
16/07/2010
1
SINUSCENTRO
João Flávio Nogueira, MDOtolaryngologist
Taís Nogueira, MDAnesthesiologist
Sinus CentroFortaleza, Brazil

16/07/2010
2
www.sinuscentro.com.br/museu

16/07/2010
3
October, 16, 1846. William Morton demonstrates anesthesia

16/07/2010
4

16/07/2010
5
• Anatomical landmarksidentification
• Complications
• Postoperative
• Trauma of the nasal mucosa may lead to formation of adhesions
Kalra G, Keir J, Tahery J. Prevention of blood staining of endoscope tip during Functional Endoscopic Sinus Surgery: sleevetechnique. J Laryngol Otol. 2009;123(12):1358-9.
• Bleeding could obscure the view of the endoscope.
• Repeated cleaning intraoperatively is time consuming.
Endoscrub – Medtronic, Jacksonville, USA, 2008

16/07/2010
6
Book Prof. Navarro

16/07/2010
7
• Inflammatory mucosa
• Clinical conditions
– HBP
– Chronic diseases
– Fever
• Smoking
• Pre-operative assesment

16/07/2010
8
• Surgeon techniques
– Instruments
– Patient positioning
– Room temperature
• Local vasoconstriction
• Infiltrations ?
16/07/2010
9

16/07/2010
10

16/07/2010
11

16/07/2010
12
Increases venous return 30%

16/07/2010
13
1 °.C
Bleed
ing
Reduces coagulation capability 30%
Sarmento Junior KM, Tomita S, Kós AO. Topical use of adrenaline in different concentrations for endoscopic sinus surgery. Braz J Otorhinolaryngol. 2009;75(2):280-9.
• Ideal patient temperature: 36°C
– Saline heat
• Lower temperatures
– Drug metabolism

16/07/2010
14
• Epinephrine
• Cocaine
• Oxymetazoline
– 5 minutes
– 10 minutes
Sarmento Junior KM, Tomita S, Kós AO. Topical use of adrenaline in different concentrations for endoscopic sinus surgery. Braz J Otorhinolaryngol. 2009;75(2):280-9.

16/07/2010
15

16/07/2010
16
• Wormald PJ, van Renen G, Perks J, Jones JA, Langton-Hewer CD.The effect of the total intravenous anesthesia compared withinhalational anesthesia on the surgical field during endoscopicsinus surgery. Am J Rhinol. 2005; 19(5):514-20.
• BACKGROUND: Bleeding during endoscopic sinus surgery (ESS) mayincrease complications and negatively effect the surgery and itsoutcome.
• The aim of this study was to compare TIVA (propofol+remifentanil)vs. inhalation anesthesia (sevoflurane).
• RESULTS: The two groups were matched for surgical procedure andcomputed tomography scores.
• Mean arterial pressure and pulse were found to influence thesurgical field.
• CONCLUSION: In patients undergoing ESS, TIVA results in a bettersurgical field than inhalational anesthesia.

16/07/2010
17

16/07/2010
18
• CO2
– Vasodilatation to target organs
– Brain
• Ideal parameters:
• Controlled hypotension
– BP: mean 60 – 70
– HR < 60 bpm
– CO2 < 35
– SPO2 > 97%
16/07/2010
19
History of dentistry. Sinus Centro MuseuAvailable at: www.sinuscentro.com.br/museu

16/07/2010
20
1 : 2,00020 amps of epinefrine + 20 mL 0,9% saline solutionPhotosensitive (60 minutes)

16/07/2010
21
0
50
100
150
200
250
Dosage I Dosage II Dosage III
Control
1:50000
1:10000
1 2000
Ave
rage
Ad
ren
alin
e(p
G/m
L)
10 – 15 minutes 10th pledget End of surgery
0,45

16/07/2010
22
Blood loss (mL)
• Operation time was shorter (1:2,000)• Less bleeding (1:2,000), p < 0,0001 • Plasmatic levels of epinephrine raised in all
groups, especially (1:2,000) • There was a trend towards elevation of blood pressure
in the groups using adrenaline 1:2,000 and 1:10,000, with a greater occurrence of hypertensive peaks.
• The elevation of blood pressure in the 1:2,000 and 1:10,000 was progressive but very slow throughout surgery, which could be related to the anesthesia technique.

16/07/2010
23

16/07/2010
24
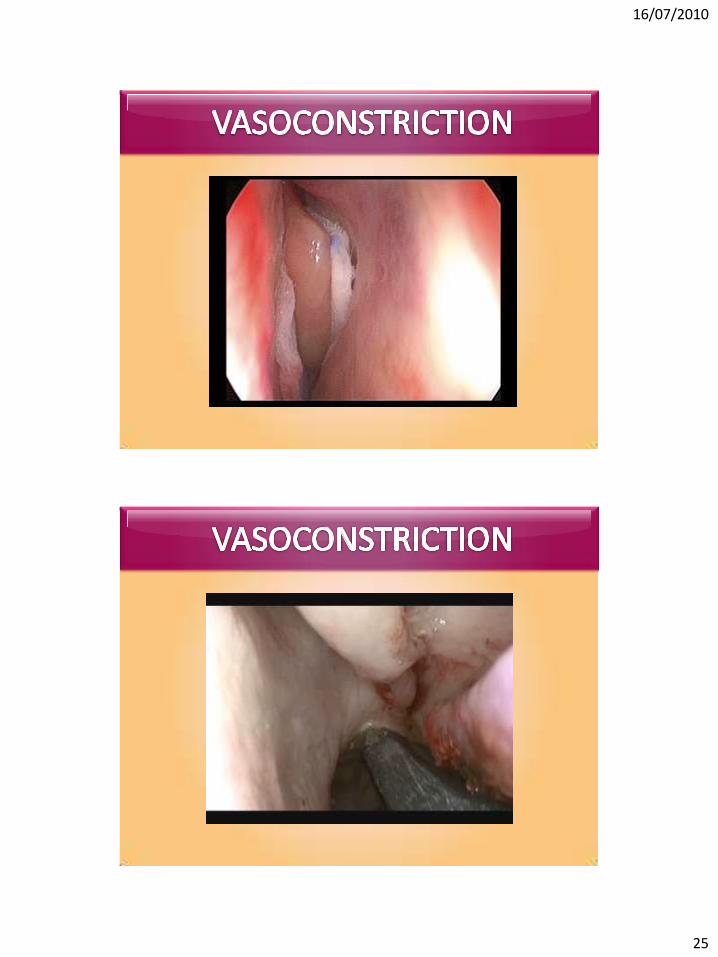
5 to 10 minutes
16/07/2010
25

16/07/2010
26
1:100.000
16/07/2010
27

16/07/2010
28
• Pterygopalatine fossa– Nasal – Endoscopy
– Oral
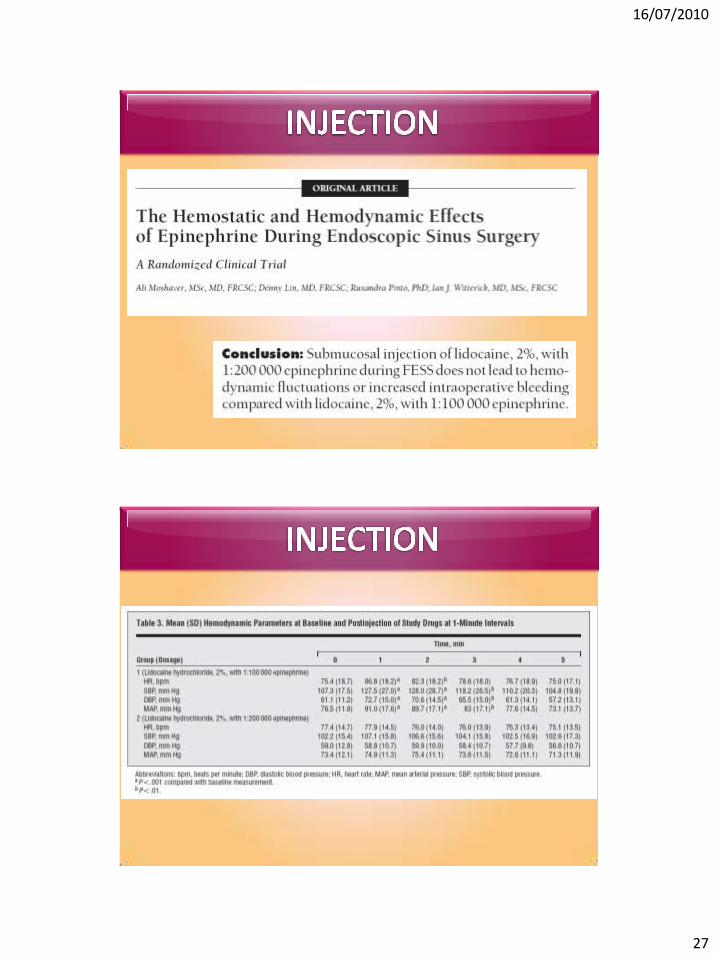
• Epinephine– 1:200,000 – 0,005 mg/mL
– 1:100,000 – 0,01 mg/mL
– 1:80,000 – 0,0125 mg/mL
– 1:50,000 – 0,02 mg/mL
– 1:10,000 – 0,1 mg/mL
– 1:2,000 – 0,5 mg/mL
10 mL 1:100,000

16/07/2010
29
10 mL 1:50,000
1 mL 1:10,000

16/07/2010
30
• Lidocain
• High BP
• Paradoxal bradicardia (severe)

16/07/2010
31
Nature, 20:August 1896

16/07/2010
32
Sir Godfrey N. HounsfieldCT – 1967Nobel Prize 1979
British Museum, 2008
Sir Godfrey N. HounsfieldCT – 1967Nobel Prize 1979
British Museum, 2008

16/07/2010
33
Brain study using CT. A tumor is clearlyobservable in the lower transverse slice.Images were presented by David Chesler at theMeeting on Tomographic Imaging in NuclearMedicine, September 15-16, 1972.
British Museum, 2008
3D reconstruction - DICOM files – Imaging Studio Software
16/07/2010
34
Nogueira JF, et al. Brief History of Otorhinolaryngology. Braz J Otorhinolaryngol, 2007 – with permission from Karl Storz company, Tutligen, Germany

16/07/2010
35
Desermeaux 1853
Nogueira JF, et al. Brief History of Otorhinolaryngology. Braz J Otorhinolaryngol, 2007
Karl Storz and Harold Hopkins 1953
Nogueira JF, et al. Brief History of Otorhinolaryngology. Braz J Otorhinolaryngol, 2007 – with permission from Karl Storz company, Tutligen, Germany

16/07/2010
36
Nogueira JF, et al. Brief History of Otorhinolaryngology. Braz J Otorhinolaryngol, 2007 – with permission from Karl Storz company, Tutligen, Germany
1970s 1980s e 1990s
October, 16, 1846. William Morton demonstrates anesthesia

16/07/2010
37

16/07/2010
38
• Adrenegic stimulation
• Increase
– HR
– BP
– Cardiac debit
• Peripheric vasoconstriction
– Increase peripheric vascular resistence
• Pre-operative assesment
– Interview
– Physical examination
– Complementary exams
• Intra-operative anesthesia
• Post-operative care

16/07/2010
39
• QUESTIONS
– Do you bleed to much during dental ?
– Females – How is your period ?
– Lacerations – How long is the bleeding time ?
– Nasal bleeding – Do you have ?
• PHYSICAL
– Hematomas
– Articular deformities
• Ask about medications in use:
• Aspirin– 7 days prior to surgery
• Coumadin– 2 – 6 days
• Ginkgobiloba– 36h
• Garlic and ginseng– 7 days

16/07/2010
40
• Hipertension• Diabetes• Heart disease• Lung disease• Renal disease• Liver disease
• MAINTAIN USE OF MEDICATION• (Except, methformin, IECA, etc)
• Orientations:
– Fasting:
• Children: 6 hours (solids); 2 hours (liquids)
• Adults: 6 hours (solids); 2 hours (liquids)
• Liquids: water, coconut water, tea, juice withoutresiduals (apple, etc)

16/07/2010
41

16/07/2010
42
• BLEEDING CONTROL
– Controlled hypotension
– Ventilation
– Positioning
• CONTROLLED HYPOTENSION
• Objective: – Reduce CD, yet preserving flux to target organs– MBP > 50 mmHg– CO2 > 30 – FiO2 > 90%

16/07/2010
43
• Ideal parameters: ASA I and II
• Controlled hypotension
– BP: mean 60 – 70
– HR < 60 bpm
– CO2 < 35
– SPO2 > 95%
• Hypnosis: PROPOFOL
• Opyoid: REMIFENTANIL
• Alpha2agonist: DEXMEDETOMIDINE
• Beta Blocker: ESMOLOL
• Alpha1agonist: DROPERIDOL
• Vasodilator: NITROPRUSSIATE

16/07/2010
44
• Opyoids and beta blockers cause importantreduction of the adrenergic response to stress
• Dexmedetomidine increases the sympaticresponses
• Propofol increases peripheric vasodilatation –liberation of nitric oxide
7565
70 6772
8070
60 6065
0
20
40
60
80
100
0 30 Min 60 Min 120 Min 180 Min
FC
PAM
• Hemodinamic parameters – PRO + REM

16/07/2010
45
• Avoids environment pollution
• Reduces final use of drugs
• Previsible awakening

16/07/2010
46
• BIS - Optional

16/07/2010
47
• Positive pressure (airway) – 20 mmHg
• Venous stasis
• Reduce pre-cargo LV and RV
• Increase post-cargo RV
Tube’s diameterWomen: 7 – 7,5Men: 8 – 8,5

16/07/2010
48
• AWAKENING
Blo
od
pre
ssu
re
Hea
rt f
req
uen
cy
CO
2
• Analgesia
• Nausea control
– Zofran
– Dexamethazone
• Patients comfort

16/07/2010
49
• ESS with local + sedation
• Ambulatory procedures
• Balloon sinuplasty ?
• Sedation:
– Adult, 70 Kg
• Dormonid
• Fentanyl
• Local anesthesia

16/07/2010
50
• Advantages– Faster procedures
– Quick recovery
– Less bleeding
– Low cost procedure
– Day basis
• Disadvantages– Unsecured airway
– Patient discomfort ?
Top 87 Bad Predictions about the FuturePublished on 3/28/2006

16/07/2010
51

16/07/2010
52
• Choosing the right anesthesia technique to ESS is important
• Tailored to the patient - TASS
• Pre, intra and post-operative care
• Future…

16/07/2010
53
• Time is important
• Clean and dry surgical field is crutial
• Different techniques
• Talk to your anesthesiologist
– TESS: Tailored endoscopic sinus surgery
– TASS: Tailored anesthesia for sinus surgery







