
Joan Doran, Program Lead
27 April 2011
Overview of HPC Teams Education Project
Working Together to Support Best Practices in Palliative Pain &
Symptom Management for LTC Residents

Objectives
1. Update re HPC Teams
2. Overview of capacity building projectsEducation for LTC Homes & Community
Primary Providers
Physician survey
Physician liaison with HPC Teams
3. Input re Education Project

Program Background
Partnership:
• Central CCAC
• Temmy Latner Centre
• Southlake Regional Health Centre
Funding:
• Aging at Home, Central LHIN
• PPSM
MOHLTC:• Mandate

Program Mandate
• Assists primary providers in application of the Model to Guide HPC assessment tools & best practice
• Offers consultation to primary providers about palliative assessment, pain and symptom management
In person, By telephone, teleconference, or Through e-mail
(MOHLTC, 2006)

Program Mandate
• Case-based education & mentoring for primary providers
• Capacity building amongst front-line service providers re delivery of palliative care
• Links providers with specialized hospice palliative care resources
(MOHLTC, 2006)

Regional Cancer Centre'sResidential Hospices
Hospital PCU's LTC Homes Respite Care Retirement
Homes
Community SupportsFaith Groups
FriendsCommunity Organizations
Palliative Care PhysicianMental Health Consultant
CNC Team
Visiting / Family PhysicianPrimary Nurse
CCAC Case ManagerPSW
Allied Health (PT, OT, SLP, DT)Social Worker
Pharmacist Laboratory Hospice Spiritual
Support
Patient / Family
COMMUNICATION
HPC Teams for Central LHINModel for Hospice Palliative Care
Tertiary / Residential Team
Informal Team
Expert Team
Core Team

Advisory Council
• Dr. Nancy Merrow• Dr. Larry Librach• Dr. Russell Goldman• Evelyn Rosen• Joan Doran• Anne Grant

Clinical Nurse ConsultantsCNC Areas
Christine
Alguire
Alliston, Bradford, Beeton, King,
Maple, Schomberg, Tottenham &
Vaughan
Mamdouh Rezk Richmond Hill & Thornhill
Margaret
Cutrara
Markham & Stouffville
Juliana Howes Aurora, East Gwillimbury, Georgina,
Newmarket
Carolyn Willson North York

HPC Program Criteria• Patients with a progressive, life threatening illness
&/or facing end of life issues
• Primary intent of treatment is palliative whether palliation of disease, palliation of symptoms (physical, psychological, social)
• Patient & family agree to referral or to consultative support
• DNR/No Code status is not required for entry onto the program
• Unmet symptom management needs of all types

Role of the CNC
• Supporting health care professionals - not replacing the primary providers
• Professional consultation re PP&SM in the community & LTC
• Capacity building targeting the knowledge & provision of palliative care

CNC Role
• Facilitation & education at Interprofessional Rounds
• Networking with health care teams within each geographical region
• Leadership in standardizing palliative care practice: EDITH, SRK, In-Home Chart
• Educational initiatives in Central LHIN
CCO Toolbox
Common Tools
Isaac
Collaborative Care Plans
Symptom Management Guidelines


Referral Process
• Majority of HPCT referrals from CCAC
• Community nurses or physicians refer directly: telephone or email
• Nursing agency or LTC can request a CNC for one or more of their staff

Referral Process (cont’d)
• HPC Teams will admit, reassess immediate needs & contact providers
• CNC provides consultation report for the physician, CCAC CM, Primary Professional
• CNC follows the client case with the professional

REPORTS ON
ACTIVITY
• Referrals and caseloads increasing as awareness of program grows
• Each contact with a primary provider to provide recommendations re care plan and pain & symptom management
Oct Nov Dec Jan Feb Mar0
50100150200250300350400
75 73 5588 67 83
315 321295 313
344 328
Referrals / CaseloadsOctober 2010 - March
2011ReferralsCaseloads
Oct Nov Dec Jan Feb Mar0
500
1000
1500
2000
12011482
11391480
1197 1274
ContactsOctober 2010 - March
2011
Contacts

Home Visits• Home Visits represent in-
home consultation with Health Care Professional
ER Avoidance
• ER visits documented by CNC, Visiting Nurse and CCAC
• ER ‘visits avoided’ entered into HPC database when CNC consultation prevents patient going to ER for PP&SM
Oct Nov Dec Jan Feb Mar0
20
40
60
80
100
120
140
91
120
97 10288
110
Home VisitsOctober 2010 - March
2011
Home Visits
Oct Nov Dec Jan Feb Mar0
10
20
30
40
50
60
70
32 2922 25
18 1913
33
15
3641
62
ER Visits / Visits AvoidedOctober 2010 - March 2011
ER VisitsER Visits Avoided
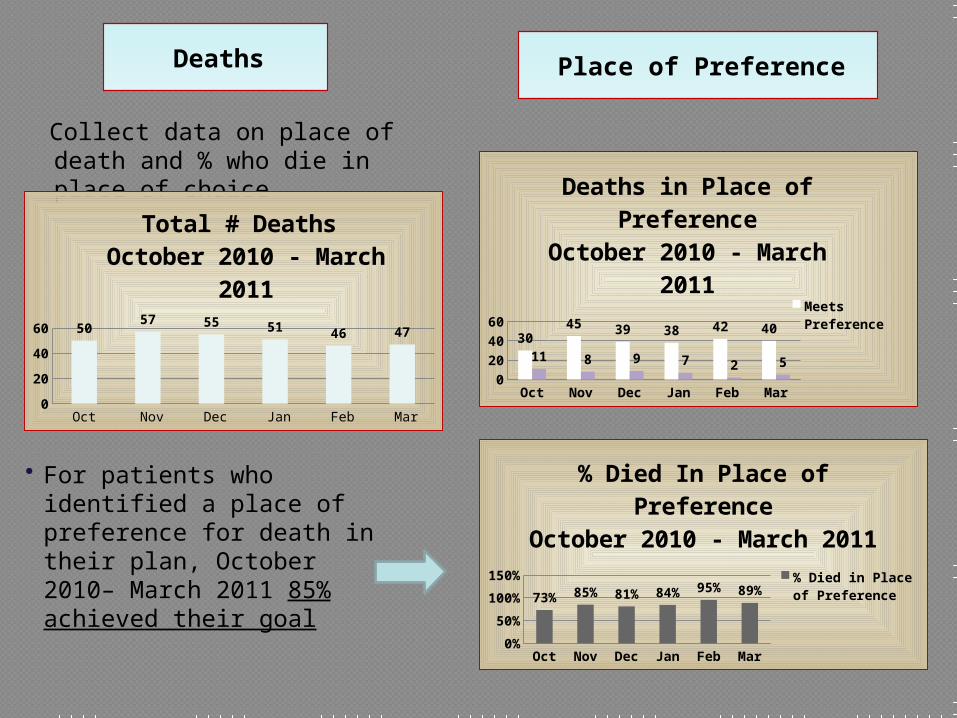
Deaths Place of Preference
Collect data on place of death and % who die in place of choice
• For patients who identified a place of preference for death in their plan, October 2010– March 2011 85% achieved their goal
Oct Nov Dec Jan Feb Mar0
1020304050
30
4539 38 42 40
11 8 9 72 5
Deaths in Place of Preference
October 2010 - March 2011
Meets Pref-erence
Oct Nov Dec Jan Feb Mar0%
50%
100%
150%
73% 85% 81% 84% 95% 89%
% Died In Place of Pref-erence
October 2010 - March 2011
% Died in Place of Preference
Oct Nov Dec Jan Feb Mar
Total # Deaths 50 57 55 51 46 47
5
35
50 57 55 51 46 47
Total # Deaths October 2010 - March
2011

Program Hours
• Core hours, 0830-1630 Mon-Fri
• After hours on-call available
• CNCs provide consultation for all health care professionals
• After Hours Phone: 905-954-5220

Contacting HPC Teams
Catherine Bazowsky, Administrative Assistant
Phone: (905) 895-4521, ext. 6388
Fax: (905) 830-5978
Email: [email protected]
Website: http://centralhpcnetwork.ca/hpc/hpcteams.html

LTC Home Education Project
Funded by Central LHIN
Provide support to LTC homes in the
provision of quality end-of-life care
Increase knowledge transfer for the
health care team

Outcomes
Reduction in ER visits
Enhanced Pain and Symptom Management
Enhanced communication with residents/families
Increase utilization of Advance Care Planning

Process
Requested Expression of InterestInterviewed & selected 4 LTC homes
Representation across LHIN
Gap analysis
Collaborated with NLOTDeveloping curriculum
Physician & RN/RPN
PSW

Process (cont)
4 Sessions
On-line Repository of Resources
Case finding among current residents
and case-based mentoring
Program evaluation

Topics
Issues and Challenges in Providing
Quality End-of-Life Care
Advance Care Planning
Working with Families
Pain Management and Last Hours

Education
Hired researcher/education assistant
MD/RN/RPN sessions facilitated by
palliative care physicians, PC experts,
with support from CNC’s
PSW sessions will be led by PalCare
Evaluation
Conduct gap analysis to determine reasons for ER transfers
Chart reviews
Interviews with MD’s, RN, Administration
Based on gap analysis, develop, implement and evaluate intervention for quality EOL care

Feedback??
What issues do you identify in providing high quality EOL care to LTC residents?
Are palliative patients being sent to ER? Why?
What needs to be in place to support LTC residents to die in their home?

Physician Survey
‘Assessment of Service Provision and Willingness to Engage’
Developed by Dr Russell Goldman and Dr Camilla Zimmerman
– TLCPC/ PMH

Purpose
To determine the level of GP/FP care
being provided to community
homebound patients

Purpose
To identify the proportion of physicians who provide the following services to homebound palliative patients: Scheduled home visits
After-hours home visits
Urgent home visits during office hours
24/7 coverage with after-hours home visits as required

Purpose
To determine what supports would facilitate PCP’s to engage in the care of homebound palliative patients
Develop a registry of PCP’s who would be willing to assume care of patients who do not have access to a FP

Methodology
Survey all FP who have a primary
practice address in Central LHIN
Mail out survey/ E mail – (OCFP
assisting)
Can complete on-line or mail in survey

Outcomes
Identify barriers to the provision of
home palliative care by FP’s
Inform the design of an intervention to
improve FP capacity and willingness
to provide home based palliative care

Outcomes
Develop a list of FP’s who are willing to take on additional palliative patients
Results will be presented at national and international conferences and published in peer- reviewed journals
Timeline – to be completed within next 6 months

Physician Liaison
Physician roster established to provide 24/7 availability
Provide support to the HCP Teams CNC’s & FP’s to care for patients in community

Questions
37







