
INSULIN THERAPY IN HOSPITALIZED
Dr. Widyati, MClin Pharm, AptFarmasis Klinik RSAL dr Ramelan
Dosen MFK Ubaya
2
PERSONAL DETAILS
• Sarjana Farmasi 1989 (UNPAD)
• Apoteker 1991 (UI)
• Observasi Hospital Pharmacy di 12 RS Australia(1995)
• MClin Pharm 1999(University of Queensland-Ausy)
• Dr: 2013 (Universitas Gajah Mada)
• Practising clinical pharmacy in hospital (Critical Care)
• Teach clinical pharmacy in UGM, Ubaya
• Org: Ketua Bidang Farklin HISFARSI, Tim Ahli ESO Badan POM
• Married, two children
• International Award: FIP International Travel Award (California,2003), ILAE Travel Award (Washington,2013)

Macam Insulin Regimen
SSI
ODI
MDIIIT
IV Insulin
Terapi Insulin Pada HOSPITALIZED
Acute IllnessChronic Illness
Critically Ill
PerioperativeDrug-induced hyperglycemi
a
Background
• Hyperglycemia frequently occurs with acute medical illness, and has been linked to increased morbidity and mortality in critically ill patients.
• Insulin therapy in hospitalized patients can be troublesome. The stress of the acute illness tends to raise blood glucose concentrations.
• Meanwhile on the other hand, the anorexia that often accompanies illness or the need for fasting before a procedure tends to do the opposite. Because the net effect of these countervailing forces is not easily predictable in a given patient, the target blood glucose concentration is usually higher than when the patient is stable.

DM in Acute Events
6
SEPSIS
ACS
STROKE


Stress Hyperglycemia
• SH develops principally through a combination of (1) increased gluconeogenesis relative to glucose clearance and (2) development of insulin resistance affecting cellular uptake of glucose (Mechanick JI, 2006)
• Additionally, proinflammatory cytokines may directly inhibit insulin secretion by pancreatic β cells through stimulation of α-adrenergic receptors (Mizock BA,2001)

Penggunaan Insulin pada Pasien DM Rawat Inap
Acute Illness
• Severe Infection
• Acute Stroke
• ACS
• KAD
• HHS
Chronic Illness
• DM Hiperglikemia
• DM dengan infeksi
• DM dengan intercurrent illness
• DM dengan kehamilan
ACUTE CASES
o Decompensation due to an intercurrent event (eg, infection, acute injury, stress)
o Severe hyperglycemia with ketonemia or ketonuria (Komplikasi Akut)
o Acute events: Acute Coronary Syndrome (ACS), Stroke
o Upcoming surgery o Allergy or other serious reaction to oral agents

The importance of hyperglycemia
• Acute illness: A strong association between hyperglycemia and poor clinical outcome, such as mortality, morbidity, length of stay, infections, and overall complications.(Umpierrez et
al,2002)
• Non-Critical illness: Hyperglycemia is associated with poor hospital outcomes, including prolonged hospital stay, infections, disability after hospital discharge, and death.

Manajemen Inpatient Hyperglycemia
• Dipersulit dengan status nutrisi (ie, nothing by mouth, enteral tube feeding), drug-induced, perubahan kondisi klinis , dan lemahnya koordinasi antara coordination of BG testing with prandial insulin administration.
• ASHP guidelines for safe use of insulin in hospitals recommend a multidisciplinary team approach, institutions develop standardized procedures for BG management
• Subcutaneous insulin therapy should be comprised of 3 components: basal (daily or twice-daily injections of long-acting insulin), prandial or nutritional (injections of rapid-acting insulin before meals), and correction insulin

Dosis Insulin
TDD Estimation Patient Characteristics
0.3 units/kg body weight Underweight
• Older age
• Hemodialysis
0.4 units/kg body weight Normal weight
0.5 units/kg body weight Overweight
≥ 0.6 units/kg body weight Obese
• Insulin resistant
• Glucocorticoids

Perioperative
• Standards for perioperative care include the following:
• Target glucose range for the perioperative period should be 80–180 mg/dL (4.4–10.0 mmol/L).
• Preoperative risk assessment for patients at high risk for ischemic heart disease and those with autonomic neuropathy or renal failure.
• The morning of surgery or procedure, hold any oral hypoglycemic agents and give half of NPH dose or full doses of a long-acting analog or pump basal insulin.
• Monitor blood glucose every 4–6 h while NPO and dose with short-acting insulin as needed.
Insulin pada Non-Critically Ill
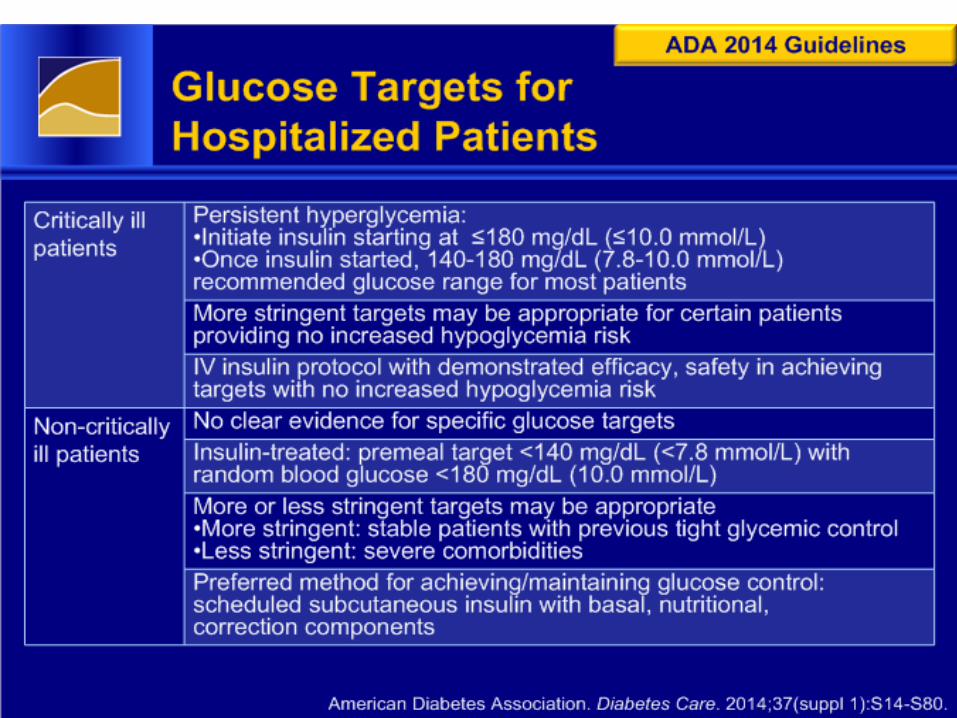
• A basal plus bolus correction insulin regimen is the preferred treatment for non-critically ill patients with poor oral intake or those who are taking nothing by mouth.
• An insulin regimen with basal, nutritional, and correction components is the preferred treatment for patients with good nutritional intake. A
• The sole use of sliding scale insulin in the inpatient hospital setting is strongly discouraged.A
( Diabetes Care 2016)

Insulin Therapy in the Non–Critical Care Setting
• The practice of discontinuing oral diabetes medications and/or insulin therapy and starting sliding scale insulin (SSI) results in undesirable levels of hypoglycemia and hyperglycemia (Hirsch,2009)

Diabetes Care 2016
• Outside of critical care units, scheduled subcutaneous insulin injections should align with meals and bedtime or every 4–6 h if no meals or if continuous enteral/ parenteral therapy is used
18

Critically Ill
• Insulin therapy should be initiated for treatment of persistent hyperglycemia ≥180 mg/dL (10 mmol/L).
• Target glucose range of 140 to 180 mg/dL (7.8 to 10 mmol/L) (A) ( ADA, 2011)
• Severe hypoglycemia (< 40 mg/dl) during critical illness should be avoided because it has been associated with increased mortality. (NICE-SUGAR, 2009)

KAD & HHD
• Insulin Therapy• Bolus of regular insulin at 0.15 units/kg body weight,
followed by a continuous infusion of regular insulin at a dose of 0.1 unit/kg/jam (5 to 7 units per hour in adults)
• If plasma glucose does not fall by 50 mg/dL from the initial value in the first hour, check hydration status; if acceptable, the insulin infusion may be doubled every hour until a steady glucose decline between 50 and 75 mg/hour
• Frequent laboratory and blood gas analyses are obtained to ensure ongoing resolution of metabolic acidosis

KAD
• “Maintenance” IV fluid at a rate of 2000 - 2400 cc/m2/day consists of 2/3 NS (0.66%) or NS– 5% Dextrose is added to IVF when blood glucose is ~ 300
mg/dL
– 10% Dextrose is added when blood glucose is ~ 200 mg/dL
• Insulin is used to treat acidosis, not hyperglycemia
– insulin should never be stopped if ongoing acidosis persists
• When the acidosis is corrected, the continuous insulin infusion may be discontinued and subcutaneous insulin initiated
• With this regimen, DKA is usually fully corrected in 36 to 48 hours

INSULIN USE IN CHRONIC CARE
INSULIN USE IN DM TYPE 2
• Indication: when glucose control can no longer be maintained with oral combination
• Insulin therapy overcome insulin resistance and provide adequate insulin even in the presence of islet beta-cell dysfunction
• Indications for insulin therapy of type 2 diabetes :
o Hyperglycemia despite maximum doses of oral agents
o Acute Cases
o Uncontrolled weight loss
o Pregnancy
o Renal disease
o A preference for insulin therapy by the patient or physician.
23

Kombinasi OAD-Insulin
• Setelah kombinasi OAD gagal mengontrol gula
Kombinasi ↓FPG (mg/dl) ↓HbA1c (%)
SU+ insulin 60-80 0,5-1.8
Metformin+ins 60-80 1,7-2,5
Acarbose+ins 0-16 0,4-0,5
Glimepiride+ins 110 2,2
Pioglitazone+ins 35-49 0,7-1,0 24

PENETAPAN DOSIS INSULIN

Dosis Insulin
TDD Estimation Patient Characteristics
0.3 units/kg body weight Underweight
• Older age
• Hemodialysis
0.4 units/kg body weight Normal weight
0.5 units/kg body weight Overweight
≥ 0.6 units/kg body weight Obese
• Insulin resistant
• Glucocorticoids

Estimating Total Daily Insulin Requirement
Type 1 diabetes
Initial dose 0.3–0.5 unit/kg
Honeymoon phase 0.2–0.5 unit/kg
With ketosis, during illness, during growth 1.0–1.5 units/kg
Type 2 diabetes
With insulin resistance 0.7–1.5 units/kg
Estimating Basal Insulin Requirements
Basal requirements vary throughout the day,approximately 50% of total daily insulin needs. The basal requirement also is influenced by the presence of endogenous insulin, the degree of insulin resistance, and body weight.

Targets
• A1c ≤ 6,5 %
• FPG/SMBG ≤ 110mg/dl
• 2 hr PPG/SMBG ≤140-180 mg/dl
Treatment Naive
• Symptomatic
• FPG ≥260 mg/dl
• A1c ≥10%, ketoacidosis, recent rapid weight loss
• Pilihan:
• 1. Once-daily Insulin
• 2. Multi-dose insulin
• 3. Intensive insulin management
Oral Agent Failure
• 7,0 %> A1c < 8,5%
• Pilihan:
• 1. Once-daily Insulin
• 2. Multi-dose insulin
• 3. Intensive insulin management

Oral Agent Failure
• A1c > 8,5%
• Pilihan:
• 1. Multi-dose insulin
• 2. Intensive insulin management
• 3. Once –daily insulin

Once-Daily Insulin
• At bedtime : NPH or Long-acting insulin
• Before supper: short-acting insulin or premix 70/30
• Dosis awal : 0,1-0,25 U/kg or 6-10 U untukmanula kurus
• Naikkan dosis setiap 2-3 hari.
• Titration schedule: >180mg/dl – 6 unit
• 141-180mg/dl – 4 unit
• 121-140mg/dl -2 unit
Multi –Dose Insulin
• 2 x suntik : NPH + Short acting insulin
• Or premix 70/30
• 3 x suntik (if nocturnal hypoglycemia): Short acting insulin before breakfast and before supper sliding scale + NPH before breakfast and bedtime or Long acting insulin
• Starting dose: 0,3-0,5 unit/kg

Intensive Insulin Management
• 1:1 basal:bolus
• Basal :NPH before breakfast, before supper or bedtime x 2 or Long acting Insulin
• Bolus: Short acting insulin at each meal
• Starting dose: 0,3-0,5 U/kg

Drug-induced Hyperglycemia

Glucocorticoids
• Mechanism: primarily by inhibiting glucose uptake into muscle.
• Postprandial glucose levels are generally most affected
• Patients who are treated with a basal/bolus regimen will probably require a higher percentage of their TDD as bolus insulin while on glucocorticoids.
• It is important to reduce insulin doses as glucocorticoids are tapered to avoid hypoglycemia.
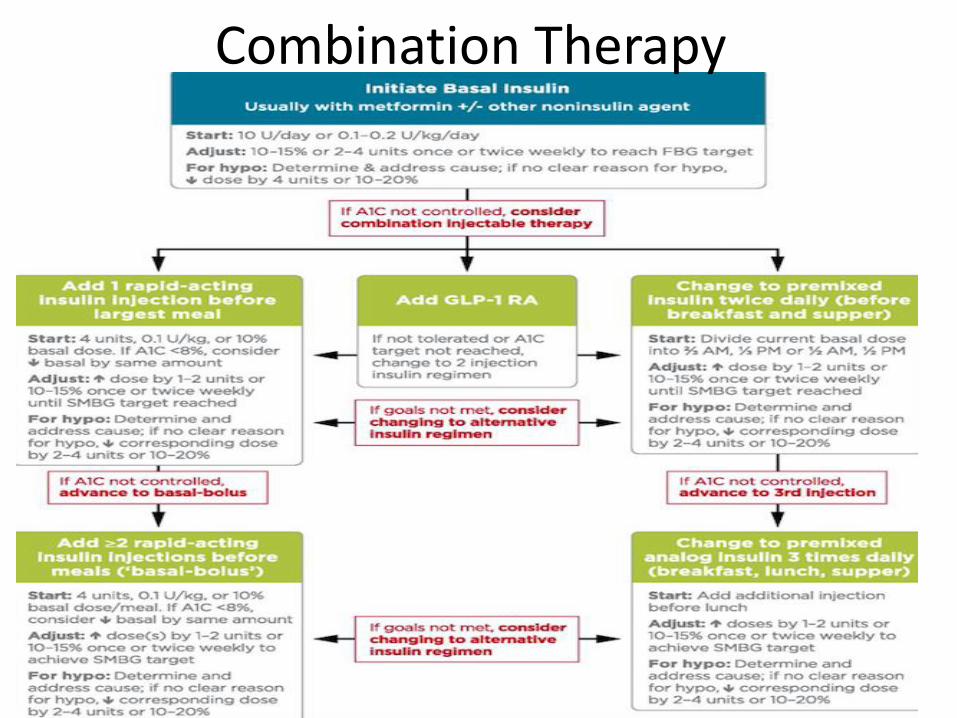
Combination Therapy
Kasus 1
• Tn HM 58th 160cm 85kg, MRS karena akanmenjalani ops katarak. Pada saat MRS hasilpemeriksaan gula puasa 216mg/dl, GD 2jamPP 234mg/dl. Menurut pengakuan Tn HM memang memiliki riwayat DM, namun tidakkontrol rutin, obatpun tidak rutin dan lebihsering meminum Glibenklamide.
Kasus 2
• Tn Y, 46th 167cm, 70kg, MRS dengan keluhanmual muntah. Pada pemeriksaan gula puasa di lab luar dijumpai GDP 253mg/dl; 2jPP 315 mg/dl. Pasien mengaku memiliki riwayat DM sudah lima tahunan dengan obatGlibenklamide 1-1-0 dan metformin 3x500mg.
• Bagaimana Pharm care untuk kasus ini?

Kasus 3
• Tn K 59th, 172cm 75kg, MRS dengan keluhankencing tidak lancar, disertai rasa panas dannyeri pada saat kencing. Pasien mengakumemiliki DM sudah 8tahun dan masih minumGliklazide 1-1-0 dan Metformin 3 x 850mg. Hasil lab: GDP 265mg/dl; 2JPP 168mg/dl; Leukosit (N), Leukosuria(+). Hasil observasiTTV TD 140/90; Temp (N). Bagaimana PharmCare pada kasus ini

Kasus 4
• Tn KP 62th, 161cm, 59kg MRS dengandiagnosa stroke infark di hemisphere kananyang luas. Hasil Lab GDP 154mg/dl sehinggadiberikan 3 x 4U s.c., namun 2 hari kemudianpasien kejang dan hasil GDP 189mg/dl. Pengakuan keluarga pasien hanya memakanmakanan RS. Bagaimana denganpenatalaksanaan DM?
Critically Ill
• Tn HO 64th, MRS dengan Stroke infark di hemisfer kiri yang luas. Hari kelima muncul problem medik baru yaitu pneumonia yang membuat pasien sangat sesak dan memerlukan ventilator (hari ke-9), sehingga dikirim ke ICU. GDA pada hari tersebut 346mg/dl, GCS 3-2-4. Bagaimana terapi insulin diberikan?

Online ResourcesAmerican Diabetes Association: www.ada.org
Diabetes UK:www.diabetes.org.uk.
National Diabetes Education Intiative: http://www.ndei.org







