KZN HIV and AIDS Spending Assessment: Preliminary Findings
Presented by Dr F. NdlovuOFFICE OF THE PREMIER
.
PROVINCIAL COUNCIL ON AIDS MEETING
25 AUGUST 2010

Outline
Methodology Total HIV and AIDS spending in KZN (public,
external & private but business limited) Sources Agents Activities Providers Beneficiaries
DOH spending on HIV and AIDS DOH voted funds for HIV and AIDS DOH CG for HIV and AIDS
Objectives of NASA in KZN To identify all the sources of financing for HIV and AIDS and
TB in KZN, for the years 2007/08 and 2008/09. To measure all the public, external and private financial
resources allocated/ committed and spent for HIV and AIDS and TB activities in KZN, for the years 2007/08 and 2008/09.
To identify the providers of the HIV and AIDS and TB services in KZN, for the years 2007/08 and 2008/09.
To identify the activities on which the funds were spent, according to the NASA classifications and the PSP priorities, for the years 2007/08 and 2008/09.
To identify the beneficiaries of the spending on HIV and AIDS and TB activities in KZN, for the years 2007/08 and 2008/09.
To make recommendations for the improved targeting of funds and efficiency of spending, according to the provincial priorities.
Methodology Aimed to include data from all sources, from all
agents and from sampled service providers. All DOH & PPSD & NHLS expenditure by activity and
service provider – from BAS records Verified with small sample of clinics / hospitals /
pharmacists / NGOs receiving DOH and /or DSD grants DOE – provided detailed expenditure of lifeskills CG DSD – did not provide BAS expenditure, so had to use
the audited expenditure amounts from budget documents and split between OVC, HBC, M&E, planning & coord, training, social services – excludes the payments made on grants (national level analysis).
Methodology cont. Other govt departments were interviewed: agriculture,
OP, treasury – they were unable to provide any HIV-specific spending.
Public wellness programme - there was no HIV-specific spending in the study years, they are creating it currently.
External sources – data obtained from EU, GF & donors to DOH only.
Missing all other external partners since they indicated that their expenditure would be obtained from Head Offices.
Missing private medical aid & insurances indicated that their expenditure would be obtained from Head Offices.
Missing: spending of most municipalities, mortuaries & C. Sections.

Methodology cont. Business sector – only DCC & SABCOAH & McCarthy
provided data, many did not respond and some indicated that their Head Offices would have to provide the data.
NGOs: were sampled from 911 database – many were not contactable, and eventually only about 60 provided data.
Research institutions – contacted: MRC, HSRC, HST, HEARD, HIVAN, RHRU, PASCA, McCord Hospt, Nelson Mandela Med.School – only got data from MRC & HEARD.
To be collected at national level – blood safety, condoms (the numbers of condoms distributed were not obtained from HAST so could not be estimated), correctional health services, private medical insurances, businesses & external funders.
DRAFT - DO NOT DISSEMINATE.
Methodology cont Data collection through interviews &
expenditure record verification. Data triangulation to ensure correct actual
expenditure. Also avoided double counting through
triangulation & creating transactions. Data cleaned and captured in Excel. Exported to NASA RTS where aggregated
and matrices produced. All analysis & graphs generated in excel.
Total Spending on HIV and AIDS in KZN
All public, external & some private (business limited)
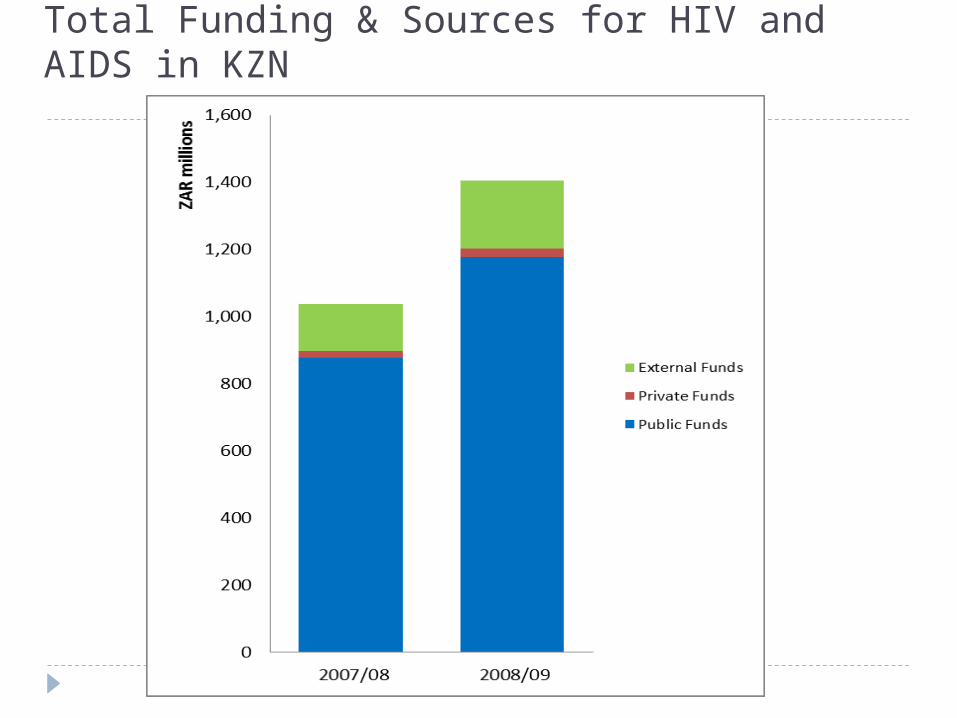
Total Funding & Sources for HIV and AIDS in KZN
DRAFT - DO NOT DISSEMINATE.

Sources of all HIV spending in KZN – further disaggregated 2007/08 & 2008/09
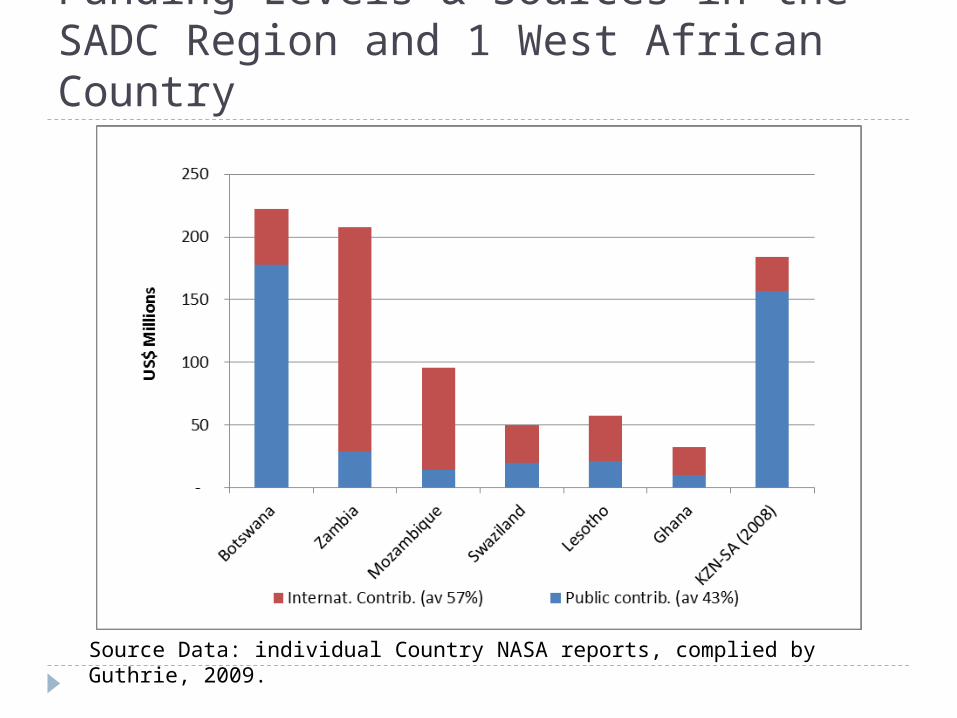
Funding Levels & Sources in the SADC Region and 1 West African Country
Source Data: individual Country NASA reports, complied by Guthrie, 2009.
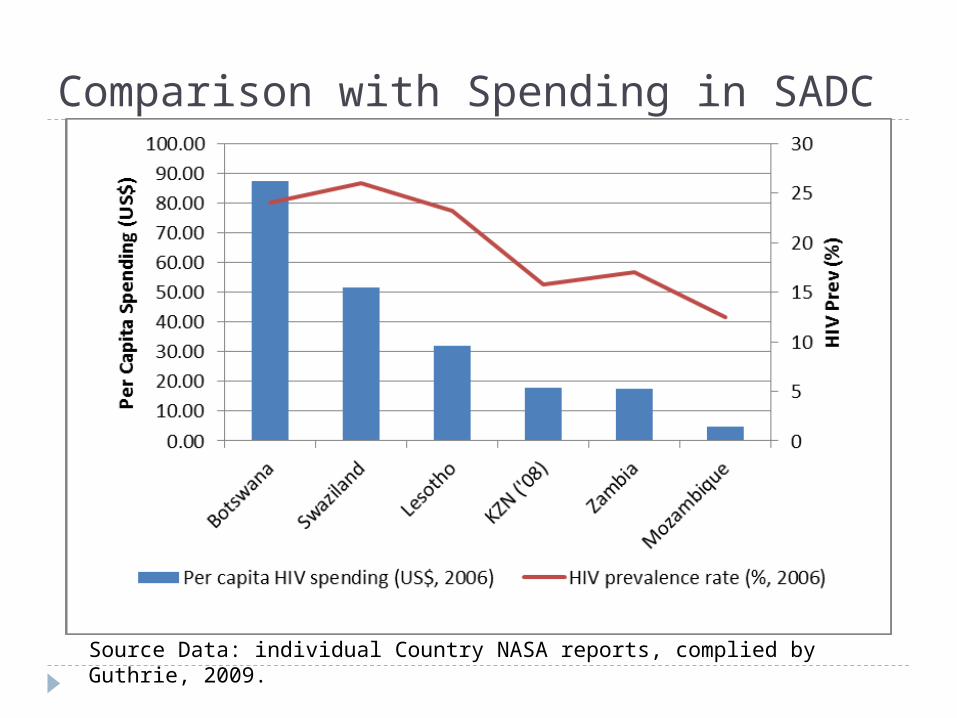
Comparison with Spending in SADC
Source Data: individual Country NASA reports, complied by Guthrie, 2009.

Multilateral AID for HIV and AIDS in KZN 2007/08 & 2008/09
0
20
40
60
80
100
120
140
160
2007/08 2008/09
ZAR
mill
iions
WHO
UNAIDS
Global Fund
European Commission
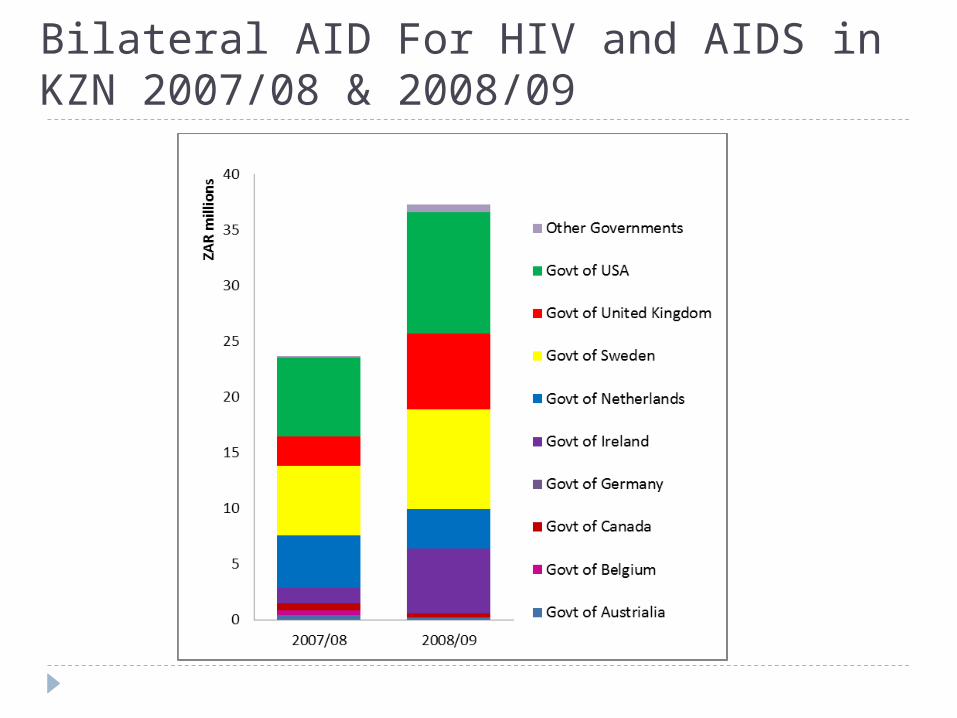
Bilateral AID For HIV and AIDS in KZN 2007/08 & 2008/09

External Foundation AID for HIV and AIDS in KZN 2007/08 & 2008/09
Agents of Spending The managers of funds – receive and send on
to providers. Decide programmatic spending. Eg. GF – CCM assumed principal recipient is
the agent But for EU funds, EU is the agent
DRAFT - DO NOT DISSEMINATE.
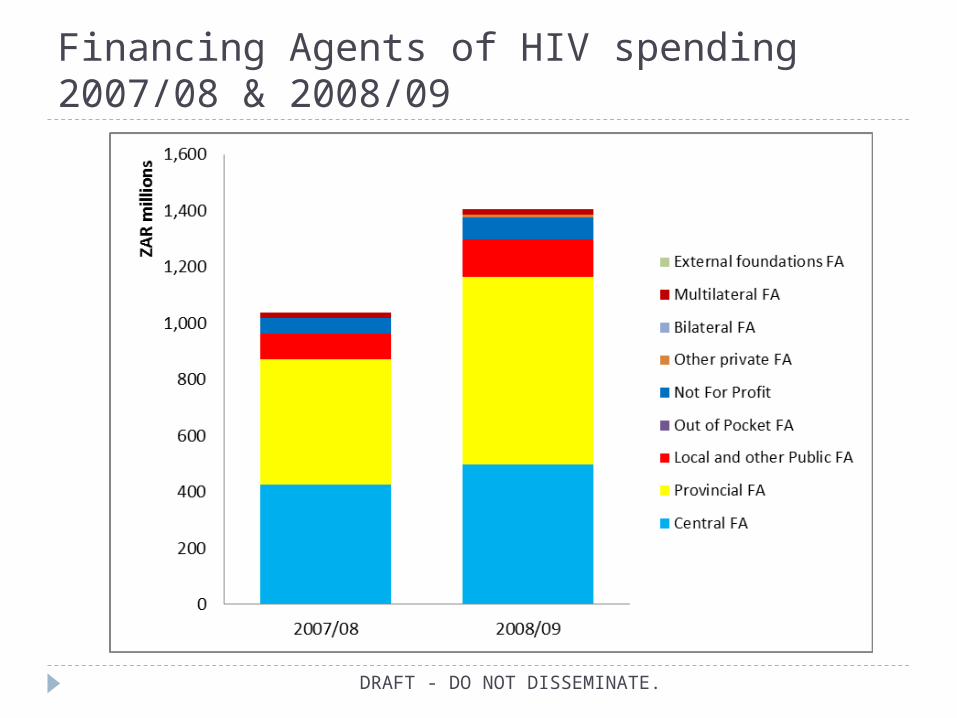
Financing Agents of HIV spending 2007/08 & 2008/09
DRAFT - DO NOT DISSEMINATE.
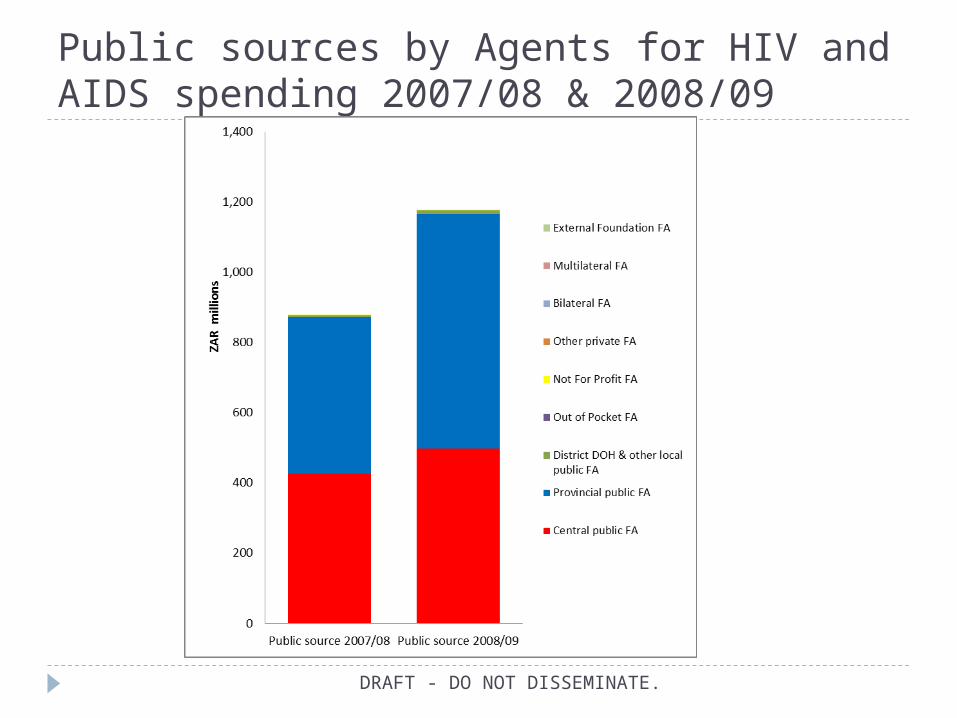
Public sources by Agents for HIV and AIDS spending 2007/08 & 2008/09
DRAFT - DO NOT DISSEMINATE.
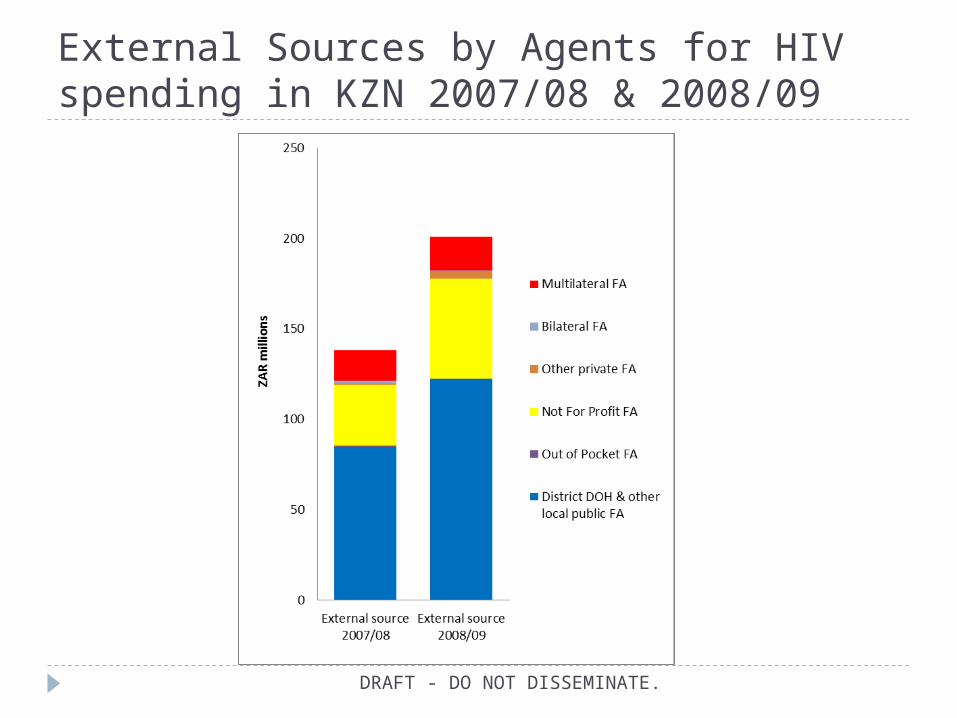
External Sources by Agents for HIV spending in KZN 2007/08 & 2008/09
DRAFT - DO NOT DISSEMINATE.

HIV and AIDS Spending Activities NASA classifications:
Prevention Treatment and care OVCs Policy, management and coordination Human Resources Social services & Protection Enabling environment Research
Each have several sub-components

Total KZN HIV and AIDS Spending Activities

Comparison with Activities in SADC
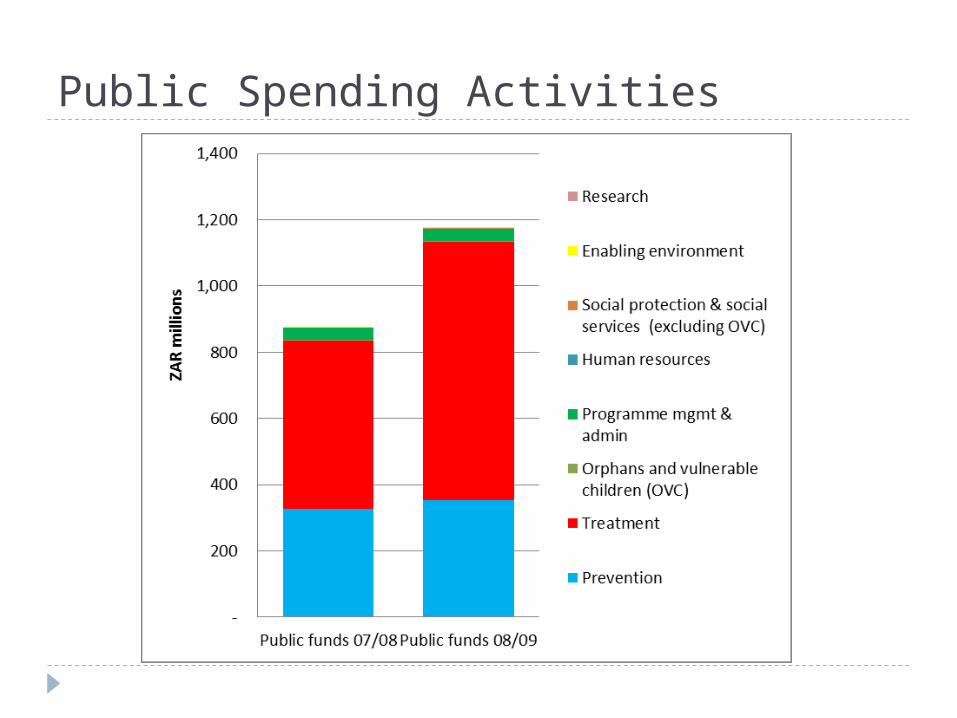
Public Spending Activities
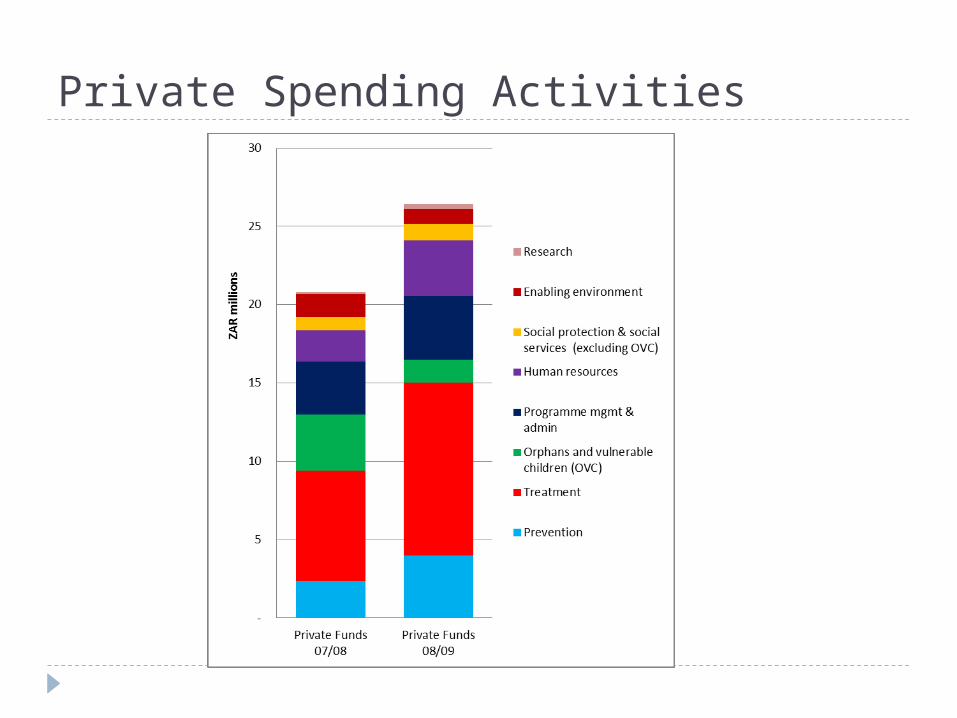
Private Spending Activities
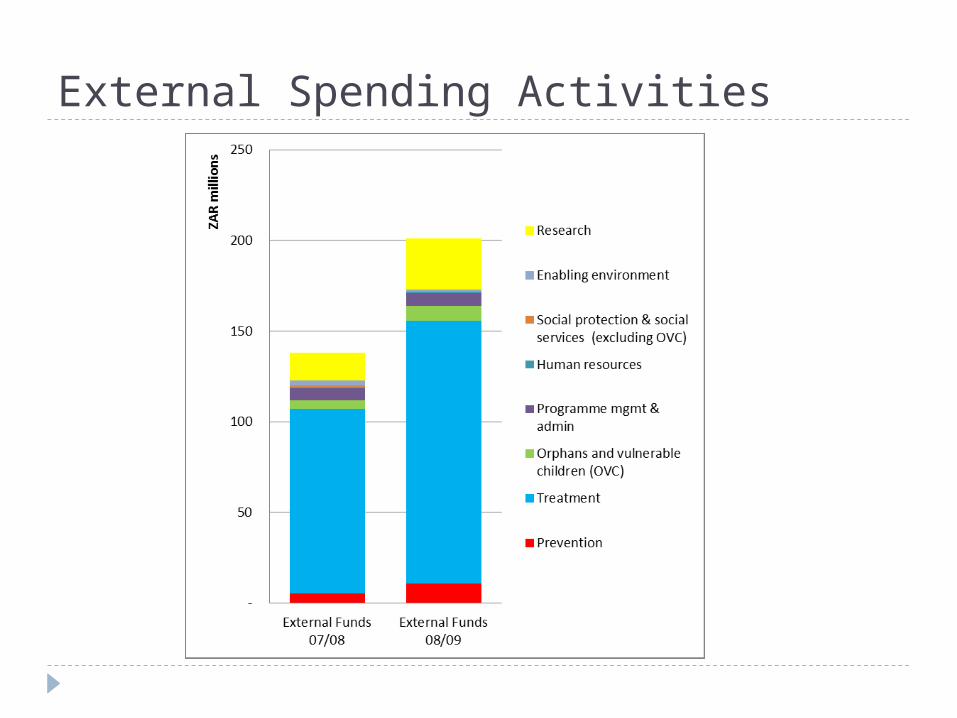
External Spending Activities
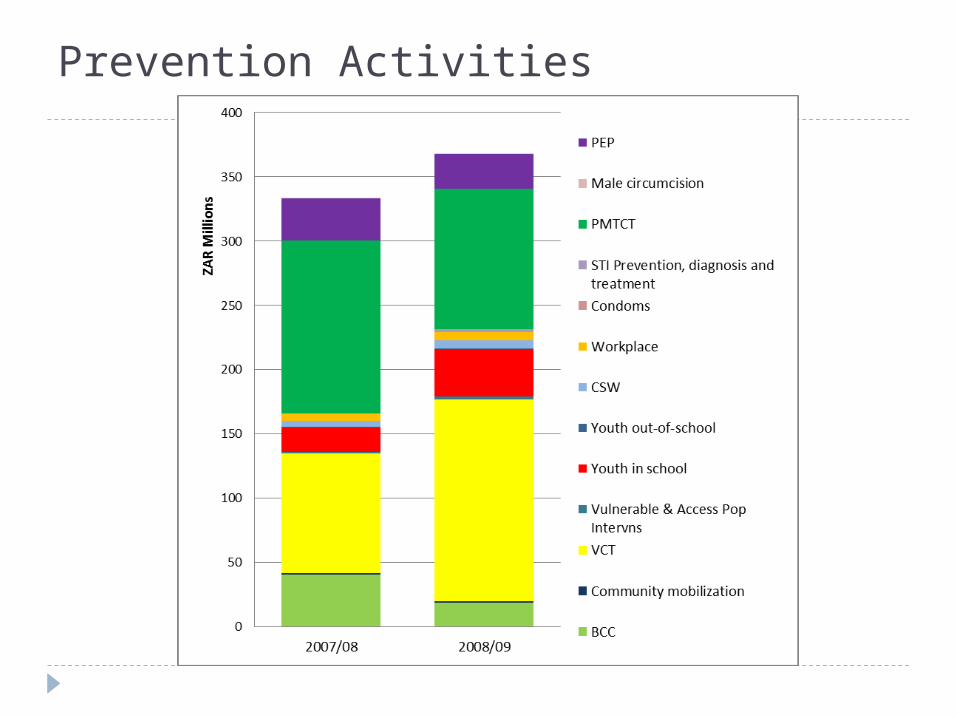
Prevention Activities

Treatment Activities
DRAFT - DO NOT DISSEMINATE.
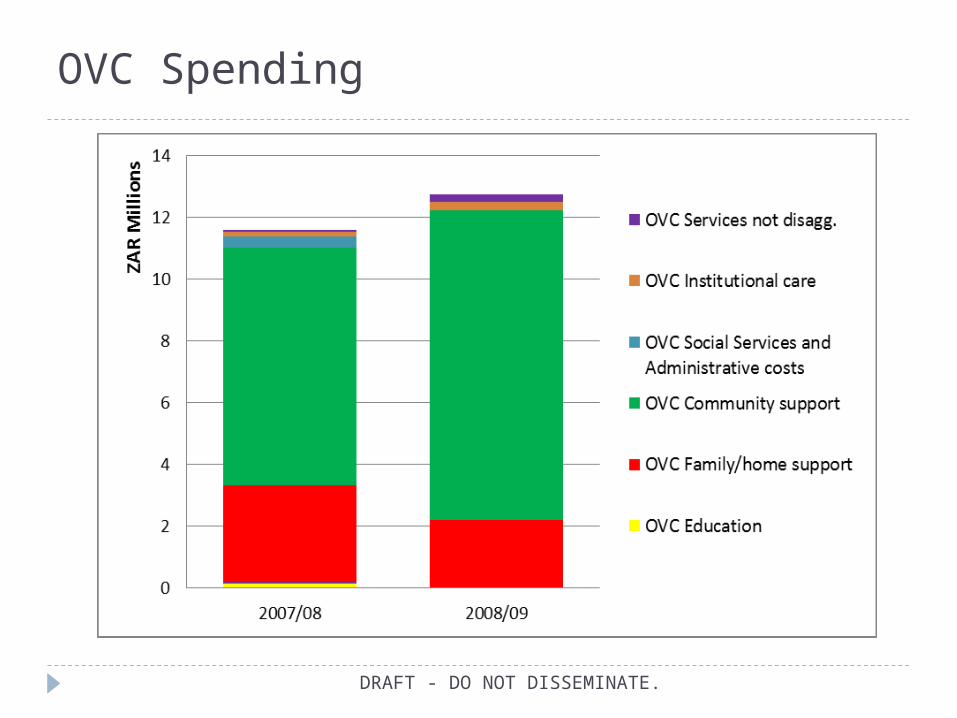
OVC Spending
DRAFT - DO NOT DISSEMINATE.
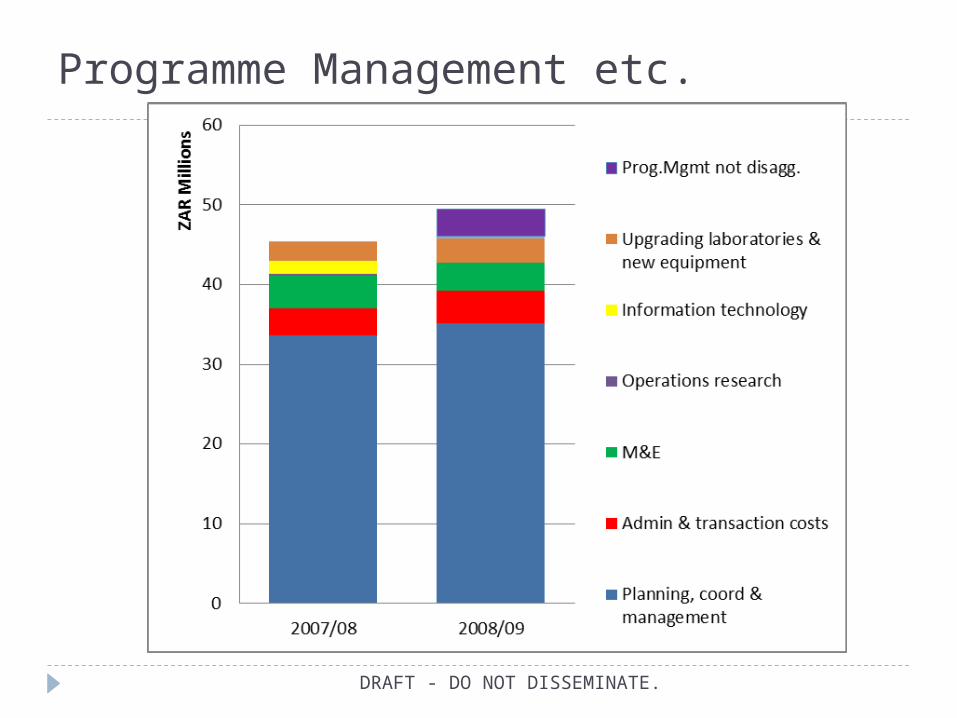
Programme Management etc.
DRAFT - DO NOT DISSEMINATE.
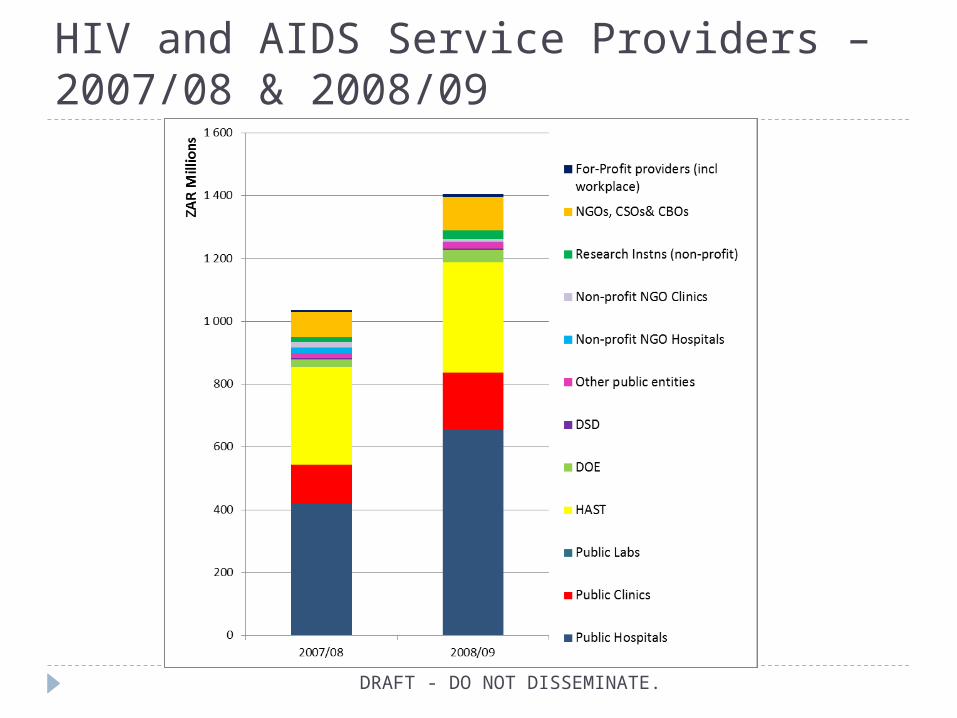
HIV and AIDS Service Providers – 2007/08 & 2008/09
DRAFT - DO NOT DISSEMINATE.
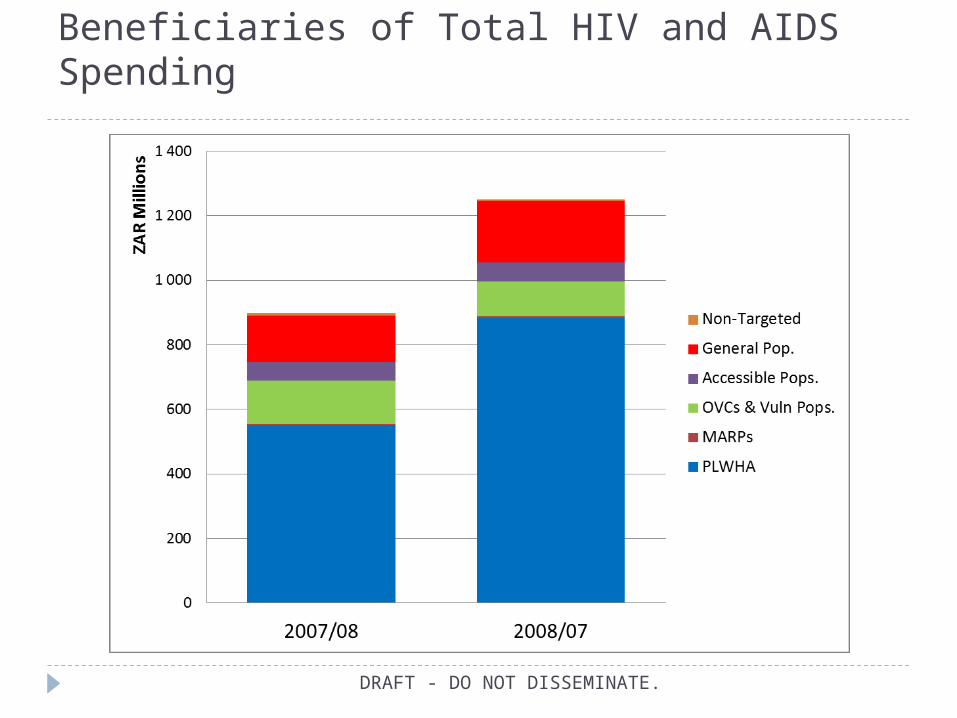
Beneficiaries of Total HIV and AIDS Spending
DRAFT - DO NOT DISSEMINATE.

Beneficiaries of HIV and AIDS Services 2007/08
DRAFT - DO NOT DISSEMINATE.

Beneficiaries by Activity (2008/09)
DRAFT - DO NOT DISSEMINATE.
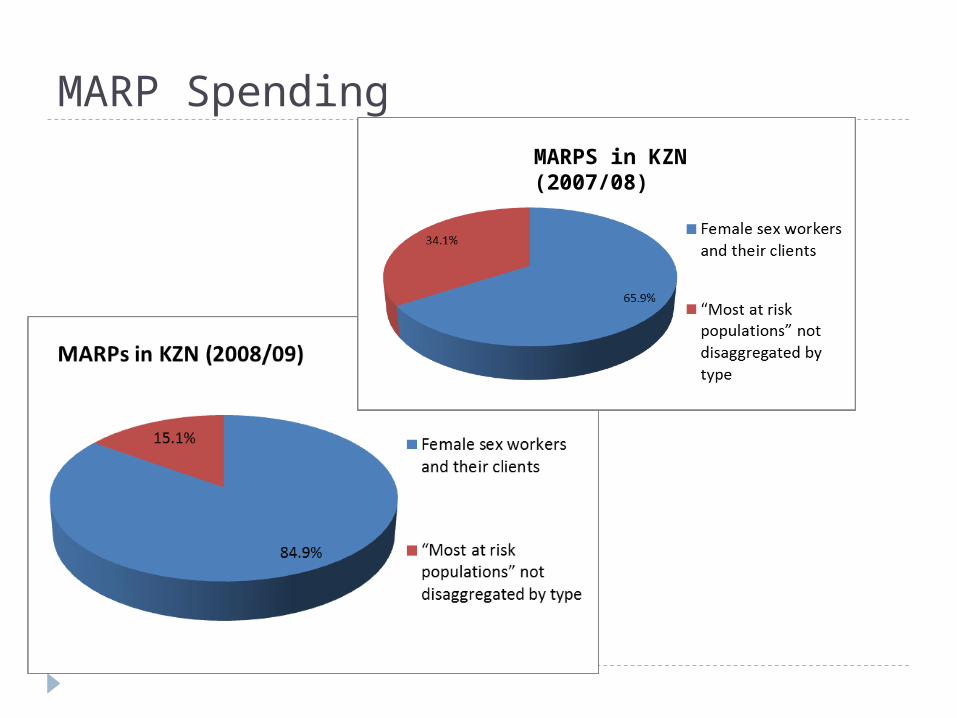
MARP SpendingMARPS in KZN (2007/08)

OVCs & Vulnerable Groups
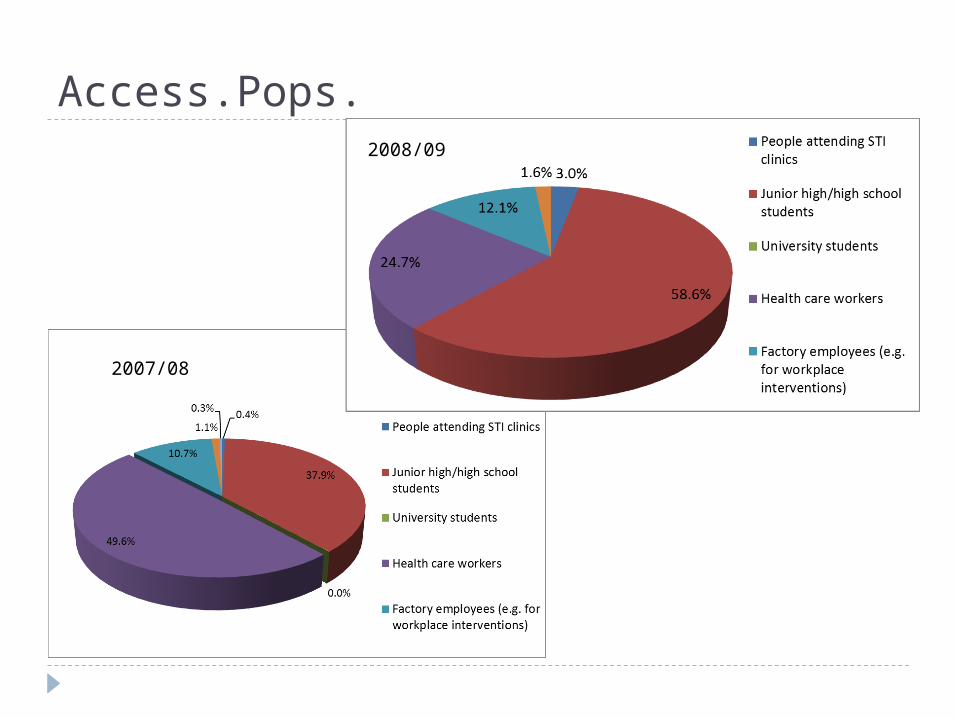
Access.Pops.
2007/08
2008/09

DOH HIV and AIDS Spending in KZN
DOH Comprehensive Conditional Grant for HIV and AIDS
DRAFT - DO NOT DISSEMINATE.
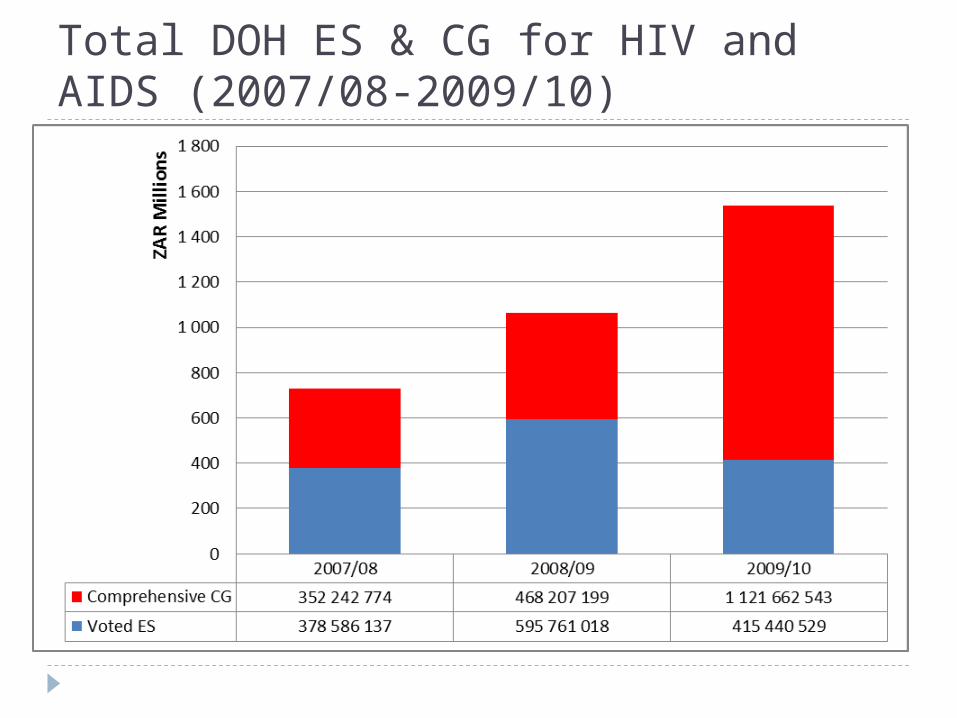
Total DOH ES & CG for HIV and AIDS (2007/08-2009/10)
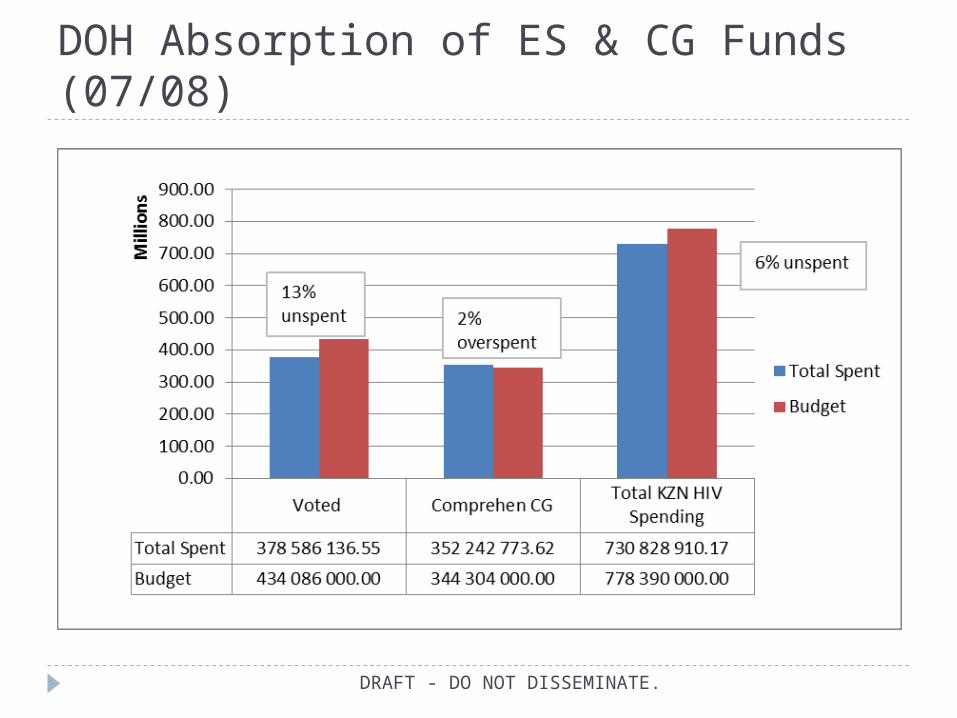
DOH Absorption of ES & CG Funds (07/08)
DRAFT - DO NOT DISSEMINATE.
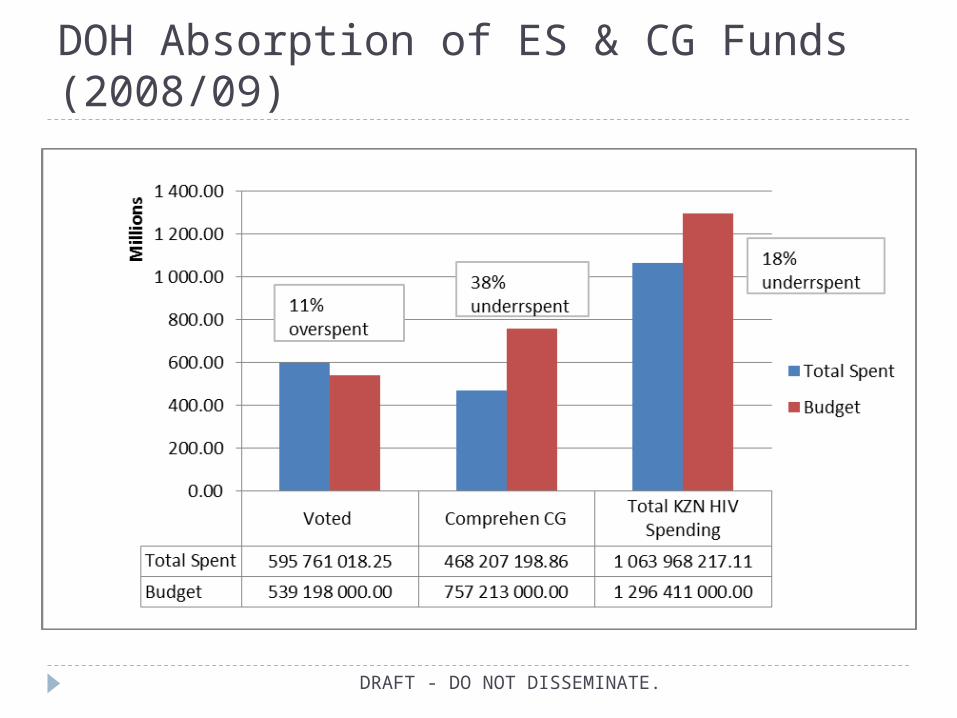
DOH Absorption of ES & CG Funds (2008/09)
DRAFT - DO NOT DISSEMINATE.

DOH Absorption of ES & CG Funds (2009/10)
DRAFT - DO NOT DISSEMINATE.

KZN DOH CG Spending by Activity 2007/08 & 08/09
DRAFT - DO NOT DISSEMINATE.
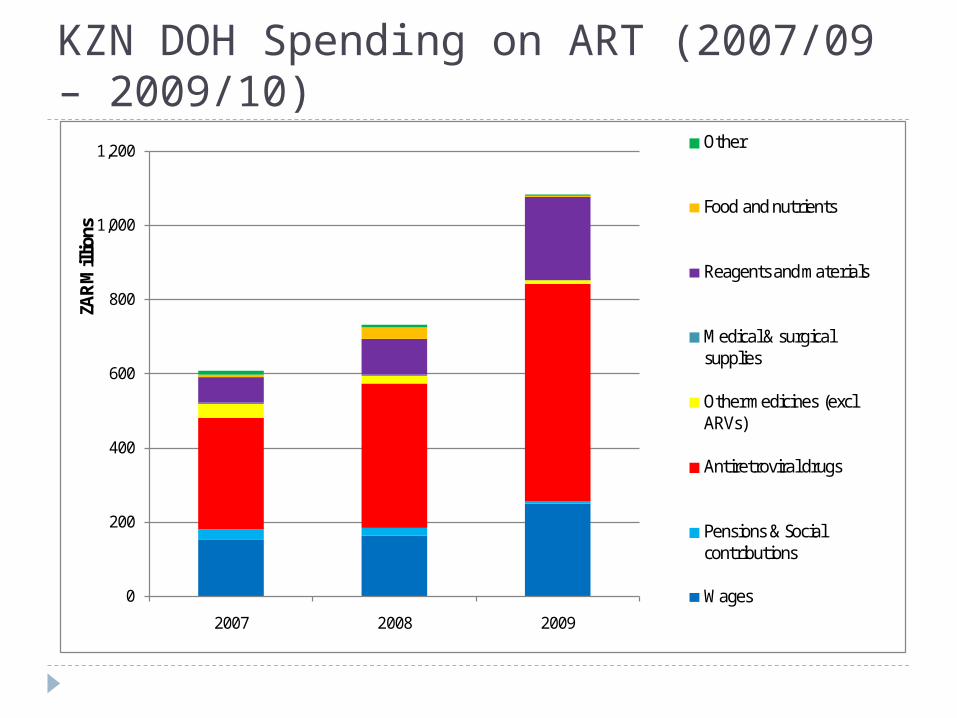
KZN DOH Spending on ART (2007/09 – 2009/10)
0
200
400
600
800
1,000
1,200
2007 2008 2009
ZAR
Mill
ions
Other
Food and nutrients
Reagents and materials
Medical & surgical supplies
Other medicines (excl ARVs)
Antiretroviral drugs
Pensions & Social contributions
Wages
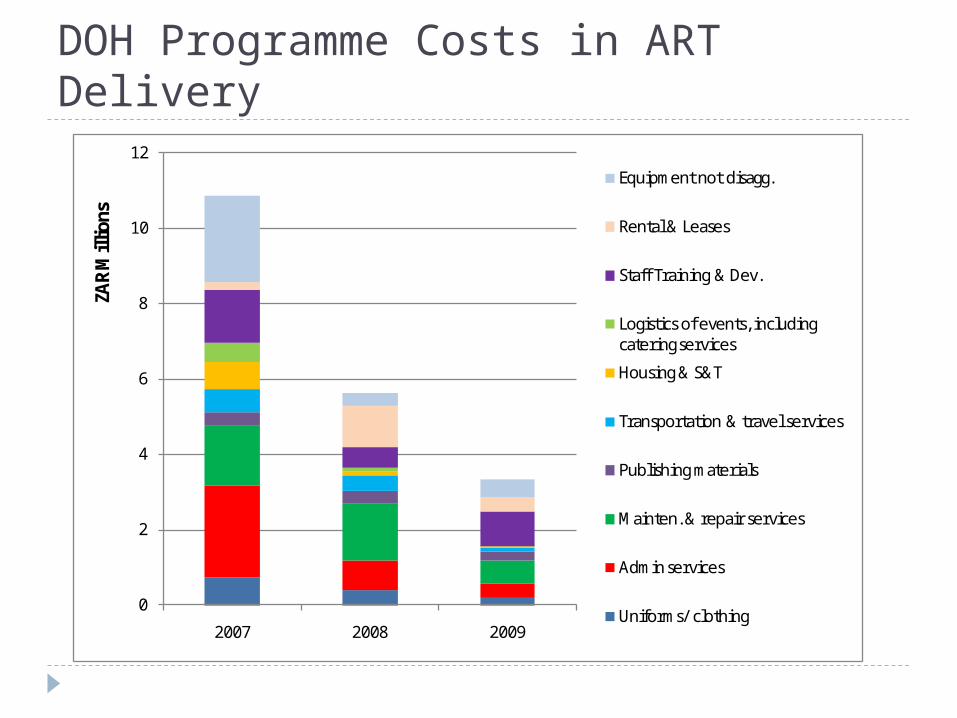
DOH Programme Costs in ART Delivery
0
2
4
6
8
10
12
2007 2008 2009
ZAR
Mill
ions
Equipment not disagg.
Rental & Leases
Staff Training & Dev.
Logistics of events, including catering services
Housing & S&T
Transportation & travel services
Publishing materials
Mainten. & repair services
Admin services
Uniforms/ clothing
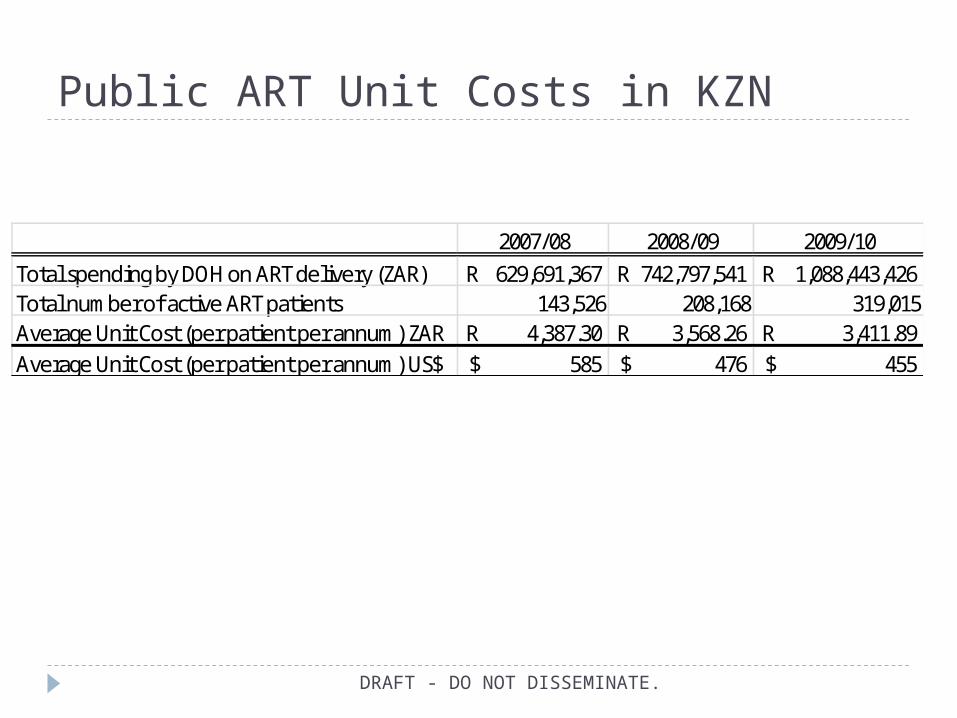
Public ART Unit Costs in KZN
DRAFT - DO NOT DISSEMINATE.
2007/08 2008/09 2009/10Total spending by DOH on ART delivery (ZAR) 629,691,367R 742,797,541R 1,088,443,426R Total number of active ART patients 143,526 208,168 319,015Average Unit Cost (per patient per annum) ZAR 4,387.30R 3,568.26R 3,411.89R Average Unit Cost (per patient per annum) US$ 585$ 476$ 455$
KZN DOH Voted Funds for HIV and AIDS
DRAFT - DO NOT DISSEMINATE.
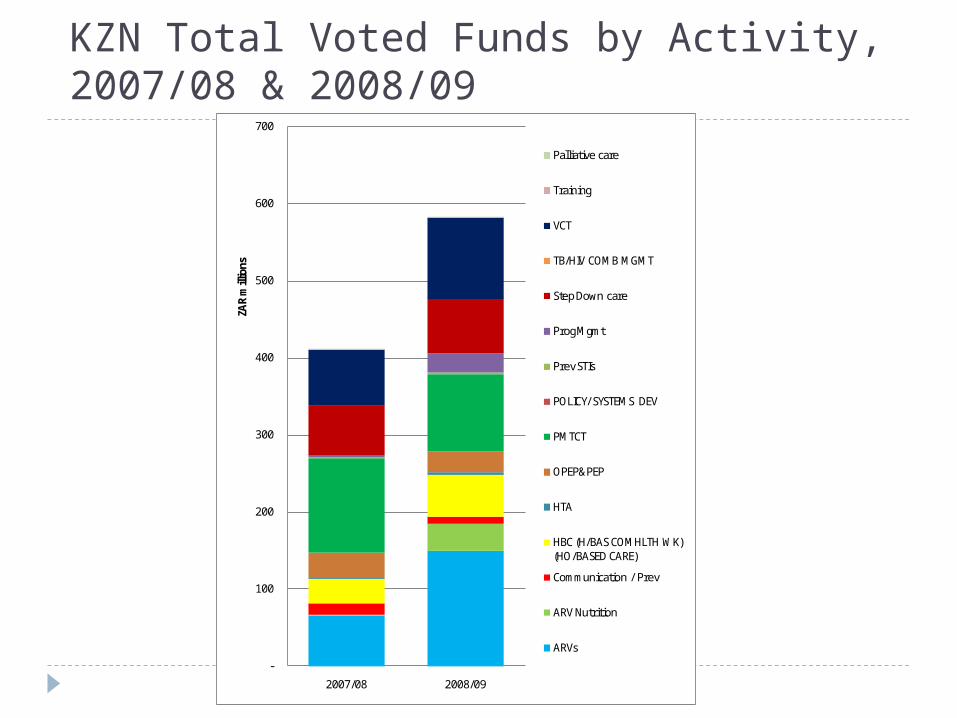
KZN Total Voted Funds by Activity, 2007/08 & 2008/09
DRAFT - DO NOT DISSEMINATE.-
100
200
300
400
500
600
700
2007/08 2008/09
ZAR
mill
ions
Palliative care
Training
VCT
TB/HIV COMB MGMT
Step Down care
Prog Mgmt
Prev STIs
POLICY/ SYSTEMS DEV
PMTCT
OPEP&PEP
HTA
HBC (H/BAS COMHLTH WK) (HO/BASED CARE)
Communication / Prev
ARV Nutrition
ARVs
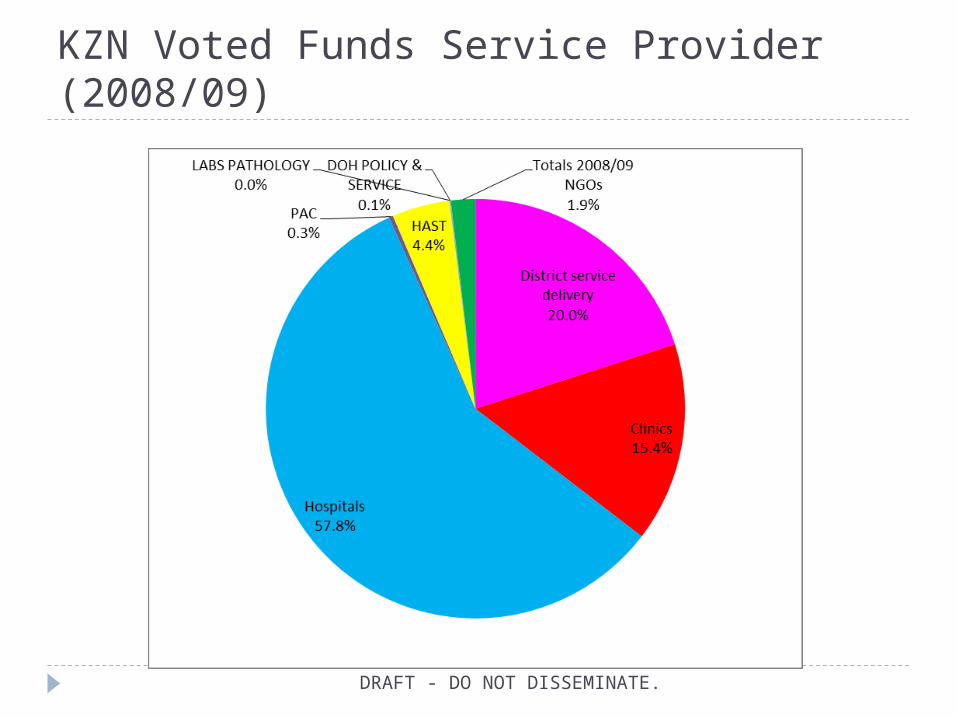
KZN Voted Funds Service Provider (2008/09)
DRAFT - DO NOT DISSEMINATE.

KZN District Service Delivery Voted Funds for HIV and AIDS (%) (2007/08-2008/09)
DRAFT - DO NOT DISSEMINATE.
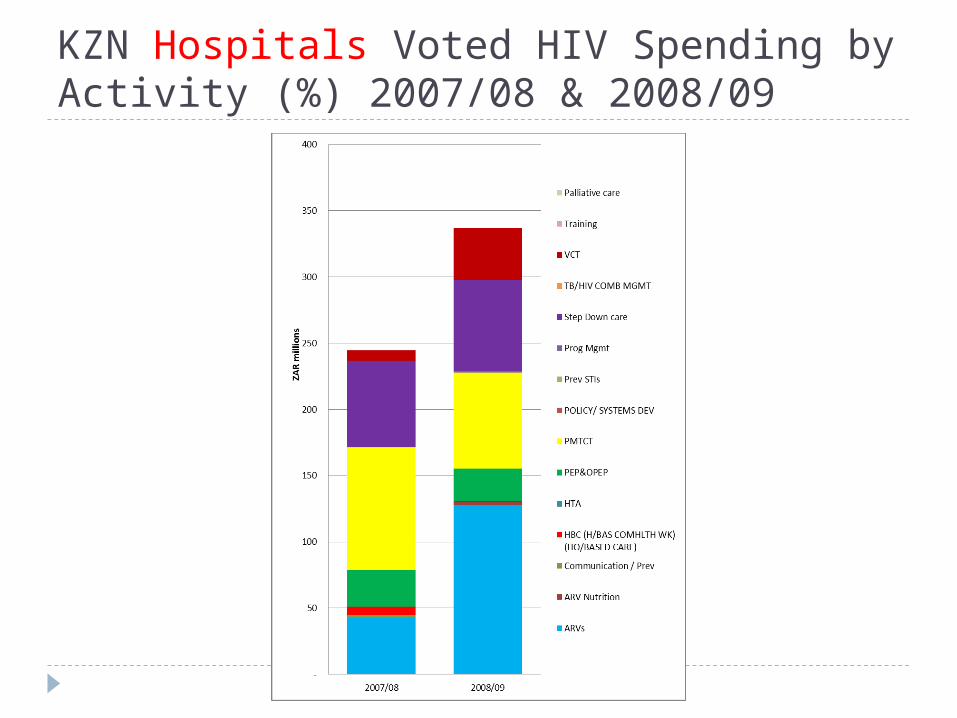
KZN Hospitals Voted HIV Spending by Activity (%) 2007/08 & 2008/09
DRAFT - DO NOT DISSEMINATE.

KZN Public Clinics Voted HIV and AIDS Spending (%)
DRAFT - DO NOT DISSEMINATE.
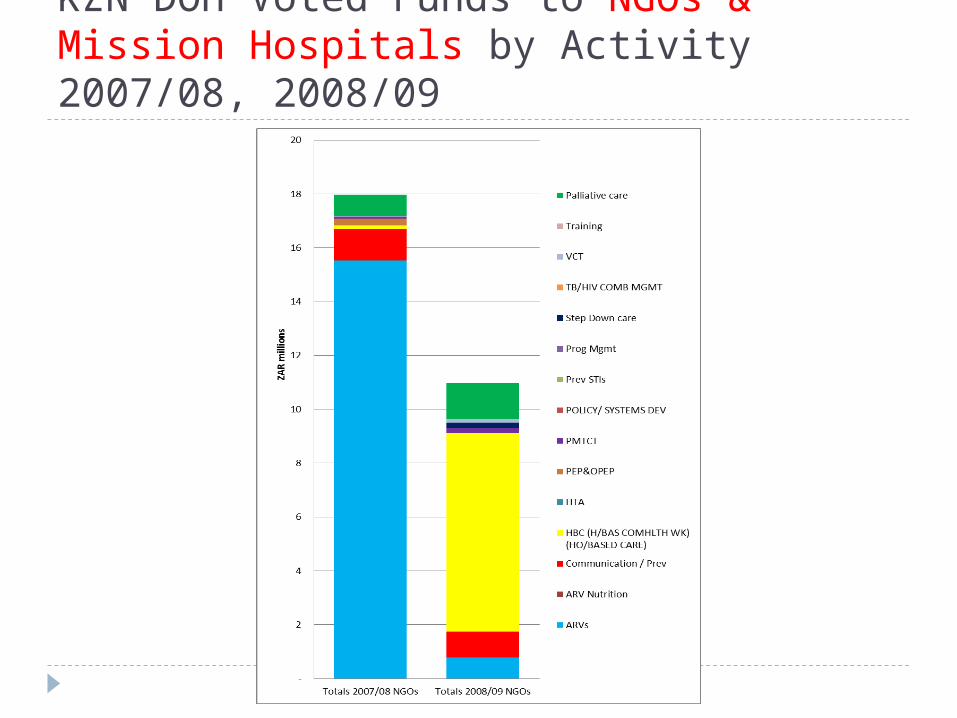
KZN DOH Voted Funds to NGOs & Mission Hospitals by Activity 2007/08, 2008/09
DRAFT - DO NOT DISSEMINATE.

KZN DOH CG for HIV and AIDS
DRAFT - DO NOT DISSEMINATE.

DOH CG HIV and AIDS Spending Activities
DRAFT - DO NOT DISSEMINATE.
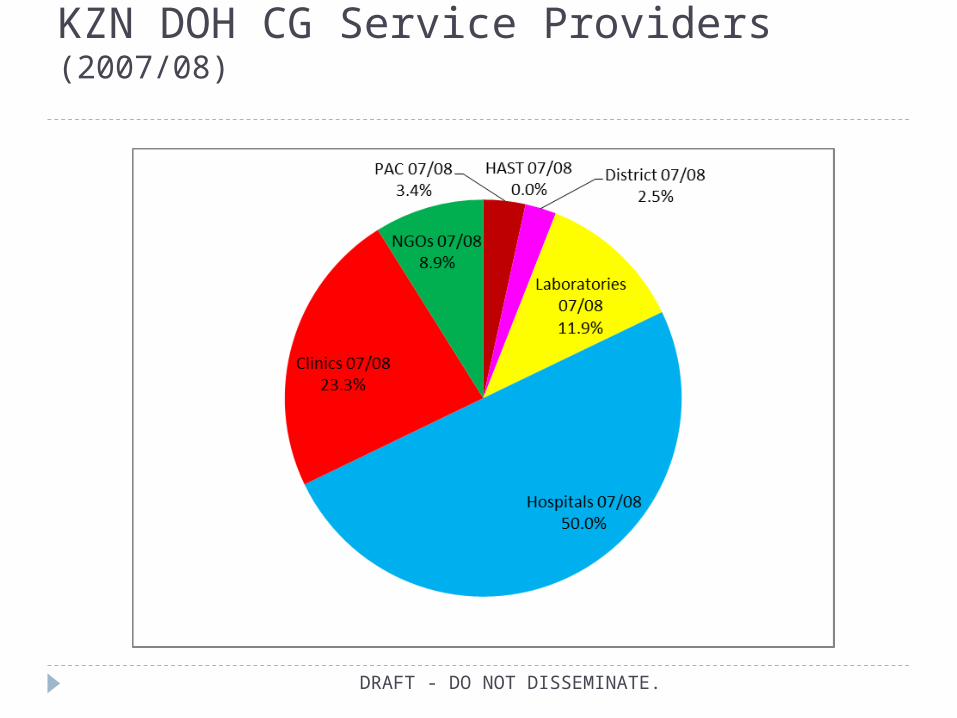
KZN DOH CG Service Providers (2007/08)
DRAFT - DO NOT DISSEMINATE.

KZN DOH CG Service Providers (2008/09)
DRAFT - DO NOT DISSEMINATE.

DRAFT - DO NOT DISSEMINATE.
KZN HAST HIV CG Spending (2007/08 & 2008/09)

DRAFT - DO NOT DISSEMINATE.
-50
-
50
100
150
200
250
300
350
Hospitals 07/08 Hospitals 08/09
ZAR
mill
ions
VCT
Step Down care
Prog Mgmt
PMTCT
PEP& OPEP
HTA
HBC
Communications/ Prev
ARV Nutrition
ARVs
KZN Hospital HIV CG Spending (2007/08 & 2008/09)
DRAFT - DO NOT DISSEMINATE.
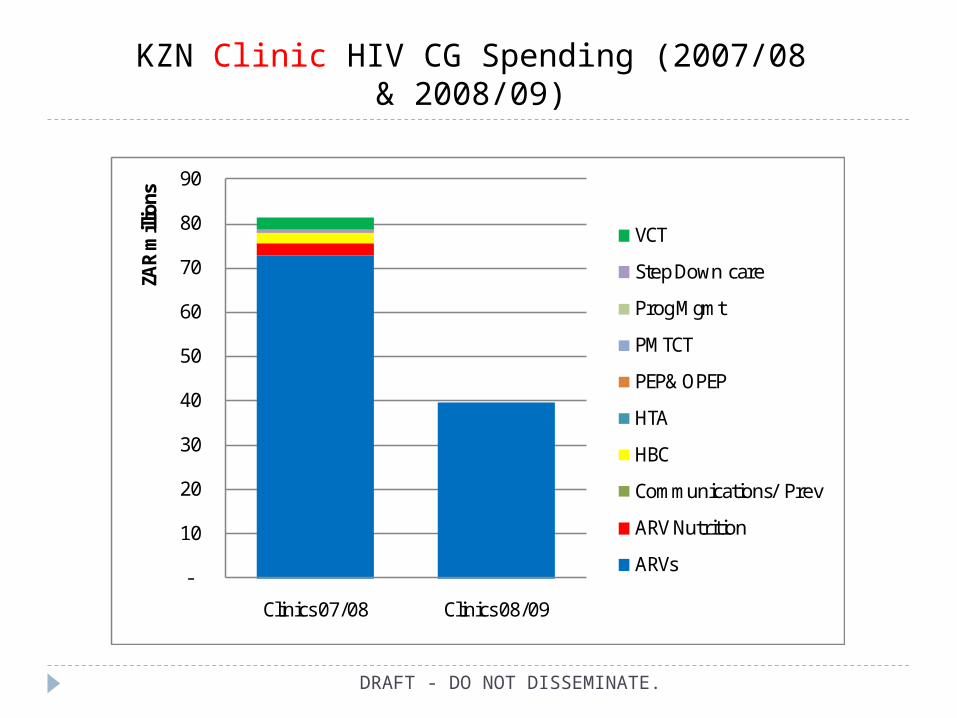
KZN Clinic HIV CG Spending (2007/08 & 2008/09)
-
10
20
30
40
50
60
70
80
90
Clinics 07/08 Clinics 08/09
ZAR
mill
ions
VCT
Step Down care
Prog Mgmt
PMTCT
PEP& OPEP
HTA
HBC
Communications/ Prev
ARV Nutrition
ARVs
DRAFT - DO NOT DISSEMINATE.
-
5
10
15
20
25
30
35
NGOs 07/08 NGOS 08/09
ZAR
mill
ions
VCT
Step Down care
Prog Mgmt
PMTCT
PEP& OPEP
HTA
HBC
Communications/ Prev
ARV Nutrition
ARVs
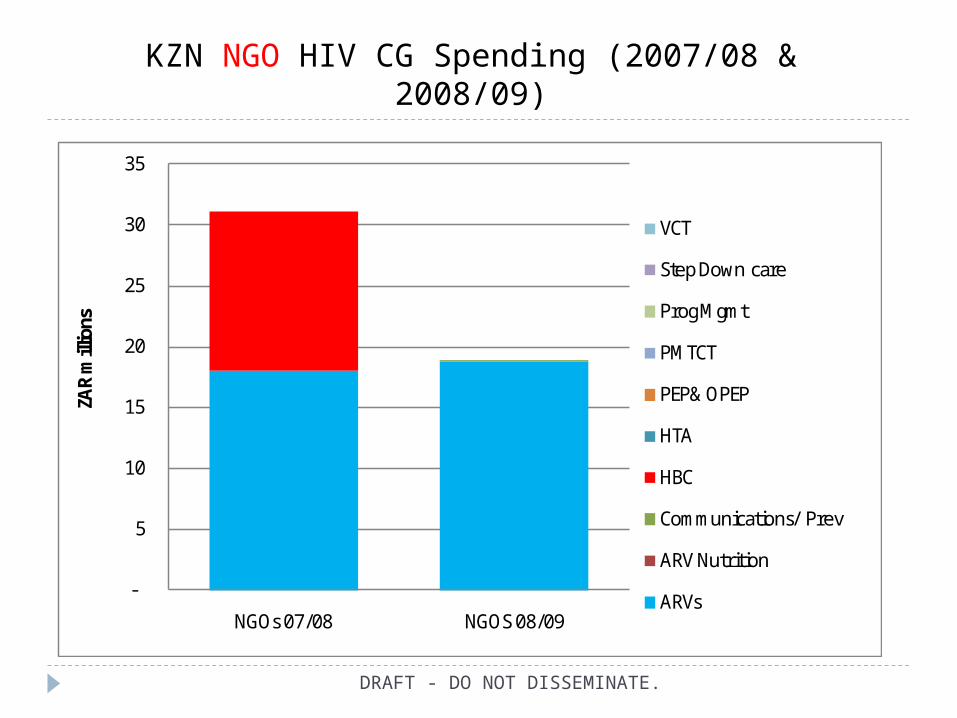
KZN NGO HIV CG Spending (2007/08 & 2008/09)
Currently the response in KZN is dominated by spending by DOH - Greater inter-sectoral effort required
More funds needed for prevention activities such as BCC, community mobilisation, male circumcision, PMTCT, youth interventions and VCT, and potentially microbicides
Prevention efforts increased for MARPs, while also attempting to address SA’s key modes of transmission
TB prophylaxis roll-out important with greater integration of TB and HIV and AIDS services
Other priority areas: OVC, Social mitigation, Enabling environment, Research – underfunded
Increased implementation of workplace wellness programmes
Additional resources for infrastructural development
DRAFT - DO NOT DISSEMINATE.
Key Points & Recommendations (1)

Key Points & Recommendations (2) Voted DOH funds should continue to target other important
interventions i.e HBC, BCC,STI prevention and VCT because CG is devoted to ART
If KZN is reducing its ES for HIV and AIDS, then the CG must also cover these important interventions other than ART
More funds needed for HBC, step-down care & palliative care – best provided through NGOs
Greater treatment efficiencies in spending – lower tender drug prices, task shifting, step-down, clinic level delivery
Skilled and professional health workers required at the district level, but require adequate recompense to retain their skills
DRAFT - DO NOT DISSEMINATE.
NGOs & CBOs play important roles and could be strengthened and expanded
DSD & DOH need to increase & standardize stipends to HBC volunteers
Financing and reporting requirements for NPOs need to be harmonized
Greater collaboration between provincial managers and district officials required in budget planning processes
An integrated Performance Budget System would greatly enhance planning, implementation & monitoring
Capacity building in data management, analysis and utilization of data in planning processes needed at district level
DRAFT - DO NOT DISSEMINATE.
Key Points & Recommendations (3)

Thank you
DRAFT - DO NOT DISSEMINATE.







