
High Acuity Care Program
LifeGas. Living healthcare.

Objectives
In this competitive bidding environment it is important to look for new revenue streams. Hear how to target and service the high acuity patient population in your area through the REMEO Ventilator Subcontracting program:
•Discuss challenges homecares are faced with
•Describe how to market high acuity programs to referral sources
•Explain how to manage high acuity patients
•Discuss equipment and disposable management options
•Key billing tips for this patient population

Challenges in homecare
Regulatory / accreditation
Displacing technology
Reimbursement
Cost increases, overtime, DOT etc
CAPEXGetting referrals
Competitive bidding
How to Survive with All the HME Changes?
Cut Cost….. Check
Cut spending….. Check
Cut staff……???
Cut quality of care…..???
Solutions…..
—Take on new patient populations
—Offer more to your referral sources
— Outsource services
You benefit:
Accept ventilator patients – and sustain relationships with your case managers.
Increase competitiveness by marketing the ability to accept high tech patients.
Add a source of income, without adding staff or increasing capital.

Keys to success…
• Sales and marketing (getting patients)
• Billing & collection
• Develop or Outsource distribution
• Keep fixed costs to a minimum, implement a fixed cost model where possible
• Make your company unique
• Program focus (specialize)
Build core competence
Flexible operation
Differentiate

Home Ventilator Patients
•Home vents do require Trained staff (Respiratory Therapists)
•Home vents can be done with low amounts of clinical staff
•Home ventilators require a lot of staff and overtime
•Home ventilators will increase my liability
•Home ventilators will jeopardize my Accreditation Status
•Home ventilators are not Profitable
•Home ventilators take lots of capital
FACT FICTION

Getting started
Accredited for ventilator
equipment?Insure adequate Capital
Equipment/Supplies are
Readily available prior to
Start up.
Establish Policy Procedure and
Training
Check ventilators, trach supplies
on Medicare 855s form
Add ventilators bynotifying accrediting
body
Yes No
Check ventilators, trach supplies
on Medicare 855s form
Establish Policy
Procedure & Training

Marketing
LifeGas provides:
Monthly home visits by a licensed Respiratory Therapist
Respiratory Therapist on call 24/7
Equipment and gases
Care and training
Key Points for Referrals:
—Standard training time to discharge
the patient
—Availability to begin training in a timely
manner
—Willingness to work with hospital staff
on training
— Demonstrate On- call support
—Do what’s best for the patient!
Communicating The Program To Referral Sources
The placement and care of the ventilator dependent patient involves a partnership among the physician, hospital, home health agency and
equipment supplier. Because of the importance of ongoing patient care in the home setting and necessity of reliable response systems, the
referring hospital/physician may at times consult with the home health agency prior to any selection of equipment supplier. It is key to market
your program and services to both Hospitals and HHA.
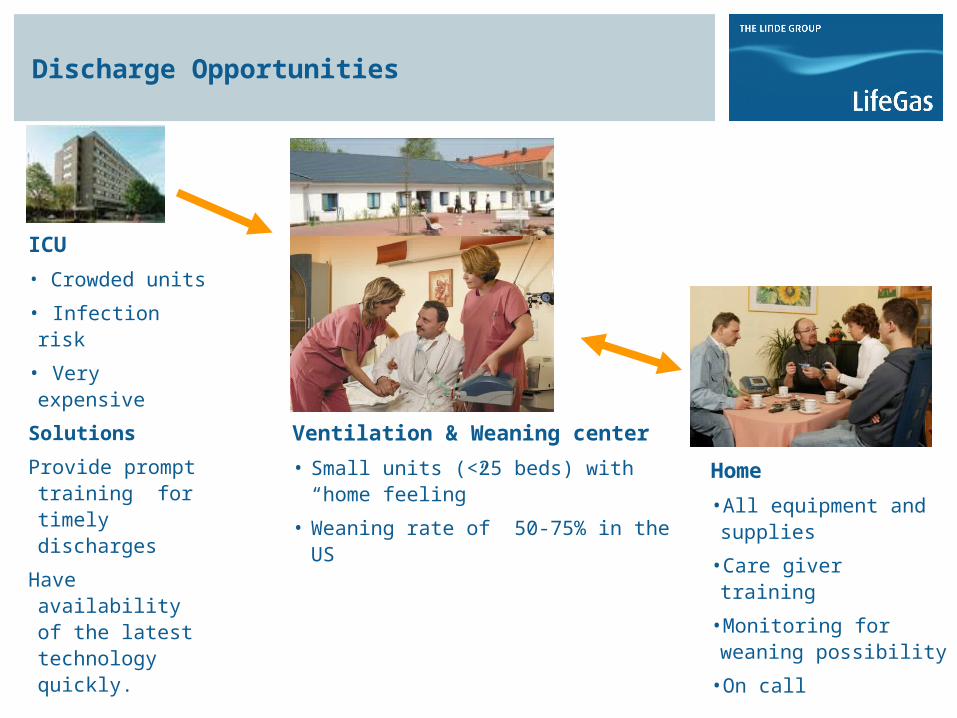
Discharge Opportunities
ICU
• Crowded units
• Infection risk
• Very expensive
Solutions
Provide prompt training for timely discharges
Have availability of the latest technology quickly.
Ventilation & Weaning center
• Small units (<25 beds) with “home feeling”
• Weaning rate of 50-75% in the US
Home
•All equipment and supplies
•Care giver training
•Monitoring for weaning possibility
•On call

Caring for High Acuity Respiratory Patients
You manage:
All marketing
Intake and insurance verification
Maintain continued communication with physician and customer
Provide support to customer (business and after hours)
Billing and billing related duties
Key Factors
—Market Research
—Personnel
—Equipment needs
—Training
—Policy and Procedures
—Acceptance Criteria
—Follow Up

Market Research
•What patients are we targeting?
•How many patients are out there?
•How many competitors in the area?
•How can I be the best in my area?
•What do referral sources want from a vent program?
•What equipment combinations will the customer be looking for?
(Types/brands, etc)
•Will I get any spillover business from taking vent patients?

Personnel
•Need a minimum of 2 clinicians willing to share 24 hour call
•Lead therapist?
•Both therapists need knowledge and experience with vent
patients
•Must be a good teacher and also a good learner
•Must be able to make decisions & communicate effectively with
caregivers
•Telephone skills & support will be key to program success

Capital Equipment
Ventilators:
•average $10K/plus
•Different referral sources may want different types of equipment
•Technology changes often (5-7 year cycle)
•Patient or insurance provider may decide to change companies, leaving you with unused expensive capital equipment
Other equipment needs:
Portable suction
Specialty secretion clearance devices
Backup batteries
Backup ventilators
Disposable (Trach/Trach care kit/yaunker…etc)

New Technology- < 5years old

Ventilator Comparison
Brand Name Market Position Unique Feature Market Rental Price
Respironics Trilogy
ALS Patient Population/HomeC
areAVAP (Average
Volume, Assured Pressure)
$425.00-$550.00
GE I Vent 101ALS Patient
Population/Homecare
PRVC (Pressure Regulated
Volume Control)$425.00-$550.00
Pulmonetics Series
950/1150
LTC/Homecare Jack of all Trades $370.00 & $425.00
PB540 LTC/Homecare Internal battery $425.00-$550.00
LP10/Achieva/HT50 Medicaid
Homecare
Inexpensive $200.00-$325.00

Policy and Procedures
•Will be the most detailed and time consuming process of
the startup
•Responsible party must be well versed in
state/federal/accrediting body requirements
•Will take weeks/months to prepare
•Consider a consultant/guidance from industry
associations
TRAINING, TRAINING, TRAINING
• Internal staff training
— Policies & Procedures
— Equipment (try to standardize)
— Clinical training
— On call services
— Laws and regulations
•Patient/Family training
— Must be comprehensive
— Must include both homecare staff and hospital staff
— Must have competency check off and hands on
— Caregivers must know emergency response procedures
— Repetition, Repetition, Repetition. Take the time to insure compliance
— Must be flexible
Acceptance Criteria
What are the characteristics of a “good” vent patient referral?
•Is the patient stable?
•What is the home environment like?
•How is the patient’s family situation? Adequate caregivers?
•Relying on home health nursing is not the answer….
•Within scope of practice and state laws
•There are patients that are better off in another care
environment
Patient Follow Up
• Establish a policy for the Follow up. Home Visit s should be scheduled to
reduce/eliminate unnecessary readmissions.
Example:
Week 1 – A clinical home visit shall be conducted once within 48hrs following Home Set Up.
Week 2 – A clinical home visit shall be conducted 1 time.
Going Forward: Once monthly and as needed.
• Report any recommendations to the physician and maintain a strong
communication with the family/caregivers.

Other Considerations
—National laws
—State laws
—Delivery Tech vs
Respiratory Therapist
—Patients transferred on
unfamiliar equipment
—Patient improvement

National and State laws
Each state has different laws governing Respiratory Care
FAQ: Is applying NC considered Practicing Respiratory Care?
In some states yes, depending on the state Respiratory Practice act.
FAQ: Is applying CPAP and BIPAP considered Respiratory Care?
Again in some states yes, refer to your states Respiratory Practice act to confirm.
FAQ: Is applying Mechanical ventilation considered Respiratory Care?
Yes, this is considered practicing respiratory care in every state.
FAQ: What if I am unsure about the Respiratory Practice act interpretation?
Contact the Board of Respiratory Care in your state

Definitions
Equipment/ delivery tech- Is responsible for the delivery of equipment and instruction to the use of the equipment, safety of equipment, cleaning and disinfecting, and trouble shooting
Clinical Respiratory Care- Pertains to “hands-on” assessment and treatment of the patient in need of respiratory care, including:
•Observing and monitoring the patient
•Teaching disease management
•Clinical assessment
•Medication use & administration
•Patient/ caregiver education

Outsourcing Options
Equipment- Buy VS RentPurchasing Equipment
—has large expense up front which sometimes takes multiple years to make up
—Ventilator have high ongoing maintenance costs (500-2000 for pm’s)
Rental Equipment
—Factored in monthly price
—Easy to budget
—No maintenance costs
Billing ServicesPrepare staff “before” taking patients
Consider outsourcing if no support available
DisposablesDevelop a standard supply list to build off of

Game-Changing Revenue
Enhance your offering, without expanding your budget.
One vent patient provides the same revenue as seven home oxygen patients.
1:8
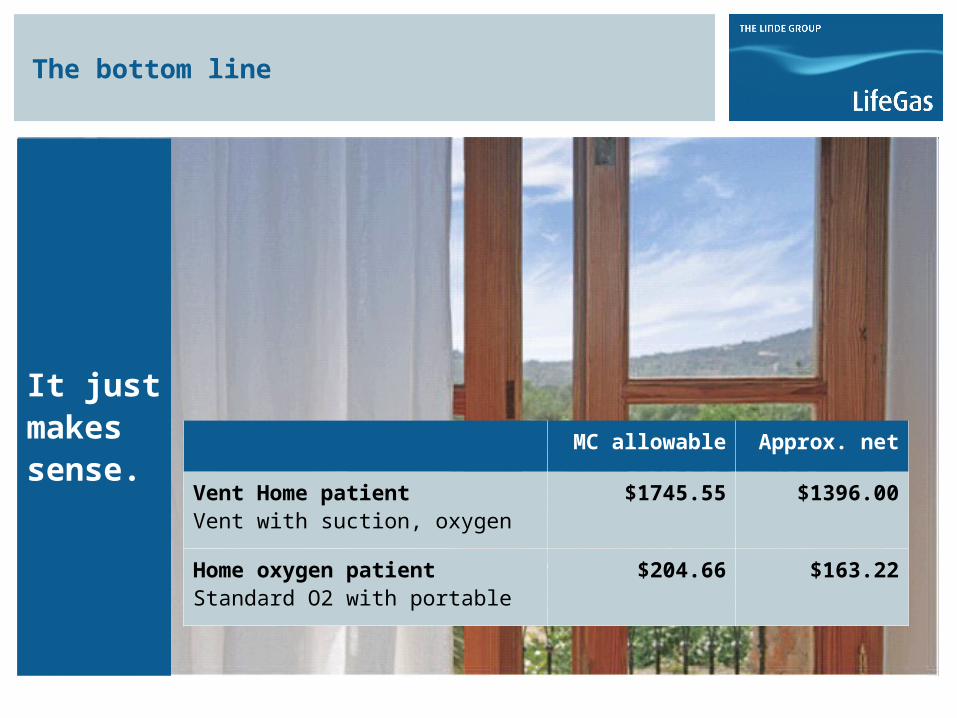
The bottom line
MC allowable Approx. net
Vent Home patientVent with suction, oxygen
$1745.55 $1396.00
Home oxygen patientStandard O2 with portable
$204.66 $163.22
It just makes sense.

Tracheostomy Supplies & Consolidated Home Health Billing (PPS)
According to Medicare guidelines, tracheostomy supplies must be provided by the primary Home Health Agency directly or under arrangement. This information can be found in the Home Health Training Manual, 2007, section 4.1.1.2, and section 4.1.12.1. Payments for these supplies are bundled into the home health agency prospective payment system, which means a portion of the prospective payment system rate represents payment for the supplies, including the supplies not listed in the plan of care. The home health agency, may make arrangements with the DME company providing equipment to the patient, or another provider, to provide the supplies needed in conjunction with the plan of care for the patient at a special retail price. If no arrangements are made prior to the patient’s discharge, the Home Health Agency will be responsible for providing any and all supplies that are referred to per the consolidated Home Health Billing System (PPS).
The following supplies are the most common to be denied due to Home Health Consolidated Billing (PPS)…………………..
•A4217---Normal Saline (Box of 100)
•A6402 ---Trach Drain Sponges (Box of 25)
•A4623 ---Trach Inner Cannula (Each)
•A4624---Suction Catheters--- (Each)
•A4629---Trach Care Kits (Each)
•A7525---Trach Mask, Adult (Each)
•A7526---Trach Collars, Adult (Each)
•A7521---Trach ,Various Sizes & Types (Each)
•A7520---Trach, Cuffless Fenestrated (Each)

Billing Reminders for Home Ventilator Patients
•If patient is prescribed oxygen, don’t
forget to have a qualifying O2 saturation
two days prior to discharge when
applicable
•It takes approximately three days for a
respiratory therapist to adequately train
the caregivers on the ventilator.
•Make sure to verify if patient will be
receiving home health services, due to
the fact that some trach supplies fall
under the consolidated billing (PPS).
•Verify if patient has had DME equipment
before from another provider.
Billing Tips Cont’d
•Don’t take a vent patient home on a
Friday, due to the weekend.
•Make sure to follow all standard
insurance verification of benefits for DME.
•Have all Dr.’s written orders in the office
prior to set up.
•Notify the local utilities company that
you have a ventilator patient in case of an
emergency.
•Ventilators use standard orders for
billing, there is no designated CMN for
them.
Thank you foryour attention.
LifeGas. Living healthcare.







