
7/15/2015
1
Managing the Patient with Congestive Heart Failure
Javier Jimenez MD PhD FACCDirector, Advanced Heart Failure and
Pulmonary HypertensionMiami Cardiac & Vascular Institute
South Miami Hospital
Speaker Disclosures
• I disclose that I am a Consultant for St Jude Medical.
• I disclose that I am a member of the speaker’s bureaus for Gilead, United Therapeutics, Bayer and Actelion Pharmaceuticals.
• I will not discuss off-label or unapproved usage.
2
Objectives
• Discuss common causes of Heart Failure• Review what is an appropriate evaluation
and management of a heart failure patient• Learn about new drug therapies
• Develop strategies to prevent re-hospitalizations
Stages, Phenotypes and Treatment of HF
Etiology of Cardiomyopathy
Cardiomyopathy
Ischemic Non-Ischemic
Primary Cardiomyopathy
MIXED
Dillated Cardiomyopathy
Restrictive-Non hyperthopied
ADQUIRED
Myocarditis
Takotsubo
Peripartum
GENETIC
RVD
HCM
Mytochondrial

7/15/2015
2
HypertensiveValvular
Drug related: chemo, etohNon Compaction
Amyloid, SarcoidThyroid, DMRA, Lupus
HemochromatosisTuberous Sclerodis
EsosinophylicMELAS
Diagnostic Testing
• Electrocardiography (EKG)• Echocardiography (E)
• Nuclear Imaging (NI)• Angiography (CA)
• Cardiac CT (CCT)• Cardiac MRI (MRI)• Endomyocardial Biopsy (BX)
• Laboratory testing (LAB)
Ischemic Cardiomyopathy What kind of cardiomyopathy
A-HCM NON -OBS
B-HTN CM
D-MUCHOPOLYS
C-AMYLOID
E-OXALOSIS
F-FRIEDIREICH ATX
Non CompactionCardiomyopathy Hyperthrophic Cardiomyopathy
7/15/2015
3
Cardiac Amyloidosis Arrhythmogenic Right Ventricular Cardiomyopathy
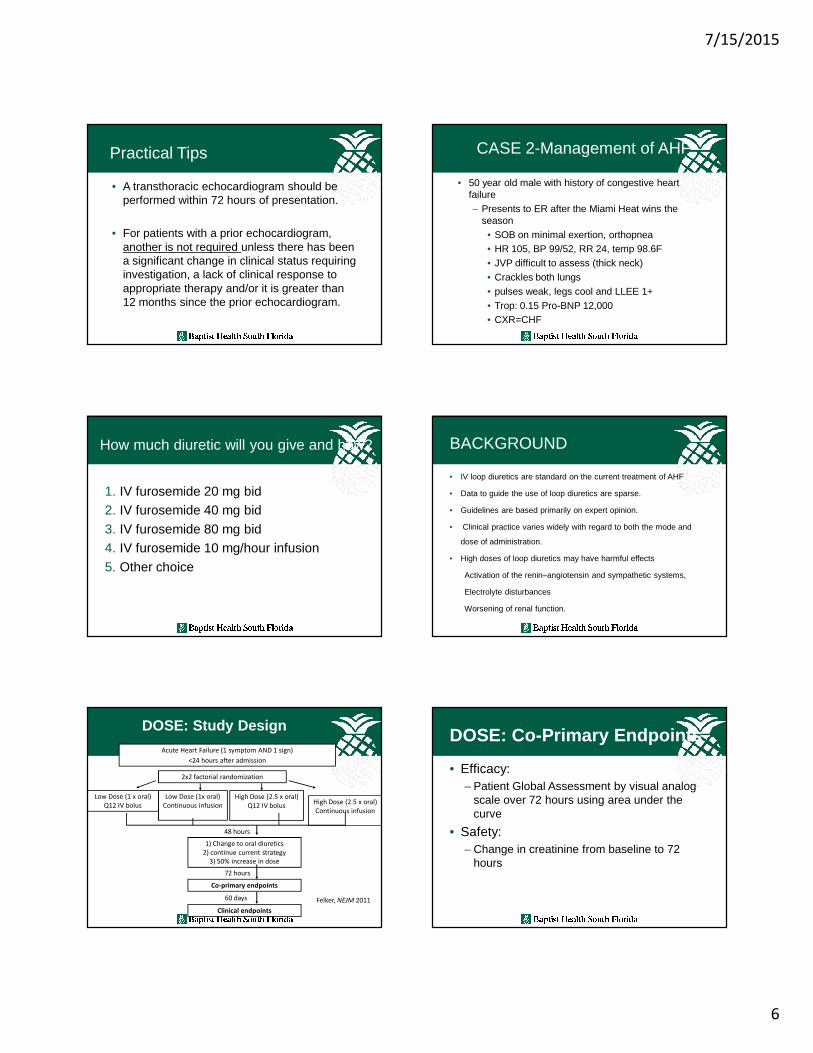
Prognosis depends on Etiology
1230 pts. referred for unexplained CM. Felker GM. NEJM 2000;342:1077
History and Physical Exam in HF
• Clues suggesting etiology of HF• Duration of illness• Severity, triggers and associated symptoms• Weight changes• Palpitations, syncope• Volume status• Disorders breathing at night• Prior hospitalizations for HF• Discontinuation of medications
CASE 1-Initial Evaluation
• 75 year old female• 2 months worsening SOB/orthopnea• Presented to ED after eating at a BBQ
• Past Hx bordeline HTN, COPD, no meds
• Physical exam• HR 98, BP 150/82, RR 28, temp 36.0C• JVP elevated, crackles, pulses 2+, legs
warm and LEE1+
CASE 1-Initial Evaluation
• 74 year old female• CXR = pending
• Labs = pending
7/15/2015
4
How confident are you that it is AHF?
1. <20%2. 21-40%
3. 41-60%4. 61-80%
5. >80%
No right answer
AHF Dx Scoring systems
Baggish AL, et al. Am Heart J 2006; 151: 48-54].
Predictor Points Our Case
Elevated NT-proBNP 4 ?
Interstitial edema on
CXR2 ?
Orthopnea 2 -
Absence of fever 2 2
Current loop diuretic
use1 -
Age > 75 years 1 -
Rales on lung
examination1 1
Absence of cough 1 1
Interpretation 4
e.g. At a score of 9, PPV 92%, NPV 82%, sens 70, spec 93
CASE-1 More information
• 75 year old female• CXR = increased pulmonary markings c/w
edema, no evidence of COPD• Labs = troponin I 0.20
– BNP 728 pg/ml– Creatinine 1.30
AHF Dx Scoring systems
Baggish AL, et al. Am Heart J 2006; 151: 48-54].
Predictor Points Our Case
Elevated NT-proBNP 4 4
Interstitial edema on
CXR2 2
Orthopnea 2 -
Absence of fever 2 2
Current loop diuretic
use1 -
Age > 75 years 1 -
Rales on lung
examination1 1
Absence of cough 1 1
Interpretation 10
e.g. At a score of 9, PPV 92%, NPV 82%, sens 70, spec 93
Risk Scores to Predict Outcomes in HF
J Am Coll Cardiol. 2013;62(16):e147-e239. doi:10.1016/j.jacc.2013.05.019
-SEATTLE HEART FAILURE MODEL
-HEART FAILURE SURVIVAL SCORE
-CHARM RISK SCORE
-CORONA RISK SCORE
-HPRESERVE SCORE
-ADHERE CLASSIFICATION
-AHA GET WITH THE GUIDELINES
-EFFECT RISK SCORE
-OPTIMIZE HF RISK PREDICTION SCORE
• What is BNP?
– A 32 amino acid polypeptide
– Secreted by cardiac myocytes in response to excessive distension of the Heart ventriclesNamed after extracts found in Pig-brain
• What is NT-proBNP?
– NT-proBNP is a biologically inactive 76 amino acid N-terminal fragment
– Co-secreted with BNP
– Even longer t1/2 than BNP (~1-2hrs vs ~20mins)
• Biological effects of Cardiac Natriuretic peptides
– Increase Natriuresis
– Decrease peripheral vascular resistance

7/15/2015
5
Recommendation
-Use a validated diagnostic scoring system forpatients in whom the diagnosis of AHF is beingconsidered
-This recommendation places a relatively high valueon evaluating the constellation of clinical findings in apatient with suspected AHF and less value on anindividual physical examination finding, presentingsymptom or investigation.
Recommendation
• In the clinical scenario when the clinical diagnosis of AHF is of intermediate pre-test probability, a BNP level can be obtained
– to rule-out AHF (BNP <100 pg/ml; NT-proBNP <300 pg/ml)
– or rule-in AHF (BNP >500 pg/ml; NT-proBNP>900 pg/ml if age 50-75 years, NT-proBNP>1800 if age >75 years) as the cause for the presenting symptoms suspicious of AHF
Practical Tips
• A precipitating cause for AHF should be sought.
• An ECG and a chest x-ray should be performed within 2 hours of initial presentation.
• Initial blood tests should include: complete blood count, creatinine, blood urea nitrogen, glucose, sodium, potassium, and troponin.
What additional tests should we order?
• A-Echocardiogram• B-Coronary CT angiogram
• C-Nuclear Stress test• D-All of them
Non Invasive testing
• Echocardiogram– Initial CHF presentation– Repeat if change in clinical status
• Nuclear Cardiac Imaging– If suspected myocardial ischemia– Viability
• Cardiac MRI– Viability– Infiltrative cardiomyopathies
Invasive testing
• Hemodynamics– Guide therapy– Impaired perfusion– Assessment volume status
• Coronary Angiography– Suspected ischemia– Planned revascularization
7/15/2015
6
Practical Tips
• A transthoracic echocardiogram should be performed within 72 hours of presentation.
• For patients with a prior echocardiogram, another is not required unless there has been a significant change in clinical status requiring investigation, a lack of clinical response to appropriate therapy and/or it is greater than 12 months since the prior echocardiogram.
CASE 2-Management of AHF
• 50 year old male with history of congestive heart failure– Presents to ER after the Miami Heat wins the
season• SOB on minimal exertion, orthopnea• HR 105, BP 99/52, RR 24, temp 98.6F• JVP difficult to assess (thick neck)• Crackles both lungs• pulses weak, legs cool and LLEE 1+• Trop: 0.15 Pro-BNP 12,000• CXR=CHF
How much diuretic will you give and how?
1. IV furosemide 20 mg bid2. IV furosemide 40 mg bid
3. IV furosemide 80 mg bid4. IV furosemide 10 mg/hour infusion
5. Other choice
BACKGROUND
• IV loop diuretics are standard on the current treatment of AHF
• Data to guide the use of loop diuretics are sparse.
• Guidelines are based primarily on expert opinion.
• Clinical practice varies widely with regard to both the mode and
dose of administration.
• High doses of loop diuretics may have harmful effects
Activation of the renin–angiotensin and sympathetic systems,
Electrolyte disturbances
Worsening of renal function.
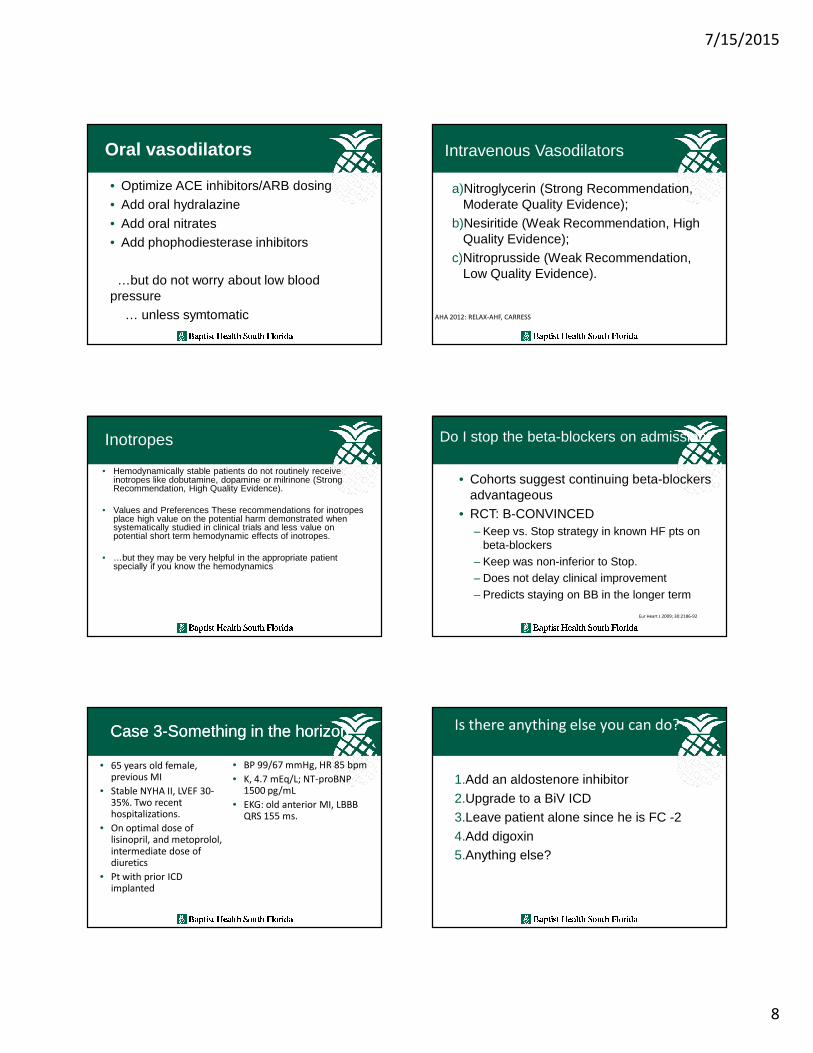
DOSE: Study Design
Acute Heart Failure (1 symptom AND 1 sign)
<24 hours after admission
2x2 factorial randomization
Low Dose (1 x oral)
Q12 IV bolus
48 hours
1) Change to oral diuretics
2) continue current strategy
3) 50% increase in dose
Co-primary endpoints
High Dose (2.5 x oral)
Q12 IV bolus
Low Dose (1x oral)
Continuous infusionHigh Dose (2.5 x oral)
Continuous infusion
72 hours
Clinical endpoints
60 days Felker, NEJM 2011
• Efficacy:– Patient Global Assessment by visual analog
scale over 72 hours using area under the curve
• Safety:– Change in creatinine from baseline to 72
hours
DOSE: Co-Primary Endpoints

7/15/2015
7
DOSE: patient global assessment DOSE: DOSE: Death, Rehosp
• There was no statistically significant difference in global symptom relief or change in renal function at 72 hours for either:
• bolus vs. infusion or low vs. high
• No clinical differences…but– High was associated with favorable trends:
– Symptom relief (global assessment and dyspnea)– Weight loss and net volume loss– Proportion free from signs of congestion– Reduction in NT-proBNP
DOSE-AHF Conclusions Recommendations: Diuretics
We recommend intravenous diuretics be given as first line therapy for patients with congestion (Strong Recommendation, Moderate Quality Evidence).
We recommend for patients requiring intravenous diuretic therapy, furosemide may be dosed intermittently (e.g. twice daily) or as a continuous infusion (Strong Recommendation, Moderate Quality Evidence).
Diuretic Resistant Patient ??
• Assess volume status• Restrict Na2+/H2O intake
• Add another type of diuretic with different site of action (thiazides, spironolactone).
• Hemodynamic assessment and/or positive inotropic agents.
• Hemodialysis, or ultrafiltration
The patient remains persistently symptomatic with Heart Failure, what is next option?
1. Add digoxin2. Increase ACEI3. Reduce beta blockers4. Add inotropic agent5. Call for help
7/15/2015
8
Oral vasodilators
• Optimize ACE inhibitors/ARB dosing• Add oral hydralazine
• Add oral nitrates• Add phophodiesterase inhibitors
…but do not worry about low blood pressure
… unless symtomatic
Intravenous Vasodilators
a)Nitroglycerin (Strong Recommendation, Moderate Quality Evidence);
b)Nesiritide (Weak Recommendation, High Quality Evidence);
c)Nitroprusside (Weak Recommendation, Low Quality Evidence).
AHA 2012: RELAX-AHF, CARRESS
Inotropes
• Hemodynamically stable patients do not routinely receive inotropes like dobutamine, dopamine or milrinone (Strong Recommendation, High Quality Evidence).
• Values and Preferences These recommendations for inotropes place high value on the potential harm demonstrated when systematically studied in clinical trials and less value on potential short term hemodynamic effects of inotropes.
• …but they may be very helpful in the appropriate patient specially if you know the hemodynamics
Do I stop the beta-blockers on admission?
• Cohorts suggest continuing beta-blockersadvantageous
• RCT: B-CONVINCED– Keep vs. Stop strategy in known HF pts on
beta-blockers– Keep was non-inferior to Stop.– Does not delay clinical improvement– Predicts staying on BB in the longer term
Eur Heart J 2009; 30:2186-92
Case 3Case 3--Something in the horizonSomething in the horizon
• 65 years old female, previous MI
• Stable NYHA II, LVEF 30-35%. Two recent hospitalizations.
• On optimal dose of lisinopril, and metoprolol, intermediate dose ofdiuretics
• Pt with prior ICD implanted
• BP 99/67 mmHg, HR 85 bpm
• K, 4.7 mEq/L; NT-proBNP1500 pg/mL
• EKG: old anterior MI, LBBB QRS 155 ms.
1.Add an aldostenore inhibitor
2.Upgrade to a BiV ICD3.Leave patient alone since he is FC -2
4.Add digoxin5.Anything else?
Is there anything else you can do?

7/15/2015
9
NYHA III* or IV heart failureNYHA III* or IV heart failureLVEF LVEF ≤ ≤ ≤ ≤ ≤ ≤ ≤ ≤ 35%35%
ACEACE--I + loop diuretic I + loop diuretic ±± digoxndigoxn
NYHA III* or IV heart failureNYHA III* or IV heart failureLVEF LVEF ≤ ≤ ≤ ≤ ≤ ≤ ≤ ≤ 35%35%
ACEACE--I + loop diuretic I + loop diuretic ±± digoxndigoxn
AldactoneAldactone®® 25 mg/day25 mg/day
(n = 822)(n = 822)
AldactoneAldactone®® 25 mg/day25 mg/day
(n = 822)(n = 822)
Primary EndpointPrimary Endpoint�� Total mortalityTotal mortality
Secondary EndpointSecondary Endpoint�� Cardiac mortalityCardiac mortality�� Cardiac hospitalizationCardiac hospitalization�� Cardiac mortality or cardiac Cardiac mortality or cardiac hospitalizationhospitalization�� Changes from baseline in NYHA classificationChanges from baseline in NYHA classification
Primary EndpointPrimary Endpoint�� Total mortalityTotal mortality
Secondary EndpointSecondary Endpoint�� Cardiac mortalityCardiac mortality�� Cardiac hospitalizationCardiac hospitalization�� Cardiac mortality or cardiac Cardiac mortality or cardiac hospitalizationhospitalization�� Changes from baseline in NYHA classificationChanges from baseline in NYHA classification
PlaceboPlacebo
(n = 841)(n = 841)
PlaceboPlacebo
(n = 841)(n = 841)
Pitt et al, N Engl J Med, 1999.Pitt et al, N Engl J Med, 1999. *History of NYHA IV within 6 months before first dose*History of NYHA IV within 6 months before first dose
3 years3 years
RALES: Study DesignRALES: Study Design RALES-All-Cause Mortality
RALES
Combined Endpoint of Cardiac
Mortality or Cardiac Hospitalization
CRT in Patients with Mild HF Symptoms:MADIT-CRT
Moss et al, NEJM 2009
1820 pts, mostly NYHA II, CRT+ICD vs. ICD aloneLow risk population, annual mortality ~3%40% reduction in HF events in CRT-ICD group
25% reduction in mortality
N Engl J Med. 1997; 336: 525-33
Placebo
(n=3403)
Digoxin
(n=3397)
Absolute
Risk
Difference
Hazard ratio
(95% CI)P value
Heart Failure 35% 27% –8%0.72
(0.66–0.79)<0.001
All-Cause 67% 64% –3%0.92
(0.87–0.98)0.006
Reduces Risk of Hospital Admission (The DIG Trial)
Digoxin significantly reduced the risk of
hospitalization due to heart failure by 28% during
37 months of average follow-up, but its effect on
hospitalization due to all causes was more modest
(a 8% reduction) N Engl J Med. 1997; 336: 525-33
HR = 0.99;
95% CI = 0.91–1.07;
P = 0.80
Does Not Increase Mortality
(The DIG Trial)
7/15/2015
10
Systolic Heart failure treatment withthe If inhibitor ivabradine Trial
Heart rate at baseline influences the effect of ivabradine on cardiovascular outcomes in chronic heart failure:
Effect of ivabradine on outcomes in patients with
chronic heart failure (LVEF <35%), one hospital
admission for HF within 12 months and HR ≥75
bpm
Betablocker
Mineralocorticoidreceptor
antagonist
Drugs That Reduce Mortality in Heart Failure With Reduced Ejection Fraction
ACEinhibitor
Angiotensinreceptorblocker
Drugs that inhibit the renin-angiotensin system have modest effects on
survival
Based on results of SOLVD-Treatment, CHARM-Alternative,COPERNICUS, MERIT-HF, CIBIS II, RALES and EMPHASIS-HF
10%
20%
30%
40%
0%
% D
ecre
ase
in M
orta
lity
One Enzyme — Neprilysin — DegradesMany Endogenous Vasoactive Peptides
Endogenousvasoactive peptides
(natriuretic peptides, adrenomedullin,bradykinin, substance P,
calcitonin gene-related peptide)
Inactive metabolites
Neprilysin
Neprilysin Inhibition Potentiates Actions of Endogenous Vasoactive Peptides That Counter
Maladaptive Mechanisms in Heart Failure
Endogenousvasoactive peptides
(natriuretic peptides, adrenomedullin,bradykinin, substance P,
calcitonin gene-related peptide)
Inactive metabolites
Neurohormonal activation
Vascular tone
Cardiac fibrosis, hypertrophy
Sodium retention
Neprilysin Neprilysininhibition
LCZ696
LCZ696: Angiotensin Receptor NeprilysinInhibition
Angiotensinreceptor blocker
Inhibition of neprilysin
Prospective comparison of AR NI with ACEI to Determine I mpact on G lobal M ortality and
morbidity in H eart Failure trial (PARADIGM-HF)
SPECIFICALLYSPECIFICALLYSPECIFICALLYSPECIFICALLY DESIGNEDDESIGNEDDESIGNEDDESIGNED TOTOTOTO REPLACEREPLACEREPLACEREPLACE CURRENTCURRENTCURRENTCURRENT USEUSEUSEUSE
OFOFOFOF ACE ACE ACE ACE INHIBITORSINHIBITORSINHIBITORSINHIBITORS ANDANDANDAND ANGIOTENSINANGIOTENSINANGIOTENSINANGIOTENSIN RECEPTORRECEPTORRECEPTORRECEPTOR
BLOCKERSBLOCKERSBLOCKERSBLOCKERS ASASASAS THETHETHETHE CORNERSTONECORNERSTONECORNERSTONECORNERSTONE OFOFOFOF THETHETHETHE
TREATMENTTREATMENTTREATMENTTREATMENT OFOFOFOF HEARTHEARTHEARTHEART FAILUREFAILUREFAILUREFAILURE
Aim of the PARADIGM-HF Trial
LCZ696400 mg daily
Enalapril20 mg daily

7/15/2015
11
• NYHA class II-IV heart failure
• LV ejection fraction ≤ 40% � 35%
• BNP ≥ 150 (or NT-proBNP ≥ 600), but one-third lower if hospitalized for heart failure within 12 months
• Any use of ACE inhibitor or ARB, but able to tolerate stable dose equivalent to at least enalapril 10 mgdaily for at least 4 weeks
• Guideline-recommended use of beta-blockers and mineralocorticoid receptor antagonists
• Systolic BP ≥ 95 mm Hg, eGFR ≥ 30 ml/min/1.73 m2
and serum K ≤ 5.4 mEq/L at randomization
PARADIGM-HF: Entry Criteria
0
16
32
40
24
8
Enalapril(n=4212)
360 720 10800 180 540 900 1260
Days After Randomization41874212
39223883
36633579
30182922
22572123
15441488
896853
249236
LCZ696Enalapril
Patients at Risk
1117
Kap
lan-
Mei
er E
stim
ate
ofC
umul
ativ
e R
ates
(%
) 914
LCZ696(n=4187)
HR = 0.80 (0.73-0.87)P = 0.0000002
Number needed to treat = 21
PARADIGM-HF: Cardiovascular Death or Heart Failure Hospitalization (Primary Endpoint)
Enalapril(n=4212)
LCZ696(n=4187)
HR = 0.80 (0.71-0.89)P = 0.00004
Number need to treat = 32
Kap
lan-
Mei
er E
stim
ate
ofC
umul
ativ
e R
ates
(%
)
Days After Randomization
41874212
40564051
38913860
32823231
24782410
17161726
1005994
280279
LCZ696Enalapril
Patients at Risk
360 720 10800 180 540 900 12600
16
24
8
693
558
PARADIGM-HF:Cardiovascular Death
10%
Angiotensin Neprilysin Inhibition With LCZ696 Doubles Effect on Cardiovascular Death of Current Inhibitors of the Renin-Angiotensin
System
20%
30%
40%
ACEinhibitor
Angiotensinreceptorblocker
0%
% D
ecre
ase
in M
orta
lity 18%
20%
Effect of ARB vs placebo derived from CHARM-Alternative trialEffect of ACE inhibitor vs placebo derived from SOLVD-Treatment trial
Effect of LCZ696 vs ACE inhibitor derived from PARADIGM-HF trial
Angiotensinneprilysininhibition
15%
Case 4-Rehospitalization 74 year old female with NYHA FC II-III HF with LVEF 20-25%BP 90/70, HR 85, Na 130, Creat 2.1mg/dL, K+ 5.0. Euvolemic , Fith day after admission. Feeling back to her baseline. Third hospital admission in two months. Ready for discharge
What should you do next?
A.Arrange for hospice careB.Start intravenous outpatient inotropesC.Change cardiologistD.Refer to an outpatient heart failure program
Worsening Chronic Heart Failure: The Major Reason for Heart Failure Hospitalizations
7/15/2015
12
Causes of Hospital Readmission for Congestive Heart Failure
17%
Other19%
Failure to Seek
Care
16%
Inappropriate Rx
Rx Noncompliance
24%
Diet Noncompliance
24%
Annals of Internal Medicine 122:415-21, 1995
Over 2/3 of HF Hospitalizations Preventable
Heart Failure Management Issues
• High Mortality• High re-admission rates
• Poor understanding of disease• Poor Rx adherence
• On-going symptoms• Reduced Quality of Life• More relevant in the Elderly
Medication Adherence Gap
• Cost of medications• Complacency-patient and physician
• Side effects• Lack of understanding
• Infrequent monitoring intervals• Lack of reinforcement
What can we do about it?
• Pt follow up soon after discharge• Medication Reconciliation
• Assessment of volume status• Make your life easy and refer to a heart
failure program
Heart Failure Clinic Team
• Nurse Practitioners• Registered Nurses
• Social work services• Nutritionists
• Pharmacists• Physician Supervising
Heart Failure Clinic TeamMCVI- South Miami Hospital
• Nurse Practitioners• Registered Nurses
• Social work services• Nutritionists
• Pharmacists• Physician Supervising
2,000 patients/year

7/15/2015
13
0% 0%
10%
0%
5%6%
12%
5%
9%
0% 0%
10%
4%5%
0%0%
0%
2%
0% 0% 0%
3%
0%
4%
0%
5%
10%
15%
20%
25%
Oct-13 Nov-13 Dec-13 Jan-14 Feb-14 Mar-14 Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14
Miami Cardiac & Vascular Institute
South Miami HospitalOctober, 2013 - September, 2014
HF Clinic Education Only Patients HF Clinic Treatment Program
National Readmit Rates = 23%
SMH Readmit Rates = 20%
10/13 Implemented
HF Education
Program
Role of Heart Failure Clinics
– Pre-transplant/ pre LVAD eligibility and work-up– Out-patient chronic parenteral inotropic therapy – Medication titration– Patient education– High risk (CHF) rehabilitation programs– Out patient LVAD chronic care– Volume management (outpatient iv diuretics)– Management of social issues
Role of Primary Care Physician
• High risk CHF Patient identification
• Assessment/modification of underlying etiology
• Promt follow up after discharge
• Medication titration• Patient education• Management of
comorbitiies• Family integration
Summary
• When heart failure cannot be controlled look for unsual etiologies
• Follow the guidelines, learn about new drugs• Discharge the patient in a “euvolemic” state
• If available seek the support of a specialized Heart Failure Clinic







