
Improving Retention, Outcomes
and Supervision with PCOMS
Presented by George S. Braucht, LPC & CPCS
March 8, 2017
Thomas Durham, PhD
Director of Training
NAADAC, the Association for Addiction Professionals
www.naadac.org
Produced By
NAADAC, the Association for Addiction Professionalswww.naadac.org/webinars

www.naadac.org/webinars
www.naadac.org/PCOMS-retention-
outcomes-supervision-webinar

Cost to Watch:
Free
CE Hours
Available:
2 CEs
CE Certificate for
NAADAC
Members:
Free
CE Certificate for
Non-members:
$25
To obtain a CE Certificate for the time you spent watching this
webinar:
1. Watch and listen to this entire webinar.
2. Pass the online CE quiz, which is posted at
www.naadac.org/PCOMS-retention-outcomes-
supervision-webinar
3. If applicable, submit payment for CE certificate or join
NAADAC.
4. A CE certificate will be emailed to you within 21 days of
submitting the quiz.
CE Certificate

Using GoToWebinar – (Live Participants Only)
Control Panel
Asking Questions
Audio (phone preferred)
Polling Questions

George S. Braucht, LPC & CPCS
Email: [email protected]
Website: brauchtworks.com
Webinar Presenter
Brauchtworks ConsultingApplying Science to Practice
Webinar Learning Objectives. Upon completion of this
session participants will be able to:
Explain four research-
based factors
responsible for client
change that cut across
professional disciplines
and preferred treatment
models.
Assess the client’s vital
perceptions of recovery
progress and satisfaction
so that services can be
empirically tailored to the
individual’s characteristics,
circumstances, and
resources.
Use the simple yet feasible,
valid, and reliable tools to
gather practice-based
evidence of service process
and outcome effectiveness.
1 32
Promoting currently experienced and cumulative career growth
I just want to help people.
Experimental-physiological psychology
Community psychology
Licensed Professional Counselor
Certified Professional Counselor Supervisor
Certified PCOMS Trainer with the Heart and
Soul of Change Project: Dr. Barry Duncan
Key References
Poll Question #1: My primary role is:
• Treatment service provider (counselor,
social worker, therapist, etc.)
• Prevention service provider
• Clinical supervisor
• Administrator
• Other
• Apparently I am in the wrong webinar

It’s never too late to be
who you might have been.
George Eliot, Middlemarch
(Mary Ann Evans, 1819-1880)
Incorporates the most robust predictors of therapeutic success into an outcome management system that partners with clients while honoring the daily pressures of front-line service providers

Compared to TAU…
Larger treatment
gains via ORS
More clients reached
reliable change
and clinically
significant change
Attended more
sessions
Compared to TAU…
More pre-post
treatment gains
More clients NOT
were retained
Achieved higher
satisfaction ratings
from therapists &
commanders
Five Randomized Controlled Trials (so far!)
Poll Question #2: Empathy, genuineness
and positive regard are the necessary
and sufficient conditions for change.
• True
• False
• Not sure

Lambert (2013) meta-analysis
Empathy: 57 studies found r of .31
Positive Regard: 18 studies found r of .27
Genuineness: 16 studies found r of .24
Each is more powerful than any technique that
you can ever wield as model differences = d of .20
Empathy, Genuineness & Positive RegardRogers, C. (1957). The necessary and sufficient conditions of
therapeutic personality change. The Journal of Consulting
Psychology, 25, 95-103.
Lambert, M. (2013). Outcomes in psychotherapy: The past and important advances.
Psychotherapy, 50 (1), 42-51.
1. Practice Intentionally Not Knowing
2. Open-ended questions
3. Affirmations/validations
4. Reflections/paraphrases
5. Summaries
6. Information-giving
Relationship Enhancement Skills
to Solicit and Provide Feedback (PINK OARSI)

See Relationship
Enhancement
Skills Overview:
PINK OARSI
at
brauchtworks.com/
Toolkit
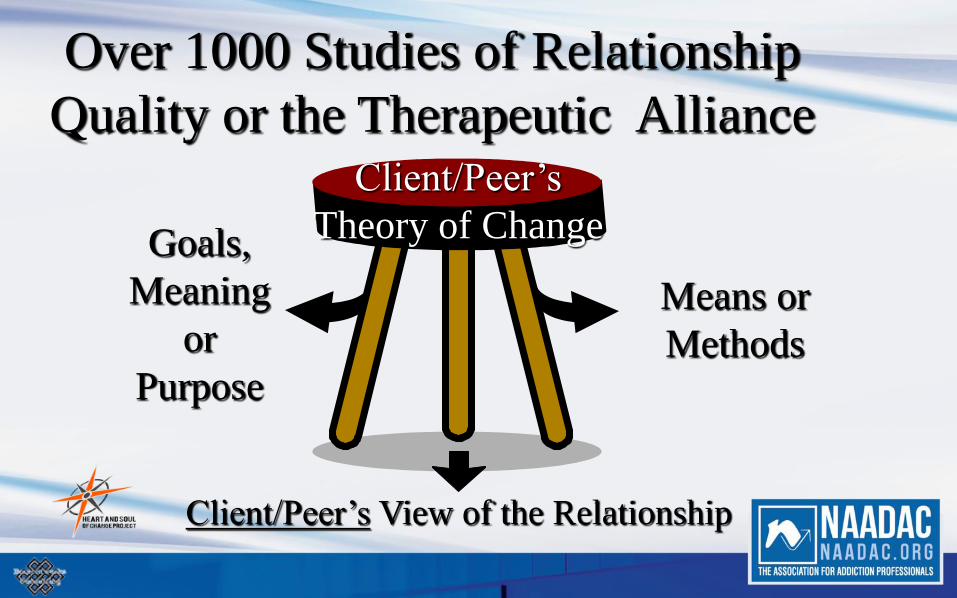
Means or
Methods
Goals,
Meaning
or
Purpose
Over 1000 Studies of Relationship
Quality or the Therapeutic AllianceClient/Peer’s
Theory of Change
Client/Peer’s View of the Relationship

Poll Question #3: What percentage of your
clients do not change or deteriorate?
• 10%
• 20%
• 30%
• 40+%
• I don’t know

youtube.com/watch?v=-
5laIowDL-o
Dr. Michael Lambert
Brigham Young University
Look and listen for:
1. What percentage of clients:
A. Don’t change
B. Deteriorate
C. Improve
D. Achieve recovery
2. What to do about treatment
failures?
A.
B.
C.

1. Empathy
2. Positive regard
3. Genuineness
4. Feedback
Four Research-based Factors Responsible
for Change Across Disciplines and Models
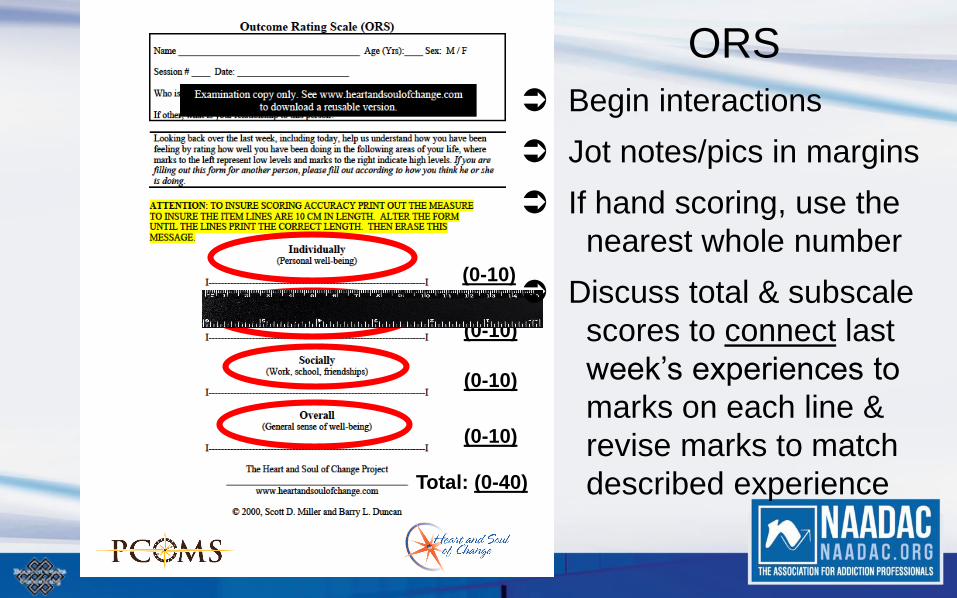
Total: (0-40)
(0-10)
(0-10)
(0-10)
(0-10)
ORS
Begin interactions
Jot notes/pics in margins
If hand scoring, use the
nearest whole number
Discuss total & subscale
scores to connect last
week’s experiences to
marks on each line &
revise marks to match
described experience

O
O OO
23
2-1
28
O
Johnny B. Good
20 29 31 30 32 31 29 30 31
An eight point increase, from
the client’s point of view!
2-8 2-15 2-22 3-14 3-21
O
3-28
O
4-6
O
4-13
O O
4-20
O
4-27
O
31
Reliable change = 6+ points
Clinically significant change/recovered =
6+ points and exceeded the clinical cutoff!
5-5
18
I

5~10 minutes before session ends
35 or less = ask with gratitude, what would
make the next session better or more useful?
Relationship Rating Scale is the version for
peer recovery support service providers

Recovery Action & Progress
(RAP) Group Handout
Facilitator’s main job: Model
PINK OARSI
60 minutes: 10 or less participants
Have blank ORSs (& GSRSs)
available before group start time
Client folders for ORSs,
GSRSs, SCORE Board,
name tag/tent, Recovery
Capital Scale & Plan, etc.
Buy a new whip because the government says it is an evidence-based practice and they will give us $$$$.
Declare that, “This is the way we have always ridden dead horses” or “This is how I learned to ride dead horses and I’ve gone far so just do as I say” perhaps to “protect your check.”
Appoint a committee to study dead horses and write a white paper on “green” ways to make them faster.
Arrange visits to far off lands to see how they ride dead horses. Attend training sessions on improving dead horse riding abilities. Harness several dead horses together for increased speed. Mindfully declare that, “No horse is too dead to beat.” Provide additional funding to buy GMO-enhanced hay. Write an organizational strategic plan on, “the horse is better, faster,
and cheaper dead.” Promote the dead horse to a supervisory position.
Cherokee Tribal Wisdom says upon discovering that you
are riding a dead horse, the best strategy is to DISMOUNT and find
a new horse. Today however, we often try other strategies.
Polling Question #4: I experience
immediate growth and cumulative
career development during or after
most supervision interactions.
• True
• False
• I don’t know or rather not say

Provider Variation: Feedback Improves Effectiveness!
Counselor's Outcomes(n=30 or more cases)
0
0.20.4
0.60.8
11.2
1.41.6
1.8
1 (n
=94)
2 (n
=74)
3 (n
=67)
4 (n
=65)
5 (n
=59)
6 (n
=58)
7 (n
=55)
8 (n
=50)
9 (n
=48)
10 (n
=48)
11 (n
=47)
12 (n
=47)
13 (n
=41)
14 (n
=41)
15 (n
=40)
16 (n
=39)
17 (n
=37)
18 (n
=35)
19 (n
=34)
20 (n
=31)
21 (n
=31)
22 (n
=30)
Counselor
Eff
ec
t s
ize
Mean Effect Size for all Cases
Miller, Duncan, Sorrell,& Brown. (2005). The partners for change outcome management system. Journal of Clinical Psychology,
61(12), 199-208.

1. Valid initial Outcome Rating Scale (ORS); Duncan, 2014
35+: Invalid initial score – why come to see you?
ORS average, 500,000+ administrations: 18-20
Goal: Less than 1/3rd over the Clinical Cutoff (25, 28, 32)
2. Reliable change index (RCI*)
6+ point increase from the initial ORS
3. Clinically significant change index (CSCI*)
6+ and cross the Clinical Cutoff
*Jacobson & Truax, (1991) & Jacobson et al, (1999)
Immediately Experienced and Cumulative Career Growth:
Three Research-based Progress Indicators
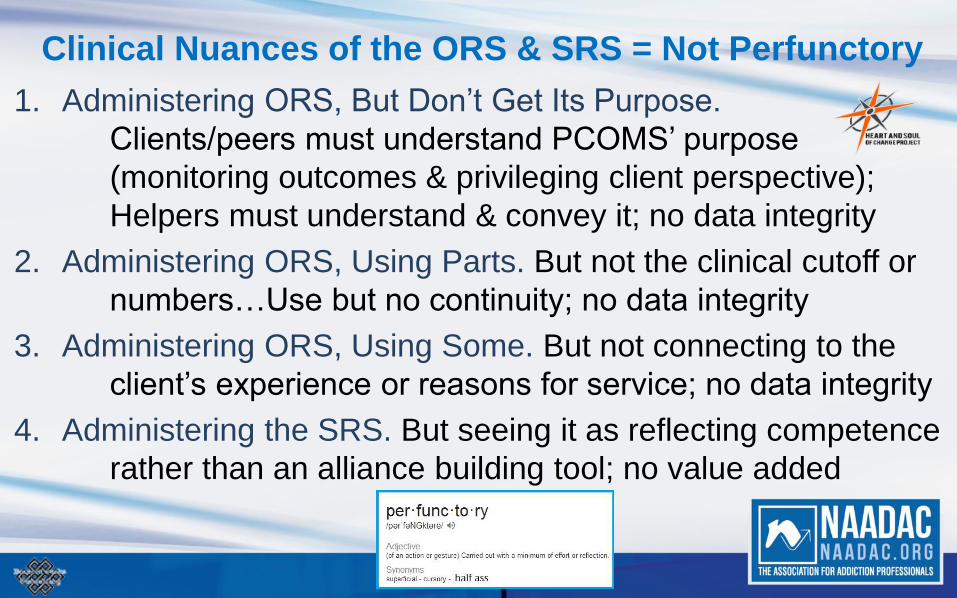
1. Administering ORS, But Don’t Get Its Purpose.
Clients/peers must understand PCOMS’ purpose
(monitoring outcomes & privileging client perspective);
Helpers must understand & convey it; no data integrity
2. Administering ORS, Using Parts. But not the clinical cutoff or
numbers…Use but no continuity; no data integrity
3. Administering ORS, Using Some. But not connecting to the
client’s experience or reasons for service; no data integrity
4. Administering the SRS. But seeing it as reflecting competence
rather than an alliance building tool; no value added
Clinical Nuances of the ORS & SRS = Not Perfunctory

1. Start by looking at all client/peer graphs or lists of ORS scores.
Job One: ensure valid use of the measures & data integrity
2. Spend the most time on at-risk clients/peers: shape discussion
and brainstorms options; look for over-utilization
3. Review stats & Appreciative Inquiry:
a. What’s working
b. Opportunities to improve
c. Ways to improve; Encourage reflection, journaling & action
4. Mentor for skill building, client/peer teaching, & ongoing reflection
Appreciative Performance Support/Clinical Supervision: Four steps for currently experienced and cumulative career growth
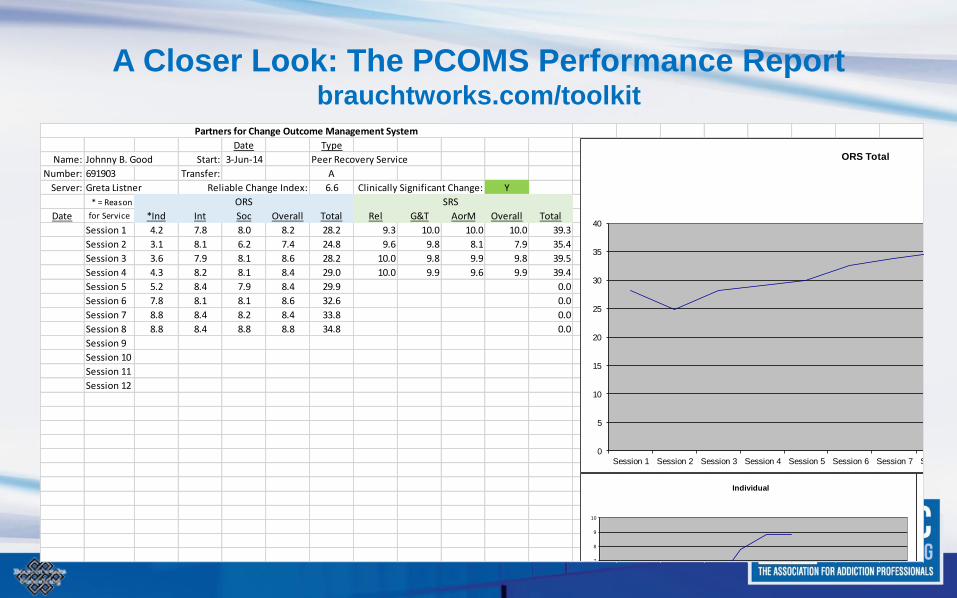
A Closer Look: The PCOMS Performance Reportbrauchtworks.com/toolkit
Date Type
Name: Johnny B. Good Start: 3-Jun-14 Peer Recovery Service
Number: 691903 Transfer: A
Server: Greta Listner Reliable Change Index: 6.6 Clinically Significant Change: Y
* = Reason ORS SRS
Date for Service *Ind Int Soc Overall Total Rel G&T AorM Overall Total
Session 1 4.2 7.8 8.0 8.2 28.2 9.3 10.0 10.0 10.0 39.3
Session 2 3.1 8.1 6.2 7.4 24.8 9.6 9.8 8.1 7.9 35.4
Session 3 3.6 7.9 8.1 8.6 28.2 10.0 9.8 9.9 9.8 39.5
Session 4 4.3 8.2 8.1 8.4 29.0 10.0 9.9 9.6 9.9 39.4
Session 5 5.2 8.4 7.9 8.4 29.9 0.0
Session 6 7.8 8.1 8.1 8.6 32.6 0.0
Session 7 8.8 8.4 8.2 8.4 33.8 0.0
Session 8 8.8 8.4 8.8 8.8 34.8 0.0
Session 9
Session 10
Session 11
Session 12
Partners for Change Outcome Management System
0
5
10
15
20
25
30
35
40
Session 1 Session 2 Session 3 Session 4 Session 5 Session 6 Session 7 Session 8
ORS Total
7
8
9
10
Individual
10

A Closer Look: The PCOMS Performance Report (cont.)brauchtworks.com/toolkit
Helper: Greta Listner Program: Peer Recovery Service Start Date: Organization:
Number Name
Entry
Program ID #
(A)ctive
(P)lanned Transfer
(U)nplanned Transfer
Start
Date
End
Date
ORS
Initial
ORS
Last
# of
Sessions
Raw
Change
Reliable Change
Index (6+ points)
Clinically Significant
Change (RCI & 25+)
SRS
Last
1 Johnny B. Good PRS 691903 A 7-Jul-14 15.1 23.0 3 7.9 Y N 39.0
2 Noe Nohow CRU 328945 P 2-Sep-14 11-Mar-14 18.6 23.0 5 4.4 N N 40.0
3 Willit Help WAC 563247 P 10-Mar-14 19-May-14 32.5 36.3 9 3.8 N N 40.0
4 Scooby Doo PRS 123456 P 11-Jul-14 13-Sep-14 14.2 19.9 12 5.7 N N 38.7
5 Swift Taylor WAC 654321 P 14-Jan-14 28-Jan-14 36.4 32.7 2 -3.7 N N 36.4
6 Mr. T CRU 234567 P 11-Aug-14 22-Sep-14 20.3 31.9 6 11.6 Y Y 40.0
7 Elvis PRS 918273 U 8-Jan-14 13-Jan-14 11.7 34.2 2 22.5 Y Y 38.8
8 Canu Elpme CRU 453627 A 17-Jan-14 20.5 19.4 2 -1.1 N N 39.4
9 Truly Yavis PRS 564738 P 14-Feb-14 28-Mar-14 23.6 31.3 6 7.7 Y Y 39.8
10
11
12
13
14
15
16
17
18
19
20
My Effect Size Participants Average Average Average Average Planned - Met RCI Planned - Met CSC Average
0.99 Active 2 21.4 28.0 5.2 6.5 2 2 39.1
Planned 6 StandDev StandDev StandDev StandDev % Planned - Met RCI % Planned - Met CSC StandDev
Unplanned 1 8.28 6.57 3.49 7.58 33.3% 33.3% 1.15
Total 9 Highest Highest Highest Highest Unplanned - Met RCI Unplanned - Met CSC Highest
36.4 36.3 12.0 22.5 1 1 40.0
Peer Recovery Support 4 Lowest Lowest Lowest Lowest % Unplanned - Met RCI % Unplanned - Met CSC Lowest
Change R Us 3 11.7 19.4 2.0 -3.7 100.0% 100.0% 36.4
We All Change 2 Total Transfers - Met RCI Total Transfers - Met CSC
3 3
% Total Transfers -Met RCI % Total Transfers -Met CSC
42.9% 42.9%
Weeks in Service
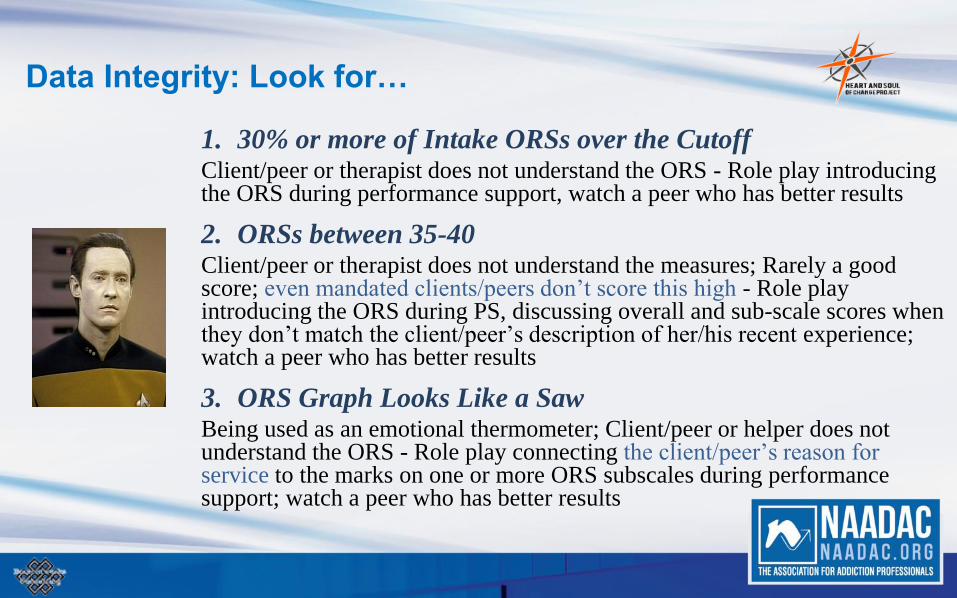
Data Integrity: Look for…
1. 30% or more of Intake ORSs over the CutoffClient/peer or therapist does not understand the ORS - Role play introducing the ORS during performance support, watch a peer who has better results
2. ORSs between 35-40Client/peer or therapist does not understand the measures; Rarely a good score; even mandated clients/peers don’t score this high - Role play introducing the ORS during PS, discussing overall and sub-scale scores when they don’t match the client/peer’s description of her/his recent experience;watch a peer who has better results
3. ORS Graph Looks Like a SawBeing used as an emotional thermometer; Client/peer or helper does not understand the ORS - Role play connecting the client/peer’s reason for service to the marks on one or more ORS subscales during performance support; watch a peer who has better results

Participating in Appreciative PCOMS Performance
Support
#1 Self-assessment, reflection and journaling that informs your
professional development plan : PCOMS Report,
Appreciative Inquiry (AI) questions:
1) What’s right with you today,
2) What could be better (improvement opportunities) &
3) What keeps you hopeful (celebrate successes)
#2 Peer support and e-Meetings: PCOMS Report & AI questions
#3 Quality improvement visits: PCOMS Report, observations,
proficiency feedback, AI questions

Typical Appreciative PCOMS Performance Support
Conversation: The longer without change, the quicker to #7
1. What does the client/peer say about goals/reason(s) for
seeking service?
2. What do the ORSs reflect about progress?
3. Is the client/peer engaged? SRSs?
4. What have you done differently?
5. What can be done differently now?
6. What other resources can be rallied?
7. Time to plan for transfer (successfully)?

Non-blaming Transfers:Warm handoff to adjunct services or planned transfers
Not dumping clients/peers
Says nothing about the helper’s
competence
Says nothing about client/peer’s
ability to change
Says everything about doing
something positive and proactive
with clients/peers who are not
benefiting

heartandsoulofchange.com


Questions?

Webinar Learning Objectives. Upon completion of this
session participants will be able to:
Explain four research-
based factors
responsible for client
change that cut across
professional disciplines
and preferred treatment
models
Assess the client’s vital
perceptions of recovery
progress and satisfaction
so that services can be
empirically tailored to the
individual’s characteristics,
circumstances, and
resources.
Use the simple yet feasible,
valid, and reliable tools to
gather practice-based
evidence of service process
and outcome effectiveness.
1 32

Start
by doing what’s necessary,
then do what’s possible,
and suddenly you are doing
the impossible.
St. Francis of Assisi

George S. Braucht, LPC & CPCS
Email: [email protected]
Website: brauchtworks.com
Brauchtworks ConsultingApplying Science to Practice
Thanks for your attention and
participation!

www.naadac.org/PCOMS-retention-
outcomes-supervision-webinar

Cost to Watch:
Free
CE Hours
Available:
2 CEs
CE Certificate for
NAADAC
Members:
Free
CE Certificate for
Non-members:
$25
To obtain a CE Certificate for the time you spent watching this
webinar:
1. Watch and listen to this entire webinar.
2. Pass the online CE quiz, which is posted at
www.naadac.org/PCOMS-retention-outcomes-
supervision-webinar
3. If applicable, submit payment for CE certificate or join
NAADAC.
4. A CE certificate will be emailed to you within 21 days of
submitting the quiz.
CE Certificate
March 22, 2017 April 26, 2017
April 12, 2017
Effective Screening for
Gambling Disorder
by Loreen Rugle, PhD, ICGC II
May 10, 2017
Upcoming Webinars
www.naadac.org/webinars
Motivating the Troops: Creating an
Advocacy Mechanism
by Sherri Layton, MBA, LCDC, CCS
Developmental Trauma Disorderby F Malcolm Horn, LCSW, MAC
Six Types of Sex Use Disorder
by Douglass Weiss, PhD

www.naadac.org/webinars
Free CEs for
Members
Levels:
Professional
Associate
Student
www.naadac.org/
join
Over 75 CEs of free educational
webinars are available. Education
credits are FREE for NAADAC
members.
WEBINAR SERIES
In each issue of Advances in
Addiction & Recovery, NAADAC's
magazine, one article is eligible for
CEs.
MAGAZINE ARTICLES
NAADAC offers face-to-face
seminars of varying lengths in the
U.S. and abroad.
FACE-TO-FACE SEMINARS
Earn CEs at home and at your own
pace (includes study guide and
online examination).
INDEPENDENT STUDY
COURSES
NAADAC Annual Conference,
September 22-26, 2017, Denver, CO
CONFERENCES
Demonstrate advanced education
in diverse topics with the NAADAC
Certificate Programs.
CERTIFICATE PROGRAMS

Contact Us!
NAADAC
44 Canal Center Plaza, Suite 301
Alexandria, VA 22314
phone: 703.741.7686 / 800.548.0497
fax: 703.741.7698 / 800.377.1136
www.naadac.org
NAADACorg
Naadac
NAADAC







