
Born in Cirebon, West JawaDokter from UNIVERSITAS INDONESIAMaster of Public Health: HARVARD-USADoctor of Science: JOHNS HOPKINS-USAPost Doc in Statistics: UNIV of MICHIGAN-USACurrent Activities:
Indonesian Public Health Association, PresidentGlobal Fund TB at FPH-UI, DirectorHealth Professions Coalition for Anti Smoking, ChairmanNational Expert Panel on TB, Health Policy SpesialistIndonesian Healthcare HIV/AIDS Roadmap development,
Head of TeamKomnas Penelitian & Pengkajian Penyakit Infeksi
(PINERE), Expert PanelIndonesian MCH-Nutrition Eval Team, Head of TeamDept of Health Policy & Administration, UI, Past Chairman;
Advice & examnine more than 150 PhD dissertationsNational Health Research Committee, Expert PanelResearch Committee in Hospital, Expert Panel
Adang Bachtiar

Visioning Public Health In Indonesia
Future Leaders’ Responsibility
Presented at Welcomimg Seminar for New Breed of Future PH Leaders & Knowledge Holders - FKMU.UI, 24.08.2013
Materi dapat diakses di: https://www.facebook.com/groups/iakmi.pusat/

Public Health Problemsin Indonesia

1-Healthcare services
2-Health Sector Program & Policies
3-Other Sectors Development

•Rejected, loaded.•Low empathy•Rush time incomplete exams
•Ineffective incentive system for HRH•Low capacity in logistic mgmt
•Problems in professional educ•No systematic
cont. educ
•Weak in referral system•Low acceptancy at
primary care
•Bureacratic reimburse process•Limited package•No Portability & cost-sharing•“Free curative” as vote gating for politician
•Keep revisitation•Non-holistic curatrive approach
•Reactive to illness, no empowerment•No PH spectrum
Policies and procedures
Sub-standardsHealth services
Patients & CommunityComplaints
Problem in HRH and logistics Delayed Tx
Poor provider-patient
relationship
Biz orientation
Substdcompetencies
No follow up
NGO report on HC quality, 2011

Delivery system•No programming nationally•Piloting: no eval•No standards
Delivery system•No programming nationally•Piloting: no eval•No standards
DK Modelling•Minim aliansi dr-drg-perawat utk keluarga•Sinkronisasi dg UKM(-)•Sinkr dg UKP lain(-)
DK Modelling•Minim aliansi dr-drg-perawat utk keluarga•Sinkronisasi dg UKM(-)•Sinkr dg UKP lain(-)
•Only 2% GDP vs 10% abroad (limited funds mobilization)•Curative orientation, not
support healthy life styles
•Only 2% GDP vs 10% abroad (limited funds mobilization)•Curative orientation, not
support healthy life styles
Chronic problems of “Dokter
Keluarga” system
Chronic problems of “Dokter
Keluarga” system
Partial services, only curative. No budgeting
•No vision for DK system•Conflict Professional Orgnz
•No vision for DK system•Conflict Professional Orgnz
More than 3 decadesNon existence of DK syst
Dokter Keluarga Workshop 2012
Govt Stewardship:•Up-down priority•Limited regulations•Low commitment at Local govt
Govt Stewardship:•Up-down priority•Limited regulations•Low commitment at Local govt
Alienated from healthcare systemSupply side problem

56% no ac-
cess
Time to access 1st ANC
Limited accesibility

1st ANC compliance
Mothers w/ =<12 mo. babies
w/ 12-60mos. Babies Total
n % n % n %
Yes 482 37,1 662 38,4 1144 37,9
No 816 62,9 1060 61,6 1876 62,1
DECREASING QUALITY OF MIDWIVES
1.Weighing pregnant woman2.Fundus uteri height3.Blood pressure meas.4.Iron tablets5.Tibia sign for pre-eclampsia

4th ANC compliance
Mothers w/ =<12 mo. babies
w/ 12-60mos. Babies Total
n % n % n %
Yes 75 5.8 133 7.7 208 6.9
No 1223 94.2 1589 92.3 2812 93.1

Health centres limited accessibility, availability, effectivity
Difficulties in HRH
placement
Low ability in budget
advocacy
Low Financial accountability
system
Limited monev & superv
Health technology
assmt & use(-)
Inadequate HC need
assessment
Substandard health care
quality
Inadequate drug supplies and logistics
Barrier to access for poor
people
Inadequate healthcare quality
climate
(Healthcare system workshop, 2008)

Using Baldrige Framework:
Low healthcare performance (low achievement, low quality), related to:
• Low healthcare leadership at healthcentre• Limited HRH capacitation and management• Ineffective health information system at health centre• Limited community empowerment
Bachtiar et al, MCH & Nutr Midterm Ev , 2012

“UNSAFETY CHAIN”
Inadequate Capacitation of Healthcare Management System
Limited good clinical governance
Non-compliance procs.
Delayed responses
Adverse Event

Conclusion? No PH continuum spectrum: Promotive-preventive separated from
curative, and rehabilitative
Hedonistic pragmatic “profit” oriented Over-rated Sectio cessarea Low access for poor people Low access in rural areas
Healthcare quality problems
Sustainability problem

Problems in
Health Programming & Policies

Primary health care is neglected (2010 Health Facility Survey) No maintenance for health devices and appliances Limited procedures for public health and/or clinical pathway/
governance Limited local government’s budget for operational and
maintenance (big proportion for routine budget, esp ‘gaji PNS’)
HRH* supply problems, related to Unstandadized HRH production system Difficult HRH recruitment and placement & maldistributed Limited health professional performance evaluation Limited career path system
*WHO: HRH contributed to est 80% success.

MDs in district area (log)
Poor
people
Pro
port
ion
GPs Mostly in Cities
Doctors tend to open private practices in (big) cities, even in a (very) high competition. It is assumed relate to incomprehensive ability
Poor/rich district

Chronic problems in drugs’ accessibility and availability
Inadequate Health information System, i.e. non-existence Knowledge Mgmt System at health centre Data collection abilities Data analysis capacity Information uses for decision making Information uses for capacity development
Mostly it’s related to limited financing health system

PHC SUSTAINABILITY

LOCAL GOVT BUDGETING FOR HEALTH Means (7 provs)
PR.1 Public Health Programs 6.58%PR 1.1 MCH 0.70%
PR 1.2 Nutrition 0.97%PR 1.3 Immunization 0.12%
PR 1.4 TBC 0.06%PR 1.5 Malaria 0.30%
PR 1.6 HIV/AIDS 0.03%PR 1.7 Diarea 0.00%
PR 1.8 Pneumonia 0.01%PR 1.9 Dengue 0.06%
PR 1.10 Other infectious diseases 0.15%PR 1.11 Non-infectious diseases 0.03%
PR 1.12 Family Planning 0.57%PR 1.13 School Health Programs 0.07%
PR 1.14 Reproductive Health 0.01%PR 1.15 Environmental Health 1.20%
PR 1.16 Health Promotion 0.41%PR 1.17 Disaster Program 0.02%
PR 1.18 Surveillance 0.05%PR 1.19 Other Public Health Programs 1.83%
Gani, 2011
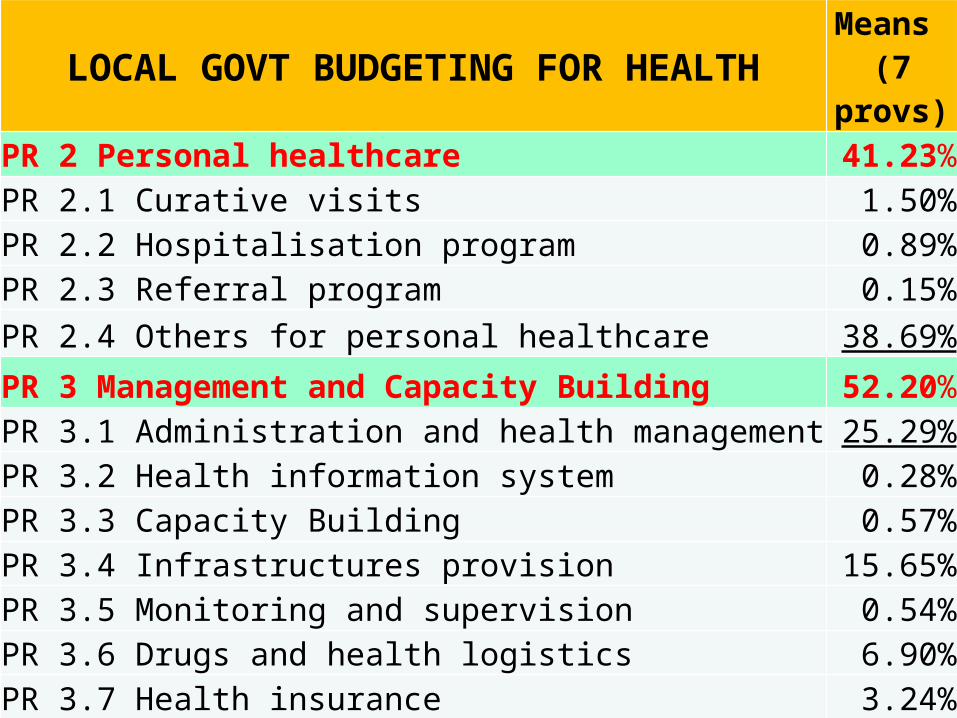
LOCAL GOVT BUDGETING FOR HEALTH Means (7 provs)
PR 2 Personal healthcare 41.23%PR 2.1 Curative visits 1.50%PR 2.2 Hospitalisation program 0.89%PR 2.3 Referral program 0.15%PR 2.4 Others for personal healthcare 38.69%
PR 3 Management and Capacity Building 52.20%PR 3.1 Administration and health management 25.29%PR 3.2 Health information system 0.28%PR 3.3 Capacity Building 0.57%PR 3.4 Infrastructures provision 15.65%PR 3.5 Monitoring and supervision 0.54%PR 3.6 Drugs and health logistics 6.90%PR 3.7 Health insurance 3.24%PR 3.8 Other Capacity Building activities 0.11%
Grand Total 100.00%

WTP
WDP
Disclaimer
Adverse
-200.0% 0.0% 200.0% 400.0% 600.0% 800.0% 1000.0% 1200.0% 1400.0% 1600.0% 1800.0%
-61.9%
-45.0%
1614.3%
490.0%
% Decreasing Financial Accountability2004-2007/08
WTP=Clean w/o restriciton WDP=Clean, but with some notes/restrictionDisclaimer=Couldn’t declare accountability Adverse=Non accountable

TOP REFERRED
REFERRED
1s
t
CURATIVE
5 LEVEL PREVENTIVE MEDICINE
INDIVIDUAL COUNSELLING
FAMILY COUNSELLING
HEALTH PROMOTION(COMMUNICATED SOCIETY)
COMMUNITY EMPOWERMENT
FAMILY RESILIENCE FOR HEALTHY LIFE STYLE
In Conclusion:
Non-Pyramidical “Energy” for Health
PH efforts
Personal HC

Problems in Other Sectors Related to
Health System

Limited understanding of Human Development Index Approach, i.e. MDG targets• Poverty as health risk (vice versa), limitly understood • Non synchronize sectors development to support HDI/MDG goals
Inappropriate, inadequate and delayed budget transaction implementation
Fragmented funding sources for health development
Limited budget accountability
Low priority HRH mgmt at local governments

CONCLUSION: Inefficient Health System
Misdirected & Overheated Personal Care Neglected PHC priorities
Budget orientation for
curative
Educate for curative
only
Overloaded hospital unsafe
care, anger and critics
Limited ability for healthy life
style regulations
Soc Det of Health esp.
Poverty
Unhealthy life styles
Low capacity for PHC devt
Limited budget for
PHC
Non-vitalized PHC
infrastructures
Low ability in health politics
PHC considered not for profit
only
Limited synergy of Acad-Buss-Govt for Comm
EmpowermentFailure in gatekeeping PHC system Low
understanding of community
empowerment
Low & non standardized PH profession’s competenciesModif: Bachtiar, 2011. WHO Meeting for CHW at Srilanka

Work Survey_1
Three (3) competencies are needed in job markets:• Computer literacy• Critical system thinking• Ability to serve
For first timer job seekers:• Positive energy and respect people• Output oriented• Abide to rules and implement regulations/commands

Work Survey_2
Three (3) barriers for first time job seekers:• No working experiences• Limited ability in human relation• Low professional competencies

ENOUGH COMPLAINING....

PH VISION BASED ON SITUATIONS

PH Profesionals Must Have_1
Knowledge-driven model• Adequate knowledge and skills to understand health
problems, at all levels, ie, individual and community
Problem-solving model• Adequate professional skills to solve health problems

Interactive model• Adequate softskills for implementing public health
solutions within social economic development frameworks and perspectives
Enlightenment model• A comprehensive involvement in social cultural,
poltical and economic development for the sake of people’s health
PH Profesionals Must Have_2
First Domain:Structurization of
Public Health Competencies

.
.
.
1a.M
onito
ring
Health
Sta
tus
1b.PH Diagnosis & Investigation
2a.Information,
Capacitation,
Empowerment
2b.Alliances
3a.H
ealth
Pol
icy &
Regul
atio
n3b.Rules
enforcement
4.Stdzed healthcare
5.High skilled HRH
6.Monev
practices
7.Mgmt System
8.RESEARCH

TUJUAN PENDIDIKAN NASIONAL
TERAMPILCERDAS
BERTAQWA

MIRACLEPROFIL LULUSAN KESMAS
Suplai Nakes Kesmas terampil utk kes bangsa yg blm optimal
(belum MIRACLE)

M MANAGER
I INNOVATOR
R RESEARCHER
A APPRENTICER
C COMMUNITARIAN
L LEADER
E EDUCATOR

PUBLIC HEALTH INDONESIAN NATIONAL
QUALIFICATION FRAMEWORK

CORE COMPETENCIES AND LEARNING OUTCOMES
Competency #1Ability to Understand Health Problems & SituationsAbility to define health problems and situationsDetermine usability and limitation of (existing) variety of dataIdentify data sources accurately as a relevant source of informationAbility to evaluate data integrity and comparabilityAbility to abide to principles of ethics in data collection and the use of informationAbility to establish data inference, quantitatively & qualitativelyAbility to evaluate existing data, in terms of risks and benefitsAbility to apply skills in data collection processes, and using IT based information mgmt.

Competency #2Ability to develop health plan dan policy
Ability to collect, to sort and to interpret data and information related to healtjh problemsCapable to establish health policy and appropriate solution to health problemCapable in describing health policy in health improvement implications, legal and administrative frameworks, and social political impactsCapable in determining level of feasibility and expected outputs of each policy optionCapable to use new methods in health situation analysis and planningAbility to make a decisive actionsAbility to develop activity plan to implement health policyAbility to interprete and describe from policy to structures, management and programs
CORE COMPETENCIES AND LEARNING OUTCOMES

Competency #3Capability in establishing effective communication
Ability in communication skills either in-writings, oral or other means
Capable in asking inputs from others effectively
Capable in structuring advocacy activitiesAbility in leading and participating in (interdisciplibary) team to elaborate health issues and their solutionsCapable in aplying and using media, communication technology and networks to spread health informationAbility in deciding appropriate communication for effective solutionCapbale in presenting accurate information on demographic characteristics, statistical data, health program and sicentific products to clients
CORE COMPETENCIES AND LEARNING OUTCOMES

Competency #4Ability to adapt local culture
Capable to apply effective, sensitive method professionally to interact with others who have different cultural background
Capable to develop and adopt-adapt specific PH solutions that accommodate cultural differences
Ability to understand social cultural dynamics that contribute to PH problems
Ability to accept different background of health providers
CORE COMPETENCIES AND LEARNING OUTCOMES

Competency #5Ability to empower community
Capable to synergize community members’ interaction with different backgroundsAbility to identify social cultural background of healthcare behaviorAbility to response to wide spectrum health interests as a part of cultural varietyAbility to identify community leaders and maintain warm effective relationship with themCapable to apply group dynamics processes to improve community participationCapable to describe government roles in providing community empowered PH servicesCapable to describe private sector roles in providing community empowered PH servicesAbility to identify potential community resources for PH services
CORE COMPETENCIES AND LEARNING OUTCOMES

Competency #6Basic Public Health Skills Mastery
Ability to identify individual and organizational responsibility in relation to basic PH services
Ability to define, diagnose, and evaluate health status in a population, determine risk factors and other causes, and define health promotion and prevention solutions
Ability to understand historical background, structures and dynamic interactive of PH system with other system
Ability to identify and capable in applying basic research methods in PH program
CORE COMPETENCIES AND LEARNING OUTCOMES

Competensy #6 (cont’d)Basic Public Health Skills Mastery
Capable in applying group dynamics process for community participation
Capable in applying PH sciences and knowledge, including social behavior applied science, chronic and infectious diseases, accident and disasters
Ability to identify research limitation, the importance of accurate observation and interrelationship concept
Ability in self interest and commitment for PH services and development by using critical thinking approach
CORE COMPETENCIES AND LEARNING OUTCOMES

Competency #7Financial Planning & Management
Capable to develop and to present health budget and financingCapable to manage health program with limited budgetCapable to apply budget process and proceduresCapable in developing strategies for budget prioritiesCapable in monitoring financial andprogram performancesCapable in developing program proposal for financial support from external sourcesAbility in appling human interrelationship skills, motivating others, and conflict resolution in organizationAbility to negotiate many interests and establishing contract and documents in providing community based PH services
CORE COMPETENCIES AND LEARNING OUTCOMES

Competency #8Leadership skills and system thinking
Menciptakan kultur dari stardar etik di dalam organisasi dan komunitas
Membantu menciptakan nilai dasar dan visi bersama dan menggunakan prinsip-prinsip ini dalam petunjuk pelaksanaan
Mengidentifikasi isu internal dan eksternal yang dapat berdampak terhadap penerapan pelayanan esensial kesehatan masyarakat (mis. Rencana strategis)
Memfasilitasi kerjasama kelompok internal dan eksternal untuk menjamin partisipasi dari stakeholder kunci.
CORE COMPETENCIES AND LEARNING OUTCOMES

Competency #8 (cont’d)Leadership skills and system thinking
Capable to contribute to the development, implementation and monitoring standardized organization performances
Capable in applying law and regulation system and political mechanism to stimulate changes
Ability to apply theories for organizational changes and professional practices development
Capable in creating conducive environment to comply to ethical standards in organization and/or in community
CORE COMPETENCIES AND LEARNING OUTCOMES

2nd Domain:Public Health Professions
Involvement

4-Capacitation inHealth Knowledge
Development
1-Capacitation in Policy & Programming
3-Capacitation in“Health is
AlsoIndividual Responsibility”
2-Alliance Capacitation

Provincial Deconcentration capacities
National Guidances
Global Opportunity
Governance
Stewardship
Financial
Capacity building
Benchmarking
Standardization
StewardshipGovernance
Financial
Capacity building
Benchmarking
Standards
HRH Performance
Decentralization capacities
Health Policy Capacity
Hlth Mgtm capacity
HRD capacity
Financial capacity
HIS & Knowl mgmt
Media & nerworks
Knowl management & borderless networks
International funding
Hlth & Devt Policy CommunicationCapacities & competency devt
Modif: Bachtiar 2009
1-Capacitation in Health Policy & Programming

2-Capacitattion in Health Alliances
1-Strong allianceCivil soc &
Govt
2-HealthPriorities
3-Targets & Programs
4-SynergyAction Plam
5-Implementationwith Involvement
6-Best Practices& replications
Health Outcome
Improvement

3-Capacitation in Self Reliance
DisadvantagesAppraisals
Advantages Appraisals
Level ofParticipation
Health Problems’Articulation
ParticipationPlan
ExperiencesOf Success
SelfReliance
Modified fr: Paton, McIver, Johnston, 2007
PH Skills

Global-R
egional, Local Wisdom
4-Capacitation in Health Knowledge Mgmt
PH PROFESSION
Health Technolgy
Learning-Knowledge–Innovation
PUBLIC HEALTH KNOWLEDGE CREATION &
PRESERVATION FOR BENEFIT OF
ALL
SupplyDemand
PH organizations
PH services
Tacit&embedded knowlOpportunity & Threats
Health Outcomes

ROLE & RESPONSIBILITY OF
PH PROFESION
1.Strong Health Profession Inst.
4.Sources for Health action
2.Health professions’Mobilization
3.Knowl & SkillsDevelopment
•SOLIDITY of the Professions•Health Profession orgz existence•Continuous standardization •Accreditation•Continuing Education
•Health System Capacitation:•Health governance•Health policy capacitation•Programming & monev facilitation
•Tacit KNOWLEDGE for:•Innovation in PH Intervention•Innovation in PH-programming•Innovation in Healthy Life Styles
•‘Health is POLITICS’:•Fiscal capacitation•Resource mobilization•Embedded PH knowl•Healthy Public Policy
Adapted from Hughes-Tuohy 2003 & Hicks & Mishra 1993

Involvement of (end) Users
Health professions’ competency development
Stakeholders involvement in each step
Goals of HealthDevt
PlanningDevt
ProcessImplem &
MonevDirect
Outputs
HealthOutcomes(Indirect)
Expected benefits:-Health system capacitation
-Evidence based-Health Improvement
3rd Domain:Close Encounter With Health Users

Close Encounters’ Means & GoalA Effective knowledge production – e.g. PublicationsB Research targeting, capacity building and absorption
(i) better targeting of future research;(ii) development of research skills, personnel and overall research capacity;(iii) critical capability to utilise appropriately existing research, including that from overseas;(iv) staff development and educational benefits.
C Informing policy and product development(i) improved information bases on which to take political and executive decisions;(ii) informing product development.
D Health and health sector benefits(i) cost reduction in the delivery of existing services;(ii) quality improvements in the process of service delivery;(iii) increased effectiveness of services e.g. increased health;(iv) equity e.g. improved alloc of resources at an area level, better targeting and accessibility;(v) revenues gained from intellectual property rights.
E Broader economic benefits(i) wider economic benefits from commercial exploitation of innovations arising from R&D;(ii) economic benefits from a healthy workforce and reduction in working days lost.
Nyantri itu adalah…
• Pembentukan dan pengembangan manusia pembelajar yang diarahkan untuk menjadi anggota sekelompok masyarakat yg ingin tahu segala sesuatu dengan melakukan kegiatan pengkajian ilmiah secara orisinil untuk kebenaran yang teruji sesuai dengan metode ilmu pengetahuan
All, start from being a scholar

• Develop continuously intelectual integrity & capability to produce scientific products (5 domains)
• Systematically prevent any wrong doing of academic integrity
Responsible Scholar is..

Mhsw &PA
Rencana Akademi& Menuju Pasar Kerja
Rencana diri menujuSarjana & Profesi
RencanaBelajar
Individual
Mahasiswa yang berdaya Mahasiswa yang sukses
RencanaMagang &
Karir
Fasilitasi KarirBertahap
Pengemb diri& sosial (ahlak)
Rencanapembelajaran
Magang &Ekstra-
kurikuler
Capaian akademik
& perbaikan
AtmosfirPT
Aksesinformasi
Residensi& Pengemb
skills
Opsi2 pembelajaran
Mgmtkonflik
Mgmtkrisis
KomunikasiMhsw-ortu-PA
Asesmen diri

ACADEMIC INTEGRITY IS HIGH PRIORITY & SERIOUS
BUSINESS (!)

Intelectuals are nation’s
assets/ fundamental,
and within their hands the rise and
fall of of nation
DEDUCTION-INDUCTION CYCLE
• AS SCHOLAR:Disrespect to others
Irresponsible & dishonestUnproductive & laziness
Prejudice and hatredNo empathy for helping each other
WHY SERIOUS ?

• MACRO LEVEL AND LONG TERM EFFECT:
Limited understanding of nature
Instant cultures & diminisihing justice
Destruction of morality and the Nation
WHY SERIOUS ?Intelectuals are nation’s
assets/ fundamental,
and within their hands the rise and
fall of of nation

»Menerima dan/atau menggunakan pekerjaan orang lain dalam kegiatan uji-kemampuan diri sebagai calon intelektual
»Memberikan dan/atau mendorong orang lain menggunakan pekerjaan bukan miliknya dalam kegiatan PENELITIAN
It begins from tiny miny small offense

ONE BIG SERIOUS ACADEMIC DISINTEGRITY IS
PLAGIARISM

PLAGIARISM
(Latin) Plagiarius = Penculik
“Stealing and using other people’s thoughts and speechs, as it is owned” (Webster Dictionary)

THESES GUIDELINES
“Plagiat adalah kegiatan pencurian karya intelektual, baik berupa ucapan, tulisan, maupun media lain ....”
Pedomen Tesis FKMUI, 2010
Plagiarism is defined as the use of the words, ideas, diagrams, etc., of publicly available work without appropriately acknowledging the sources of these materials. This constitutes plagiarism whether it is intentional or unintentional and whether it is the work of another or of you.
An example fromThe Univ. Washington

3 TYPES PLAGIARISM
3 TYPES PLAGIARISM

FORGERY-FABRICATION
Publikasi hasil riset, padahal milik orang lain
Meminjam pekerjaan orang lain untuk mendapat “nama”

Mengkopi materi yang telah diterbitkan termasuk dari internet
Membeli makalah dari “pedagang ilmu”
FORGERY-FABRICATION

• Mengkombinasikan “sana” dan “sini” tanpa menyebutkan sumbernya
• Dan seringkali “Nggak ngerti sendiri” jadinya
“Cut-and-Paste”

• Membuat kutipan “....” tapi lupa(!) mengutip sumbernya
• Menuliskan sebagai Daftar Pustaka tetapi tidak ada hubungan dengan tulisan yg dibuat
Inappropriate Citations
Inappropriate Citations

Merubah alinea milik orang lain tetapi masih menggambarkan fikiran orang tersebut secara jelas, tetapi “lupa” menyebutkannya
Inappropriate Citations
Inappropriate Citations

• Kelas Kakap– Seluruh karya “dicuri”
• Kelas Teri (yang dibiarkan akan menjadi kelas kakap)– Umumnya Bab Tinjauan Pustaka– Lebih sering lagi: alinea yang dicuri
CONTOH-CONTOHCONTOH-CONTOH

CONTOH ALINEA YG DICURICONTOH ALINEA YG DICURI
Biaya pengadaan barang farmasi merupakan posisi terbesar dari biaya rutin.. dst. Burr W. Hupp (1969) menyimpulkan bahwa jika perusahaan tidak sukses dalam pengendalian persediaan, maka.. dst

– Si penulis ternyata tidak memiliki artikel Burr W Hupp (1969)
– Di dalam Daftar Pustaka tidak tercantum Burr W Hupp
CONTOH ALINEA YG DICURICONTOH ALINEA YG DICURI

• Dalam perhitungan pembiayaan rumah sakit, salah satu yang penting diperhatikan adalah biaya rutin penyediaan logistik rumah sakit, karena besarnya biaya yang harus disediakan.. Burr W. Hupp (1969) seperti dikutip oleh X (1997) menyimpulkan bahwa manajemen rumah sakit akan berhasil dengan baik, bila mampu mengendalikan pengadaan logistik.
Jadi, seharusnya?Jadi, seharusnya?

• Teguran ‘terbuka’ (social punishment)
• Penilaian keprofesian
Apa hukuman pelanggaran?Apa hukuman pelanggaran?

Meneliti ulang
Skors dalam profesinya
Dipecat dari pekerjaannya
Di anulir gelar akademik yang didapat
Apa hukuman pelanggaran?Apa hukuman pelanggaran?

Expectations From The Future Leaders
Competitive AdvantagesCompetitive AdvantagesEV
IDEN
CE B
AS
ED
P
UB
LIC
HEA
LTH
CA
RE
EV
IDEN
CE B
AS
ED
P
UB
LIC
HEA
LTH
CA
RE
GLO
BA
L C
ULT
UR
AL
CO
MP
ETEN
CE
GLO
BA
L C
ULT
UR
AL
CO
MP
ETEN
CE
HR
H M
GM
T S
KIL
LS
HR
H M
GM
T S
KIL
LS
ABILITY FOR RESOURCE MOBILZATIONABILITY FOR RESOURCE MOBILZATION
COMMITMENT “HEALTH IS RIGHTS”COMMITMENT “HEALTH IS RIGHTS”
HEA
LTH
P
RO
FESS
ION
S
SY
NER
GIS
M
(ON
E H
EA
LTH
)
HEA
LTH
P
RO
FESS
ION
S
SY
NER
GIS
M
(ON
E H
EA
LTH
)
HEALTHOUTCOME

Universities;Research Centers
KNOWLEDGE SUPPLIERS
Consultants, ProfessionalPractioners,
Informal leaders
PH FACILITATORS
Govt, privates & Communities
DECISION-MAKERS
YOUR GOAL(S)
Knowledge is defined as “a justified true belief that increases an entity’s capacity for effective action” (Nonaka 1994).

Akhlakul
Kharimah
Leadership
Inter-indiv behavior
Indiv Behavior in
Orgnz
Softskills-Softskills-Softskills
Musa, Nadhoriyah As Suluk At Tandzimi min Mandhuril Islam, 1995

LEADERSHIP1
Fairness Leading “walk the talk” Visioner Honesty Responsible Intelligent/smart Orator/Communicator Knowledgable/transfering know-how
Madhi, Al Qiyadah Al Muatsiroh, 2002

LEADERSHIP2
Skillful manager Decisive Creating condusive working climate, i.e trust, warm,
peaceful, outcome focus Caring interaction, i.e to subordinates, clients etc Empowering and participation Effective-efficient

Individual behavior
Ihlas because of Allah Self evaluation & correction Honesty Optimistic Taubat Managing Knowledge Humble

Inter-individual behavior
Team work for the benefit of others (i.e., community) Amar ma’ruf nahi munkar Empathy and caring Obey to the leader Not doing ghibah Prevent from SMS attitudes (hatred/dengki)
Musa, 1995; Luth, 2001, Tasmara, 1996; 2001

Musyawarah Hard work for helping others Patience (for solving others’ problem) Continuous positive improvement High/best achievement orientation
Musa, 1995; Luth, 2001, Tasmara, 1996; 2001
Self control Honesty Responsible Balance between hard work & achievement, with akhirat
orientation Optimizing the works
Musa, 1995; Luth, 2001, Tasmara, 1996; 2001

Professional Efective and efficient Creative Managing new knowledge Teamwork Serving others with IHLAS for service excellence
Musa, 1995; Luth, 2001, Tasmara, 1996; 2001

From those who have much..,
much is also expected

Closing Remarks

THE POWER OF “WE”
Reflection
ACTIONDialogue
Adapted fr: Freire, P. (1995) Pedagogy of the Oppressed. New York: Continuum Publishing Co
ThankYou
.
.
.
.







