
Kentucky Health Information Exchange
(KHIE)
Kentucky e-HealthHistorical Overview
• March 8, 2005– Legislation (Senate Bill 2) to create a
secure interoperable statewide electronic health network• Kentucky eHealth Network Board (KeHN)• Health care Infrastructure Authority
– University of Kentucky– University of Louisville– Supported by the Cabinet for Health & Family
Services
• Appointment of several committees– Health Information Exchange
Kentucky Health Information ExchangeThe Beginning
2007 Medicaid Transformation Grant ($4.9M)
Allowed development of core functionality ofThe Kentucky Health Information Exchange
(KHIE)
6 Pilot Hospitals and 1 Clinic signed the KHIE Participation Agreement
KHIE pilot went live online April 1, 2010
KHIE and ARRA
2009 - American Recovery & Reinvestment Act (ARRA)
to provide State Grants to Promote Health Information Technology
to improve the quality and efficiency of health care
and expand the secure, electronic movement and use of health information among organizations
according to nationally recognized standards
Governor’s Office of Electronic Health Information
GOEHI Overview
In August 2009, Governor Steve Beshear named the Cabinet for Health and Family Services
as the state entity responsible for the administration of Kentucky’s Health Information Exchange (KHIE)
and issued an Executive Order to create GOEHI
Charged with providing leadershipfor statewide health information technology
ARRA Funding
State HIE Cooperative Agreement
•Strategic & Operational Plan submitted August 27, 2010
•ONC must approve plan before operational funds will be made available
•Kentucky expected to receive $9.75M

KHIE GOAL
Provide HIE Connectivity
to as many providers as possible
over the next year or so
with little or no startup cost to the providers

KHIE – The Stakeholders
• KHIE Coordinating Council– 23 Members on the Council
• 6 Committees reporting to the Council(Six to ten members serve on each committee)
– Accountability & Transparency– Business Development & Finance– Interoperability & Standards Development– Provider Adoption & Meaningful Use– Privacy & Security– Population Health
CHFS Administrative Order in February 2010

Kentucky Environmental Scan
• Laboratory - 60% Labs operating can deliver reports electronically
43% Providers receiving reports electronically
• Pharmacy – 85% Pharmacies capable of receiving e-Prescribing
16% Providers actually e-Prescribing
• Nationally < 4% Providers fully utilizing EMR Systems
Key Findings
Identifying ‘challenges’ (and resolutions)!!
• Many vendors/EMR systems not ready to process CCD(Continuity of Care Document – Standard of patient data transfer)
• Cost of EMR upgrades to hospitals & physician practices
• Disruption of practice for EMR implementation
• Getting Participant Agreements signed with KHIE

Current Work & Progress(!)
ACS and Axolotl in Partnership for KHIE Connectivity
Four Additional Hospitals and Two FQHC Clinics being added
Outreach and Informational Sessions:
• Four Regional KHA meetings in September & October• KPCA Annual Meeting October 18• Regional AHIMA Meetings October 22nd & November 5th • Five CME Meetings with KY REC• KHA/KMA e-Health conference November 17• One-on-One meetings at Provider Locations
KHIE & RHIO’s
• KHIE is working closely with all RHIO’s in Kentucky including HealthBridge, the Northeast KY RHIO and LouHIE
• KHIE and HealthBridge have a signed MOU to connect Health Bridge to the KHIE
KHIE and REC Coordination
2 Regional Extension CentersFor Provider EMR Adoption, Implementation,
And Connectivity
University of Kentuckyand
HealthBridge

Kentucky Regional Extension Centers
Source: Kentucky Hospital Association, 2010
Bath
Boone
Boyd
Bracken
Campbell
Carter
Elliott
Fleming
Gallatin
Grant
Greenup
Kenton
Lawrence
Lewis
Magoffin
Mason
Menifee
Montgomery
Morgan
Nicholas
Pendleton
Powell
Robertson
Rowan
Wolfe
Bourbon
Boyle
Clark
Fayette
Franklin
Garrard
Harrison
Jessamine
Madison
Mercer
Owen
Scott
Woo
dfo
rd
Breckinridge
Bullitt
Carroll
Grayson
Hardin
Henry
Jefferson
LarueMarion
Meade
Nelson
Oldham
Shelby
Spencer
Trimble
Washington
Adair
Allen
Anderson
Ballard
Barren
Bell
Breathitt
Butler
Caldwell
Calloway
Carlisle
Casey
Christian
Clay
Clinton
Crittenden
Cumber
land
Daviess
Edmonson
Estill
Floyd
Fulton
Graves
Green
Hancock
Harlan
Hart
Henderson
Hickman
Hopkins
Jackson
Johnson
Knott
Knox
Laurel
Lee
Leslie
Letcher
Lincoln
Livingston
Logan
Lyon
Marshall
Martin
Mccracken
Mccreary
Mclean
Metcalfe
Monroe
Muhlenberg
Ohio
Owsley
Perry
Pike
Pulaski
Rockcastle
Russell
Simpson
Taylor
Todd
Trigg
Union
Warren
Wayne
Webster
Whitley
Healthbridge Tri-State REC
UK & Healthbridge
UK, UL & Kentucky REC
University of Kentucky REC

KHIE and CHFS Cabinet Resources
• KHIE is the resource for Cabinet data– 2 years of Medicaid Claims Data currently available in
production with nightly data load updates
• State Laboratory Results– Newborn Screenings– All other legally available state lab tests available– Currently in testing mode with the two lab vendors
• Immunization Registry – In production in pilot stage– Currently in design phase to connect the Immunization Registry
to the KHIE
• Future interfaces with Public Health planned

KHIE Rollout
• Continue to add hospitals in groups of 4-5• Two methods to submit
– Using CCD (Continuity of Care Document)– Using Edge Server allowing access to the
Virtual Health Record• Provide server to providers that choose
the Edge Server method• Working with EHR Vendors statewide to
get interfaces built

Medicaid Incentive Program Physicians
• Medicaid - Physicians whose caseloads include at least 30% Medicaid patients are eligible to receive up to $63,750 over the course of 6 years.
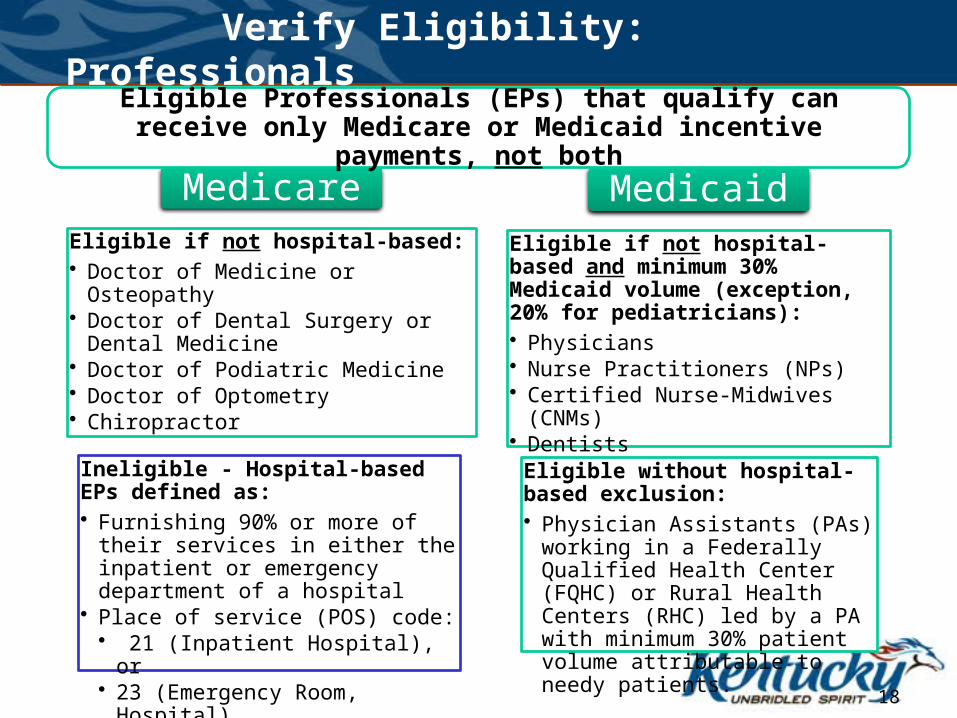
MedicareEligible if not hospital-based:• Doctor of Medicine or Osteopathy• Doctor of Dental Surgery or Dental
Medicine• Doctor of Podiatric Medicine• Doctor of Optometry• Chiropractor
Ineligible - Hospital-based EPs defined as:• Furnishing 90% or more of their
services in either the inpatient or emergency department of a hospital
• Place of service (POS) code:• 21 (Inpatient Hospital), or• 23 (Emergency Room, Hospital)
MedicaidEligible if not hospital-based and minimum 30% Medicaid volume (exception, 20% for pediatricians):• Physicians• Nurse Practitioners (NPs)• Certified Nurse-Midwives (CNMs)• Dentists
Eligible without hospital-based exclusion: • Physician Assistants (PAs) working
in a Federally Qualified Health Center (FQHC) or Rural Health Centers (RHC) led by a PA with minimum 30% patient volume attributable to needy patients.
18
Eligible Professionals (EPs) that qualify can receive only Medicare or Medicaid incentive payments, not both
Verify Eligibility: Professionals

Patient Volume
• One member, one provider, same day – one encounter
• A “proxy” at the clinic level is acceptable, but all EPs need to be included
• Count only Medicaid not KCHIP• Passport members can be included• Methodology to include “panels”
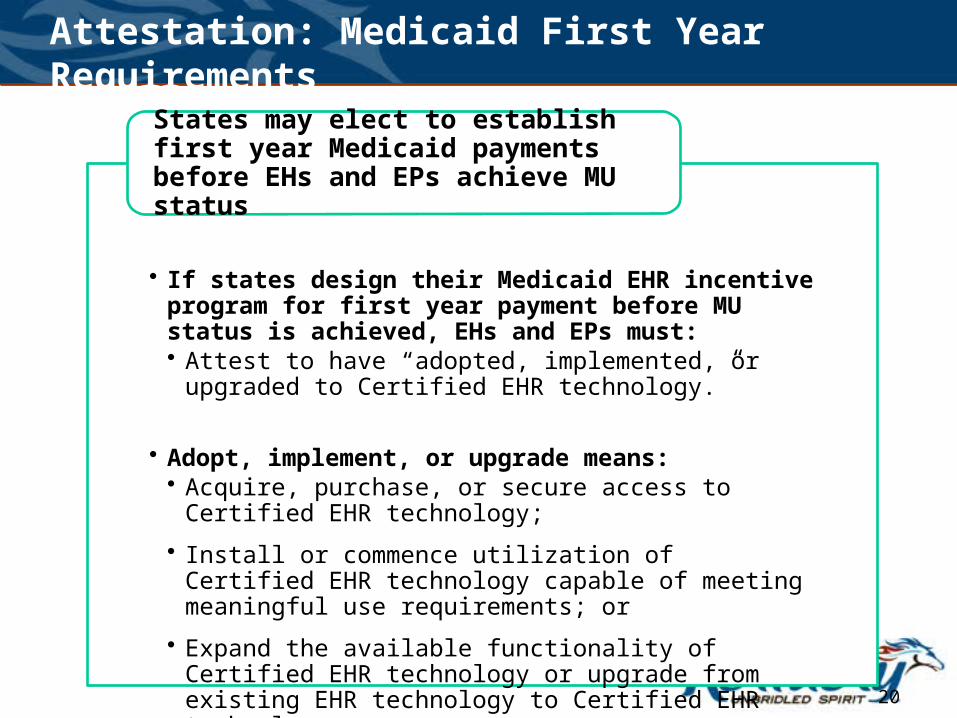
Attestation: Medicaid First Year Requirements
• If states design their Medicaid EHR incentive program for first year payment before MU status is achieved, EHs and EPs must:• Attest to have “adopted, implemented, or upgraded to
Certified EHR technology.”
• Adopt, implement, or upgrade means:• Acquire, purchase, or secure access to Certified EHR
technology;
• Install or commence utilization of Certified EHR technology capable of meeting meaningful use requirements; or
• Expand the available functionality of Certified EHR technology or upgrade from existing EHR technology to Certified EHR technology.
States may elect to establish first year Medicaid payments before EHs and EPs achieve MU status
20
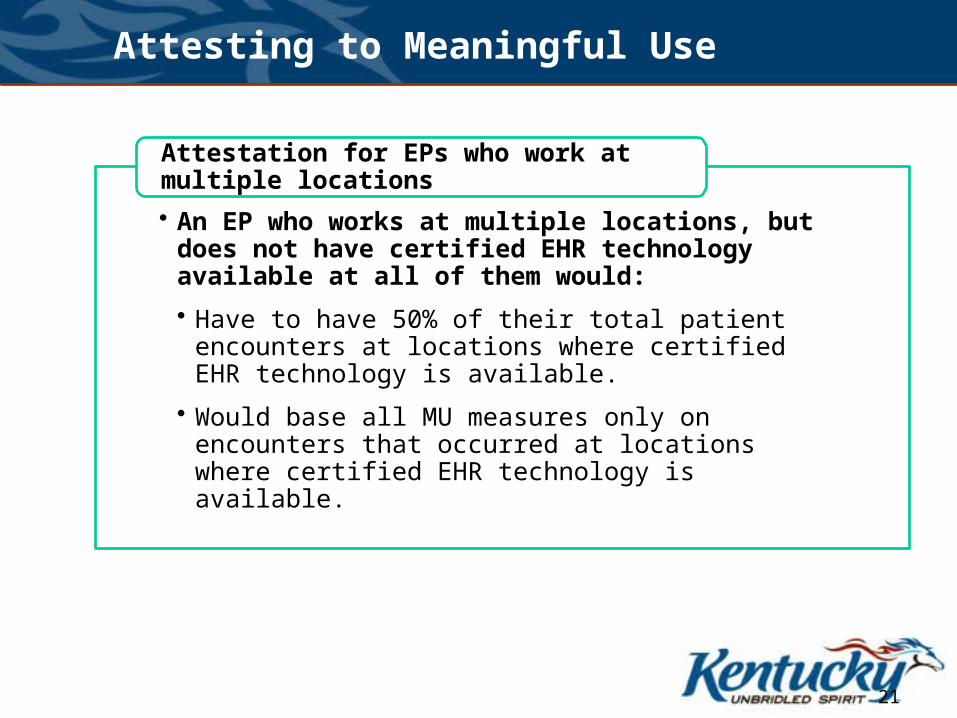
Attesting to Meaningful Use
• An EP who works at multiple locations, but does not have certified EHR technology available at all of them would:
• Have to have 50% of their total patient encounters at locations where certified EHR technology is available.
• Would base all MU measures only on encounters that occurred at locations where certified EHR technology is available.
Attestation for EPs who work at multiple locations
21

EP - AIU costs
• Medicaid pays 85% of the Net Average Allowable cost.
• Can include costs from the past.• Hardware, software, connectivity,
training, initial data entry, practice workflow redesign
• Maintain auditable records
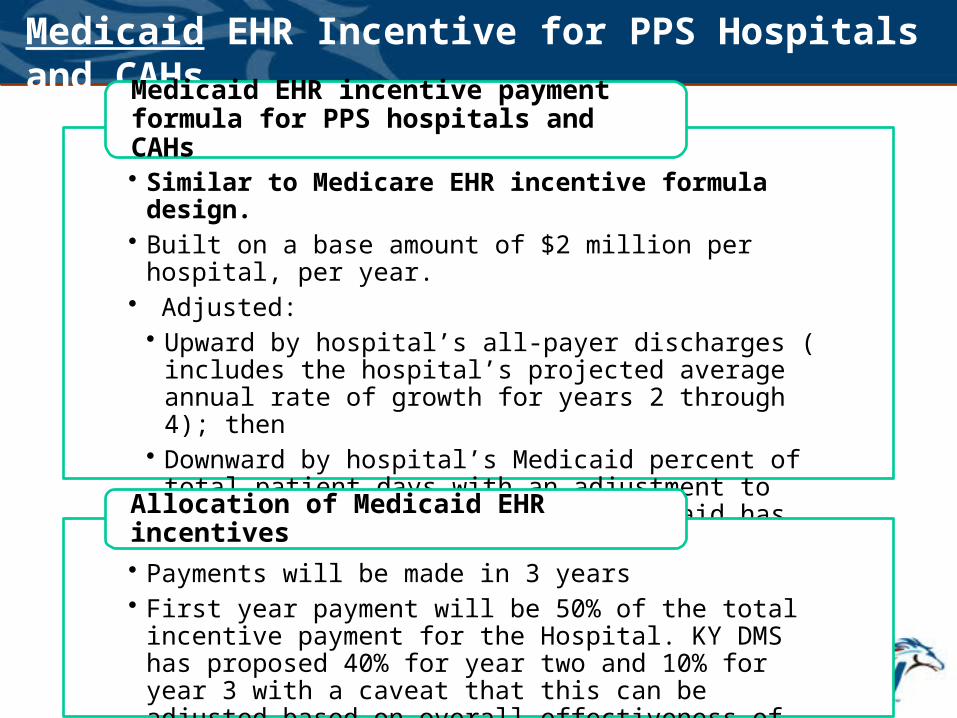
Medicaid EHR Incentive for PPS Hospitals and CAHs
• Similar to Medicare EHR incentive formula design.• Built on a base amount of $2 million per hospital, per year.• Adjusted:• Upward by hospital’s all-payer discharges ( includes the
hospital’s projected average annual rate of growth for years 2 through 4); then
• Downward by hospital’s Medicaid percent of total patient days with an adjustment to account for charity care (KY medicaid has proposed using the DISH payment K-MAP4 form).
Medicaid EHR incentive payment formula for PPS hospitals and CAHs
• Payments will be made in 3 years• First year payment will be 50% of the total incentive payment
for the Hospital. KY DMS has proposed 40% for year two and 10% for year 3 with a caveat that this can be adjusted based on overall effectiveness of the program.
Allocation of Medicaid EHR incentives
Register for EHR Incentive Program
• CMS will establish on-line provider registration as early as January 2011• http://www.cms.gov/EHRIncentivePrograms/
• Eligible hospitals and physicians and other professionals should register even before they are meaningful users.
Electronic registration
24
“We frequently talk about health IT with an emphasis on the technology.
But at the heart of the transformation of our health system, it’s really all
about people.
Above all, it’s about improving care for all Americans.”
Dr. Charles Friedman

More information on the KHIE can be found on the Governor’s Office of Electronic Health Information
website at
http://chfs.ky.gov/os/goehi/







