
June 28, 2004Mark Duffett
Leslie Gauthier
The Medley® Pathway to Patient Safety
“If you find a path with no obstacles, it probably doesn’t lead anywhere”

July 2001: Investment in the Medley® Infusion System
• Hamilton first to implement hospital-wide• Implemented a “pump for a pump”• Guardrails were only a promise• Safety features:
– drug calculator– free flow protection– tamper protection– ergonomic design
• Software log—new way of investigating incidents• Beginning of a partnership with Alaris Medical
Initial Issues Identified
• “Air-in-line” alarms• Secondary infusions:
– Different, louder alarm when infusion complete– Alarm if secondary med not “unclamped”– Infusion issues related to high rates (>200mL/hr)
• Keypad noises– awaking patients or a safety feature?
• No graphic display of site pressure • Door Failure• VTBI rate set too low

Canada Day Weekend 2001: Problems
• “System/Communication Errors” appeared on units in the PICU
• There was the perception that the devices powered down and stopped infusing
• Investigation:– Software log confirmed the devices continued to
infuse– Caused by a capacitor problem
First upgrade!

February 2002: Guardrails
• Significant milestone for Hamilton• Consensus building for the dataset• Practice standardization
But…• No bolus feature available• Limited number of drugs supported• Added complexity
July 2002: Disaster Mode
• Multiple incidents the week of July 16th
• “Runaway infusions”, incorrect rates and programming
• Response:– Communication and education for all staff – Mandated use of solusets– Reiterate mandatory use of guardrails– Eliminate bolusing from continuous infusions

July 2002: Investigation
• Joint investigation with HHS, St. Joseph’s and Alaris
• Findings:– “Fluid Ingression” problems – 4 malfunctioning keypads identified– Log analysis showed that after each keypad
malfunction ”START” was selected
• Twofold problem:– Technical malfunction– User/technology interface

June 2002: Results
• Improved processes for incident investigation, including:– Biomedical Support 24 hrs/ 7 days/week– Medley incident form– Segregation of the Medley devices and tubings– Completion of incident reports
• Feedback to Alaris:– Customer Call Centre and the turnaround time for
analyzing the software logs– Why are Guardrails under the “OPTIONS” key?

June 2002: Results
• Provided staff an opportunity to verbalize their concerns regarding their perceptions of the safety of the Medley® system
• Upgrade in August 2002 to replace keypads• Practice issues
– Guardrails underused– Bolusing from continuous infusions
• Competency checklists

October 2002: Upgrade
Hardware:• APM seals
Software:• Guardrails for bolus doses of infusions• Increased capacity of Guardrails system• CQI software installed
May 2003: Upgrade
Hardware:• Correct “System/Communication Errors”
Software:• revisions to the Guardrails • 1st download of CQI data:
– 10% of all devices in the city over 6 months

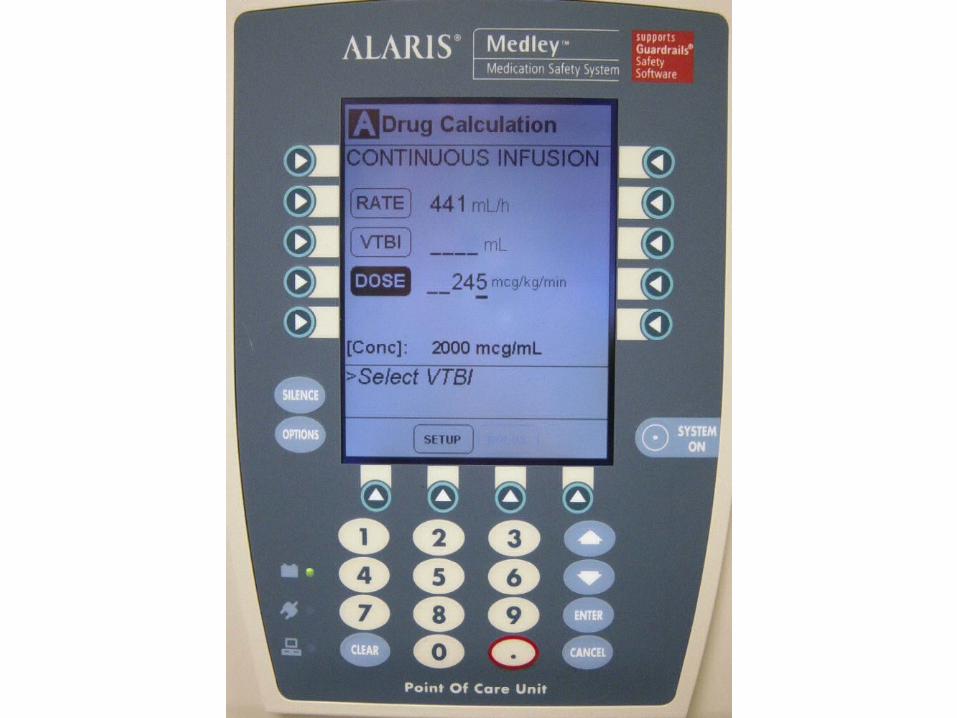
Dobutamine Incident
RN description of event:• The pump “all of a sudden” increased the rate to 905
mL/h following the hanging of a new 250 mL bag of dobutamine
Software log showed:• The pump alarmed for the VTBI absorbed• Door opened• 75 seconds later new VTBI selected• 245 entered in the dose field instead of the VTBI field• “START” selected • Guardrails were not being used
Overinfusions
• A number of incidents where the RN identified that the pump “ran away”
• Software log showed no problems• Most likely caused by improper set loading
resulting in free flow
Solution to be implemented soon!

December 2004: Upgrade
Hardware:• Capacity for syringe platform (NICU, PICU, OR)• Corrective actions for fluid ingression
Software:• Guardrails are not under “OPTIONS”• Updates to the Guardrails
– to deal with issues identified in the CQI download in May 2003 Direct access to the Guardrail Software
• Easier access to the CQI data • 2nd CQI download

June 2004: Audit
Software:• Download of CQI data• Are channel labels used appropriately?• Guardrails audit
– Use of guardrails– Overrides of alerts– Appropriate patient profile used
• Can we gain insight into the overrides?
Hardware:• Are we using this expensive technology
appropriately?

June 2004: Device Use Audit
Hend General MUMC NICU
# pumps 149 235 211 55
# pumps with a pt 90 118 95 35
# LVP not used with a pt 30 56 32 38
No clear indication (%) 20% 20 % 14% 0%
Not plugged in (%) 27% 27% 22% 2%
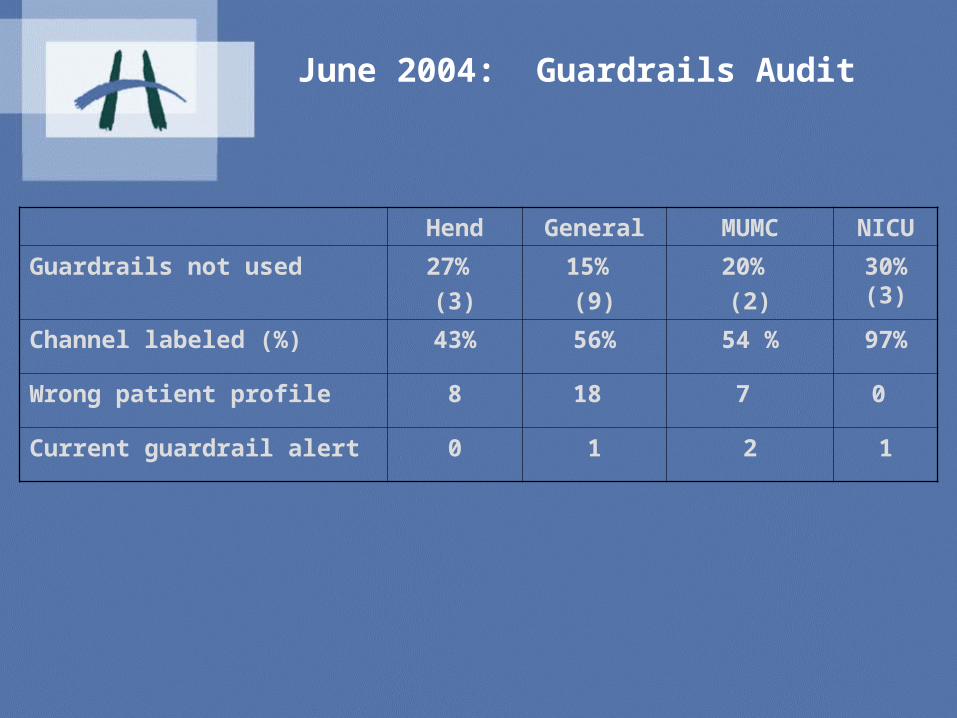
June 2004: Guardrails Audit
Hend General MUMC NICU
Guardrails not used 27% (3)
15% (9)
20% (2)
30% (3)
Channel labeled (%) 43% 56% 54 % 97%
Wrong patient profile 8 18 7 0
Current guardrail alert 0 1 2 1
System Improvement Using CQI Data
• Does the system prevent errors?• Can we increase Guardrail use? • Can we reduce nuisance alerts?• Can we improve the response to alerts?

What Do With CQI Data?
CQI Data
Adverse Events
Prevented
Guardrail Changes
Opportunities to improve practice!
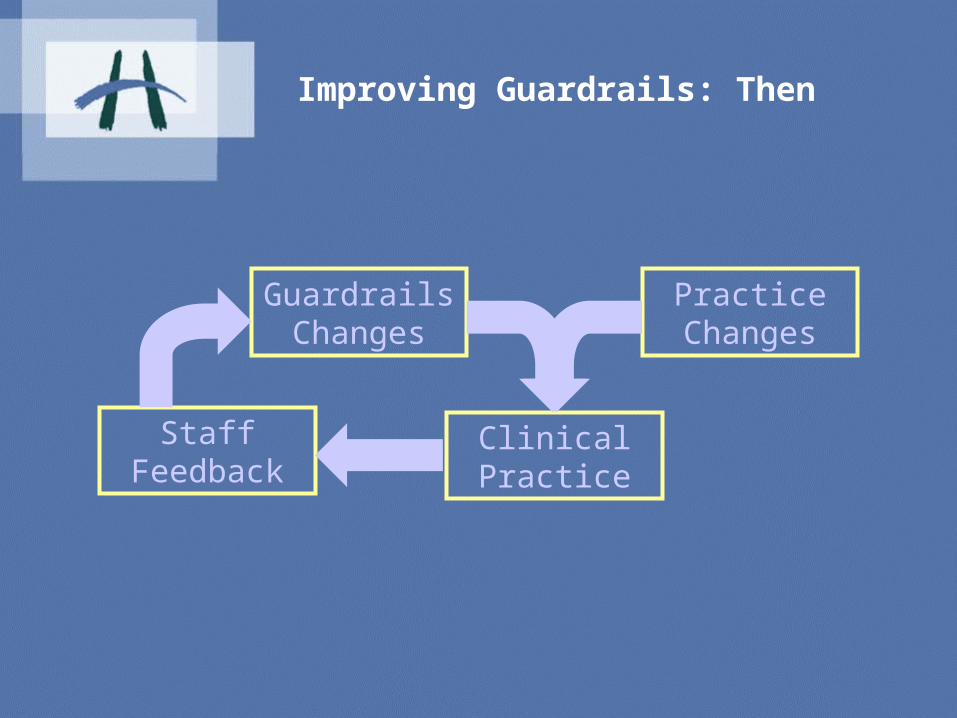
Improving Guardrails: Then
Guardrails Changes
Practice Changes
Clinical Practice
Staff Feedback

Improving Guardrails: Now
Guardrails Changes
CQI Data
Practice Changes
Clinical Practice
Staff Feedback
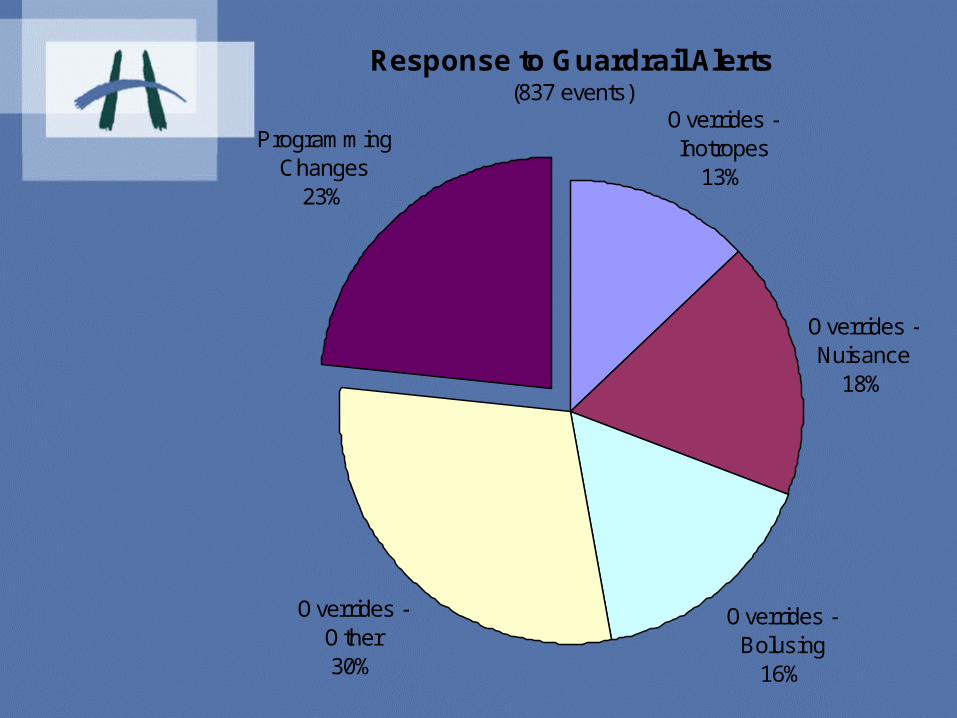
Response to Guardrail Alerts(837 events)
Overrides - Nuisance
18%
Overrides - Bolusing
16%
Overrides - Other30%
Programming Changes
23%
Overrides - Inotropes
13%

Summary of Downloaded Data(analyzed by event)
Total Changes
Alerts 2675 250 9.3 %
Events 837 196 23 %
69 potentially clinically significant events
= 576 events/year prevented at
Hamilton Health Sciences

Can We Reduce Nuisance Alerts?
0
100
200
300
400
500
600
700
amiod
aron
e
dana
paro
id
diltia
zem
dobu
tam
ine
dopa
mine
epine
phrin
e
eptifi
batid
e
fent
anyl
furo
sem
ide
hepa
rin
hydr
omor
phon
e
insuli
n (re
gular
)
KCl High
dos
e inf
us.
labet
alol
Ale
rts
May 2003 - Dec 2003 Dec 2003 - Jun 2004

Can We Increase Guardrail Use?
0
1000
2000
3000
4000
5000
6000
7000
8000
9000
10000
Nov 2002 - May 2003 May 2003 - Dec 2003 Dec 2003 - June 2004
Tota
l Ale
rts
-1
1
3
5
7
9
11
13
15
% C
om
pli
ance
wit
h A
lert

Can We Increase Guardrail Use?
0
100
200
300
400
500
600
700
amiod
aron
e
dana
paro
id
diltia
zem
dobu
tam
ine
dopa
mine
epine
phrin
e
eptifi
batid
e
fent
anyl
furo
sem
ide
hepa
rin
hydr
omor
phon
e
insuli
n (re
gular
)
KCl High
dos
e inf
us.
labet
alol
Ale
rts
May 2003 - Dec 2003 Dec 2003 - Jun 2004

0
10
20
30
40
50
60
70
80
90
100
mag
nesiu
m s
ulfat
e
mida
zolam
milri
none
mor
phine
nitro
glyce
rin
nitro
prus
side
nore
pinep
hrine
oxyt
ocin
pant
opra
zole
phen
yleph
rine
prop
ofol
sodiu
m b
icarb
onat
e
vaso
pres
sin
vecu
roniu
m
Ale
rts
Res
ult
ing
in C
han
ges
(%)
May 2003 - Dec 2003 Dec 2003 - Jun 2004
Can We Improve the Response to Alerts?
Work in Progress: Hardware
• Issues with secondary medication infusions:– Alarms, clamps etc.
• Correction for the free flow problem• Fluid Ingression• Batteries• Keypad Failure related to an electronic
circuit• Disposables, e.g. blood filters for NICU• Allocation of this expensive resource

Work in Progress: Software
• Improve Guardrails dataset• Guardrails for secondary infusions• Improvements to Guardrails software• Improvement in CQI data downloading and
analysis.
Work in Progress: Practice
• Better incident reporting• Improve front line staff’s knowledge, skill
and understanding of the safety platform• Standardization of practice• Improve decision making skills related to
alerts and overrides• Improve understanding of over-rides• Disseminate audit/download results.
What Have We Learned?
• This is a process, not a project. • This is a complex process.
• Buying technology to improve patient safety isn’t an easy fix. It requires continuous investment in staff and infrastructure to support it at make it successful.

It took Thomas Edison 2000 experiments to invent the light bulb.
He said, “I never failed once. It just happened to be a 2000 step process”








