
“Indicazione, efficacia e sicurezzadello switching tra terapie antiaggreganti piastiniche”
Guido ParodiDipartimento CardioToracoVascolare
Azienda Ospedaliero-Universitaria CareggiFirenze
CardioLuccaLucca, 28 Novembre 2014
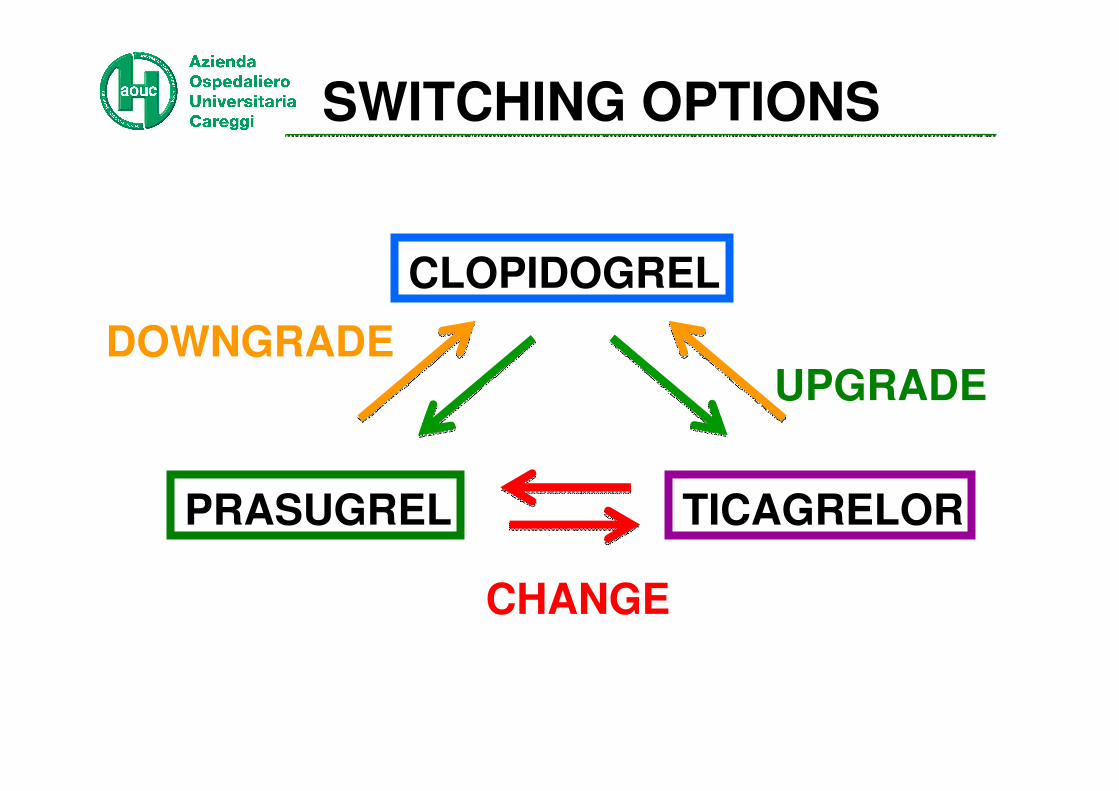
CLOPIDOGREL
PRASUGREL TICAGRELOR
UPGRADEDOWNGRADE
CHANGE
SWITCHING OPTIONS

CLOPIDOGREL
PRASUGREL TICAGRELOR
UPGRADE
SWITCHING OPTIONS
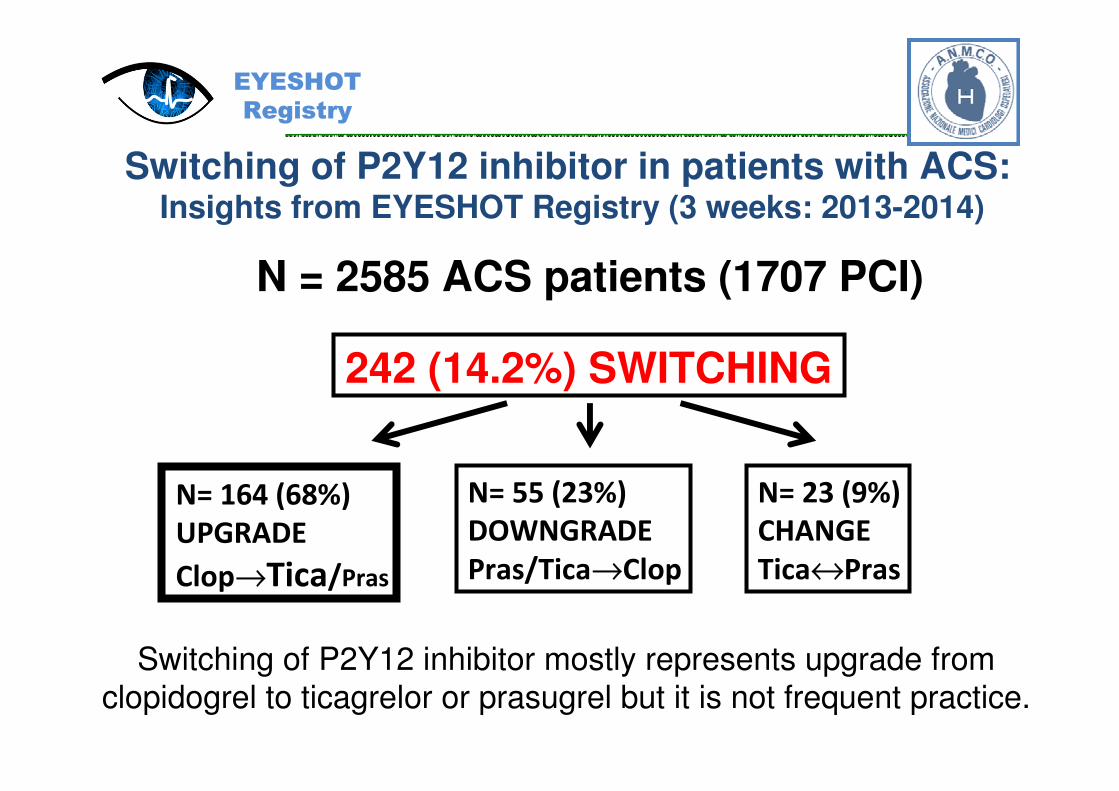
Switching of P2Y12 inhibitor in patients with ACS:Insights from EYESHOT Registry (3 weeks: 2013-2014)
N = 2585 ACS patients (1707 PCI)
N= 164 (68%)
UPGRADE
Clop→Tica/Pras
N= 55 (23%)
DOWNGRADE
Pras/Tica→Clop
N= 23 (9%)
CHANGE
Tica↔Pras
Switching of P2Y12 inhibitor mostly represents upgrade from clopidogrel to ticagrelor or prasugrel but it is not frequent practice.
242 (14.2%) SWITCHING
EYESHOT
Registry
%
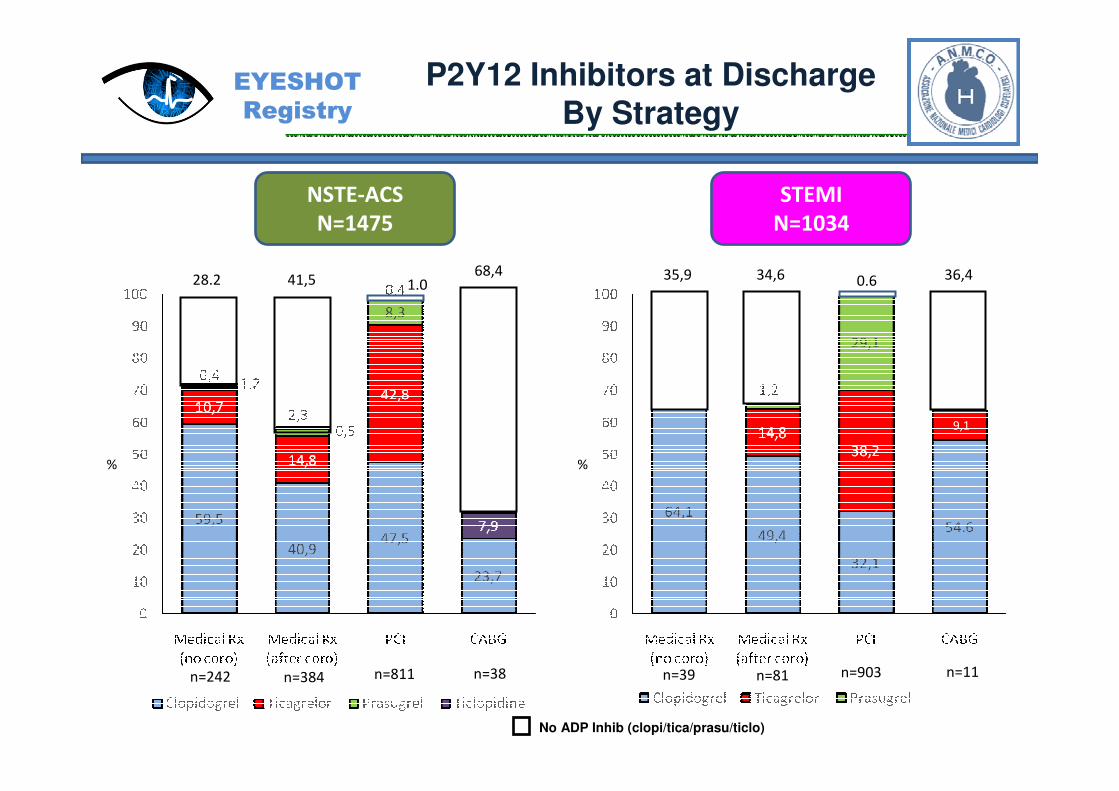
NSTE-ACS
N=1475
P2Y12 Inhibitors at DischargeBy Strategy
%
STEMI
N=1034
9,1
n=39 n=81 n=903 n=11n=242 n=384 n=811 n=38
No ADP Inhib (clopi/tica/prasu/ticlo)
28.2 41,568,4
1.035,9 34,6 36,40.6
EYESHOT
Registry
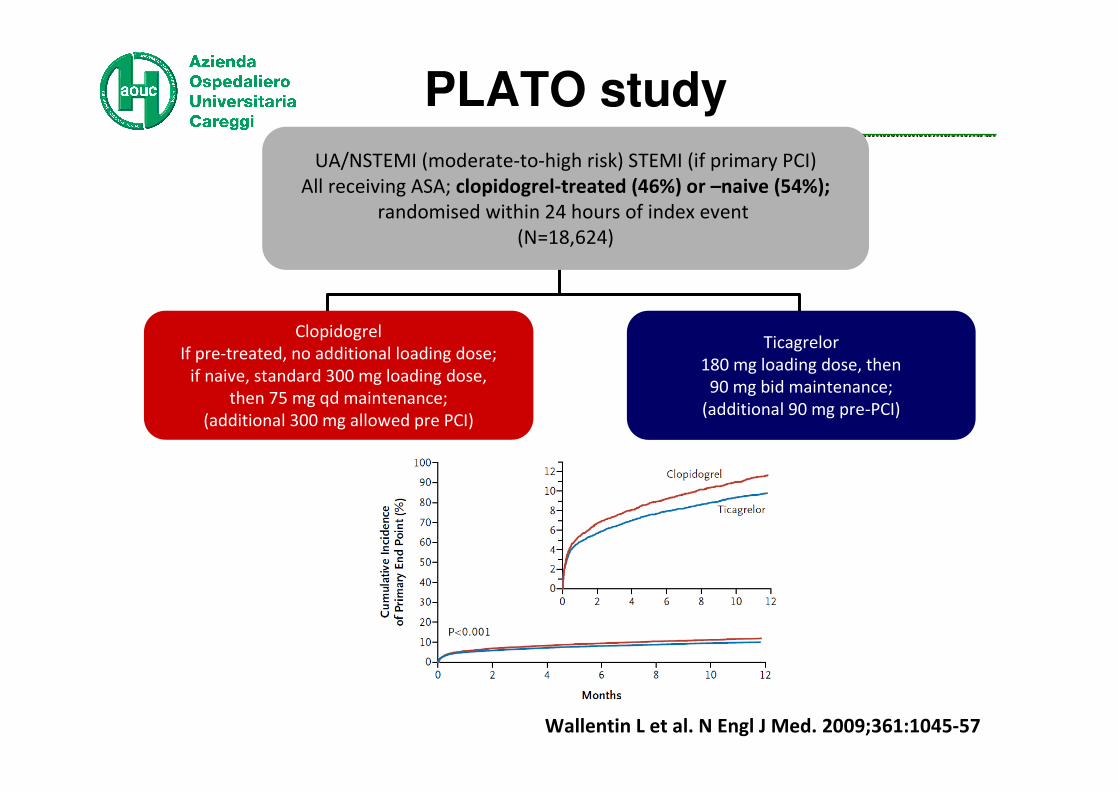
PLATO study
Clopidogrel
If pre-treated, no additional loading dose;
if naive, standard 300 mg loading dose,
then 75 mg qd maintenance;
(additional 300 mg allowed pre PCI)
Ticagrelor
180 mg loading dose, then
90 mg bid maintenance;
(additional 90 mg pre-PCI)
UA/NSTEMI (moderate-to-high risk) STEMI (if primary PCI)
All receiving ASA; clopidogrel-treated (46%) or –naive (54%);
randomised within 24 hours of index event
(N=18,624)
Wallentin L et al. N Engl J Med. 2009;361:1045-57
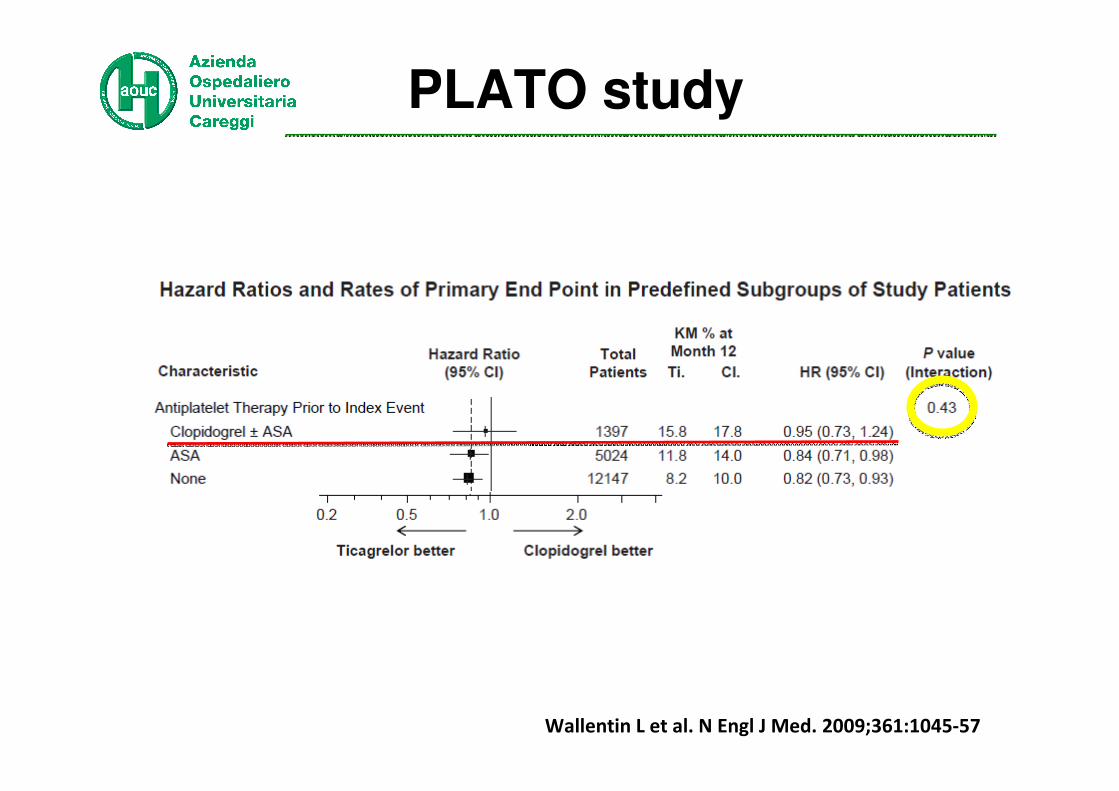
PLATO study
Wallentin L et al. N Engl J Med. 2009;361:1045-57

Gurbel PA et al. Circulation 2010:121:1188-1199
The RESPOND StudyInhibition of platelet aggregation in clopidogrel responders
(n=57 stable CAD patients)

Brar SS et al. J Am Coll Cardiol 2011;58:1945-54

card
iov
asc
ula
r d
ea
th,
no
nfa
tal
my
oca
rdia
l in
farc
tio
n,
or
stro
ke
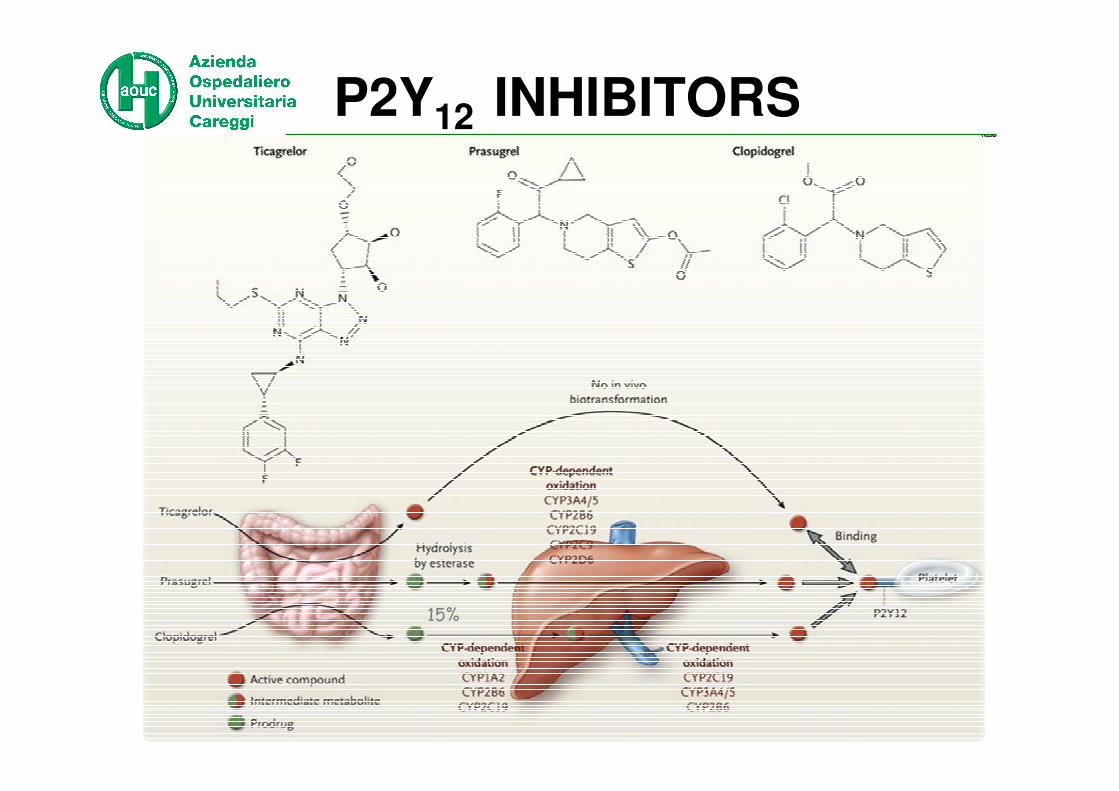
15%
P2Y12 INHIBITORS
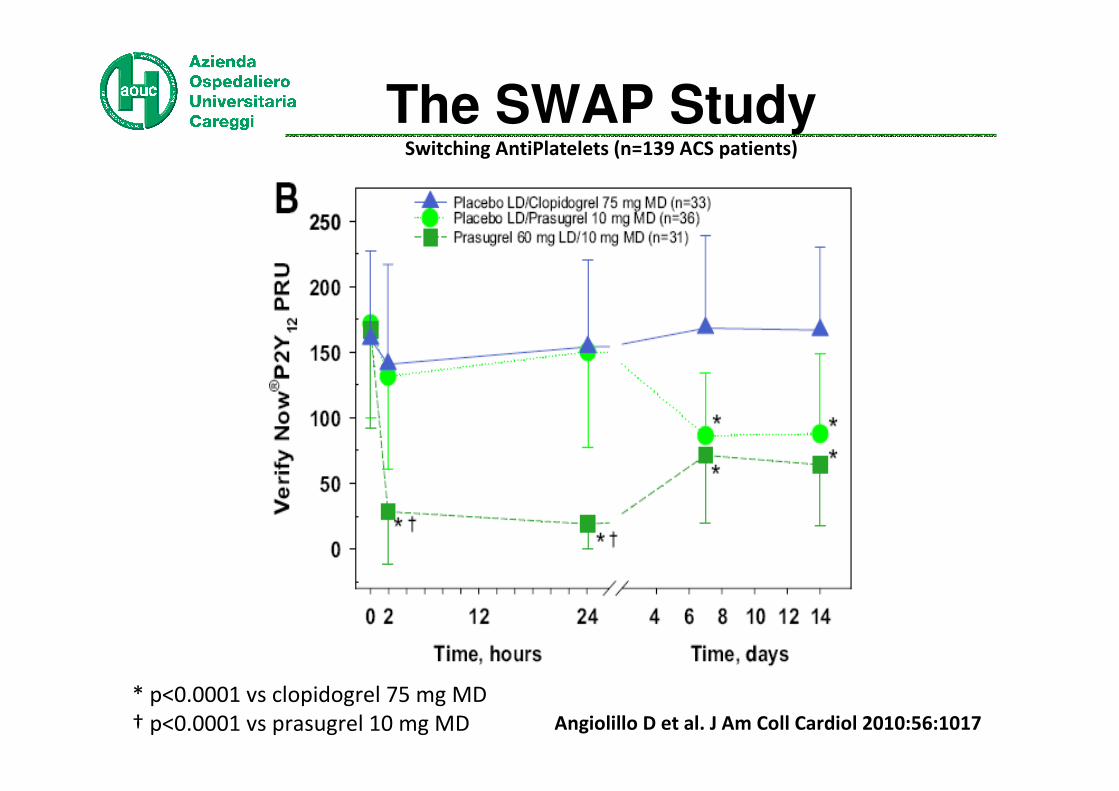
Angiolillo D et al. J Am Coll Cardiol 2010:56:1017
The SWAP StudySwitching AntiPlatelets (n=139 ACS patients)
* p<0.0001 vs clopidogrel 75 mg MD
† p<0.0001 vs prasugrel 10 mg MD

Loh JP. Am J Cardiol 2013
Previous clopidogrel load = 90 pts
Prasugrel only load=516 pts
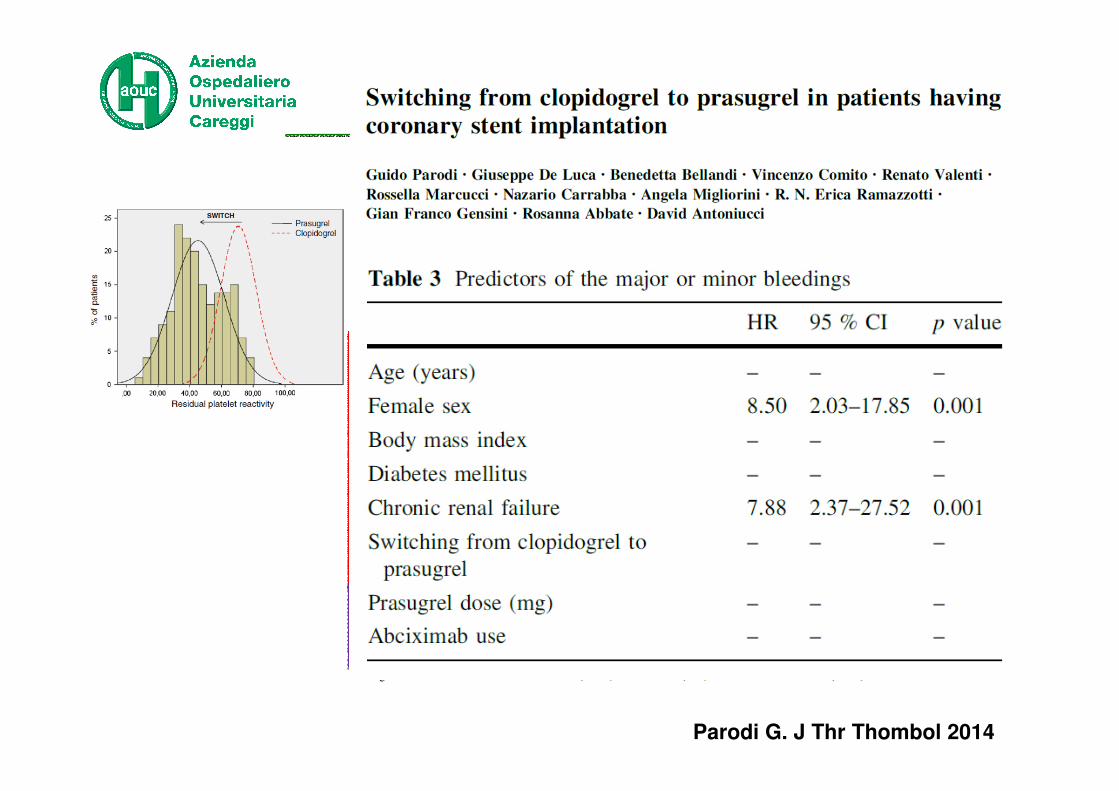
Parodi G. J Thr Thombol 2014
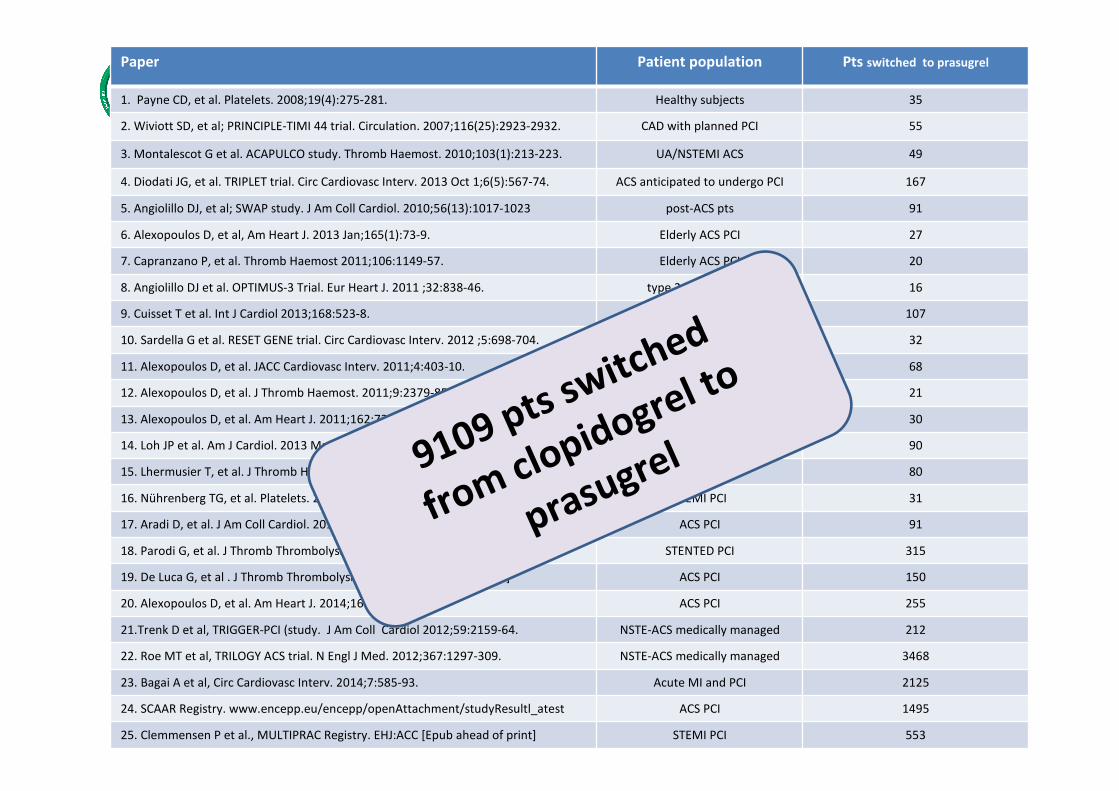
Paper Patient population Pts switched to prasugrel
1. Payne CD, et al. Platelets. 2008;19(4):275-281. Healthy subjects 35
2. Wiviott SD, et al; PRINCIPLE-TIMI 44 trial. Circulation. 2007;116(25):2923-2932. CAD with planned PCI 55
3. Montalescot G et al. ACAPULCO study. Thromb Haemost. 2010;103(1):213-223. UA/NSTEMI ACS 49
4. Diodati JG, et al. TRIPLET trial. Circ Cardiovasc Interv. 2013 Oct 1;6(5):567-74. ACS anticipated to undergo PCI 167
5. Angiolillo DJ, et al; SWAP study. J Am Coll Cardiol. 2010;56(13):1017-1023 post-ACS pts 91
6. Alexopoulos D, et al, Am Heart J. 2013 Jan;165(1):73-9. Elderly ACS PCI 27
7. Capranzano P, et al. Thromb Haemost 2011;106:1149-57. Elderly ACS PCI 20
8. Angiolillo DJ et al. OPTIMUS-3 Trial. Eur Heart J. 2011 ;32:838-46. type 2 DM and CAD 16
9. Cuisset T et al. Int J Cardiol 2013;168:523-8. diabetic PCI patients 107
10. Sardella G et al. RESET GENE trial. Circ Cardiovasc Interv. 2012 ;5:698-704. stable patients undergoing PCI 32
11. Alexopoulos D, et al. JACC Cardiovasc Interv. 2011;4:403-10. PCI w stent 68
12. Alexopoulos D, et al. J Thromb Haemost. 2011;9:2379-85. chronic HD with CAD 21
13. Alexopoulos D, et al. Am Heart J. 2011;162:733-9. Stable CAD, 87% undergoing PCI 30
14. Loh JP et al. Am J Cardiol. 2013 Mar 15;111(6):841-5. ACS PCI 90
15. Lhermusier T, et al. J Thromb Haemost. 2012;10:1946-9. ACS PCI 80
16. Nührenberg TG, et al. Platelets. 2013;24:549-53. STEMI PCI 31
17. Aradi D, et al. J Am Coll Cardiol. 2014;63:1061-70. ACS PCI 91
18. Parodi G, et al. J Thromb Thrombolysis. 2014. [Epub ahead of print] STENTED PCI 315
19. De Luca G, et al . J Thromb Thrombolysis. 2014 [Epub ahead of print] ACS PCI 150
20. Alexopoulos D, et al. Am Heart J. 2014;167:68-76.e2. ACS PCI 255
21.Trenk D et al, TRIGGER-PCI (study. J Am Coll Cardiol 2012;59:2159-64. NSTE-ACS medically managed 212
22. Roe MT et al, TRILOGY ACS trial. N Engl J Med. 2012;367:1297-309. NSTE-ACS medically managed 3468
23. Bagai A et al, Circ Cardiovasc Interv. 2014;7:585-93. Acute MI and PCI 2125
24. SCAAR Registry. www.encepp.eu/encepp/openAttachment/studyResultl_atest ACS PCI 1495
25. Clemmensen P et al., MULTIPRAC Registry. EHJ:ACC [Epub ahead of print] STEMI PCI 553
9109 pts switched
from clopidogrel to
prasugrel
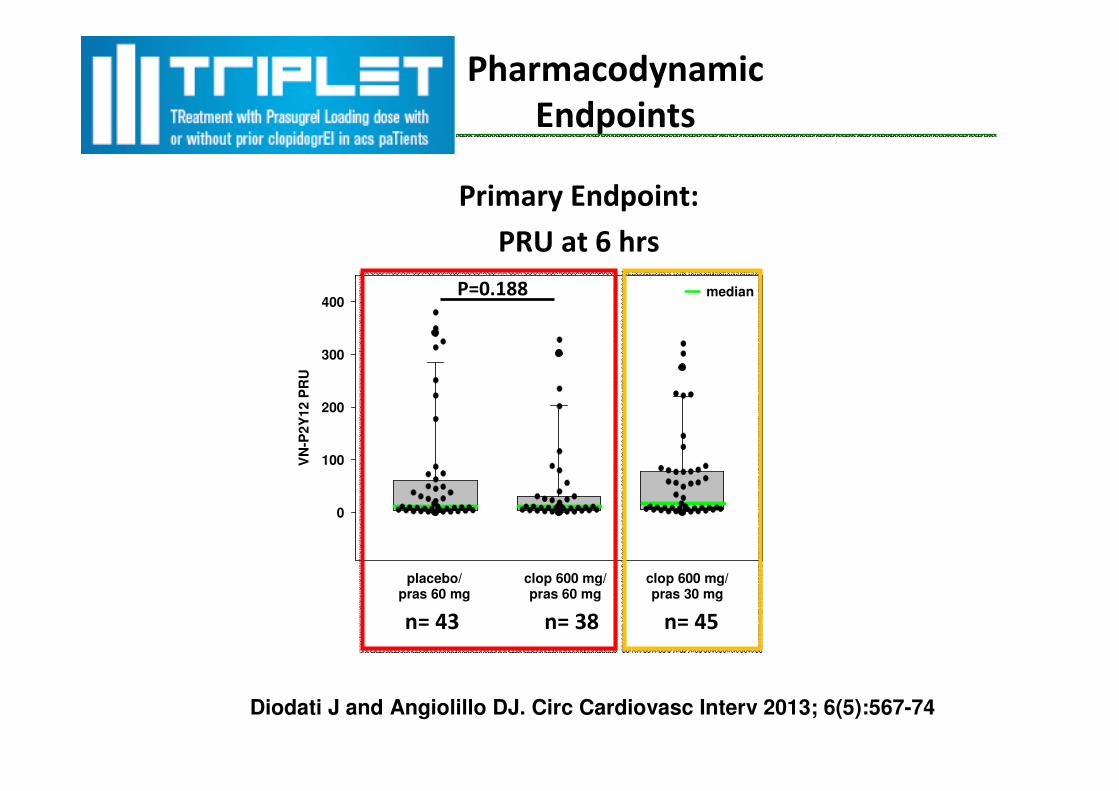
VN
-P2
Y12 P
RU
0
100
200
300
400
clop 600 mg/pras 60 mg
clop 600 mg/pras 30 mg
median
placebo/pras 60 mg
Pharmacodynamic
Endpoints
Primary Endpoint:
PRU at 6 hrs
n= 43 n= 38 n= 45
P=0.188
Diodati J and Angiolillo DJ. Circ Cardiovasc Interv 2013; 6(5):567-74
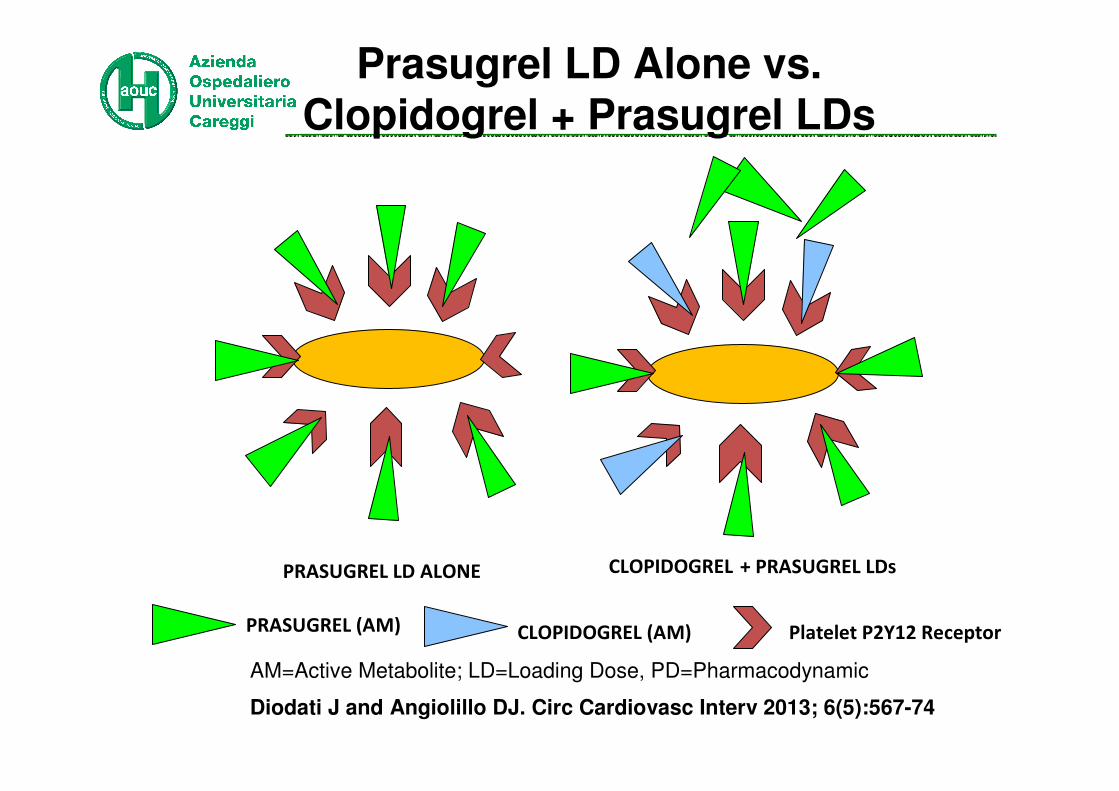
Prasugrel LD Alone vs. Clopidogrel + Prasugrel LDs
PRASUGREL (AM) CLOPIDOGREL (AM)
PRASUGREL LD ALONE CLOPIDOGREL + PRASUGREL LDs
Platelet P2Y12 Receptor
AM=Active Metabolite; LD=Loading Dose, PD=Pharmacodynamic
Diodati J and Angiolillo DJ. Circ Cardiovasc Interv 2013; 6(5):567-74

2011

CLOPIDOGREL
PRASUGREL TICAGRELOR
DOWNGRADE
SWITCHING OPTIONS

BackgroundBackground
Kerneis M et al. JACC Cardiovac Interventions 2013
1) Increase of platelet aggregation (10-fold)
2) Unmask poor responder to clopidogrel
3) Reduce minor bleeding
DOWNGRADINGPrasugrel → Clopidogrel
CLOPIDOGREL
PRASUGREL TICAGRELOR
CHANGE
SWITCHING OPTIONS

0
50
100
150
200
250
300
350
Prasugrel 60 mg LD/
10 mg MDPrasugrel 10 mg MD
Prasugrel Total
Ticagrelor
Pre-Run-In
Baseline
Pre-
Rand.
Baseline
2 hrs Post
First
Rand.
Dose
4 hrs Post
First
Rand.
Dose
24 hrs Post
First
Rand.
Dose
48 hrs Post
First
Rand.
Dose
7 Days Post
First
Rand.
Dose
230208
PR
U (
me
an
±S
D)
SWAP 2Ticagrelor → Prasugrel
Angiolillo D. J Am Coll Cardiol 2014
Sudden cardiac death of a patient with LM stent 48 hours after switching from Ticagrelor to Prasugrel without loading dose.
Parodi G and Storey RF. Eur Heart J: ACC 2014; Sep 29

Was identical characteristics, frequency and severity of DYSPNOEA episodes present before starting TICAGRELOR?
Spontaneous DYSPNOEA
improvement within 3 days
YES
FOLLOW-UP
NO
Can the patient tolerate the DYSPNOEA
with appropriate reassurance and counselling?
YESNO
Consider switching to prasugrel (or clopidogrel if
prasugrel is contraindicated) using a full loading dose at least 24 hours from the last ticagrelor intake
Look for an alternative
cause
YES Is the DYSPNOEA associated with orthopnoea, paroxysmal nocturnal dyspnoea
or chest tightness or pain, related to exertion or limiting exercise capacity and/or is there an identifiable cause on physical examination?
NO
YES Possible ticagrelor-
related DYSPNOEA
NO
Parodi G and Storey RF. Eur Heart J: ACC 2014; Sep 29
CONCLUSIONS
1) Switching from Clopidogrel to
Ticagrelor or Prasugrel reduces platelet reactivity
3) Whether to switch depend on risk profile (anatomy)
4) How to switch: starting with a loading dose
5) Downgrading to clopidogrel should be
considered only in the case of relevant side-
effect or of the need for oral anticoagulation
6) A warning regarding switching from ticagrelor to
prasugrel (or clopidogrel)!
MOST FREQUENT SWITCH







