Dr. Sara Davison
Honoring Patient Choice: Conservative
Kidney Management for Patients
Unlikely to Benefit from Dialysis

Presenter Disclosure
• Faculty: Sara Davison
• Relationships with commercial interests:• Grants/Research Support: CIHR, Alberta Innovates, NARP• Speakers Bureau/Honoraria: None• Consulting Fees: None• Other: None

Potential for conflict(s) of interest
• Dr. Sara Davison has no potential conflicts of interest to declare

Caring For Bob

• Describe the development and philosophy of the online, interactive CKM Pathway for patients who choose to not have dialysis.
• Describe the key components of Conservative Kidney Management and the CKM Pathway
• Identify which patients are most likely to benefit from CKM using the Patient Decision Aid
Learning Objectives

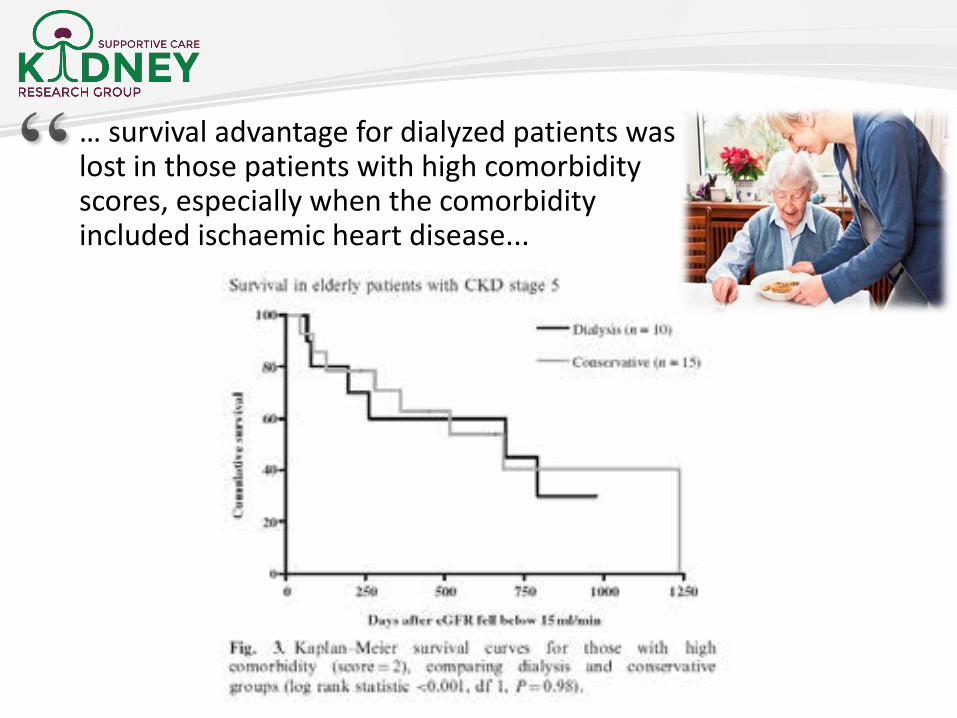
… survival advantage for dialyzed patients was lost in those patients with high comorbidity scores, especially when the comorbidity included ischaemic heart disease...

“Comprehensive conservative care” is planned holistic patient-centered care for patients with G5 CKD -includes:
Shared decision-making
Delay progression of kidney disease & minimize complications
Detailed communication including advance care planning
Symptom management
Psychological support
Social and family support
Cultural and spiritual domains of care
Does not include dialysis
Conservative Kidney Management (CKM) is an alternative treatment option to dialysis or transplant

Develop, Implement & Evaluate a Provincial CKM Clinical Pathway
The goal …….
Live well without dialysis
Providing sustainable, high-quality, evidence-based care for patients unlikely to benefit from dialysis in a coordinated, standardized & equitable manner across Alberta.

Co-Developed: Community Stakeholders

• Readiness to change assessment- Involved all nephrology multidisciplinary
staff - involved in the care of patients
with advanced CKD
• Barriers and facilitators to care- World Cafés- Provincial-wide surveys
CKM Pathway Development
11

12
Content Education Implementation Access Communication Resources
CKD guidelines
Kidney clinic education
Learning collaborative
On-line access
Professional roles (negotiated)
Patient Decision Aid
Symptom Rx Cross training (community)
Balanced score cards
Interactive “3 min rule”
NetCare access to consultation letters
EMS Assess, treat and refer
Patient care map
“Crucial” conversation training
Local opinion leaders
Telehealth & combined community clinics
CKM status on Green Sleeve(GCD)
24/7 palliative care support
Referral triggers
On-line education modules
Consensus building
Resource lists
Care Plans (Green Sleeve)
Patient support groups
HCP care plan
CME credits Flexibility at the local level
Phone line for HCP
Letters to primary care
Crisis Rx Scripts for Health Link (patients)
Home care and GP care conferences
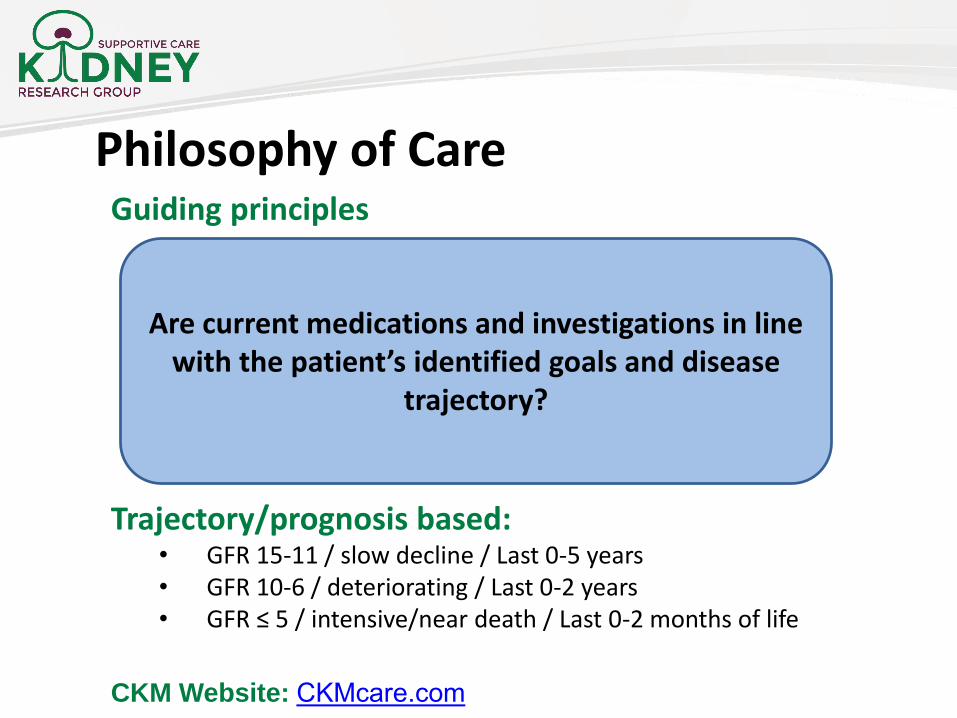
Guiding principles
Trajectory/prognosis based: • GFR 15-11 / slow decline / Last 0-5 years• GFR 10-6 / deteriorating / Last 0-2 years• GFR ≤ 5 / intensive/near death / Last 0-2 months of life
CKM Website: CKMcare.com
Are current medications and investigations in line with the patient’s identified goals and disease
trajectory?
Philosophy of Care


Patient Symptom Handouts
ItchPainNausea & vomitingTirednessRestless legsSleepSwellingShortness of breathSymptom diary
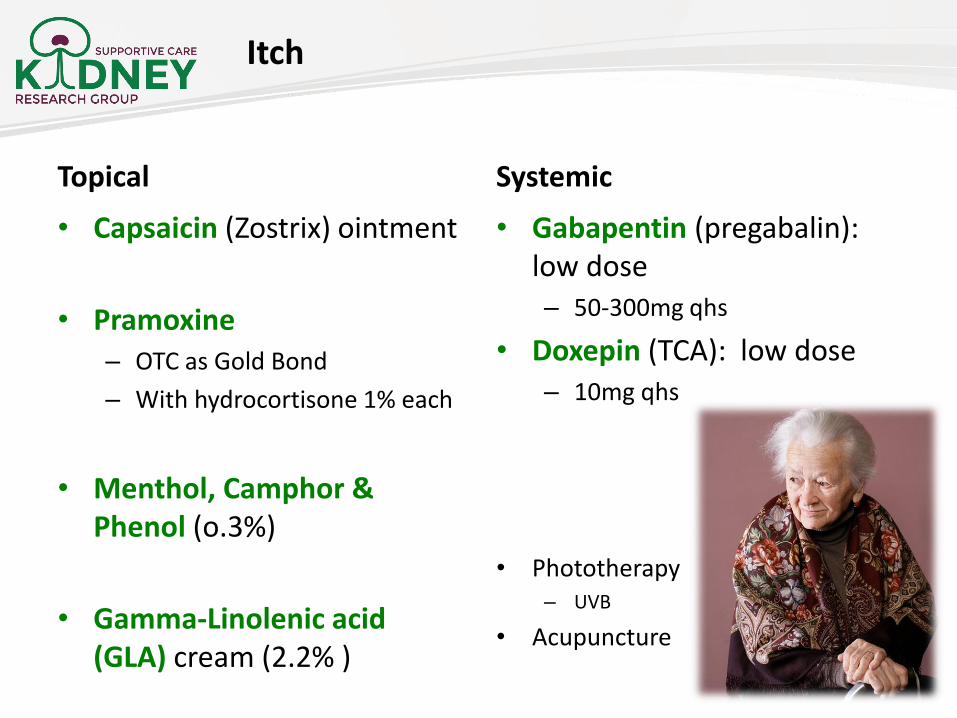
Topical
• Capsaicin (Zostrix) ointment
• Pramoxine– OTC as Gold Bond
– With hydrocortisone 1% each
• Menthol, Camphor & Phenol (o.3%)
• Gamma-Linolenic acid (GLA) cream (2.2% )
Systemic
• Gabapentin (pregabalin): low dose– 50-300mg qhs
• Doxepin (TCA): low dose– 10mg qhs
• Phototherapy– UVB
• Acupuncture
Itch

CKD Guidelines & Guiding Principles for a Palliative Approach to Care
CKD Guideline
Guiding Principle Recommendation
Lipids Reduce risk of cardiovascular related mortality and morbidity.
Patients will not likely receive benefit from statins in the last few years of life; possible improvement in QOL from stopping statins. …… Stop statins for CKM patients.
Blood Pressure
Avoid very high readings while optimizing cognition and physical function (minimize risk of falls).
≤160/90 mmHgGFR < 5: No longer necessary to monitor BP. BP medications can be stopped.Diuretics are a unique consideration……

CKD Guidelines & Guiding Principles for a Palliative Approach to Care
CKD Guideline
Guiding Principle Recommendation
Ca / PO4 Hyperphosphatemia can contribute to pruritusand RLS. Ca & Po4 depositions can lead to myalgias, arthralgias, and pseudogout.
Patients can liberalize their diet if they want. Interventions only if high PO4 is thought to be contributing to symptoms. If the patient desires treatment – monitor levels every 3 months. GFR < 5: stop interventions and monitoring.
Vit D May recommend active vitamin D to address the potential role of active vit D deficiency in fatigue, weakness, and muscle loss.
Vitamin D3: there is lack of consensus to support routine supplementation in patients with CKD.Calcitriol (active form of vitamin D). Suggested starting dose: calcitriol 0.25mcg PO 3 times a weekPTH monitoring is not required

EMS Palliative and End of Life Care
Assess, Treat and Refer Program (EMS ATR)
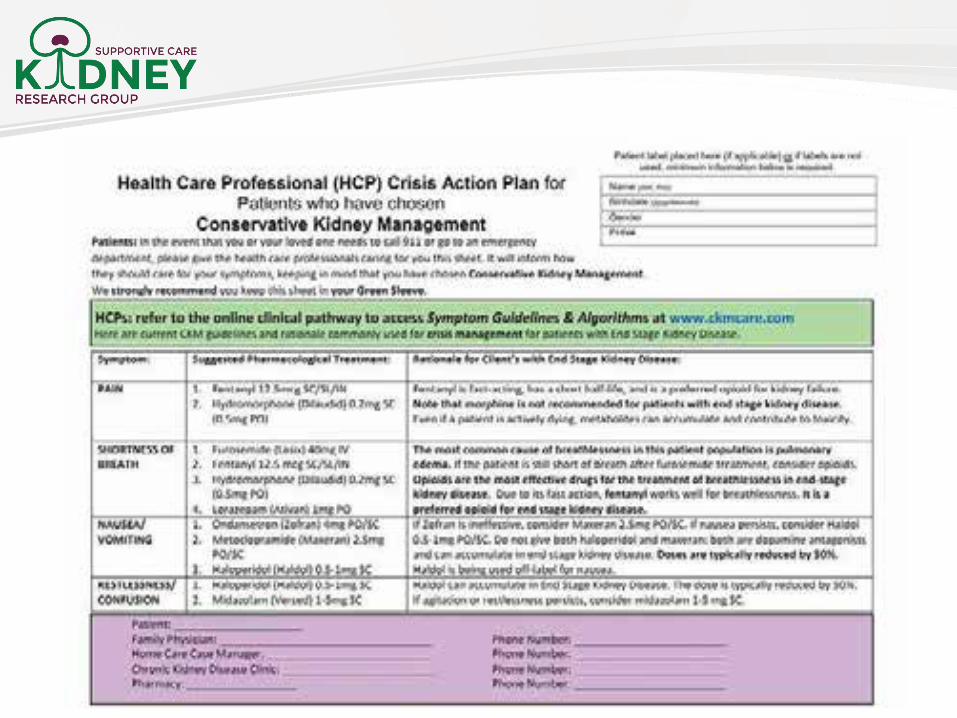
• EMS Crisis Action Plan
• Patient Crisis Action Plan
• Participation in 2nd Innovation Collaborative
Community Partners
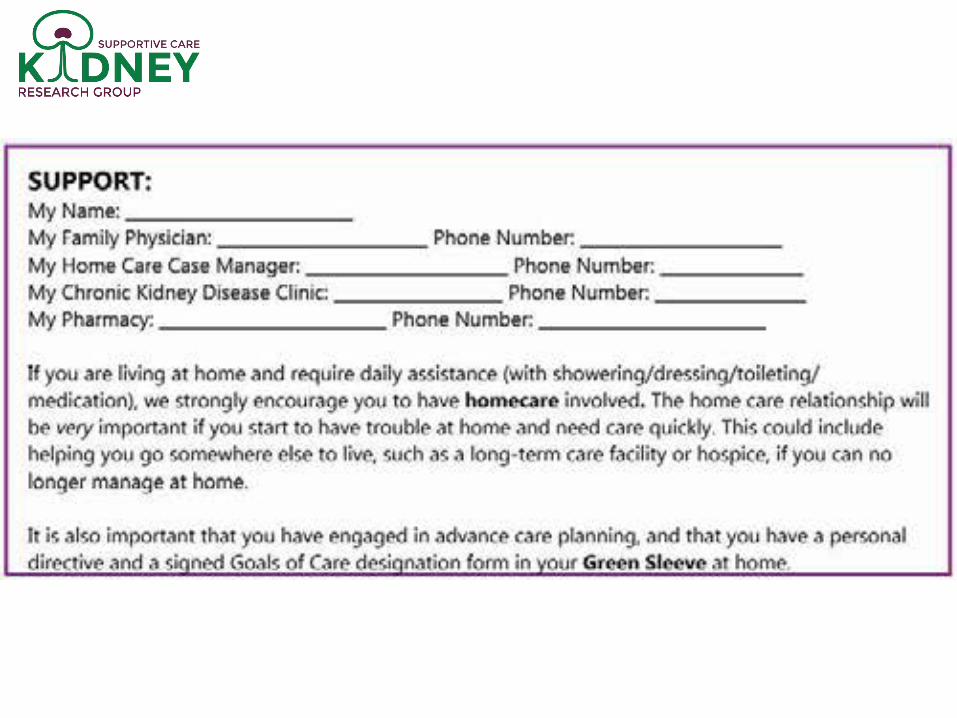
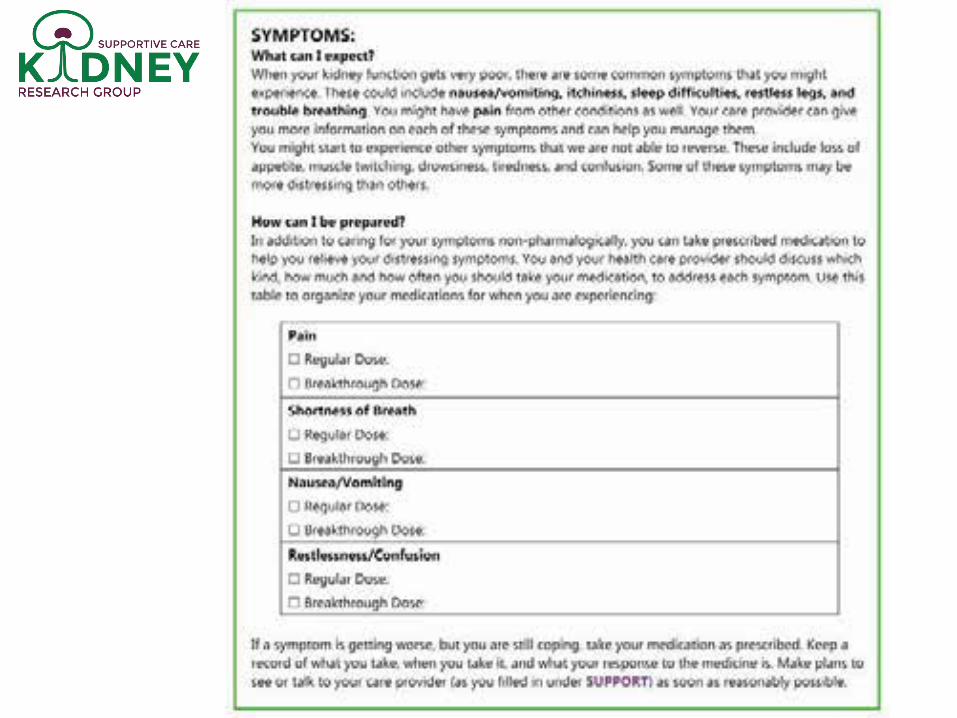
A crisis action plan is used to plan for and be prepared for a decline in your kidney function. This plan will help you: know who to call (SUPPORT), which medication to take (SYMPTOM) and what to do in an EMERGENCY, as your kidney function worsens.
Patient Crisis Action Plan



Home Care
• Ongoing project participation from Home Care stakeholders
• Streamlining of referrals
• Easy access to referral on CKM Pathway
• Targeting Home Care Clinical Nurse Educators
• Presentation to Home Care Staff
• Home Care Presentation to the Chronic Kidney Disease Clinics
Community Partners……



Patient Resources

Quality Indicators
Targets
Action Plans
Care and patient outcomes
Self evaluation
Implementation: Innovation Collaborative

Great Teams, Great Care Award

• Passive decision making (pertains primarily to older patients)
• Older patients generally accept dialysis, they do not choose it.
• Their acquiescence reflects standard clinical pathways that they generally do not question.
• Passive acceptance generates profound questions about the meaning and worth of their life on dialysis.
• 62% regret the decision to start dialysis v. conservative therapy
Davison CJASN 2010
• Confusion re: goals of treatment, about what is gained & lost
• Do I really need this? Can I ever get off? When will this end?
Decision-Making Around Dialysis Initiation

Qualitative study: 31 elderly dialysis patients (US). Ladin K. NDT 2016, Aug 30
• Many felt they had no choice in the decision to start dialysis “My doctor told me that … I had to do dialysis.”
• Were not informed fully of their options.
• Those who recalled shared decision-making tended to have a more positive experience on dialysis.
Study of 99 HD patients (US) Song MK et al. NDT 2013;28(11):2815-23.
• 70% reported that the risks and burdens of dialysis had never been mentioned prior to starting dialysis
• 67% felt that they had been given no choice about starting dialysis
• Only 1 patient recalled the option for CKM being discussed.
Decision-Making Around Starting Dialysis
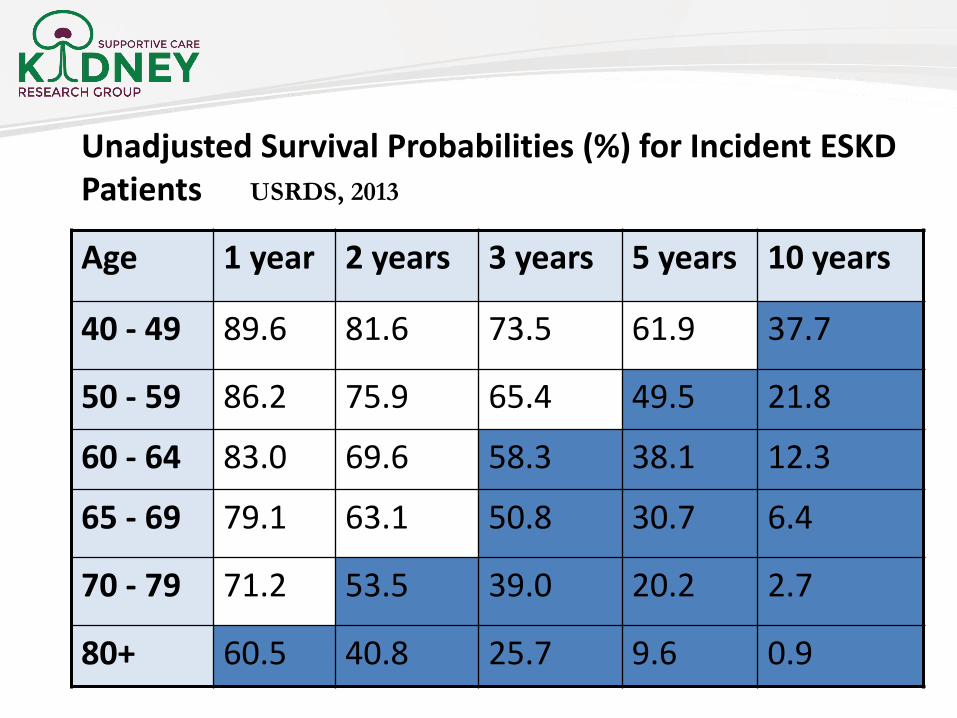
Unadjusted Survival Probabilities (%) for Incident ESKD Patients
Age 1 year 2 years 3 years 5 years 10 years
40 - 49 89.6 81.6 73.5 61.9 37.7
50 - 59 86.2 75.9 65.4 49.5 21.8
60 - 64 83.0 69.6 58.3 38.1 12.3
65 - 69 79.1 63.1 50.8 30.7 6.4
70 - 79 71.2 53.5 39.0 20.2 2.7
80+ 60.5 40.8 25.7 9.6 0.9
USRDS, 2013

Survival for ESKD Patients v. General Population
50
60
40
30
20
10
020 30 40 50 60 70 80
General population
Dialysis
Expected remaining life-years
Age (years)
EuropeUS Whites
dialysis no dialysis
Similar life expectancy

Caring For Fred
• 77 year retired farmer with long standing hypertension.
• Recent MI with 3V CABG
• Still lives independently on his farm in rural AB
• eGFR ~ 12 ml/min/1.73m2 (currently stable)

Caring For Fred
“What is the right care for Fred?”
1. What is his risk for progression to needing dialysis?
2. What is his anticipated prognosis on dialysis v. CKM?

Smart phone app: http://www.qxmd.com/kidney-failure-risk-equation(model is based on age, gender, GFR and UACR)
C statistic 0.91
What is Fred’s Predicted Probability of Needing Dialysis Over 2 & 5 Years?
Risk of Progression to ESKD (dialysis)
Fred: 77 yearseGFR 12 mlUACR 70 mg/g
Over 2 years
Over 5 years
21%
52%


1. Dialysis is not for everyone. Dialysis can’t cure kidney failure, but it helps some patients live longer and feel better.
2. The older and sicker the patient, the less likely it is that dialysis will help. There is less (if any) advantage to dialysis if:
a. Multiple comorbidities b. Dementia or frailtyc. IHD/CHF d. Nursing home
3. Some people will live as long and feel better with Conservative Kidney Management (CKM), which does NOT include dialysis.
4. Alberta’s CKM Pathway provides evidence-based care strategies for an integrated care plan including a patient decision aid to facilitate discussions about whether dialysis or CKM is the right care for a given patient.
5. Future directions: PAN SCN initiative for a single supportive/EOL care pathway, regardless of comorbidity.
CKM website CKMcare.com
Summary

Acknowledgements
Kidney Supportive Care Research Group (KSCRG)
www.ualberta.ca/~kscrg
CKM website CKMcare.com
My inspirations . . .

Questions?
“The good physician treats the disease. The great physician treats the patient who has the disease.”Sir William Osler







