results show that there is a small shift on ethical practice and governance
issues since respondents still thought that it was not easy to apply governance issues
are difficult to apply when they had low salaries and that the policy makers at higher
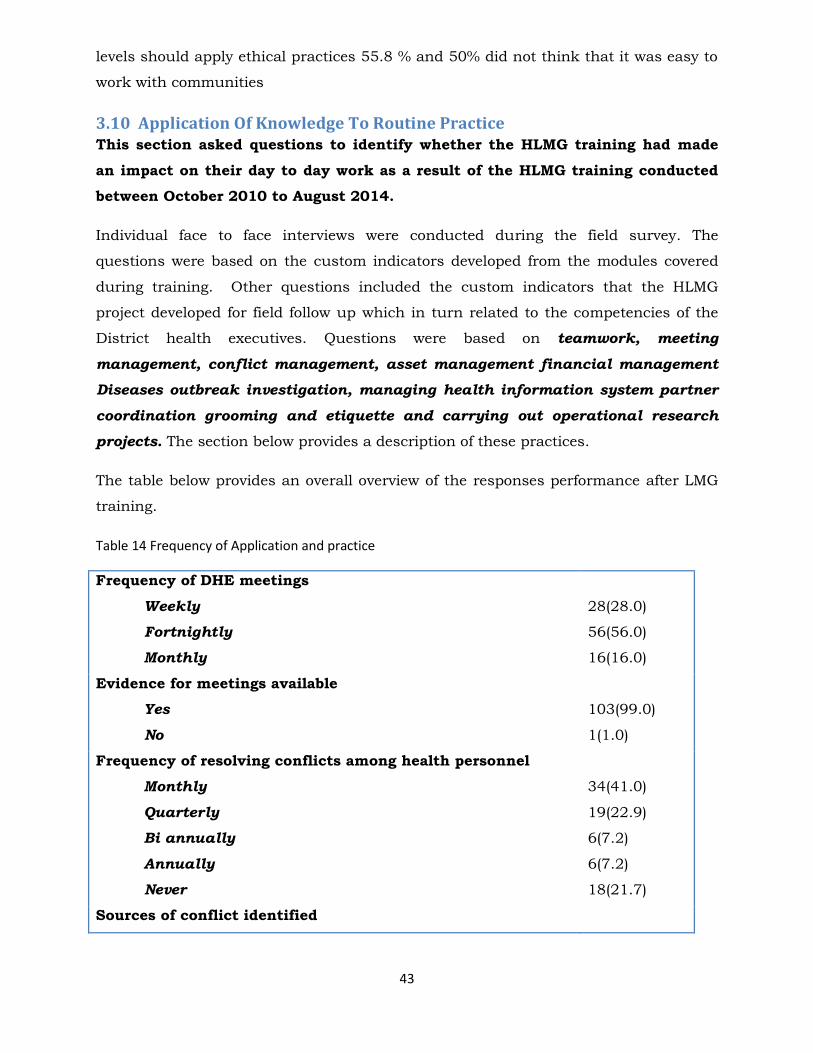
43
levels should apply ethical practices 55.8 % and 50% did not think that it was easy to
work with communities
3.10 Application Of Knowledge To Routine Practice This section asked questions to identify whether the HLMG training had made
an impact on their day to day work as a result of the HLMG training conducted
between October 2010 to August 2014.
Individual face to face interviews were conducted during the field survey. The
questions were based on the custom indicators developed from the modules covered
during training. Other questions included the custom indicators that the HLMG
project developed for field follow up which in turn related to the competencies of the
District health executives. Questions were based on teamwork, meeting
management, conflict management, asset management financial management
Diseases outbreak investigation, managing health information system partner
coordination grooming and etiquette and carrying out operational research
projects. The section below provides a description of these practices.
The table below provides an overall overview of the responses performance after LMG
training.
Table 14 Frequency of Application and practice
Frequency of DHE meetings
Weekly
Fortnightly
Monthly
28(28.0)
56(56.0)
16(16.0)
Evidence for meetings available
Yes
No
103(99.0)
1(1.0)
Frequency of resolving conflicts among health personnel
Monthly
Quarterly
Bi annually
Annually
Never
34(41.0)
19(22.9)
6(7.2)
6(7.2)
18(21.7)
Sources of conflict identified
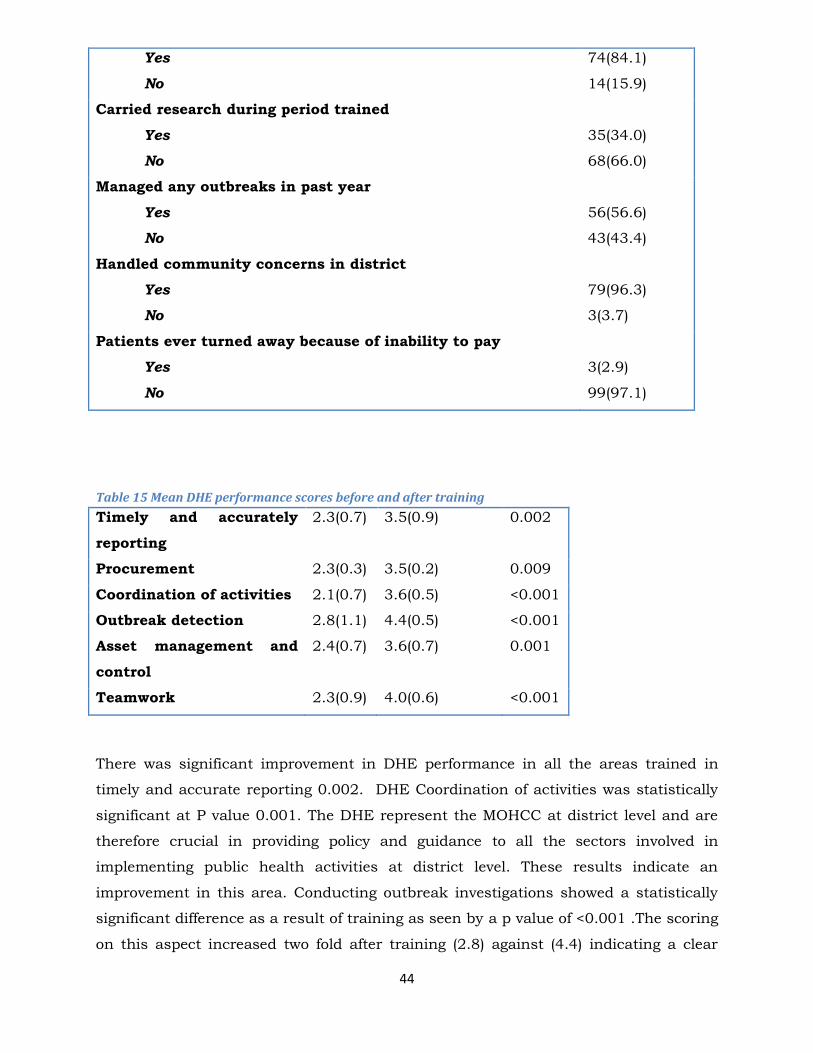
44
Yes
No
74(84.1)
14(15.9)
Carried research during period trained
Yes
No
35(34.0)
68(66.0)
Managed any outbreaks in past year
Yes
No
56(56.6)
43(43.4)
Handled community concerns in district
Yes
No
79(96.3)
3(3.7)
Patients ever turned away because of inability to pay
Yes
No
3(2.9)
99(97.1)
Table 15 Mean DHE performance scores before and after training
Timely and accurately
reporting
2.3(0.7) 3.5(0.9) 0.002
Procurement 2.3(0.3) 3.5(0.2) 0.009
Coordination of activities 2.1(0.7) 3.6(0.5) <0.001
Outbreak detection 2.8(1.1) 4.4(0.5) <0.001
Asset management and
control
2.4(0.7) 3.6(0.7) 0.001
Teamwork 2.3(0.9) 4.0(0.6) <0.001
There was significant improvement in DHE performance in all the areas trained in
timely and accurate reporting 0.002. DHE Coordination of activities was statistically
significant at P value 0.001. The DHE represent the MOHCC at district level and are
therefore crucial in providing policy and guidance to all the sectors involved in
implementing public health activities at district level. These results indicate an
improvement in this area. Conducting outbreak investigations showed a statistically
significant difference as a result of training as seen by a p value of <0.001 .The scoring
on this aspect increased two fold after training (2.8) against (4.4) indicating a clear
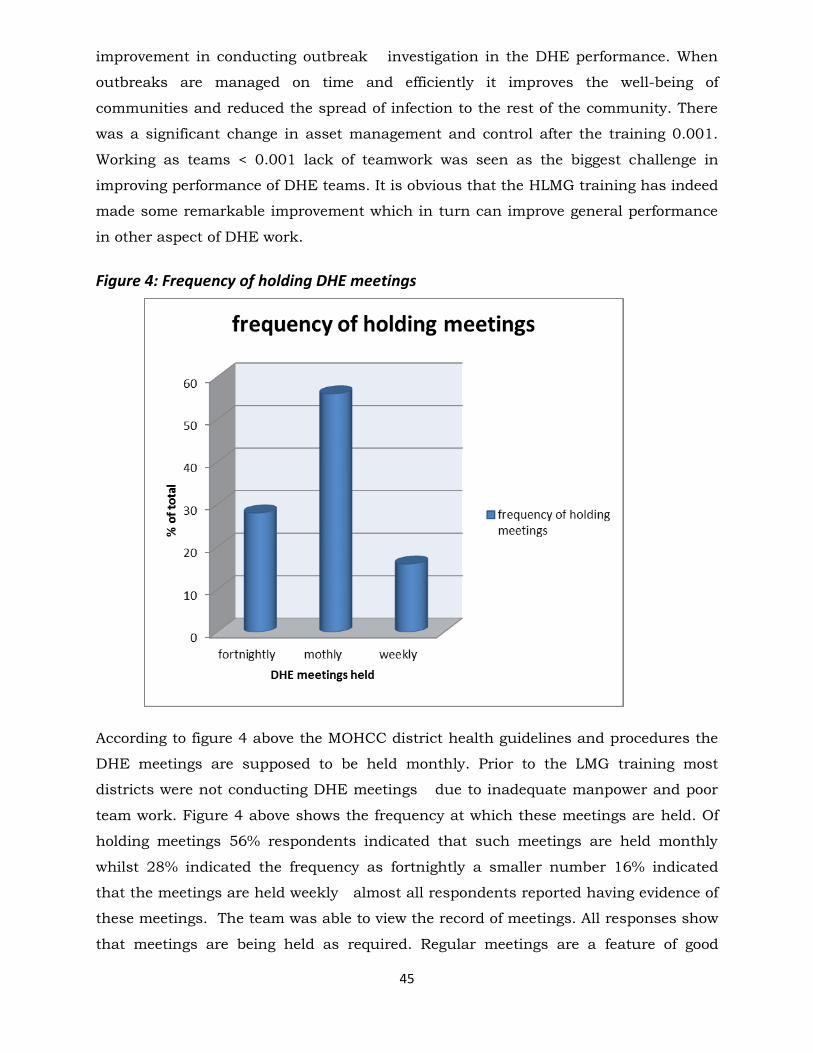
45
improvement in conducting outbreak investigation in the DHE performance. When
outbreaks are managed on time and efficiently it improves the well-being of
communities and reduced the spread of infection to the rest of the community. There
was a significant change in asset management and control after the training 0.001.
Working as teams < 0.001 lack of teamwork was seen as the biggest challenge in
improving performance of DHE teams. It is obvious that the HLMG training has indeed
made some remarkable improvement which in turn can improve general performance
in other aspect of DHE work.
Figure 4: Frequency of holding DHE meetings
According to figure 4 above the MOHCC district health guidelines and procedures the
DHE meetings are supposed to be held monthly. Prior to the LMG training most
districts were not conducting DHE meetings due to inadequate manpower and poor
team work. Figure 4 above shows the frequency at which these meetings are held. Of
holding meetings 56% respondents indicated that such meetings are held monthly
whilst 28% indicated the frequency as fortnightly a smaller number 16% indicated
that the meetings are held weekly almost all respondents reported having evidence of
these meetings. The team was able to view the record of meetings. All responses show
that meetings are being held as required. Regular meetings are a feature of good
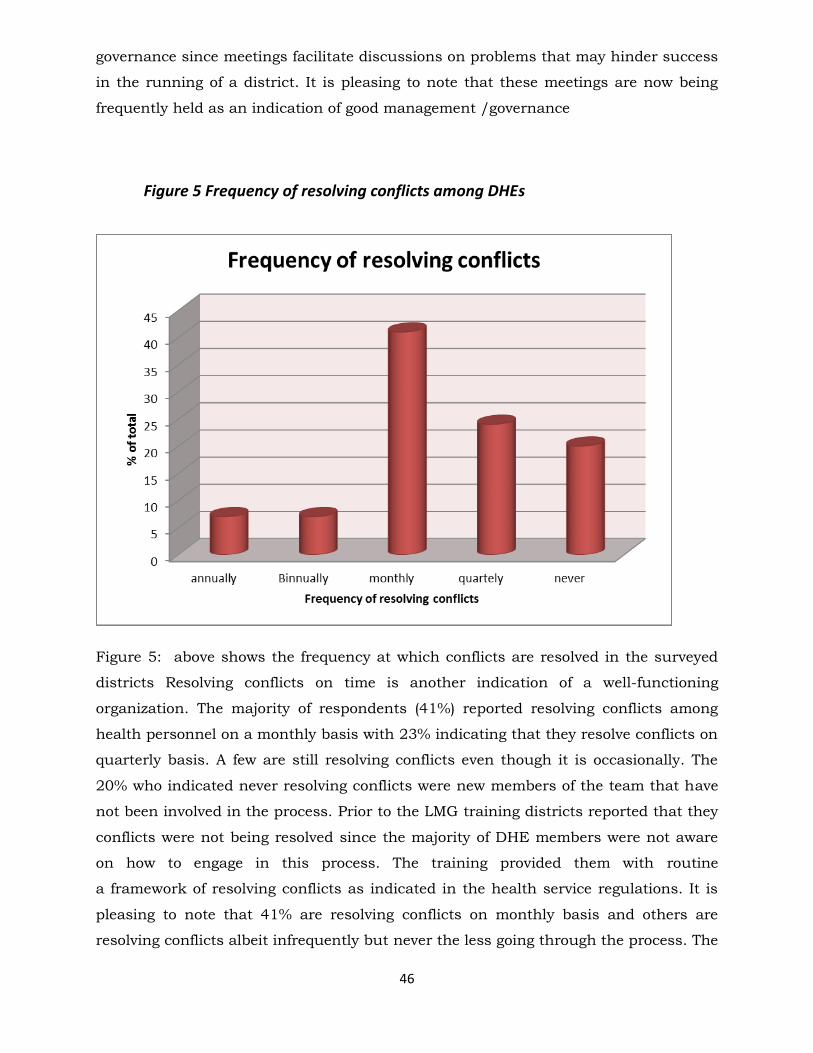
46
governance since meetings facilitate discussions on problems that may hinder success
in the running of a district. It is pleasing to note that these meetings are now being
frequently held as an indication of good management /governance
Figure 5 Frequency of resolving conflicts among DHEs
Figure 5: above shows the frequency at which conflicts are resolved in the surveyed
districts Resolving conflicts on time is another indication of a well-functioning
organization. The majority of respondents (41%) reported resolving conflicts among
health personnel on a monthly basis with 23% indicating that they resolve conflicts on
quarterly basis. A few are still resolving conflicts even though it is occasionally. The
20% who indicated never resolving conflicts were new members of the team that have
not been involved in the process. Prior to the LMG training districts reported that they
conflicts were not being resolved since the majority of DHE members were not aware
on how to engage in this process. The training provided them with routine
a framework of resolving conflicts as indicated in the health service regulations. It is
pleasing to note that 41% are resolving conflicts on monthly basis and others are
resolving conflicts albeit infrequently but never the less going through the process. The
47
types of conflicts being resolved include: Absenteeism, accommodation conflicts,
misappropriation of funds, social, staff disputes, insubordination, and teamwork
conflicts. The sources of conflicts were indicated as
Professional diversity, Drunkenness and lack of Respect, limited resources,
Absenteeism, difference in knowledge levels, frustration due to working environment,
frustration due to working environment, goal differences
Welfare of DHT members
This aspect of evaluation also focused on the improvement of the work environment
since part of the LMG training covered aspects on how districts can improve their
work environment in order to keep morale high for their teams as part of managing
wellness in the workplace. The following were some ways DHE had improved their
workplace environment for the benefit of all health workers working at district level
There was a general indication that some DHEs had gone out of their way to cater for
the welfare of their staff by putting in place recreational facilities such as soccer
teams, netball facilities, and creating environments in which games such as volleyball,
darts, snooker could be played in a relaxed environment. Other districts indicated that
they had identified a room where staff can watch TV together and access the internet.
Most importantly was the putting in place support mechanisms for, psycho-social
support through group interaction. However, 54% of the surveyed districts had not
put anything in place for their workmates.
Asset Registers
One of the problems before training was the fact that most districts did not have asset
registers in place and this was causing a lot of pilfering of Government property since
the assets could not be monitored 88% of the respondents said their offices now kept
an asset register that indicates all the assets that the district owns and this could be
produced at any time when required. The asset register is now being regularly updated
in accordance with any newly acquired assets. Ethical principles are being adhered to
during procurement .All the DHE members are now participating in the procurement
process
Operational Research
One of the key activities in the strengthening of health care systems is the need to use
evidence in the planning of public health interventions and in developing indicators for
48
monitoring and evaluation. The LMG training included a component of carrying out
operational research. The districts were encouraged to bring their T5 forms to the
training for problem identification. The analysis of these forms a basis for conducting
operational research .At the end of the workshop they presented a proposal on how
they were going to carry out the research. The evaluation identified that very few
districts were carrying out research. As planned after the workshop only 34% reported
having carried out any research. Various reasons were given important of which were
lack of time capacity and resources to conduct the operational research
Outbreak investigation/management
57% of the respondents reported carrying out outbreak investigation and
successfully managing the outbreak. Malaria was the most common outbreak
investigated and successfully managed. The malaria programme is funded through
global funds. It is therefore apparent that the funding provided provides resources and
maybe the motivation to carry out malaria outbreak investigation.
Community concerns Patients’ ability to pay
96% of the respondents reported having responded to community concerns in the
districts. Examples of Community concerns included cost of health care services,
waiting time at the hospital and general attitudes of health care workers towards the
community 3% of the respondents reported that some patients were being turned
away because of inability to pay for services.
RBF and HTF beneficiaries
Thirty two (32) respondents reported that their districts were beneficiaries of RBF and
74 reported their districts being HTF beneficiaries. Three respondents from Bulilima
and Chiredzi districts reported that their districts were benefiting from both Results
based funding (RBF) and the Health Services Transmissions Fund (HTF).
Handling and sharing resources
The majority of the DHEs agreed that it was still difficult to pull resources together as
DHE. They indicated that it was easy when the funding comes directly to the District
through the DMO .Their concern was that the national level programme managers are
still directing funding to an individual which then makes it difficult to work a as team.
Other districts reported that they were sharing resources such as per-diems for

49
supervision .They said that in such cases they all went for supervision even when
specific officers are listed as the only people to go as a result they were able to share
resources.
The National health strategy, using health information and working with
partners
Respondents agreed that they are now planning their programmes with reference to
indicators outlined in the National Health strategy with reference to data obtained
from the health information system since they learned how to translate data into
information that is useful for planning. Knowledge of the NHS had also facilitated the
DHEs to guide partners in terms of the requirements of the MHCC policy frame work.
The DHEs indicated that they were now more confident to in interacting with other
sectors as policy makers. Introduction of new issues is always a difficult process;
however the training DHEs obtained from the LMP has helped them to introduce
change using the consensus building process as part of teamwork.
50
DHE EVALUATION QUALITATIVE
DATA
51
CHAPTER 4
4.1 Qualitative Evaluation For DHEs Qualitative information was collected through focus group discussions and in some
cases group discussions in the selected districts. The discussion focused on the
knowledge gained per module covered during training and its application thereof. A
total of four focus group discussions were conducted as part of the evaluation in four
provinces.
Developing Focus group discussion guide
A focus group discussion guide was developed (see annex) based on the custom
indicators developed for monitoring and evaluation of the LMG training. The following
indicators were addressed in the FGD guide: conducting regular DHE meetings ,
concluding disciplinary cases, Recording disciplinary cases in the misconduct
register, conducting coordination meetings with developmental partners detecting
Outbreaks on time ,reporting outbreaks on the weekly diseases surveillance system
controlling outbreaks on time , providing Clinics with supervision and support
number of Pregnant women booked for ANC for the first visit. Members of the
research team were trained on the conduct of Focus Group Discussions (FGD).
Selection of participants
Participants to the FGDs were selected into the FGD based on:
Having participated in the LMG training in the past 3 years
Being members of the DHE
4.2 Conducting FGDs
Communication was made to the Provincial Medical Director about the evaluation a
month before the evaluation. The communication outlined the date and time for the
visits so that arrangement could be done in advance and some members of the DHE
could easily be found in place on the specific dates since the DHEs are usually very
busy with programme activities. In each case the team passed through the Provincial
Medical Director`s (PMD) office to discuss the purpose of the visit and obtain an
endorsement from the PMDs office on the districts to be visited.
52
Four FGDs were conducted in four clusters between 18th and 31st March 2014. Thirty-
One DHE members participated in the FGDs. The participants were conveniently
selected to be interviewed as regions. Manicaland, Mash West, Midlands and
Matabeleland North provinces were selected.
Procedurally the purpose of the FGD was explained to the participants and the rules
for conducting the FGD were explained as outlined on the FGD guide. The discussions
started by asking a general question on how health workers are managing health care
services and the challenges they are encountering on day to day basis. This question
was then followed by specific questions related to the roles and functions of the DHEs
and how they are performing these roles after the LMG training. Focus group
discussions were conducted in the board room that was kindly provided by the DHE.
Participants were asked to describe their experiences before training and how they are
now applying the knowledge gained from the training The discussions also included
the challenges that are being faced by DHE in applying what they learned during the
training as well as possible solutions to these challenges
The FGDs were conducted by three people. The facilitator was responsible for asking
questions the second person was responsible for the recording the conversations on
tape and the third person was observing as well as recording the discussions using
pen and paper. This same procedure was used for the four FGDs. Each FGD lasted
about an hour.
Data Management
After data collection the next step was the transcription of the discussions which were
recorded in English. The completed transcriptions were compared with hand-written
notes to fill in inaudible phrases or gaps in the tapes. The two common methods in
content analysis are identification of themes, and incidence density. In theme
identification, the research looked for particular patterns, themes, concerns or
responses which were posed repeatedly by the focus-group respondents. The group
(rather than the individual) was the unit of analysis
4.3 Transcription and Analysis Phase 1: The field notes were labeled for venue, date of FGD and person who
conducted the FGD. After data collection the next step was the transcription of the
individual, pre-labeled tapes.
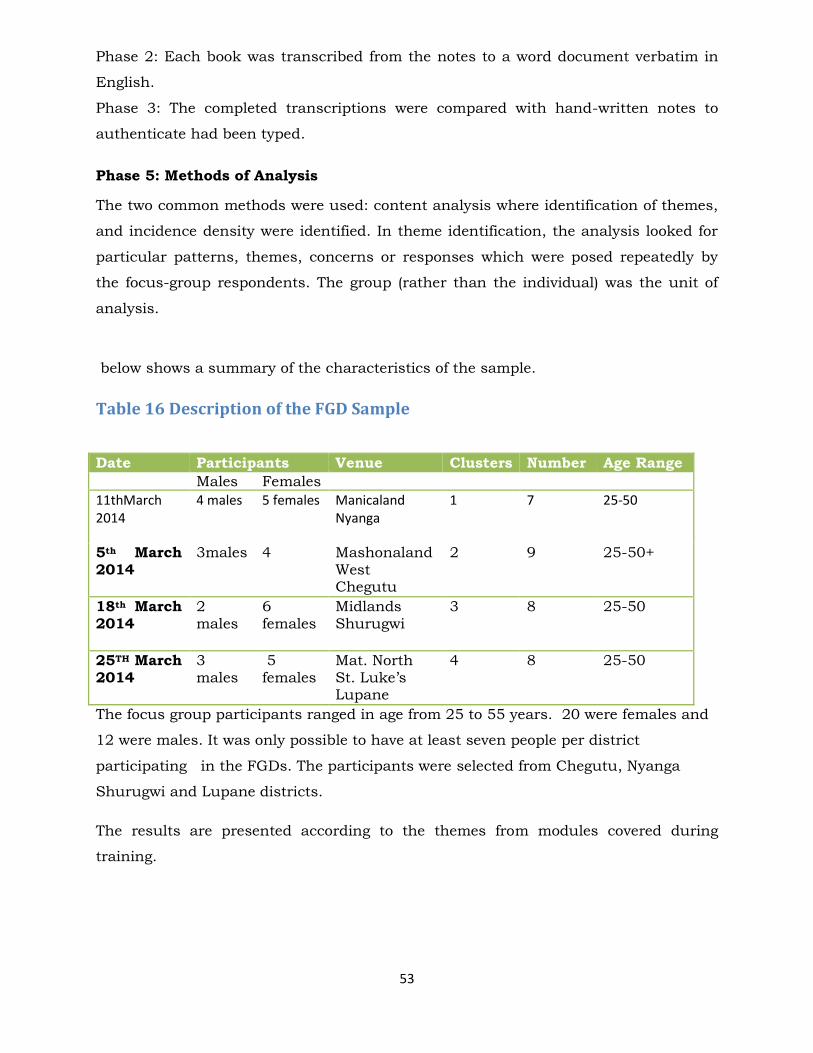
53
Phase 2: Each book was transcribed from the notes to a word document verbatim in
English.
Phase 3: The completed transcriptions were compared with hand-written notes to
authenticate had been typed.
Phase 5: Methods of Analysis
The two common methods were used: content analysis where identification of themes,
and incidence density were identified. In theme identification, the analysis looked for
particular patterns, themes, concerns or responses which were posed repeatedly by
the focus-group respondents. The group (rather than the individual) was the unit of
analysis.
below shows a summary of the characteristics of the sample.
Table 16 Description of the FGD Sample
Date Participants Venue Clusters Number Age Range
Males Females
11thMarch 2014
4 males 5 females Manicaland Nyanga
1 7 25-50
5th March 2014
3males 4 Mashonaland West Chegutu
2 9 25-50+
18th March 2014
2 males
6 females
Midlands Shurugwi
3 8 25-50
25TH March 2014
3 males
5 females
Mat. North St. Luke’s Lupane
4 8 25-50
The focus group participants ranged in age from 25 to 55 years. 20 were females and
12 were males. It was only possible to have at least seven people per district
participating in the FGDs. The participants were selected from Chegutu, Nyanga
Shurugwi and Lupane districts.
The results are presented according to the themes from modules covered during
training.
54
4.5 Results Of FGDs
Working as DHE Teams
Team work was a serious problem in most districts because of vertical funding of
programmes which resulted in each member of the DHE doing his or her own
activities. The LMG training focused on highlighting the benefits of teamwork and the
challenges that can arise in working as a team and how the team leader can resolve
some of these challenges
The discussions revealed that the HLMG training has improved communication
among team members and there is now integration of activities.All the districts
mentioned learning about teamwork as having the most singular out of the whole
training They said that the training had strengthened team work among the DHEs. All
the districts mentioned learning about team work as having the most singular benefit
of the LMG training.
Teamwork has resulted in the integration of activities through combining trips
especially on outreach program has resulted in the effective and efficient utilization of
scarce resources. The benefits of the training are also manifest in the improvement in
service delivery as there is evidence that now DHE members understood the role of
each member and their related activities.
There was also a revelation that most activities used to be departmentalized and each
person was carrying out his/her individual programme duties. The DHEs having
realized the importance of team work have revived meetings such as DHE General
meeting, Staff meeting and HOD meetings so as to work together as teams and
increase efficiency.
Eighty-five per cent of the districts visited indicated that DHE Meetings are now
running smoothly because of the renewed team spirit among the members. There was
lack of appreciation of programmes run by other members before the LMG training
which resulted in house fighting for resources. After the training they came back, sat
down as a team to chat the way forward to work together. The DHE training has
taught them to work together and share resources and this is done through
conducting DHE meetings regularly and share information pertaining to their specific
programmatic areas.
55
A member of the DHE stressed that the module on team building was of significant
importance as it fosters team spirit and DHE Cohesion. They also highlighted that as a
result of regular meetings communication has improved and decisions are wholly
owned by the DHE as indicated below:
Team spirit and cohesion is clearly described below:
“After the training we realized that there is need for consensus decision making .There
is no longer a dictator here, no matter how small the decision is we take the inclusive
approach since they are decisions for the whole district not for specific individuals’.
Before the training EPI used to be managed by the DNO. It is true that DNO is the
technical person there is need for inputs from other members. IRS program was
specifically for the DEHO, now everyone is aware of what is happening in the district.
Record keeping has improved as we learn from the training all the meetings are
recorded accurately and agreed upon by the DHE. The DHE meetings are very crucial as
they help in resource allocation especially vehicles. There are different programs and all
members will participate when they are aware of other activities
Appreciation of each other work and sharing information
All the members now appreciate the importance of other departments and the
decisions are made in the DHE meetings. It was mentioned that planning of activities
is now being done as a team as well as support and supervision to the rural health
centres. Teamwork has also created a conducive environment for sharing information
as expressed below:
`Soon after the training I shared the information with everyone during the nurse`s meetings, this has given everyone a chance to reflect on their day to day activities and incorporate Health leadership, Management and Governance principles``-DNO Lupane
The training emphasizes the importance of training as a team and this is very critical
especially during this time of scarce resources, there is need for proper coordination of
activities together to get maximum benefits. Conflict is inevitable in all organization
and one of the causes is limited
“We hope that all new members of the district will be able to undergo the same training such that in the process of decision making everyone will be at the same level”
56
LMG Training as induction on the Health Service Regulations
The majority of respondents admitted that during their long stay in the system they
did not attend any training about the health services regulations.. There was a
realization among the respondents that currently the MOHCC was not providing any
induction for newly appointed officers and the LMG training was seen as fulfilling this
important role as indicated by a newly appointed GMO in a statement below:
“This is a very important training which serves as an induction training .When I was
promoted into managerial position there was no induction and all of a sudden I was
expected to perform and lead the district. I have been in the District for many years and
have not gone for any training like this. It was really an eye opener, as I have gained
knowledge in working as teams, improve my leadership skills, communicate and plan
together such that our activities as the DHE are coordinated. GMO Chegutu.
Mashonaland West Province.
This point was further supported by the DMO Nyanga who said:
“The health Services Regulations training was very useful to us as the district as we
are now using the information to conduct training for nurses in conditions of services
and health services regulations“
“I have never attended any induction training since I joined the Public health system
and it was very challenging in interpreting the Health Services Regulations. When I
came back from the training, I gave the regulations to all the departments and conducted
an orientation exercises on the Health Service Regulations. The workshop had adequate
information and I am now confident of conducting disciplinary hearing.
Disciplinary and Grievance Procedures
DHE s indicated that many new officers had just been thrown into the deep end of
leadership and management when their pre-service training had not prepared them for
such tasks. The sentiments are expressed in the statement below:
“We were drafted into the DHE without any leadership induction and I was expected to
lead experienced and older colleagues- DMO –Mat North West
57
Another participant from Matabeleland weighed in saying...”if the training had been
done earlier we could have averted a lot of court case that we are now saddled with. We
can now manage disciplinary hearings better
There was consensus for the FGD participants that resolving of conflicts and
responding to grievances has improved as a result of LMG training .The improvement
has been attributed to the fact that DHEs are now aware of the requirements and
processes for conducting disciplinary procedures since the LMG training includes the
health service regulations in the training. Misconducts were not finalized because of
lack of proper knowledge on grievance handling and disciplinary procedures the
following statement supports the appreciation for the health service regulation training
The lack of training in discplinary procedures could be the major reason why there
were many pending disciplinary cases prior to this training. They said that hrough
applying what they had learnt from the LMG training, they had managed to resolve
all the pending disciplinary cases and employ measures that deter indiscipline
behaviours of staff members
Decision making process
The participants reported that there has been improvement in the decision making
process after the LMG training, before the training decisions were made on an
individual basis but now the DHE is taking a leading role in making important
decisions. There has been great improvement in the decision making process as
illustrated by the statement below:
‘‘During the meetings we also discuss on how best to utilize the Health Service Fund, all
the activities to be carried out are agreed upon and there is now transparency in terms
of resource allocation. After the training we came to realize that in a team there are
members with different personalities with their weaknesses and strength. It is the
responsibility of the DHE to recognize that and maximize on individual strengths and
minimize on weaknesses. DNO Mat North
58
Effect of partial support provided to DHEs by the LMGP
The DHE, s major role is to coordinate sectors that are involved in public health and
health care delivery activities. Over the past 5 years it has been difficult for DHEs to
conduct coordination meetings in form of District Health Team meetings due to lack of
resources. Some districts had not held any DHT meetings since 2010.The LMG project
has been providing partial support to districts (6000USD) to conduct such meetings.
Districts have successfully District Team Meetings with successful outcomes. The
appreciation of the support provided by the LMG project is expressed in the statement
below:
We planned for a DHT meeting with the resources from the LMG project. The meeting
was a success and we managed to host a total of 55 participants for three days. The
participants were from the MOHCC, NGO, Local government, Ministry of Agriculture,
private sector and mission hospitals. We were able to get a full picture of what is
happening in the district and develop recommendations to this effect” DHE Shurugwi
Management and Coordination of activities among DHEs
There was an appreciation among the DHEs that decision making process has greatly
improved and now decisions are made as a team and there is ownership of projects
and programs. Communication has improved after the training, both internally and
external.
Respondents expressed that as a result of the LMG training, sub committees have
been formed in order to speed up the decision making process as well as to encourage
ownership of decisions. Examples of some committees formed include TB, OI, PMTCT
and Infection Control. There was also an affirmation that the consultation in decision
making has helped in resource allocation and coordination of activities. Coordination
between departments has improved communication. The issue on coordination is
illustrated through the following statement:
“The major benefits as a result of the DHE training is the improvement in information
sharing as a result of improved communication information is now shared between
departments .This is evidenced by how projects are being managed, for example the EPI
project was predominantly for the nurses, and IRS for the DEHO now all departments
are included in planning and project management. The administration department takes
59
a leading role in logistics and the Accounts department in making payments, the HR
also involved in recruitment of the personnel who do the spraying. Shurugwi DHE
Coordination- the DHE is a multi-disciplinary set up which needs skills and
experience in coordination in order to produce desired deliverables
The participants were happy that the training emphasised the leading role of the DHE
in all health related activities in the district. This proved to be very beneficial to the
DHEs as they used to leave their partners coordinating health related activities
without informing the DHE. The training imparted a renewed sense of ownership
among the DHEs as indicated below:
… “Now we ask the partners to submit their plans which we study and approve unlike
before’’……..DMO
The DHEs reported that they are now confident of their coordinative and leading role
with regards to other sectors. They are now able to redirect efforts towards the
MOHCC priority areas as well as their district priorities. In turn partners now also
understand the DHEs role health care delivery. Before training they said that it was
common for one programme manager to conduct a meeting with the partners, now
every DHE member is now involved in these meetings with partners.
Conducting meetings
The Meetings are now productive unlike what was happening in the past where there
were a lot of conflicts and reduced output. Most districts reported that they had not
been conducting DHEs regularly since they did not see the importance of having
regular DHE meetings. After the training, the same districts are now meeting regularly
to plan and discuss pertinent issues for the district. The DHE meetings were revived
and other meetings such as the General meeting, Staff meeting and Head of
Departments meetings were now scheduled for. Eighty-five per cent of the districts
visited indicated that DHE Meetings are now running smoothly because of the
renewed team spirit among the members. Other districts reported that most activities
used to be departmentalized and each person was carrying out his/her individual
programme duties. There was lack of appreciation of some projects by other members
which resulted in disorganization and in-house fighting.
60
“The DHE training has taught me to work together and share resources and this is done
through conducting DHE meetings regularly and share information pertaining to each
other’s specific programmatic areas”-DHE Lupane.
DHEs highlighted that as a result of regular meetings communication has improved
and decisions are wholly owned by the DHE. Data quality assessments were done
through reviewing of meeting minutes. This review highlighted that there is an
improvement in the quality of the meetings being held as shown by the availability of
meeting agenda being circulated to all the members before the meetings, action points
clearly defined and members assigned the roles to do after the meeting.
Strengthening health care programme implementation
When asked. “What did you benefit from the training you received”, the participants
mentioned several areas covered by the modules
Role Clarity…The training also helped to clarify on the core DHE members as there was
confusion on who should be part of the DHE. This has caused problems in terms of
reporting and delegation of duties and responsibilities.
Teamwork- the DHEs are functioning well because of improved team work
DHE the meetings are the backbone of district health functioning. The participants
mentioned that the meetings provide a platform to discuss on how best to utilize the
Health Service Fund; all the activities to be carried out are agreed upon. As a result of
the training they indicated that there is now transparency in terms of resource
allocation.
….”After the training we came to realize that in a team there are members with different
personalities with their weaknesses and strength. It is the responsibility of the DHE to
recognize that and maximize on individual strengths and minimize on weaknesses’’-
DNO
The training has strengthened team work among the DHEs. The DHEs reported that
they had not been conducting DHE meetings regularly due to verticalization and lack
of shared values. Since the training emphasized the need for shared vision and
61
collective decision making most districts are now holding executive meetings regularly
and this has in turn greatly improved service delivery in the districts…
…. “Now the clinical members are also involving us in their programmes and we are all
contributing significantly in our districts” -….. DHSA Chegutu
Procurement
Most of the districts were under the results based financing or the targeted
approaches programme and were thus involved in a lot of procurement. However many
have not been trained in proper procurement procedures. The FGD participants
indicated that the module on Procurement opened their eyes especially to improper
activities that had been taking place before. They can now understand the
procurement procedure language as shown in the statement below:
“The PTC would tell me that we have sole bidders some of which I could understand the
procedures”… DMO-
The benefits of the training are also manifest in the improvement in service delivery as
there is evidence that participants understood the role of Central Buying Unit and
Procurement and Tender
Asset management
The DHE manages the assets of the government health centres in the districts and are
expected to keep up to date inventories and stock control documents.
The participants indicated that that asset management had been very poor due to lack
of institutional memory as well as lack of knowledge in dealing with redundant and
obsolete equipment which continued to gobble up valuable space in the institutions.
The training helped participants helped the DHEs understand the process of disposing
of such assets and maintain records of both government and donor funded equipment.
According to the participants this also helps in curbing pilferage of assets. The finding
on improved asset management is supported by the national level reports which now
shoe that districts as well as provinces have improved in asset management
62
Finances
The DHE is responsible for managing district resources. The participants indicated
that the rest of DHE members had no interest in finance matters except the
accountants and vice versa. The training helped them to appreciate the collective role
of the DHE in the mobilization of finances and accountability of whatever resources
they have. The appreciation of being involved in finances is shown by the following
statement
‘Now we don’t blame the accountant when the money falls short of our expectations, it’s
now a collective decision on where and how to deploy our financial resources”…..DEHO
HRH
The DHE manages HRH matters at their local level. Most DHE members were not
trained on handling HRH issues like recruitment, interviewing disciplinary hearings
and boards of inquiry. The result was that most of the matters were poorly done and
the ministry in turn lost several cases due to mishandling. The module on HRH was
indicated as having been very helpful and has thus served as induction for DHEs
which should have been done before assuming the management roles and this
importance is reflected in the following statement
… The module on HRH should be a must on anyone getting into the DHE to reduce
misunderstanding and appreciation of how sometimes there are limited resources
DHSA-
The Health Services Regulations training was very useful to us as the district as we are
nw using the information to conduct trainings for nurses in conditions of services and
health services regulations“
“I have never attended any induction training since I joined the Public health system
and it was very challenging in interpreting the Health Services Regulations. When I
came back from the training in Mutare, I gave the regulations to all the departments and
conduct an orientation exercises in trying to get a clear understanding of the regulations.
The workshop had adequate information and I am now confident of conducting
disciplinary hearing
63
Support and Supervision to Primary Health Centres
The DHE provides support and supervision to primary health centres within their
respective districts. This is meant to strengthen the facilities through capacity building
as well as appraising on the development of the facilities infrastructure. The
participants indicated that this activity was being done mainly along programme lines
like PMTCT, OI ART, TB or EPI. The training helped them organize this activity as DHE
while taking advantage of programmes which have resources. …
“I can now join the team going for OI ART to go and attend to the maintenance of
facilities”…. DHSA
Support for District Health Team (DHT) meetings
The LMG project has been financially supporting districts to hold DHT meetings.The DHT is a
platform for the DHE to meet with staff from the facilities and discuss operational plans as well
updating the staff on any new guidelines to be followed. It is also a forum to meet with all the
key stakeholders in the district. It should be conducted quarterly. The participants in the FGDs
indicated that they were very grateful to the Leadership project for having resuscitated the DHT
meetings which had long been forgotten.
…I have been in the district for five years and have never attended a single DHT meeting now I
have been able to due to the support provided by the LMGP…DMO
The DHT meetings have facilitated the coordination of sectors involved in health care delivery
at district level. It can be seen that the trainings has made districts appreciate the importance
of taking a leading role in all health related activities as the support has increased coordination
meetings as supported by the statement below:
“The financial support provided by the LMGP has made it possible to conduct DHE
meetings with health workers from clinics and rural hospitals. This has made our
supervision task much easier since we have also managed to disseminate the
information from the DHE training to our entire health worker at district level.”
Chegutu DHE
DHT meetings have also helped to coordinate other health related partners and this is seen as
of paramount importance as the DHE should take a leading role in supervising all health
activities regardless of the implementing partner. After the training they have managed conduct
DHT meetings with all their partners.
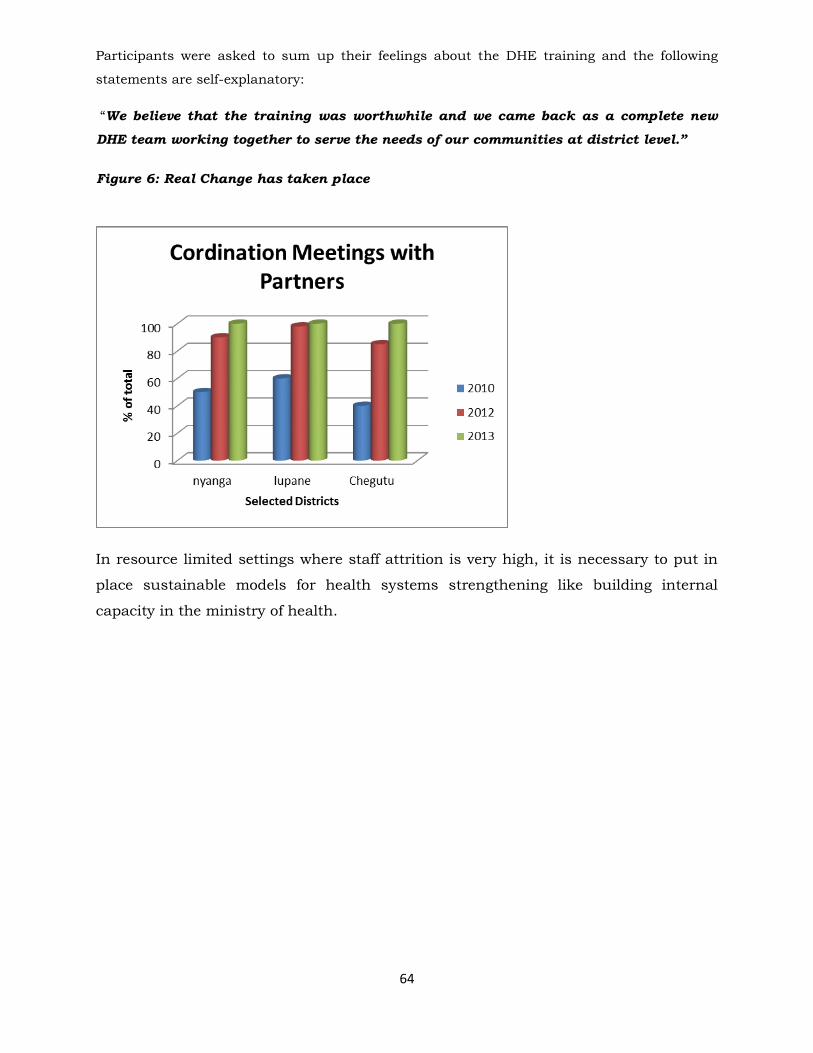
64
Participants were asked to sum up their feelings about the DHE training and the following
statements are self-explanatory:
“We believe that the training was worthwhile and we came back as a complete new
DHE team working together to serve the needs of our communities at district level.”
Figure 6: Real Change has taken place
In resource limited settings where staff attrition is very high, it is necessary to put in
place sustainable models for health systems strengthening like building internal
capacity in the ministry of health.
65
Figure 7: Disciplinary Cases
PROVINCIAL HEALTH EXECUTIVES
EVALUATION REPORT
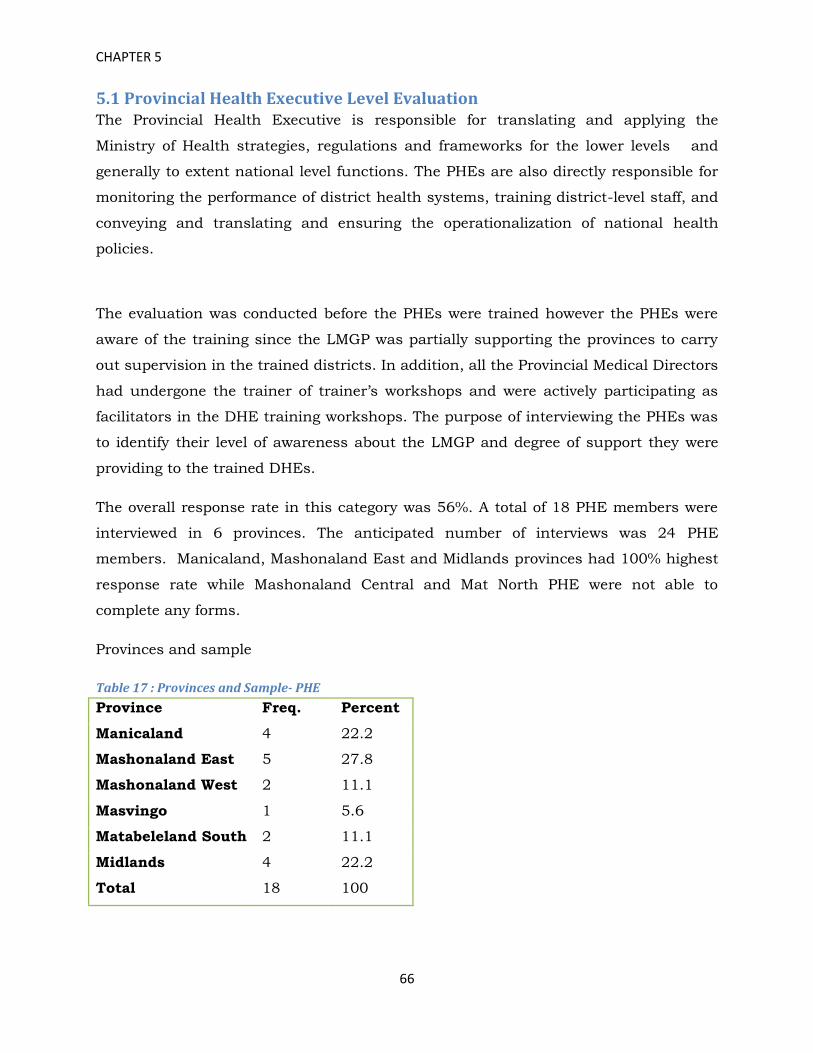
66
CHAPTER 5
5.1 Provincial Health Executive Level Evaluation The Provincial Health Executive is responsible for translating and applying the
Ministry of Health strategies, regulations and frameworks for the lower levels and
generally to extent national level functions. The PHEs are also directly responsible for
monitoring the performance of district health systems, training district-level staff, and
conveying and translating and ensuring the operationalization of national health
policies.
The evaluation was conducted before the PHEs were trained however the PHEs were
aware of the training since the LMGP was partially supporting the provinces to carry
out supervision in the trained districts. In addition, all the Provincial Medical Directors
had undergone the trainer of trainer’s workshops and were actively participating as
facilitators in the DHE training workshops. The purpose of interviewing the PHEs was
to identify their level of awareness about the LMGP and degree of support they were
providing to the trained DHEs.
The overall response rate in this category was 56%. A total of 18 PHE members were
interviewed in 6 provinces. The anticipated number of interviews was 24 PHE
members. Manicaland, Mashonaland East and Midlands provinces had 100% highest
response rate while Mashonaland Central and Mat North PHE were not able to
complete any forms.
Provinces and sample
Table 17 : Provinces and Sample- PHE
Province Freq. Percent
Manicaland 4 22.2
Mashonaland East 5 27.8
Mashonaland West 2 11.1
Masvingo 1 5.6
Matabeleland South 2 11.1
Midlands 4 22.2
Total 18 100

67
A total of 18 PHE members were interviewed in the six provinces. The highest number
being in Mashonaland East where 5 respondents were interviewed
Regarding gender, males constituted the larger percentage of respondents with 62.5%
whilst 37.5% were females.
Age distribution
Table 18: Age Distribution- PHE
Age group in
years
Frequency Percent Designation Freq. Percent
26-35 5 27.8 ACCOUNTANT 5 29.4
36-45 6 33.3 PHSA 3 17.7
46+ 7 38.9 PMD 3 17.7
Total 18 100 A/PNO 1 5.9
MOH-MCH 1 5.9
PEHO 1 5.9
PNO 1 5.9
Provincial
Nutritionist
1 5.9
Prov.
Pharmacist
1 5.9
Total 17 100
Table 18 shows the age distribution of the sample. The highest number of the
respondents was in younger age groups combined as the age group (26-45) age group
totaling 61.1% of the sample. Younger people tend to move around looking for
greener pastors. This finding confirms the initial concern of the MOHCC that health
mangers in place were too young and in most cases inexperienced.
PHE members who were found at the PMD offices and responded to the
questionnaires given to them The Provincial Health Executive is chaired by the PMD
and comprises of the other key members such as the, PNO, PEHO, PHSA, PEDCO,
PMCHO, Provincial Pharmacist and Provincial Accountant. Officers such the PHPO
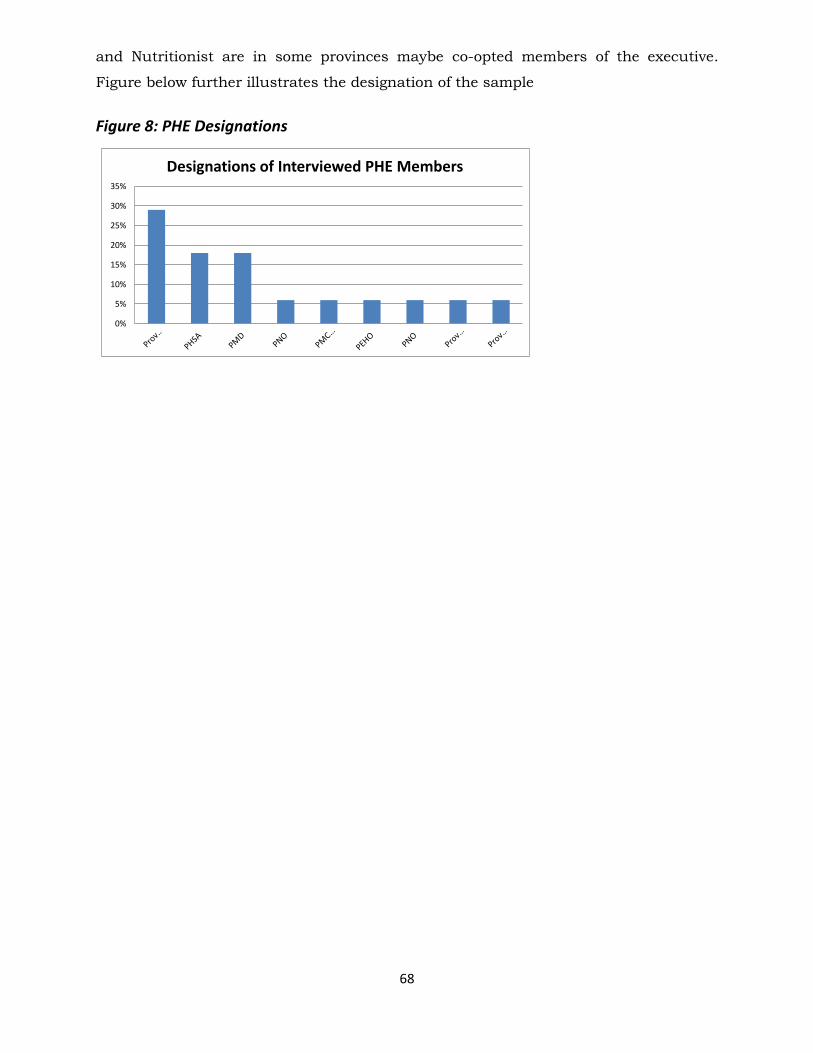
68
and Nutritionist are in some provinces maybe co-opted members of the executive.
Figure below further illustrates the designation of the sample
Figure 8: PHE Designations
0%
5%
10%
15%
20%
25%
30%
35%
Designations of Interviewed PHE Members
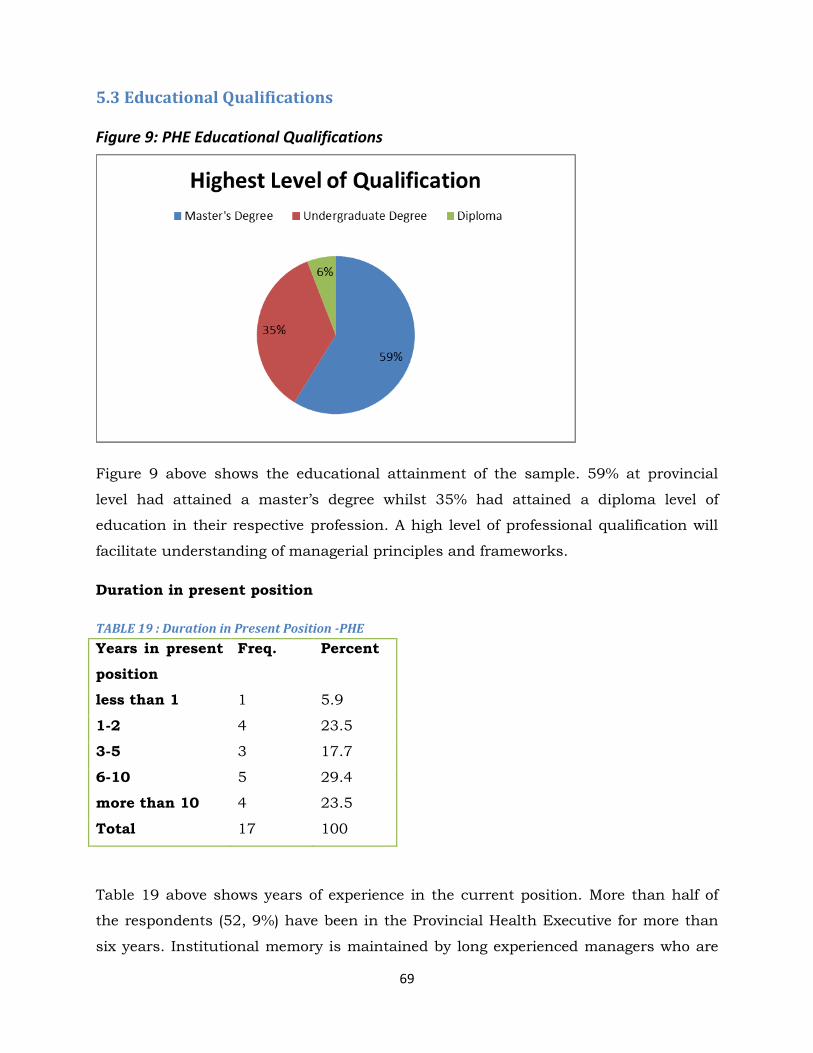
69
5.3 Educational Qualifications
Figure 9: PHE Educational Qualifications
Figure 9 above shows the educational attainment of the sample. 59% at provincial
level had attained a master’s degree whilst 35% had attained a diploma level of
education in their respective profession. A high level of professional qualification will
facilitate understanding of managerial principles and frameworks.
Duration in present position
TABLE 19 : Duration in Present Position -PHE
Years in present
position
Freq. Percent
less than 1 1 5.9
1-2 4 23.5
3-5 3 17.7
6-10 5 29.4
more than 10 4 23.5
Total 17 100
Table 19 above shows years of experience in the current position. More than half of
the respondents (52, 9%) have been in the Provincial Health Executive for more than
six years. Institutional memory is maintained by long experienced managers who are
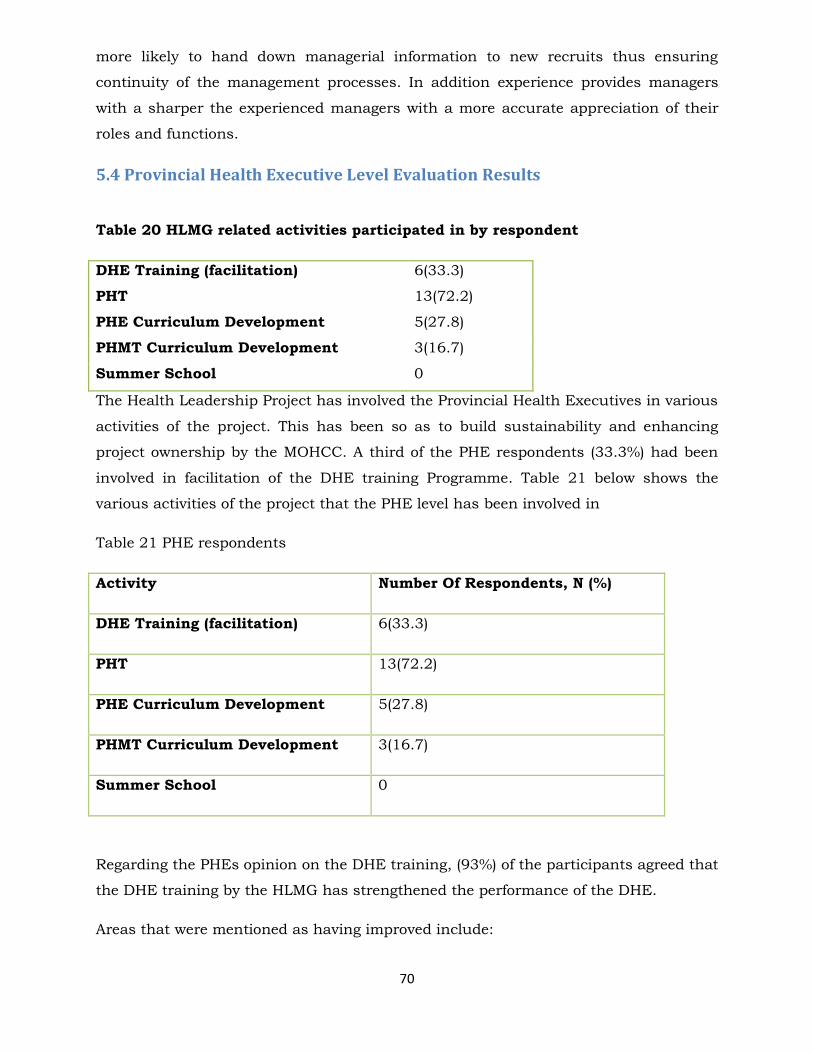
70
more likely to hand down managerial information to new recruits thus ensuring
continuity of the management processes. In addition experience provides managers
with a sharper the experienced managers with a more accurate appreciation of their
roles and functions.
5.4 Provincial Health Executive Level Evaluation Results
Table 20 HLMG related activities participated in by respondent
DHE Training (facilitation) 6(33.3)
PHT 13(72.2)
PHE Curriculum Development 5(27.8)
PHMT Curriculum Development 3(16.7)
Summer School 0
The Health Leadership Project has involved the Provincial Health Executives in various
activities of the project. This has been so as to build sustainability and enhancing
project ownership by the MOHCC. A third of the PHE respondents (33.3%) had been
involved in facilitation of the DHE training Programme. Table 21 below shows the
various activities of the project that the PHE level has been involved in
Table 21 PHE respondents
Activity Number Of Respondents, N (%)
DHE Training (facilitation) 6(33.3)
PHT 13(72.2)
PHE Curriculum Development 5(27.8)
PHMT Curriculum Development 3(16.7)
Summer School 0
Regarding the PHEs opinion on the DHE training, (93%) of the participants agreed that
the DHE training by the HLMG has strengthened the performance of the DHE.
Areas that were mentioned as having improved include:
71
Team work
Coordination of activities
Submission of programme acquittals
Supervisory skills
Consistence in DHE meetings
The majority of the respondents (81%) were aware that the HLMG project has been
providing partial support for District Support and Supervision.
All the respondents have been involved in support and supervision of the districts
supported by HLMG.
The frequency of support and supervision has been mostly quarterly.
Support and supervision is conducted by using a checklist and follow-up on the
projects which the DHE came up with during training.
About 94% of the participants reported that all programme managers participate in
district supervision.
Leadership Project Support
The majority of respondents (81%) were aware that the HLMG project has been
providing partial support for District support and supervision. They also confirmed
that they had participated in the supervision of the trained districts as part of their
duties. And this has increased the collection of information to assess performance
The PHEs were asked to rate the performance of DHEs in relationship to the
before and after LMG training
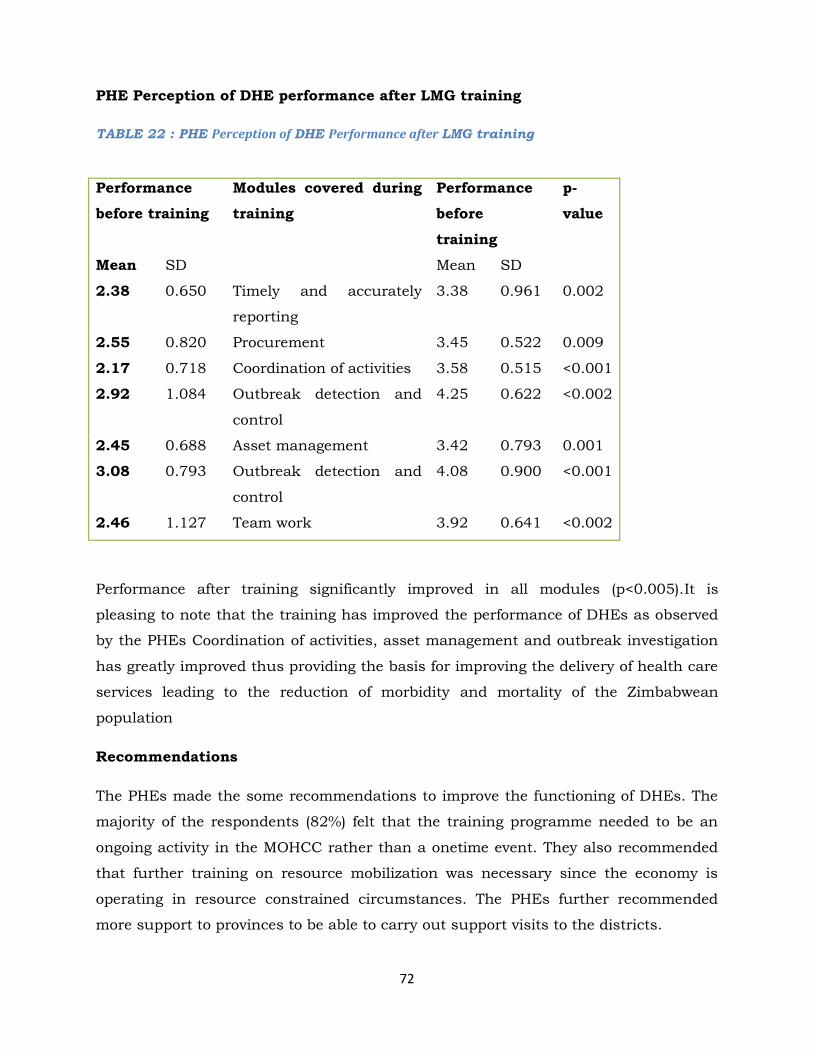
72
PHE Perception of DHE performance after LMG training
TABLE 22 : PHE Perception of DHE Performance after LMG training
Performance
before training
Modules covered during
training
Performance
before
training
p-
value
Mean SD Mean SD
2.38 0.650 Timely and accurately
reporting
3.38 0.961 0.002
2.55 0.820 Procurement 3.45 0.522 0.009
2.17 0.718 Coordination of activities 3.58 0.515 <0.001
2.92 1.084 Outbreak detection and
control
4.25 0.622 <0.002
2.45 0.688 Asset management 3.42 0.793 0.001
3.08 0.793 Outbreak detection and
control
4.08 0.900 <0.001
2.46 1.127 Team work 3.92 0.641 <0.002
Performance after training significantly improved in all modules (p<0.005).It is
pleasing to note that the training has improved the performance of DHEs as observed
by the PHEs Coordination of activities, asset management and outbreak investigation
has greatly improved thus providing the basis for improving the delivery of health care
services leading to the reduction of morbidity and mortality of the Zimbabwean
population
Recommendations
The PHEs made the some recommendations to improve the functioning of DHEs. The
majority of the respondents (82%) felt that the training programme needed to be an
ongoing activity in the MOHCC rather than a onetime event. They also recommended
that further training on resource mobilization was necessary since the economy is
operating in resource constrained circumstances. The PHEs further recommended
more support to provinces to be able to carry out support visits to the districts.

73
74
PROVINCIAL HOSPITAL RESULTS
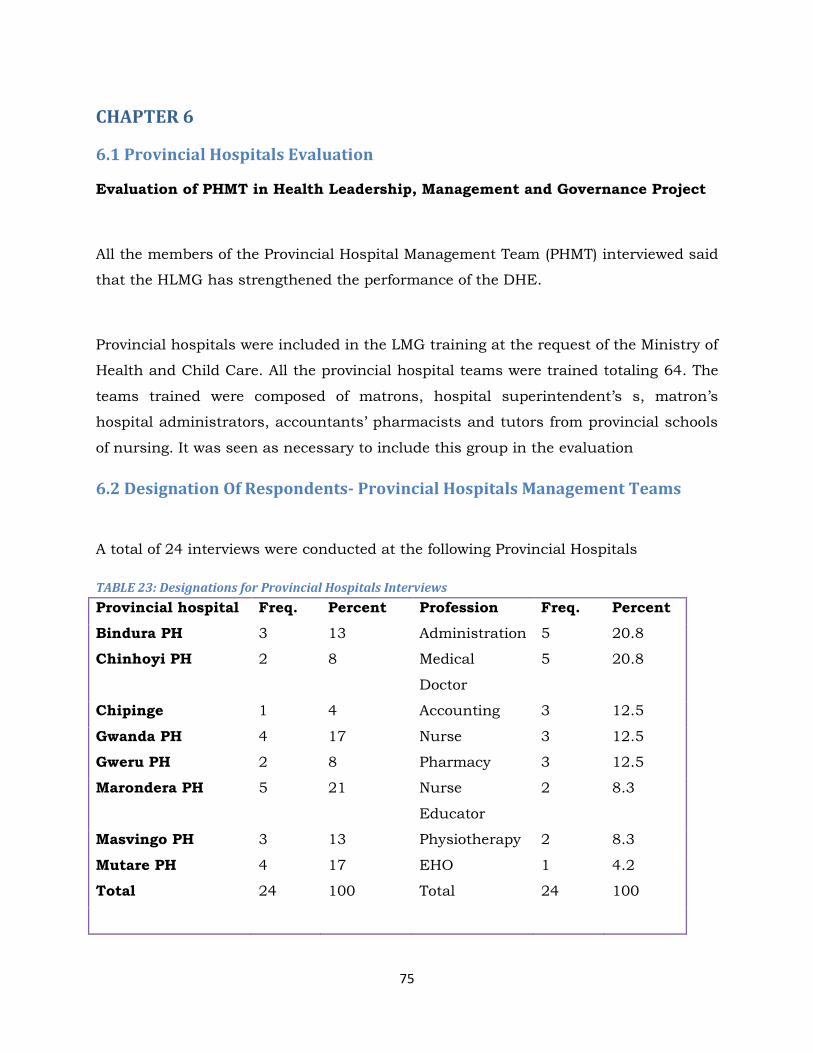
75
CHAPTER 6
6.1 Provincial Hospitals Evaluation
Evaluation of PHMT in Health Leadership, Management and Governance Project
All the members of the Provincial Hospital Management Team (PHMT) interviewed said
that the HLMG has strengthened the performance of the DHE.
Provincial hospitals were included in the LMG training at the request of the Ministry of
Health and Child Care. All the provincial hospital teams were trained totaling 64. The
teams trained were composed of matrons, hospital superintendent’s s, matron’s
hospital administrators, accountants’ pharmacists and tutors from provincial schools
of nursing. It was seen as necessary to include this group in the evaluation
6.2 Designation Of Respondents- Provincial Hospitals Management Teams
A total of 24 interviews were conducted at the following Provincial Hospitals
TABLE 23: Designations for Provincial Hospitals Interviews
Provincial hospital Freq. Percent Profession Freq. Percent
Bindura PH 3 13 Administration 5 20.8
Chinhoyi PH 2 8 Medical
Doctor
5 20.8
Chipinge 1 4 Accounting 3 12.5
Gwanda PH 4 17 Nurse 3 12.5
Gweru PH 2 8 Pharmacy 3 12.5
Marondera PH 5 21 Nurse
Educator
2 8.3
Masvingo PH 3 13 Physiotherapy 2 8.3
Mutare PH 4 17 EHO 1 4.2
Total 24 100 Total 24 100
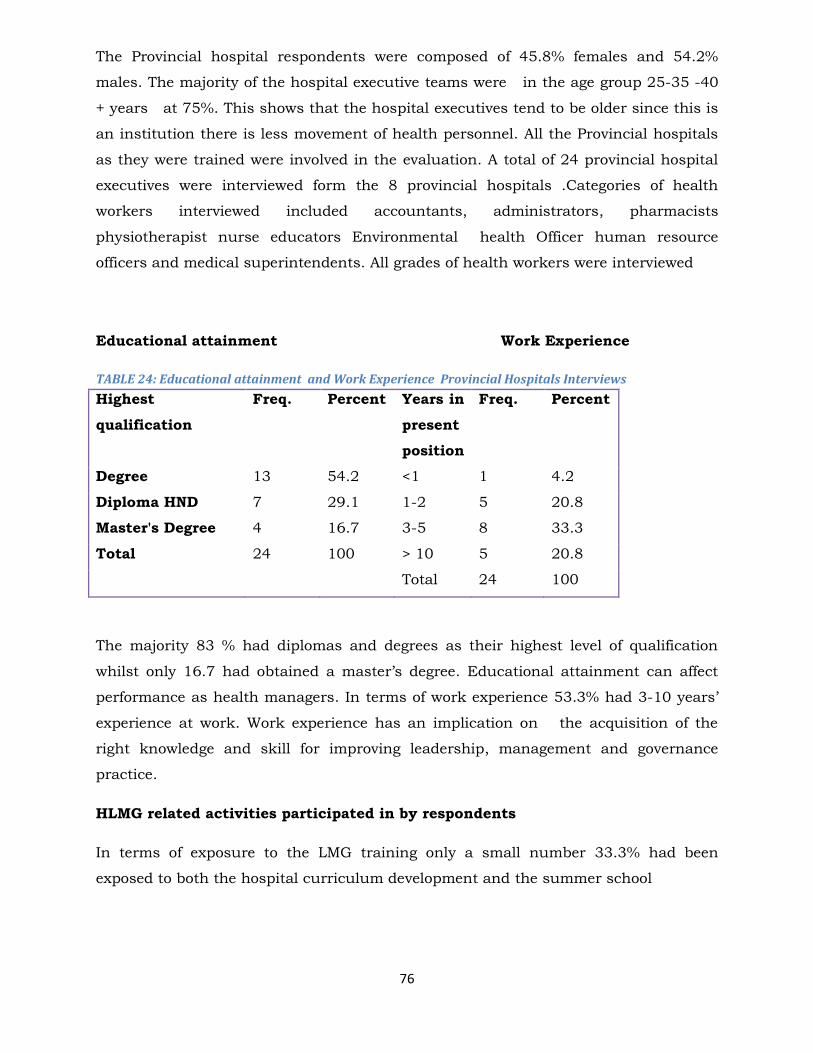
76
The Provincial hospital respondents were composed of 45.8% females and 54.2%
males. The majority of the hospital executive teams were in the age group 25-35 -40
+ years at 75%. This shows that the hospital executives tend to be older since this is
an institution there is less movement of health personnel. All the Provincial hospitals
as they were trained were involved in the evaluation. A total of 24 provincial hospital
executives were interviewed form the 8 provincial hospitals .Categories of health
workers interviewed included accountants, administrators, pharmacists
physiotherapist nurse educators Environmental health Officer human resource
officers and medical superintendents. All grades of health workers were interviewed
Educational attainment Work Experience
TABLE 24: Educational attainment and Work Experience Provincial Hospitals Interviews
Highest
qualification
Freq. Percent Years in
present
position
Freq. Percent
Degree 13 54.2 <1 1 4.2
Diploma HND 7 29.1 1-2 5 20.8
Master's Degree 4 16.7 3-5 8 33.3
Total 24 100 > 10 5 20.8
Total 24 100
The majority 83 % had diplomas and degrees as their highest level of qualification
whilst only 16.7 had obtained a master’s degree. Educational attainment can affect
performance as health managers. In terms of work experience 53.3% had 3-10 years’
experience at work. Work experience has an implication on the acquisition of the
right knowledge and skill for improving leadership, management and governance
practice.
HLMG related activities participated in by respondents
In terms of exposure to the LMG training only a small number 33.3% had been
exposed to both the hospital curriculum development and the summer school
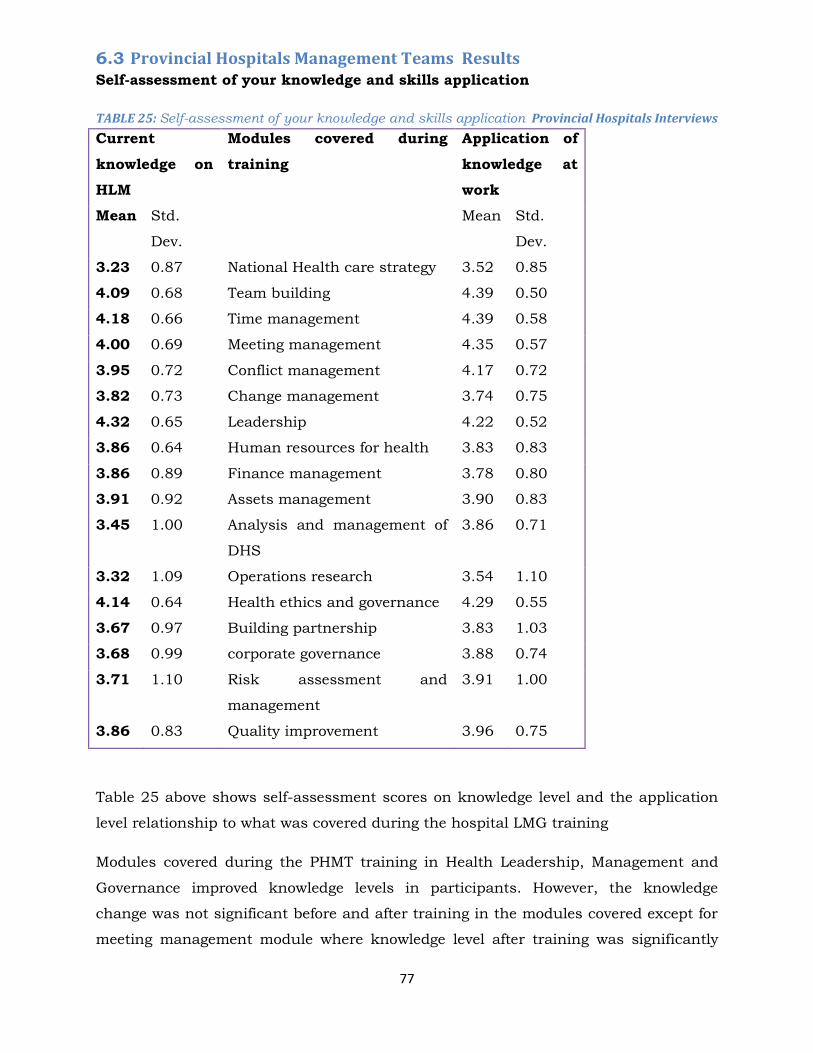
77
6.3 Provincial Hospitals Management Teams Results Self-assessment of your knowledge and skills application
TABLE 25: Self-assessment of your knowledge and skills application Provincial Hospitals Interviews
Current
knowledge on
HLM
Modules covered during
training
Application of
knowledge at
work
Mean Std.
Dev.
Mean Std.
Dev.
3.23 0.87 National Health care strategy 3.52 0.85
4.09 0.68 Team building 4.39 0.50
4.18 0.66 Time management 4.39 0.58
4.00 0.69 Meeting management 4.35 0.57
3.95 0.72 Conflict management 4.17 0.72
3.82 0.73 Change management 3.74 0.75
4.32 0.65 Leadership 4.22 0.52
3.86 0.64 Human resources for health 3.83 0.83
3.86 0.89 Finance management 3.78 0.80
3.91 0.92 Assets management 3.90 0.83
3.45 1.00 Analysis and management of
DHS
3.86 0.71
3.32 1.09 Operations research 3.54 1.10
4.14 0.64 Health ethics and governance 4.29 0.55
3.67 0.97 Building partnership 3.83 1.03
3.68 0.99 corporate governance 3.88 0.74
3.71 1.10 Risk assessment and
management
3.91 1.00
3.86 0.83 Quality improvement 3.96 0.75
Table 25 above shows self-assessment scores on knowledge level and the application
level relationship to what was covered during the hospital LMG training
Modules covered during the PHMT training in Health Leadership, Management and
Governance improved knowledge levels in participants. However, the knowledge
change was not significant before and after training in the modules covered except for
meeting management module where knowledge level after training was significantly
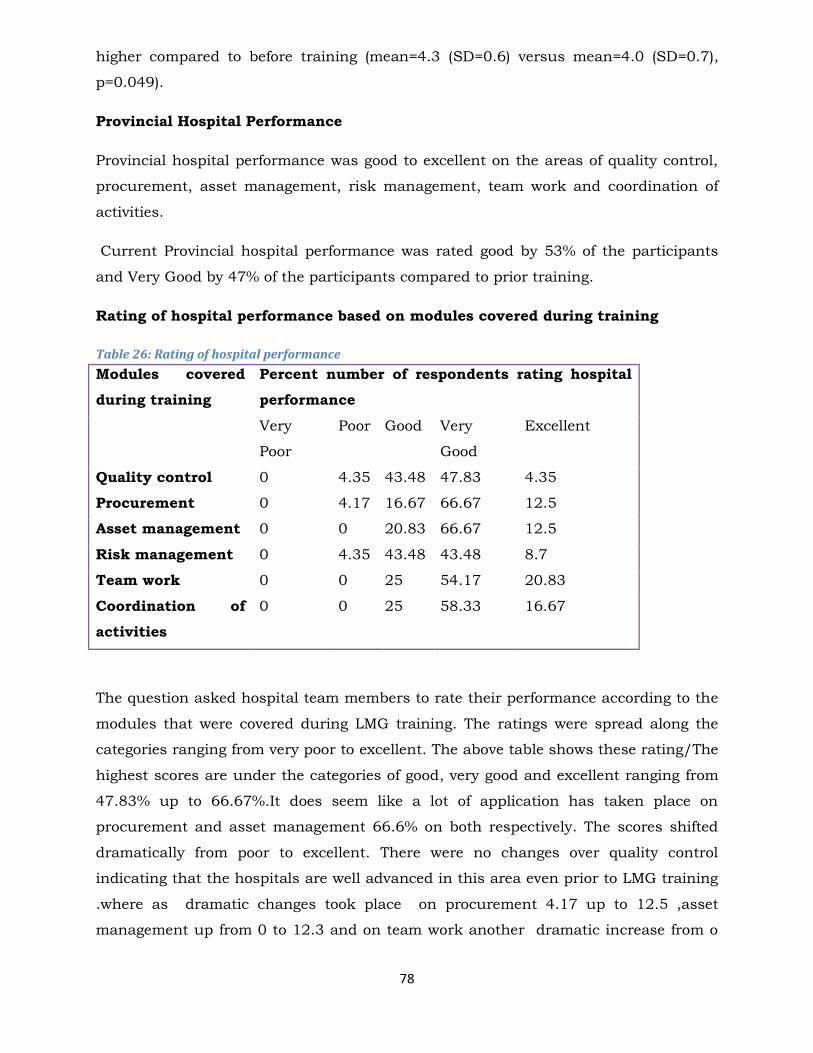
78
higher compared to before training (mean=4.3 (SD=0.6) versus mean=4.0 (SD=0.7),
p=0.049).
Provincial Hospital Performance
Provincial hospital performance was good to excellent on the areas of quality control,
procurement, asset management, risk management, team work and coordination of
activities.
Current Provincial hospital performance was rated good by 53% of the participants
and Very Good by 47% of the participants compared to prior training.
Rating of hospital performance based on modules covered during training
Table 26: Rating of hospital performance
Modules covered
during training
Percent number of respondents rating hospital
performance
Very
Poor
Poor Good Very
Good
Excellent
Quality control 0 4.35 43.48 47.83 4.35
Procurement 0 4.17 16.67 66.67 12.5
Asset management 0 0 20.83 66.67 12.5
Risk management 0 4.35 43.48 43.48 8.7
Team work 0 0 25 54.17 20.83
Coordination of
activities
0 0 25 58.33 16.67
The question asked hospital team members to rate their performance according to the
modules that were covered during LMG training. The ratings were spread along the
categories ranging from very poor to excellent. The above table shows these rating/The
highest scores are under the categories of good, very good and excellent ranging from
47.83% up to 66.67%.It does seem like a lot of application has taken place on
procurement and asset management 66.6% on both respectively. The scores shifted
dramatically from poor to excellent. There were no changes over quality control
indicating that the hospitals are well advanced in this area even prior to LMG training
.where as dramatic changes took place on procurement 4.17 up to 12.5 ,asset
management up from 0 to 12.3 and on team work another dramatic increase from o
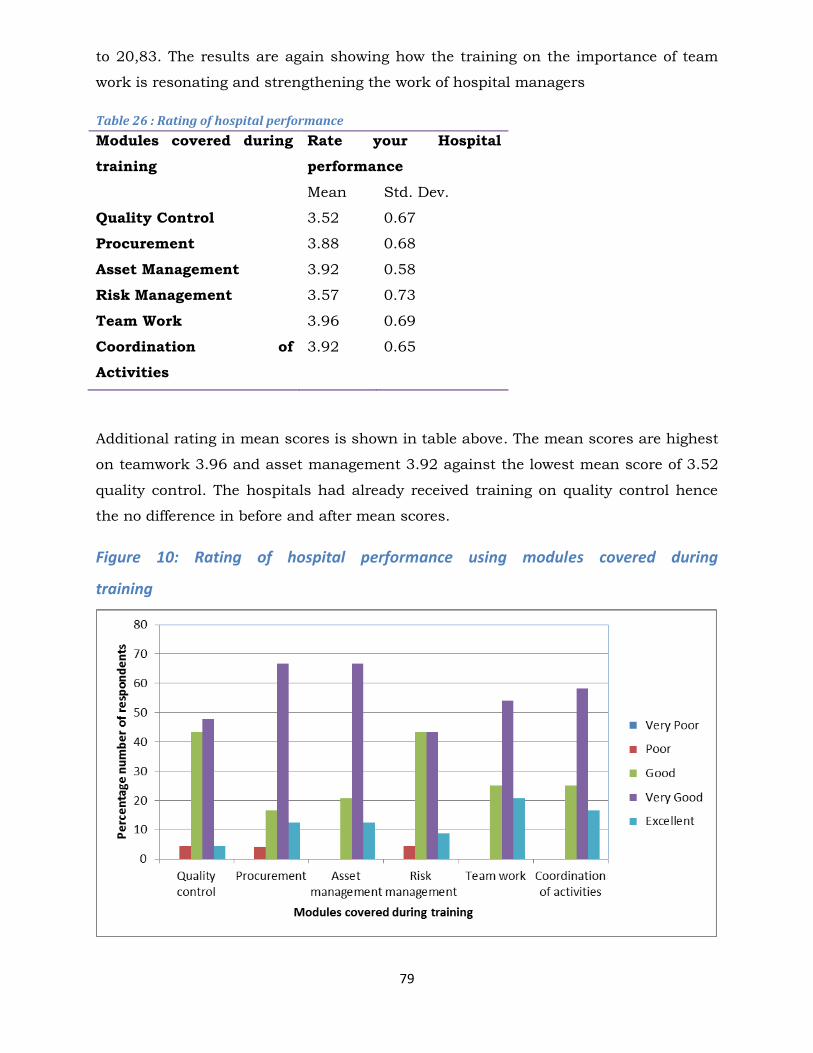
79
to 20,83. The results are again showing how the training on the importance of team
work is resonating and strengthening the work of hospital managers
Table 26 : Rating of hospital performance
Modules covered during
training
Rate your Hospital
performance
Mean Std. Dev.
Quality Control 3.52 0.67
Procurement 3.88 0.68
Asset Management 3.92 0.58
Risk Management 3.57 0.73
Team Work 3.96 0.69
Coordination of
Activities
3.92 0.65
Additional rating in mean scores is shown in table above. The mean scores are highest
on teamwork 3.96 and asset management 3.92 against the lowest mean score of 3.52
quality control. The hospitals had already received training on quality control hence
the no difference in before and after mean scores.
Figure 10: Rating of hospital performance using modules covered during
training
80
Figure 4 above shows a graphic presentation on the rating on performance against the
modules covered. There is an obvious bias over the increase of positive rating in all the
modules indicating an obvious increase on knowledge gain and performance of their
roles and functions as PHT the positive rating is however the ratings are more
pronounced and positive on coordination of activities procurement and asset
management. Risk management and quality improvement are aspects that hospitals
are already focusing on hence the low rating
81
CHAPTER 7
7.1 Stakeholder Perspectives
The main stakeholders in this project are the Ministry of Health and Child Care Health
Provincial Medical Directors, District Medical Officers Services Board, Management
Sciences for Health, Centers of Disease Contorl as the funding partner and the
University of Zimbabwe Department of Community Medicine. The stakeholder
perspectives are derived from this range of partners Harare, Bulawayo City Health
Directorates
82
7.2 Dr L Mbengeranwa- Executive Chairman- Health Service Board The HSB appreciates great work from CDC, MOHCC and UZDCM. HE said the
constitution of Zimbabwe has provided for every citizen a right to access to basic
health services and the HSB and MOHCC are in the process of realigning their
respective statutes to comply with the constitution as well as the ZIMASSET blueprint
which seeks to achievable sustainable development and social and equity. It is
imperative for PMDs keep copies of ZIMASSET and the country’s constitution which
highlight the importance of responsive governance systems. It is in this regard that the
HSB through HMGP in collaboration with UZDCM, MOHCC and CDC is already
implementing ZIMASSET in health worker capacity building. The project is already
bearing fruits and the boards is very pleased with the topics covered as it forms a
critical executive knowledge so required of our public health managers. He appealed
for continuous support for capacity building and pleaded with funding agencies to
continue strengthening the health delivery system in Zimbabwe
7.3 Brigadier-General Dr G. Gwinji: Permanent Secretary MOHCC The PS explained that the health sector has faced challenges in recent times which
have made it difficult for young doctors and other health professionals to acquire and
maintain the management skills necessary to function effectively at lower levels of the
health system especially at district level. He said that it was important for the District
Health Executive to acquire basic knowledge and skills of management if service
delivery is to be fully restored and sustained over time.
We are happy that the Department of Community Medicine (DCM) of the University of
Zimbabwe’s (UZ) College of Health Sciences (CHS) in partnership with, the MOHCC,
Health Services Board and the Management Sciences for Health (MSH), responded to
an RFA from CDC Atlanta for a proposal to support effective leadership in health
planning, program implementation and patient care in the public sector in Zimbabwe
in response to the training needs of the MOHCC
The LMG project will address
The PS indicated that in order to achieve the health Millennium Development Goals
(MDGs) and its stated desire to have the highest possible level of health and quality of
life for all its citizens, the Republic of Zimbabwe needs to have a health workforce that
83
is well trained in technical areas as well as in leadership and management at all levels
of the health delivery system this project will go a long way in strengthening health
manpower skills for achieving positive health outcomes.
The PS indicated that the current health professionals work very hard and they
remain dedicated to better health outcomes Despite their commendable efforts and
dedication, the majority of health professionals now in leadership and managerial
positions are young and lack the knowledge, skills and experience needed to play their
role effectively because they have not benefited from mentorship of more experienced
staff. The LMG project has come at the right time to address such shortcomings.
The PS also referred to previous manpower development an effort which was a
contribution of various organizations. We see the LMG project as another effort to offer
the necessary leadership and management training for health workers that take up
positions of leadership at all levels of the health delivery system and will also enable
senior managers to have opportunities for planning, reviewing service provision and
supporting supervision. The PS ended up by appreciating CDC for funding the HLMG
training
7.4 CDC Perspective- Dr P Kilmarx The US: Centers for Disease Control and Prevention in Zimbabwe is very pleased
working with MoHCC, and the HSB to support the UZDCM in training Zimbabwe’s
Public health manpower in leadership management and governance. This will ensure
strong and effective leadership that is key to successful program implementation. If a
country has strong governance and human resources management it will be possible
to implement large scale programs like Art. The US: Centers for Disease Control and
Prevention in Zimbabwe is happy with the collaborative efforts it has entered into with
government of Zimbabwe to strengthen and sustain good leadership, management and
governance in Zimbabwe’s health care system.
7.5 Director Human Resources- Ms J Mudyara The DHR stressed that people in leadership positions come from different
backgrounds such as private and public. In some cases people are promoted to senior
positions without requisite managerial and leadership skills. Managers at National
Level are expected to run divisions in central hospitals/institutions and provinces
effectively and efficiently, Induct, supervise, motivate and appraise team members.
They are also expected to represent the Accounting Officers, handle grievances and
84
resolve conflicts and chair or be a member of an interviewing panel or disciplinary
committee.
The Ministry has responded to the challenges faced through filling of vacant posts,
conducting workshops and meetings in area of expertise and piecemeal training of
members in various areas. However the challenge of inadequate resources is stifling
progress. The presenter also highlighted areas which need training and they include
inter alia team building, report writing and presentation skills, stress management,
procurement/tender procedures and induction procedures. She suggested that as a
way forward there is need for mandatory training for all health personnel in Health
Service Regulations, Government protocol, Results Based Management including
Performance management, chairing of meetings, committees, computer appreciation,
finance for non-finance managers and time management. The director also indicated
that training was required in department and professionalism in order to further
strengthen the leadership skills of health managers. She indicated that the LMG
project has come at an opportune time to support the MOHCC in its effort to rebuild
the health care system
7.6 The Executive Director Health Services Board – Ms. R.R. Kaseke The HSB places special emphasis on training of managers in leadership and
management on a continuous basis. Succession planning to strengthen institutional
memory and build leadership and management capacity amongst successors is also
critical for continuity and preservation of institutional memory.
Efforts are being made to equip the health professionals with leadership and
management skills and this entails the provision of the induction and the in service
training for all health workers as well as the establishment of Manpower Planning and
Development Department. The executive director end up appreciating the role the
LMG project in addressing leadership management and governance knowledge and
skills for health managers at all level. The appreciation is demonstrated by the
statement below:
“The Board is cognisant that the health sector is labour intensive and that
there is need to have the right number of workers possessing the right skills,
knowledge and capacities”

85
7.7 Dr G. Sikipa, Technical Advisor from MSH Dr. Sikipa explained that MSH has played a significant role at an international level in
addressing the deficiencies and gaps in health leadership and management and it was
happy to be associated with the current Leadership management and governance
project It was noted that there are good doctors yet they are poor managers as
evidenced by a weak health delivery system in terms of planning, budgeting and
management. Inadequate capacity in human resources development, including
training and personnel management has also worsened the plight. MSH therefore
strives to strengthen administration, leadership and governance at all levels of the
health sector and has leadership training programmes in various African countries.
MSH has experience in leadership training as evidenced by its support for the current
LMG project. MSH will thus continue to provide technical support during the project
lifeline so as to improve the leadership management and government skills of health
managers at all levels in Zimbabwe. He ended up by indicating that:
“Lack of leadership and managerial skills is prevalent in the newly promoted
cadres who are in leadership positions”
7.8 National Level Perspectives/ Administration Asset returns are designed to depict a summary of the state of assets at any given
time. The summary indicates categories of items and their quantities and is born out
of an inventory – register system. All provincial centres are expected to submit asset
returns bi-annually, the first being at the end of June whilst the second would be
submitted at the end of December of each year. The move would make it easy for the
system to quickly reveal any deficiencies in terms of losses or damages. It was
highlighted that in 2010 the Ministry of Health Head Office was not receiving not
receiving 100% of returns. Below is a table illustrating those who have managed to
submit their asset returns in 2010 and those who failed.
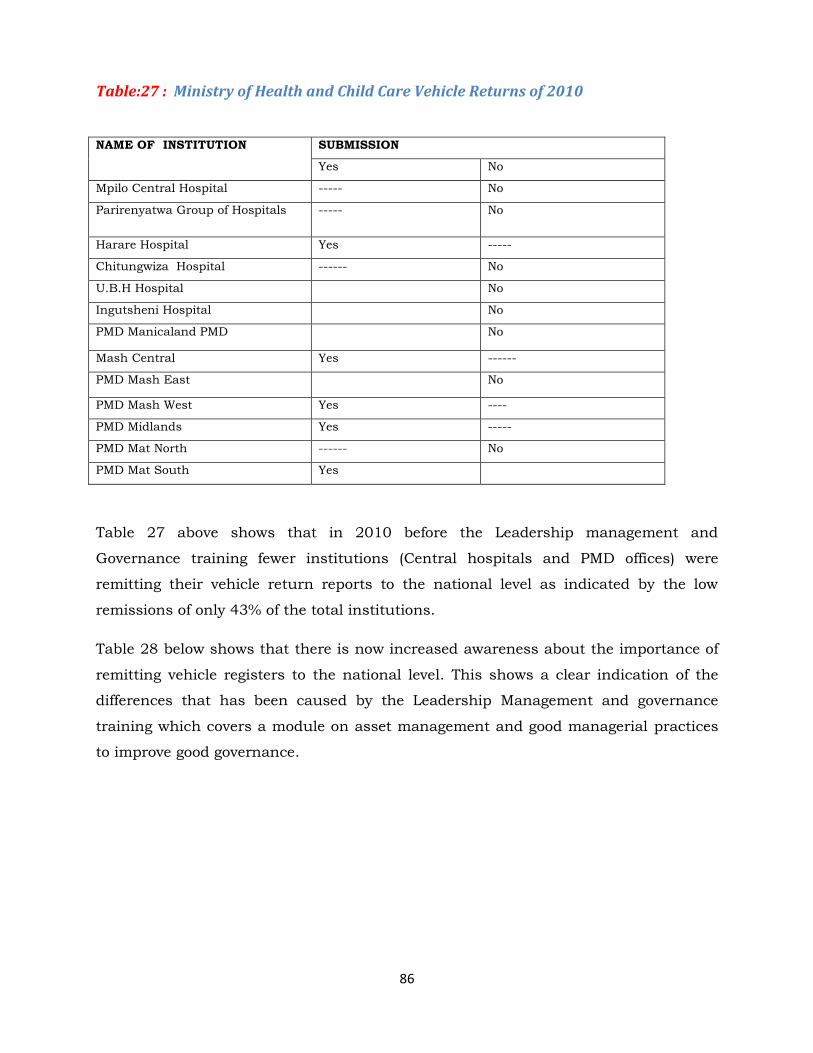
86
Table:27 : Ministry of Health and Child Care Vehicle Returns of 2010
NAME OF INSTITUTION SUBMISSION
Yes No
Mpilo Central Hospital ----- No
Parirenyatwa Group of Hospitals ----- No
Harare Hospital Yes -----
Chitungwiza Hospital ------ No
U.B.H Hospital No
Ingutsheni Hospital No
PMD Manicaland PMD No
Mash Central Yes ------
PMD Mash East No
PMD Mash West Yes ----
PMD Midlands Yes -----
PMD Mat North ------ No
PMD Mat South Yes
Table 27 above shows that in 2010 before the Leadership management and
Governance training fewer institutions (Central hospitals and PMD offices) were
remitting their vehicle return reports to the national level as indicated by the low
remissions of only 43% of the total institutions.
Table 28 below shows that there is now increased awareness about the importance of
remitting vehicle registers to the national level. This shows a clear indication of the
differences that has been caused by the Leadership Management and governance
training which covers a module on asset management and good managerial practices
to improve good governance.
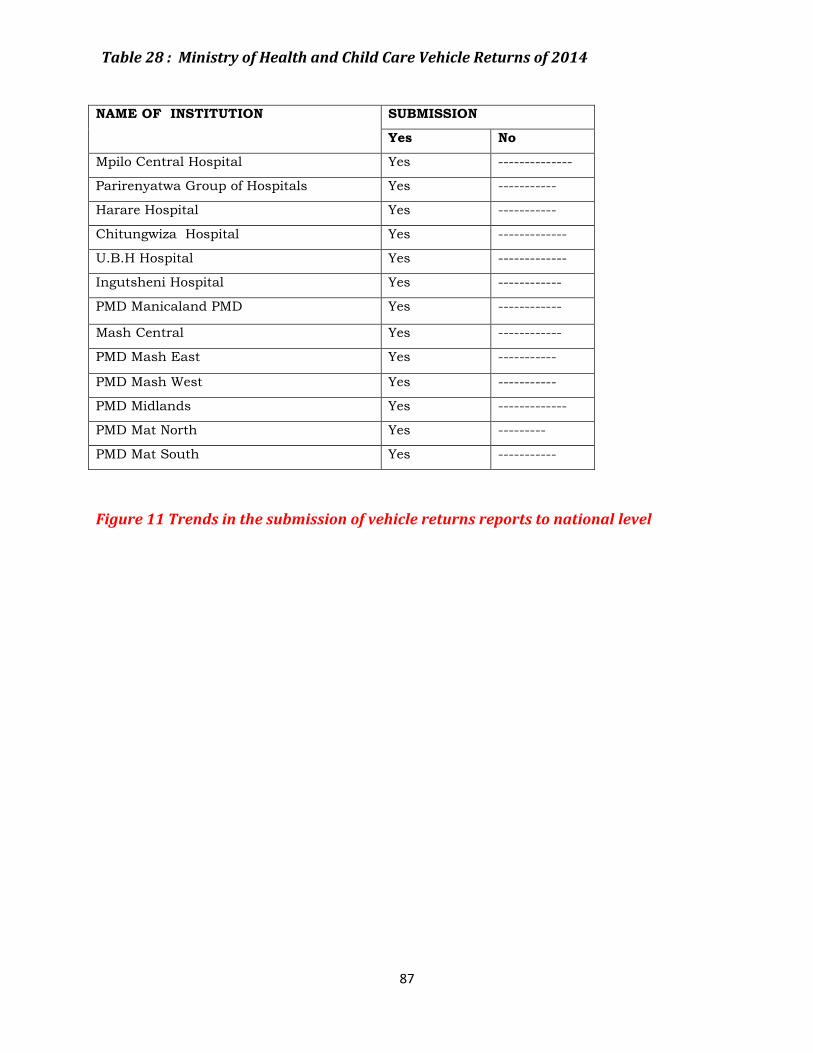
87
Table 28 : Ministry of Health and Child Care Vehicle Returns of 2014
NAME OF INSTITUTION SUBMISSION
Yes No
Mpilo Central Hospital Yes --------------
Parirenyatwa Group of Hospitals Yes -----------
Harare Hospital Yes -----------
Chitungwiza Hospital Yes -------------
U.B.H Hospital Yes -------------
Ingutsheni Hospital Yes ------------
PMD Manicaland PMD Yes ------------
Mash Central Yes ------------
PMD Mash East Yes -----------
PMD Mash West Yes -----------
PMD Midlands Yes -------------
PMD Mat North Yes ---------
PMD Mat South Yes -----------
Figure 11 Trends in the submission of vehicle returns reports to national level
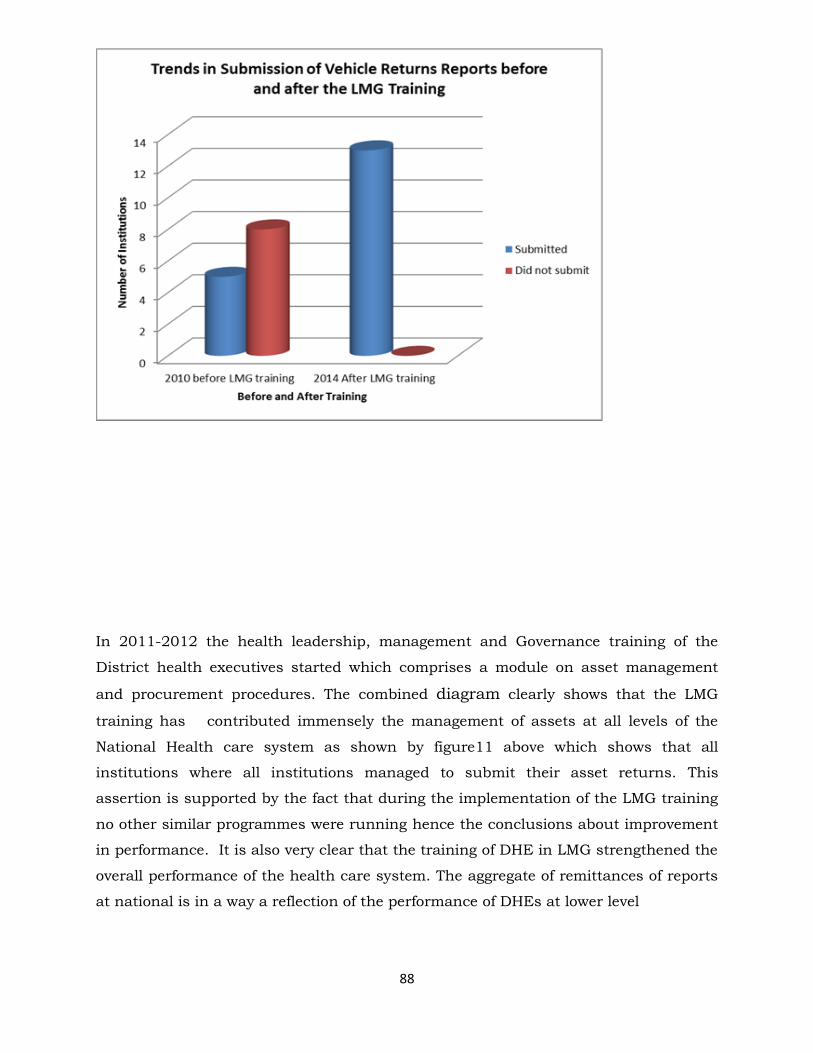
88
In 2011-2012 the health leadership, management and Governance training of the
District health executives started which comprises a module on asset management
and procurement procedures. The combined diagram clearly shows that the LMG
training has contributed immensely the management of assets at all levels of the
National Health care system as shown by figure11 above which shows that all
institutions where all institutions managed to submit their asset returns. This
assertion is supported by the fact that during the implementation of the LMG training
no other similar programmes were running hence the conclusions about improvement
in performance. It is also very clear that the training of DHE in LMG strengthened the
overall performance of the health care system. The aggregate of remittances of reports
at national is in a way a reflection of the performance of DHEs at lower level

89
7.9 Provincial Medical Directors Perspectives
PMD MIDLANDS- Dr. M Chemhuru
The PMD mentioned that there is a great improvement in the district performances
and this can be attributed to the Health Leadership, Management and Governance. An
assessment which was done in the province before the training under the MPH
program by Doctor M Muchekeza revealed that there were many problems especially in
coordination of activities, communication and team work. After the districts were
trained she is noticing a change on how the districts are performing. Areas of Notable
Improvements in DHE performance, Meeting Management, Outbreak detection and
control, Management of disciplinary cases and Health outcomes .Below is a case study
of Gokwe North District in Midlands.
7.10 Case Studies- Districts Case study of Gokwe North District
Gokwe North district is in Midlands Province and it was trained in January 2013.A
total of 5 DHE members were trained in Health leadership, management and
governance. The District medical Officer was trained separately with Gokwe South
Province in July 2011. The district has 19 Health Centres (6 Government clinics, 7
Rural District Council, 4 Mission Clinics, 1 mission hospital and 1 District Hospital).
The curriculum at the medical school did not cover health leadership, management
and governance at district level. It is difficult for the new DMO who just assume
leadership position in the district to lead and provide guidance to the team without
management and leadership skills. The training was very useful to the team especially
issues to do with human resources, procurement and management of public financial
resources.
Despite the DHE being remote the training has managed to build and strengthen team
work within the members. Team spirit has been strengthened by the fact that everyone
appreciates the role of the DHE members and this will enable the team to achieve
more. The DHE decides what to buy and give authority this shows that the whole DHE
is now taking part in deciding what to buy and when. They reported that before the
LMG training buying was solely done by the accountant and the administrator without
consulting other members. Improved performance is also being manifest in how the
DHE schedule and conduct its meetings. They have managed to hold most of the
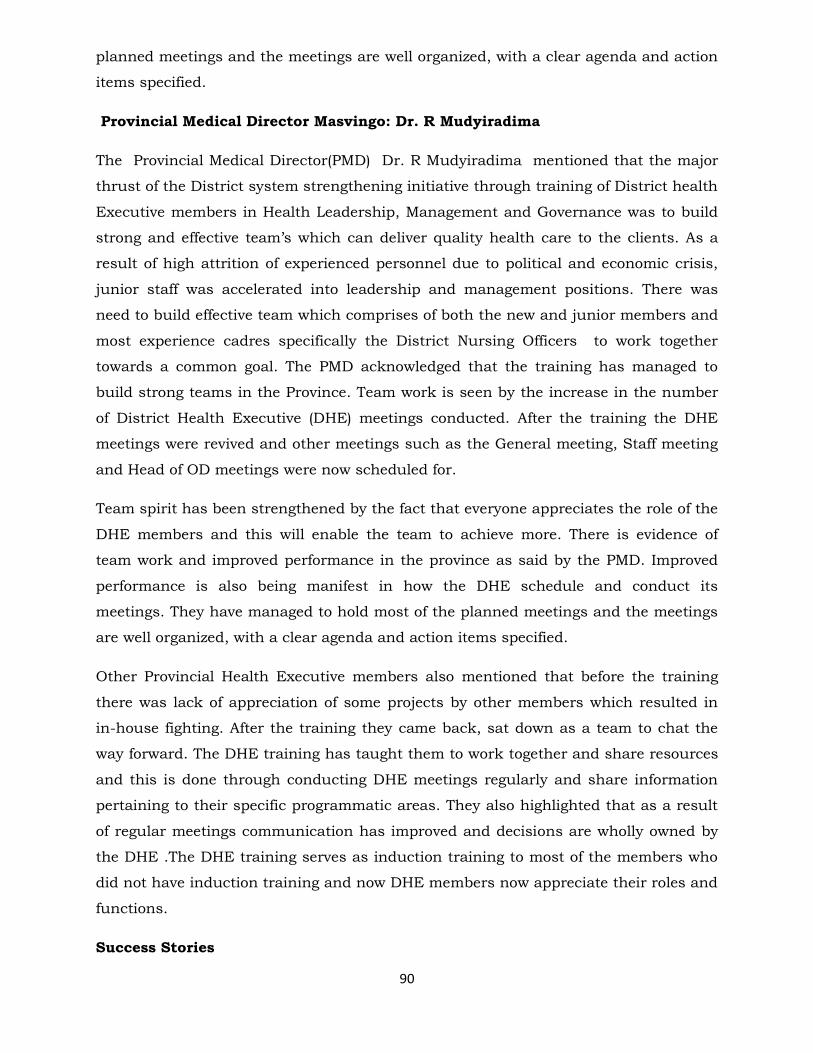
90
planned meetings and the meetings are well organized, with a clear agenda and action
items specified.
Provincial Medical Director Masvingo: Dr. R Mudyiradima
The Provincial Medical Director(PMD) Dr. R Mudyiradima mentioned that the major
thrust of the District system strengthening initiative through training of District health
Executive members in Health Leadership, Management and Governance was to build
strong and effective team’s which can deliver quality health care to the clients. As a
result of high attrition of experienced personnel due to political and economic crisis,
junior staff was accelerated into leadership and management positions. There was
need to build effective team which comprises of both the new and junior members and
most experience cadres specifically the District Nursing Officers to work together
towards a common goal. The PMD acknowledged that the training has managed to
build strong teams in the Province. Team work is seen by the increase in the number
of District Health Executive (DHE) meetings conducted. After the training the DHE
meetings were revived and other meetings such as the General meeting, Staff meeting
and Head of OD meetings were now scheduled for.
Team spirit has been strengthened by the fact that everyone appreciates the role of the
DHE members and this will enable the team to achieve more. There is evidence of
team work and improved performance in the province as said by the PMD. Improved
performance is also being manifest in how the DHE schedule and conduct its
meetings. They have managed to hold most of the planned meetings and the meetings
are well organized, with a clear agenda and action items specified.
Other Provincial Health Executive members also mentioned that before the training
there was lack of appreciation of some projects by other members which resulted in
in-house fighting. After the training they came back, sat down as a team to chat the
way forward. The DHE training has taught them to work together and share resources
and this is done through conducting DHE meetings regularly and share information
pertaining to their specific programmatic areas. They also highlighted that as a result
of regular meetings communication has improved and decisions are wholly owned by
the DHE .The DHE training serves as induction training to most of the members who
did not have induction training and now DHE members now appreciate their roles and
functions.
Success Stories

91
Mutare District
The training has managed to bring a new thinking in the district. It was an eye opener
as team work was really emphasized. Soon after the LMG training, Mutare district
discussed on how best they could cascade the LMG training to the other key members
of the district who were not included out in the DHE initial training. The module on
building effective partnership was very useful since it provided negotiating skills to the
DHE members who then used the skills to discuss with their partners with regards to
resources needed for cascading the LMG training to their wards and rural health
centres. A partner (Plan International)1 who has an interest in capacity building at
community level was identified and was willing to provide support for this training.
Plan International is working in the district under the project of women and
children`s rights. The district was able to take advantage of the work being done by
the organization. A short proposal for our Health, Leadership, management and
Governance was prepared and funding was availed. The funding provided was
complemented by the partial funding from the LMGP for supporting DHT meetings.
The training modules received from the DHE training in form of a CD were used for
cascading training. Key topics were selected since the funding was only for three days.
A three days training was conducted for 12 participant’s .The 5 DHE members that
had been trained in the DHE LMG training facilitated in the lower level training.
Mutare district found that cascading the training was very useful as all members now
have the same understanding. This has facilitated good working relationships and a
good working environment has been created for the benefits of all health team
members and clients at community level. Mutare district managed to solicit for
financial support from their partners and they cascaded the training to other heads of
departments as well as SIC clinics. This was a very positive development as capacity
was built throughout the district health systems
Centenary District
Centenary district health executive used the information learnt during the training to
document all their activities in a manner that attracted a lot of support from donors in
Italy. The DHE agreed that the training equipped them with skills to communicate,

92
document and package their work and sell their ideas to potential funding partners.
They have since sent a proposal for funding to their Italian partners and a grant for
maternal and child health has been provided towards renovations for the waiting
mother’s shelters
Successful stories
This quarter with the support from the project we have managed to conduct our first
District Health Team Meeting since 2010.The meeting was a success and we manage to
with the resources that you provided. A total of 55 participants attended a three day
meeting at Chaminuka training Centre. This provides a good platform for the DHE to get
a full picture of what is happening in the district. As emphasized during the training the
DHE should take a leading role in coordinating health related activities. Sometimes due
to limited resources it is difficult to visit all the clinics in the district so the DHT meeting
we conducted, it enable us to share experiences with all clinics and partners in the
district as well as getting their success and challenges they are facing
This quarter with the support from the project we have managed to conduct our first
District Health Team Meeting since 2010.The meeting was a success and we manage to
with the resources that you provided. A total of 55 participants attended a three day
meeting at Chaminuka training Centre. This provides a good platform for the DHE to get
a full picture of what is happening in the district. As emphasized during the training the
DHE should take a leading role in coordinating health related activities. Sometimes due
to limited resources it is difficult to visit all the clinics in the district so the DHT meeting
we conducted, it enable us to share experiences with all clinics and partners in the
district as well as getting their success and challenges they are facing
Successful Stories Mutare DHE
The training has managed to bring a new thinking in the district. It was an eye opener
as team work was really emphasised. Soon after the training we discussed on how
best we can cascade the training to the other key members of the district who were let
out in the initial training. The module on building effective partnership was very useful
to us as it enables us to look at our partners and identify one who can support us in
cascading the training. Plan International is working in the district under the project
of women and children`s rights, so we prepare a short proposal for our Health,
Leadership, management and Governance training using the materials that we

93
received from the DHE training .We were fortunate enough to receive the funding and
we selected key topics that can be covered in three days and conducted the 3 day
training for 12participants. The 5 DHE members who were trained facilitated in our
training and we also included the GMO, Matron, HRO and the RDC in the training.
Cascading the training is very useful as all members have the same understanding
and when we discuss health related issues pertaining to the district everyone will be at
the same page.
Lupane District
The discussion reviled that there is a great improvement in communication between
the members .The DHE is based at St Luke’s Mission hospital and communication has
improved between the DHE members and the Mission hospital staff .The issue of team
work which was emphasised during the training has enabled planning together of all
health related activities. The module on Human resources was a refresher and helped
them to appoint 18 student nurses in the district. This has also led to the decline of
disciplinary cases during the fourth quarter. There was no misconduct cases reported
from the period July to September 2012.
Management of meetings has greatly improved as the members highlighted that the
meetings are now coordinated with each member effectively contributing to the
success of the district. An invitation is circulated in advance to all the participants.
There is a remarkable improvement in the operation of the trained districts .The
health Leadership, Management and Governance training has contributed to some
extend towards the strengthening of health manpower skills for improved delivery of
services and towards improving quality of care. There has been reported improved
team work, proper management of time, improved running of meetings, reduced
conflicts, correct handling of grievances, protection and efficient utilization of
financial and material resources, improved handling of patients and other health care
users through good ethical practice, coordination with other sectors and partners. The
LMGT includes some aspects of the rules regulations and operational procedures for
DHE members. The inclusion of this subject has helped to introduce new members of
staff to the processes of health care delivery system. This component has been well
appreciated by the participants who indicated that some of the DHE members did not
undergo induction training so these trainings are providing them with requisite
information on how they should perform their day to day duties. If resources are

94
available all the DHE teams should be trained at the same time so that they can
efficiently work together
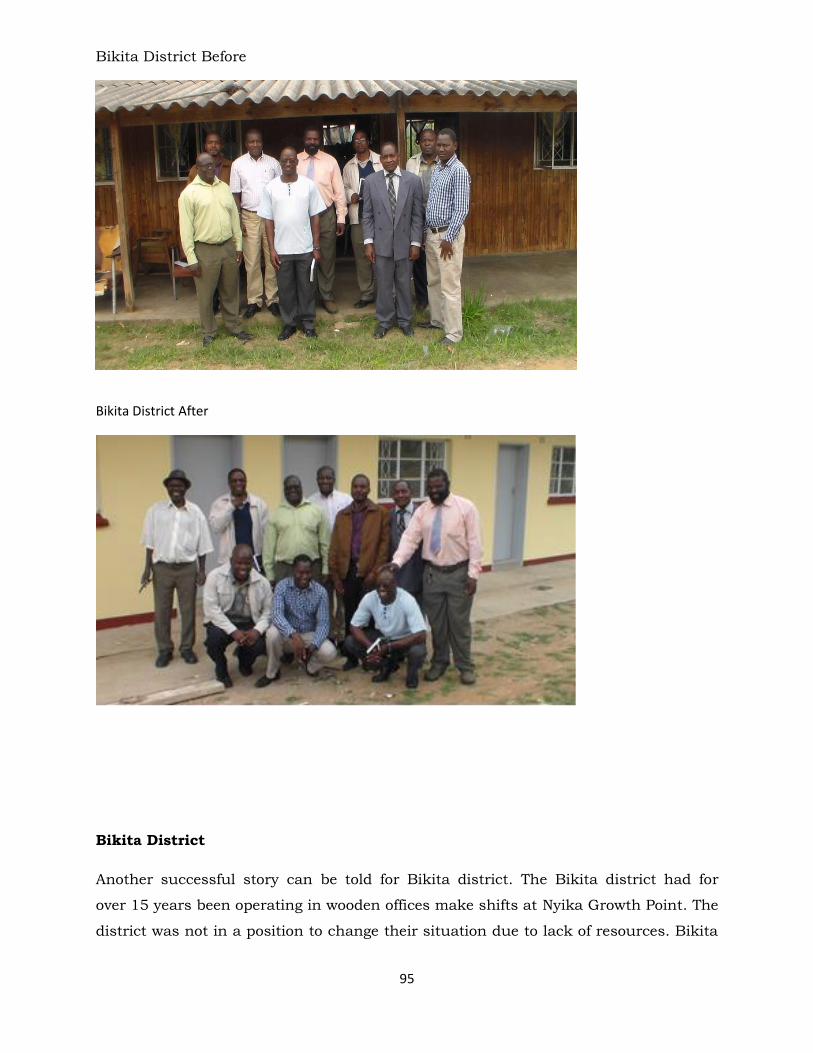
95
Bikita District Before
Bikita District After
Bikita District
Another successful story can be told for Bikita district. The Bikita district had for
over 15 years been operating in wooden offices make shifts at Nyika Growth Point. The
district was not in a position to change their situation due to lack of resources. Bikita

96
district was trained in LMG principles in 2014. Immediately after the LMG training
they realized that they could change their situation through working with partners.
The training in LMG gave them the confidence knowledge skills and confidence to
analyze their partners in terms of their objectives and the partner’s objectives. They
identified a partner that had been operating at the same center and were paying an
exorbitant amount of rentals to the local authority. They approached this partner with
a proposal to assist them to build an office block. The partner obliged since the DHE
included a proviso that they would use these offices under a special arrangement. In
the end the partner gained office space and Bikita district became owners of brand
new offices which gave them motivation and a high morale which the LMG team
witnessed during the evaluation exercise.

97
CHAPTER 8
8.1 Discussions
The evaluation findings indicate that the leadership project that has demonstrated real
change in the functioning of DHEs across all the provinces as illustrated by the
responses and the statements coming from the DHEs themselves. The project started
training the lower levels district health executives since the MOHCC indicated that
this was the level that serves the community and improvement at this level would
benefit all levels. It seems that the MOHC was correct as the evaluation has indicated
improved performance at this crucial level.
There is a remarkable improvement in the operation of the trained districts .The
health Leadership, Management and Governance training has contributed to some
extend towards the strengthening of health manpower skills for improved delivery of
services and towards improving quality of care. There has been reported improved
team work, proper management of time, improved running of meetings, reduced
conflicts, correct handling of grievances, protection and efficient utilization of
financial and material resources, improved handling of patients and other health care
users through good ethical practice, coordination with other sectors and partners. The
LMGT includes some aspects of the rules regulations and operational procedures for
DHE members. The inclusion of this subject has helped to introduce new members of
staff to the processes of health care delivery system. This component has been well
appreciated by the participants who indicated that some of the DHE members did not
undergo induction training so the LMG training has provided the newly deployed with
requisite information on how they should perform their day to day duties. If resources
are available all the DHE teams should be trained at the same time so that they can
efficiently work together. All newly deployed health managers should undergo this
training so as to continuously improve health care delivery
98
8.2 Recommendations
Recommendations
a) In-service training for health managers should continue to be competency
based using the already developed modules so as to ensure success, relevance and
usefulness in the strengthening of the health care systems.
b) Province hospitals and districts to have a an orientation programme that helps
new health managers to understand the health system management processes and
the health service regulations so that they can perform their duties in response to the
MOHCC priorities
c) Methods such as group work and cases studies were found to be very conducive
for learning in future such methods should be used in order to enhance adult learning
d) DCM in collaboration with MOHCC and HSB can work together to develop a
pre-deployment training for health managers to prepare them for new appointments as
health managers at provincial and district level
e) HLMG issues should be included in the training curricula of health workers
since the participants considered the subject as essential for all health mangers as an
important part that prepares them for their roles and functions.
f) There was concern that there should be a continued follow up and mentorship
of trained managers on regular basis.
g) HLMG Training should be made a requirement for promotion to management
positions.
h) The MOHCC to support the identification of further funding for HLMG training
in Zimbabwe in collaboration with interested partners. HLMG should continue to be
supported financially since this evaluation is indicating the need to for in- service
training and pre-deployment training to cater for the high attrition in the MOHCC and
also to cater for other partners that are involved in public health initiatives.
i) DCM LMGP to train trainers of trainers for each province in leadership
management and governance as a sustainable strategy for ensuring quality in health
care delivery and the training to emphasis the concept of working as teams since the
participants rated this module very highly and field work follow up has also indicated
that the module on working as teams was most favourable and the skills are being
applied in the health teams day to day work
Conclusion
99
Success Stories
This quarter with the support from the project we have managed to conduct our first
District Health Team Meeting since 2010.The meeting was a success and we manage to
with the resources that you provided. A total of 55 participants attended a three day
meeting at Chaminuka training Centre. This provides a good platform for the DHE to get
a full picture of what is happening in the district. As emphasized during the training the
DHE should take a leading role in coordinating health related activities. Sometimes due
to limited resources it is difficult to visit all the clinics in the district so the DHT meeting
we conducted, it enable us to share experiences with all clinics and partners in the
district as well as getting their success and challenges they are facing
8.3 Lessons Learnt The institution of a task force is of great importance in the management of a project
since it provides a conducive environment for project development implementation and
evaluation. The task force especially when chaired by policy makers makes access to
institutions and decision makers much easier.
Proving this leadership, management and governance training has come at a time
when it is most needed and appreciated and this has provided a constant source of
motivation for continuation for the project staff as well for other members of the task
force.
The LMGP has been able to work with facilitators from the MOHCW specialty
departments and this has enhanced the quality of content that is given since these
facilitators have hands on experience and are also at the policy making level and
are therefore credible than if we were using facilitators from other sectors which
may not be conversant with policy issues. Working with the MOHCW personnel will
also ensure sustainability since they are training their own personnel.
The parameters set out for coverage indicators of performance in response to the
initial proposal in response to the RAF proved not to be realistic e.g. “supporting 124
DHT meetings per year” with the current budget. There is need to redefine some of the
targets toward a more realistic goal.







