
Lecture 1Lecture 1

Human Immunodeficiency Human Immunodeficiency InfectionInfection
HIVHIV
Acquired Immunodeficiency Acquired Immunodeficiency SyndromeSyndrome
AIDS/SIDAAIDS/SIDA
HIV/SIDA/AIDSHIV/SIDA/AIDS Have you heard of thisHave you heard of this What have you heardWhat have you heard Do you know anyone who has thisDo you know anyone who has this What causes this infectionWhat causes this infection Can it be curedCan it be cured

HIV/SIDA/AIDSHIV/SIDA/AIDS Can it be curedCan it be cured Can this infection be preventedCan this infection be prevented If so how can it be preventedIf so how can it be prevented Does everyone who has it have Does everyone who has it have
symptomssymptoms
HIV and the DRCHIV and the DRC
1 of 20 nations-the highest risk HIV/AIDS1 of 20 nations-the highest risk HIV/AIDS Over 1 million infected personsOver 1 million infected persons Estimated infection incidence 2-4%Estimated infection incidence 2-4% Treatment rate <5%Treatment rate <5%
• Lack of an infrastructureLack of an infrastructure• Lack of health servicesLack of health services• Lack testing and prevention strategyLack testing and prevention strategy• Problems getting the meds to the peopleProblems getting the meds to the people• Costs $5/mo and $15 for a CD4 testCosts $5/mo and $15 for a CD4 test

HIV and the DRCHIV and the DRCAntenatal surveillance dataAntenatal surveillance data
Rates of HIV infection in pregnant womenRates of HIV infection in pregnant women Urban Kisangai (Orientale) 3-9.5%Urban Kisangai (Orientale) 3-9.5% Mwene Ditu (Kasai Orientale) 6.9Mwene Ditu (Kasai Orientale) 6.9 Matadi (Bas Congo P) 4.3Matadi (Bas Congo P) 4.3 Rural Neisu and Buta >5.0Rural Neisu and Buta >5.0

HIV does not come fromHIV does not come from• Being in the same room Being in the same room • HuggingHugging• TouchingTouching• Eating togetherEating together• Sharing clothesSharing clothes• Shopping or working togetherShopping or working together• Eating at the same tableEating at the same table

HIV/SIDA/AIDSHIV/SIDA/AIDSPreventionPrevention
Do not share razors, toothbrushesDo not share razors, toothbrushes Condoms are not totally preventive; Condoms are not totally preventive;
avoid sex with an infected personavoid sex with an infected person Where possible adequate treatment Where possible adequate treatment
to lessen risk to lessen risk Male circumcisionMale circumcision Always wear gloves when touching Always wear gloves when touching
any body fluids of anotherany body fluids of another

HIV/SIDA/AIDSHIV/SIDA/AIDSPreventionPrevention
In the hospital or any treatment facilityIn the hospital or any treatment facility All needles, surgical instruments, must All needles, surgical instruments, must
be sterilizedbe sterilized Be careful handling any blood or Be careful handling any blood or
bodily fluidsbodily fluids Blood to be transfused should be Blood to be transfused should be
tested if possibletested if possible• Lab has the ability to test bloodLab has the ability to test blood• Lab has the ability to test patientsLab has the ability to test patients

HIV/SIDA/AIDSHIV/SIDA/AIDS Where the test is available,all pregnant Where the test is available,all pregnant
women should be tested to prevent MTCTwomen should be tested to prevent MTCT Positive women should receive meds to Positive women should receive meds to
prevent MTCTprevent MTCT Educate on prevention of transmission to Educate on prevention of transmission to
partnerpartner Discuss breastfeeding options-now can Discuss breastfeeding options-now can
have meds but this is dependent on med have meds but this is dependent on med accessibilityaccessibility
Teach not to chew food then give to Teach not to chew food then give to childrenchildren
Educate community re stigmatizationEducate community re stigmatization

What is HIV/AIDSWhat is HIV/AIDS
Chronic viral infection- causing Chronic viral infection- causing progressive immune system progressive immune system deterioration leading to opportunistic deterioration leading to opportunistic infections, cancers, multiple organ infections, cancers, multiple organ system failure, neurologic system failure, neurologic manifestations and wasting.manifestations and wasting.
Two types of virusTwo types of virus HIV-1 most commonHIV-1 most common HIV-2 West AfricaHIV-2 West Africa

What is HIV?What is HIV?
Retrovirus leads to AIDSRetrovirus leads to AIDS NO CURENO CURE Prevention-only optionPrevention-only option Treatment prolongs quality of Treatment prolongs quality of
life-a chronic diseaselife-a chronic disease Transmitted sexually (most Transmitted sexually (most
common) & body fluid contactcommon) & body fluid contact• Pediatric most commonly MTCTPediatric most commonly MTCT
HIV Infection SymptomsHIV Infection Symptoms
Acute infection-similar to any Acute infection-similar to any viral infectionviral infection
Incubation: 6-8 wks Incubation: 6-8 wks Symptoms last 3 wksSymptoms last 3 wks

Acute HIV InfectionAcute HIV Infectionsigns and symptomssigns and symptoms
SymptomsSymptoms FeverFever Joint/muscle painJoint/muscle pain MalaiseMalaise Sore throatSore throat HeadacheHeadache PhotophobiaPhotophobia
SignsSigns Swollen lymph Swollen lymph
nodesnodes Mucosal ulcersMucosal ulcers Maculopapular rashMaculopapular rash

HIV HIV Latent PeriodLatent PeriodMonths to Years (10-12)Months to Years (10-12)
Signs and SymptomsSigns and Symptoms Generalized lymphadenopathyGeneralized lymphadenopathy Recurrent vaginal yeast infectionsRecurrent vaginal yeast infections AsymptomaticAsymptomatic
AIDS/SIDAAIDS/SIDASome manifestationsSome manifestations
Candidiasis Candidiasis ((oesaphagus,respiratory system)oesaphagus,respiratory system)
Invasive cervix cancerInvasive cervix cancer Severe infections often Severe infections often
called opportunisticcalled opportunistic• Protozoa (toxo), viruses Protozoa (toxo), viruses
(CMV, herpes), (CMV, herpes), bacteria(Tb, MAI), bacteria(Tb, MAI), fungi/yeast(PCP,as-fungi/yeast(PCP,as-pergillus)pergillus)
Extra Pulmonary TBExtra Pulmonary TB Chronic herpes Chronic herpes Any disseminated mycosisAny disseminated mycosis
WastingWasting Pneumocystis pneumoniaPneumocystis pneumonia Chronic diarrheaChronic diarrhea LymphomasLymphomas Kaposi’s sarcomaKaposi’s sarcoma Kidney and heart failureKidney and heart failure BlindnessBlindness EncephalitisEncephalitis MeningitisMeningitis DementiaDementia

HIV HIV
DiagnosisDiagnosis Rapid test for HIV antibody usually 2 HIV Rapid test for HIV antibody usually 2 HIV
Monitoring the infection-special labMonitoring the infection-special lab HIV RNA levels (viral load)HIV RNA levels (viral load) CD4 countsCD4 counts
Additional co-infectionsAdditional co-infections Hepatitis A,B and CHepatitis A,B and C Sex transmitted infectionsSex transmitted infections

Other lab testsOther lab tests
CBC, differentialCBC, differential Biochemistries-liver and kidney Biochemistries-liver and kidney
function, lipid profile, glucosefunction, lipid profile, glucose Hepatitis A, B and CHepatitis A, B and C Cytomegalovirus and Toxoplasmosis Cytomegalovirus and Toxoplasmosis
antibodiesantibodies Syphilis and other STD’sSyphilis and other STD’s Cervical cytologyCervical cytology

HIV LabHIV Lab
Virus levels-very high before Virus levels-very high before symptoms, then decline, rise symptoms, then decline, rise again as disease progresses again as disease progresses (months to years)(months to years)
CD4 count declines with CD4 count declines with progressive destruction of the progressive destruction of the immune system immune system (months to years)(months to years)

HIV/AIDS-SIDAHIV/AIDS-SIDATreatmentTreatment
Antiretroviral drugs in combination (HAART)Antiretroviral drugs in combination (HAART) Virus may become resistant requiring Virus may become resistant requiring
changeschanges Lifelong adherence to drugs is essentialLifelong adherence to drugs is essential Aim to obtain a non-detectable viral load Aim to obtain a non-detectable viral load
and CD4 count >250cells/mm3and CD4 count >250cells/mm3 Prevent opportunistic infections Prevent opportunistic infections Requires care by HIV specialistsRequires care by HIV specialists

HIV HIV PreventionPrevention
Universal precautionsUniversal precautions• Gloves-handling body fluidsGloves-handling body fluids• Proper disposal of all body tissues and Proper disposal of all body tissues and
fluidfluid• Clean blood spills with proper fluids – Clean blood spills with proper fluids –
chlorine solutionschlorine solutions Proper blood bank testing Proper blood bank testing

HIV HIV PreventionPrevention
Everyone knowing their infection Everyone knowing their infection statusstatus• Testing all pregnant women (and their Testing all pregnant women (and their
partners and or children if +) prevent partners and or children if +) prevent MTCTMTCT
• Decreases risk takingDecreases risk taking MonogamyMonogamy Safer sexSafer sex
• +/-condom use (at best 70% effective)+/-condom use (at best 70% effective)

Consenting OptionsConsenting Options OPT INOPT IN
• Discuss HIVDiscuss HIV• Sign consent Sign consent • Discuss ARV & confirmatory testsDiscuss ARV & confirmatory tests
OPT OUTOPT OUT• Routine care-mention all labs being doneRoutine care-mention all labs being done• Discuss ARV prophylaxis & confirmatory tests Discuss ARV prophylaxis & confirmatory tests
if probably infected (first test +)if probably infected (first test +)• Sign only if refusalSign only if refusal

Lecture 2Lecture 2

Prevention Prevention HIV MTCTHIV MTCT

HIV in PregnancyHIV in Pregnancy
How does virus get to the baby?How does virus get to the baby? Crosses the placenta-maternal blood Crosses the placenta-maternal blood
enters fetal blood enters fetal blood May be in vaginal secretionsMay be in vaginal secretions Maternal blood present in vaginal Maternal blood present in vaginal
secretions during laborsecretions during labor

Possible Routes of Possible Routes of TransmissionTransmission
In-utero At Birth During Breastfeeding

Timing HIV MTCTTiming HIV MTCT
In utero 25%–40% of casesIn utero 25%–40% of cases Intrapartum 60%–75% of casesIntrapartum 60%–75% of cases Additional risk with breastfeedingAdditional risk with breastfeeding
14% 14% risk with established infection risk with established infection 29% 29% risk with primary infection risk with primary infection
Most transmission occurs intrapartumMost transmission occurs intrapartum


PACTG 076 Trial Targeted 3 PACTG 076 Trial Targeted 3 Potential Time Points of MTCTPotential Time Points of MTCT
Pregnancy Labor and delivery Infant Pregnancy Labor and delivery Infant
Antepartum Intrapartum PostpartumAntepartum Intrapartum Postpartum AZT IV AZT AZT AZT IV AZT AZT ______________________________________________________________________Result: 67% reduction in MTCT Result: 67% reduction in MTCT 25.5% placebo arm25.5% placebo arm 8.3% AZT arm 8.3% AZT arm
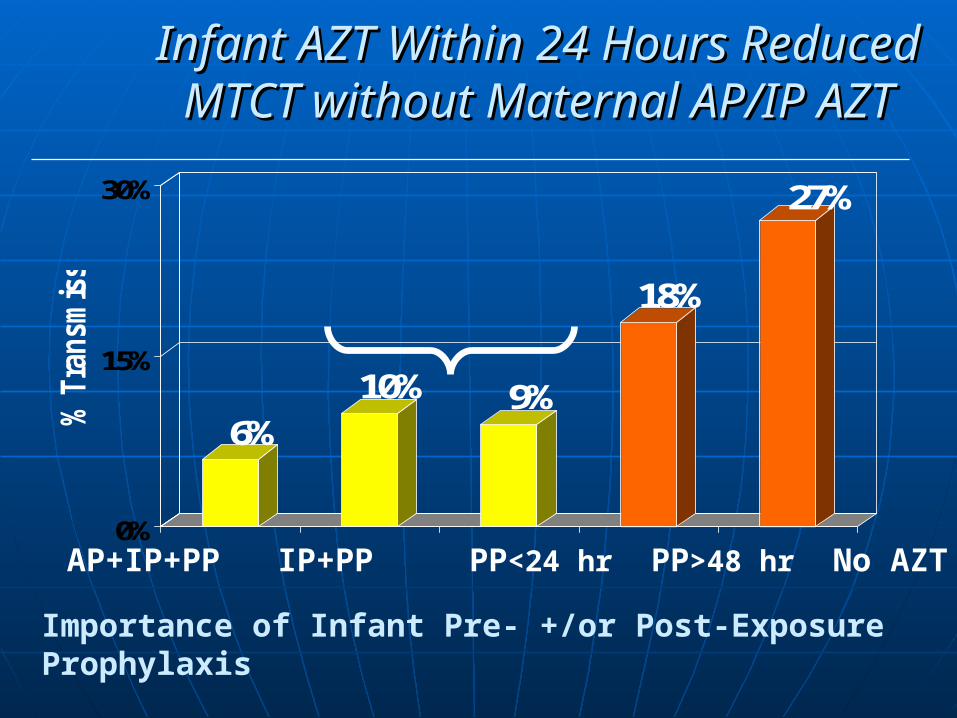
Infant AZT Within 24 Hours Reduced Infant AZT Within 24 Hours Reduced MTCT without Maternal AP/IP AZTMTCT without Maternal AP/IP AZT
6%10% 9%
18%
27%
0%
15%
30%
% T
ransm
issio
n
AP+IP+PP IP+PP PP<24 hr PP>48 hr No AZT
Importance of Infant Pre- +/or Post-Exposure Prophylaxis
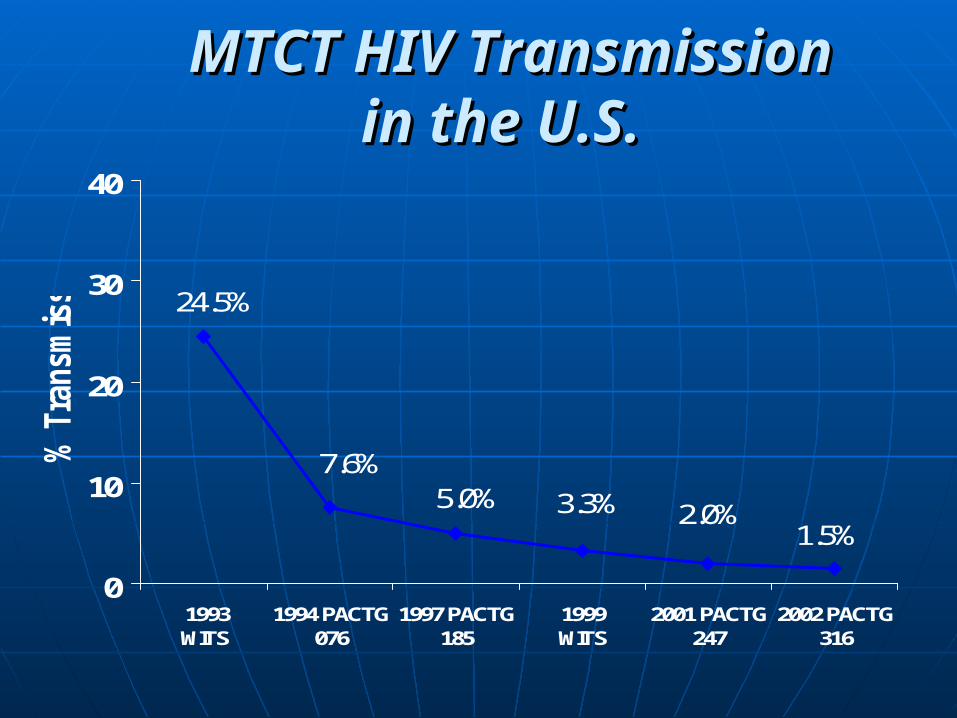
MTCT HIV Transmission MTCT HIV Transmission in the U.S.in the U.S.
1.5%2.0%3.3%5.0%
7.6%
24.5%
0
10
20
30
40
1993 WITS
1994 PACTG076
1997 PACTG185
1999 WITS
2001 PACTG247
2002 PACTG316
% T
ransm
issio
n
Preventing HIV MTCTPreventing HIV MTCT
Early identificationEarly identification• Test for HIV as early as possible and treatTest for HIV as early as possible and treat
Pregnancy managementPregnancy management• Proper prenatal careProper prenatal care• Monitor fetal growthMonitor fetal growth• Decide on mode of deliveryDecide on mode of delivery
Maternal medical managementMaternal medical management• Serial labs to follow CBC, glucose, kidney and liver Serial labs to follow CBC, glucose, kidney and liver
function, viral load and CD4 countsfunction, viral load and CD4 counts

Preventing HIV MTCT Preventing HIV MTCT
Maternal medical managementMaternal medical management Treat all infectionsTreat all infections
• Vaginal, urine, respiratoryVaginal, urine, respiratory• Decreases challenges to immune Decreases challenges to immune
systemsystem Serial labs to follow disease status Serial labs to follow disease status
and effect of HIV medsand effect of HIV meds CBC, glucose, kidney and liver CBC, glucose, kidney and liver
function, viral load and CD4 countsfunction, viral load and CD4 counts

Preventing MTCTPreventing MTCT
Delivery & postpartum managementDelivery & postpartum management• If undelivered at 40 weeks consider If undelivered at 40 weeks consider
induction induction • DO NOT rupture membranes if possibleDO NOT rupture membranes if possible• Avoid episiotomyAvoid episiotomy• HIV meds in laborHIV meds in labor• If breastfeeding continue medsIf breastfeeding continue meds

Preventing MTCTPreventing MTCT
Neonatal prophylaxis/treatmentNeonatal prophylaxis/treatment• Initiate HIV meds as soon as possible after Initiate HIV meds as soon as possible after
deliverydelivery• Notify a pediatric provider of potential HIV Notify a pediatric provider of potential HIV
infection for careinfection for care• Ideally get HIV RNA viral load or better DNA Ideally get HIV RNA viral load or better DNA
viral load at 2-4 wks of age and at 12 weeks if viral load at 2-4 wks of age and at 12 weeks if not BF*not BF*
• BF then same 6-12 weeks after all exposure to BF then same 6-12 weeks after all exposure to breast milk stopsbreast milk stops
• Infant should be tested if abnormal growth and Infant should be tested if abnormal growth and developmentdevelopment
*breastfeeding

Factors Influencing MTCTFactors Influencing MTCT
MaternalMaternal• HIV-1 RNA levels HIV-1 RNA levels • Low CD4 countLow CD4 count• Other infectionsOther infections
(hepatitis C, CMV, (hepatitis C, CMV, bacterial vaginosis)bacterial vaginosis)
• Maternal injection Maternal injection drug usedrug use
• Lack of ARV during Lack of ARV during pregnancypregnancy
ObstetricObstetric• Length of Length of
ruptured ruptured membranes??membranes??
• chorioamnionitischorioamnionitis• Vaginal delivery Vaginal delivery • Invasive Invasive
proceduresprocedures
Infant Infant PrematurityPrematurity
Lecture 3Lecture 3
ANTIRETROVIRAL DRUGS ANTIRETROVIRAL DRUGS
IN PREGNANCYIN PREGNANCY

Antiretroviral Drugs in Antiretroviral Drugs in PregnancyPregnancy
Viral Load (VL) affects rate of MTCTViral Load (VL) affects rate of MTCT• Although rare, transmission can Although rare, transmission can
occur despite a non-detectable occur despite a non-detectable (ND) VL and adequate therapy(ND) VL and adequate therapy
Combination drugs better than singleCombination drugs better than single Adherence to drug is essentialAdherence to drug is essential
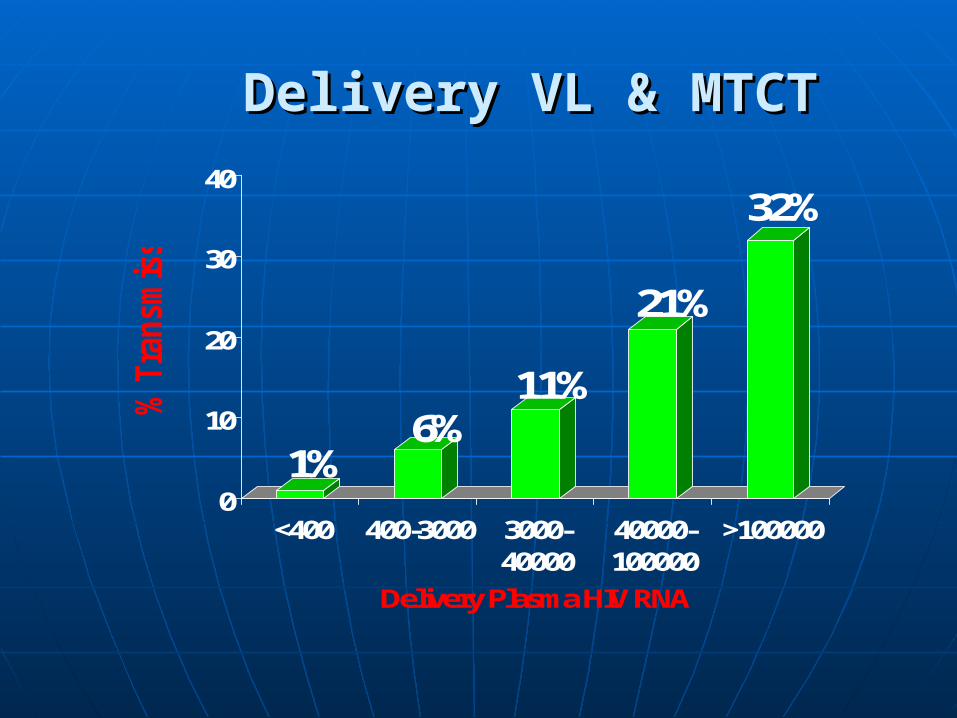
Delivery VL & MTCTDelivery VL & MTCT
1%6%
11%
21%
32%
0
10
20
30
40%
Tra
nsm
issio
n
<400 400-3000 3000-40000
40000-100000
>100000
Delivery Plasma HIV RNA
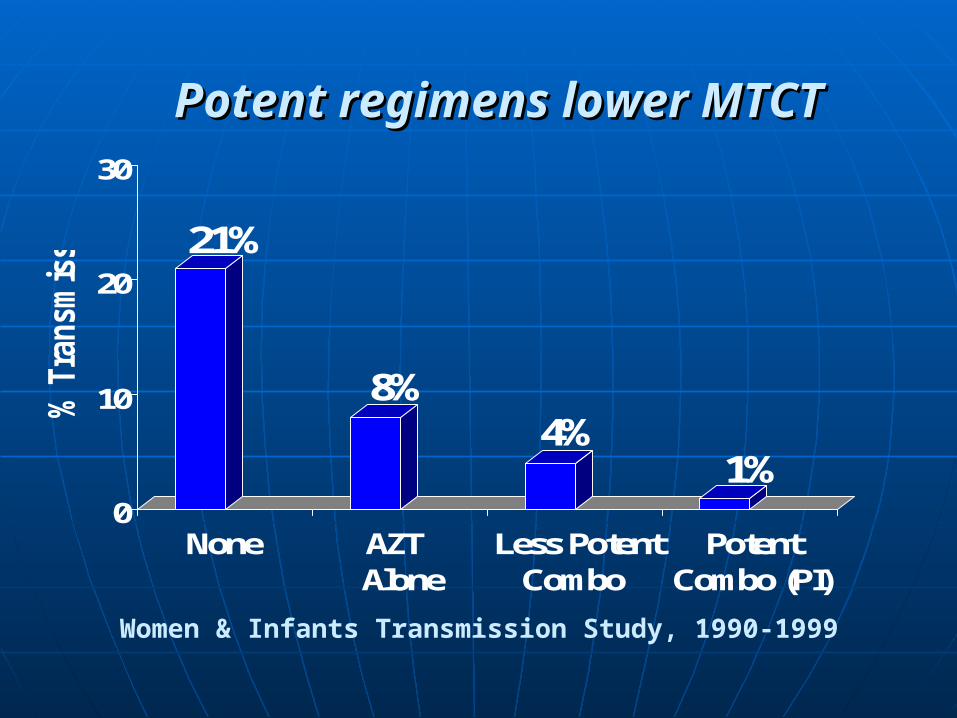
Potent regimens lower MTCTPotent regimens lower MTCT
21%
8%4%
1%0
10
20
30
% T
ransm
issio
n
None AZT Alone
Less PotentCombo
PotentCombo (PI)
Women & Infants Transmission Study, 1990-1999
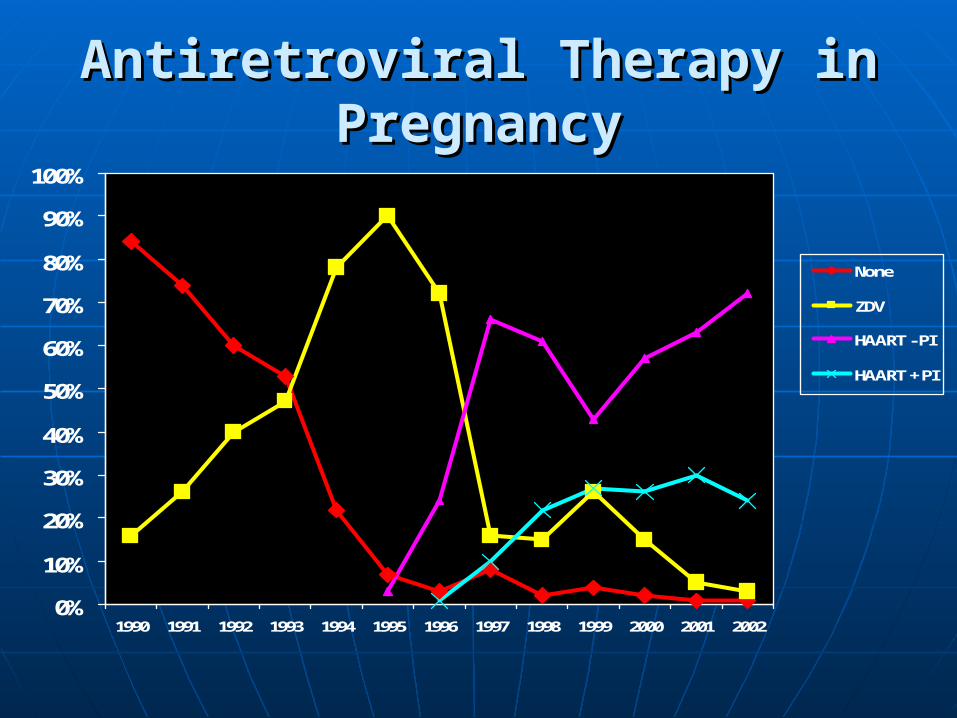
Antiretroviral Therapy in Antiretroviral Therapy in PregnancyPregnancy
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002
None
ZDV
HAART - PI
HAART + PI

ARV in PregnancyARV in Pregnancy
ROLEROLE
Reduce perinatal transmissionReduce perinatal transmission
Improve maternal healthImprove maternal health

Classification of ARV DrugsClassification of ARV Drugs
All are inhibitors of viral actionAll are inhibitors of viral action Nucleoside reverse transcriptase -Nucleoside reverse transcriptase -
NRTINRTI Non-nucleoside NNRTINon-nucleoside NNRTI Protease PIProtease PI Integrase InhibitorIntegrase Inhibitor Entry InhibitorEntry Inhibitor
Effects of ARV in PregnancyEffects of ARV in Pregnancy
Pregnant womanPregnant woman
FetusFetus
NewbornNewborn


ARV and Birth DefectsARV and Birth Defects
Rate same as in the general Rate same as in the general population not taking ARV’s 1.5-3%population not taking ARV’s 1.5-3%
EFV has a small but increased risk of EFV has a small but increased risk of neural tube defects neural tube defects • Ideally initiation avoided in the first Ideally initiation avoided in the first
trimestertrimester
ARV concernsARV concerns
Multi drug resistanceMulti drug resistance Lactic acidosis (ddl + d4T you are Lactic acidosis (ddl + d4T you are
unlikely to use these)unlikely to use these) EfavirenzEfavirenz Gestational DM (protease inhibitors)Gestational DM (protease inhibitors) May affect other drugs due to May affect other drugs due to
interference with enzyme activityinterference with enzyme activity

Guidelines for ART in PregnancyGuidelines for ART in Pregnancy
Use optimal ARV for the woman’s health Consider potential fetal/infant impact Discuss preventable risk factors for MTCT Support decision-making by the woman
following discussion of known and unknown benefits and risks
Acceptance or refusal of ARV should not result in denial of care or punitive action

Lecture 4Lecture 4
WHO WHO HIV/AIDS HIV/AIDS
GuidelinesGuidelines

WHO ARV Drugs for PregnancyWHO ARV Drugs for PregnancyDrugDrug InitialInitial Drug typeDrug typeAzidothymidine/Azidothymidine/
ZidovudineZidovudineAZTAZT NRTINRTI
Lamivudine/EpivirLamivudine/Epivir 3TC3TC NRTINRTINevirapine/Nevirapine/
ViramuneViramuneNVPNVP NNRTINNRTI
Efavirenze/SustivaEfavirenze/Sustiva EFVEFV NNRTINNRTITenofavir/VireadTenofavir/Viread TDFTDF NRTINRTIEmtricitabine/Emtricitabine/
EmtrivaEmtrivaFTCFTC NRTINRTI
Lopinovir/r /KaletraLopinovir/r /Kaletra LPV/rLPV/r PIPIAbacavir/ZiagenAbacavir/Ziagen ABCABC NRTINRTI
WHO Guidelines 2010WHO Guidelines 2010
Goals of earlier treatmentGoals of earlier treatment Benefit maternal healthBenefit maternal health Maximally reduce MTCTMaximally reduce MTCT Provide prophylaxis after delivery to Provide prophylaxis after delivery to
mother during breastfeedingmother during breastfeeding• BF essential to prevent infant death BF essential to prevent infant death
from malnutrition & diarrheafrom malnutrition & diarrhea

WHO Guidelines 2010 WHO Guidelines 2010
Without ARV prophylaxis risk of MTCT Without ARV prophylaxis risk of MTCT 35% with breastfeeding (BF)35% with breastfeeding (BF) 25% without BF25% without BF Prophylaxis can reduce this to Prophylaxis can reduce this to 5% with BF5% with BF 2% or less without BF2% or less without BF

HIV HIV Infant ProphylaxisInfant ProphylaxisPrevention MTCTPrevention MTCT
MotherMother Start as early as Start as early as
possiblepossible Continue Continue
throughout throughout pregnancy, labor, pregnancy, labor, delivery and the delivery and the duration of duration of breastfeedingbreastfeeding
InfantInfant
Breastfeeding (BF)Breastfeeding (BF) Daily from birth Daily from birth
until 1 week after until 1 week after ALLALL BF is stopped BF is stopped
Not BFNot BF Daily until 4-6 Daily until 4-6
weeks of ageweeks of age

WHOWHO Prophylaxis Prophylaxis RegimenRegimenMother Mother AntenatallyAntenatally
OPTION AOPTION A
Twice daily AZT-Twice daily AZT-start as early as 14 start as early as 14 wkswks
OPTION BOPTION B AZT+3TC+LPV/r orAZT+3TC+LPV/r or AZT+3TC+ABC orAZT+3TC+ABC or AZT+3TC+EFV orAZT+3TC+EFV or TDF+3TCTDF+3TC
(or FTC)+EFV(or FTC)+EFV
Option A Option A WHO WHO Prophylaxis labour and deliveryProphylaxis labour and delivery
IF maternal AZT for IF maternal AZT for <4 wks<4 wks before before deliverydelivery
Single dose NVP + Single dose NVP + twice daily twice daily AZT+3TC for 7 AZT+3TC for 7 days post deliverydays post delivery
If maternal AZT for If maternal AZT for >4 wks>4 wks before before deliverydelivery
Can omit single Can omit single dose NVPdose NVP
AZT twice daily AZT twice daily labourlabour
Stop AZT at Stop AZT at deliverydelivery

OPTION A**OPTION A**Prophylaxis Regimen-Prophylaxis Regimen-InfantInfant
Breastfeeding (BF)Breastfeeding (BF) NVP single dose NVP single dose
daily from birth for daily from birth for a minimum 4-6 wks a minimum 4-6 wks ANDAND until 1 week until 1 week after all exposure after all exposure to breast milk is to breast milk is stoppedstopped
Not BFNot BF NVP single dose NVP single dose
daily ordaily or Single dose Single dose
NVP+twice daily NVP+twice daily AZT x 4-6 weeksAZT x 4-6 weeks
**Infant meds to start 6-12 hours after birth

OPTION B** OPTION B** Prophylaxis Regimen-Prophylaxis Regimen-InfantInfant
Regardless of mode of infant feedingRegardless of mode of infant feeding Daily single dose NVP orDaily single dose NVP or Twice daily AZTTwice daily AZT Start within 6-12 hours of delivery or Start within 6-12 hours of delivery or
as soon as possible, until baby is 4-6 as soon as possible, until baby is 4-6 weeks of age weeks of age

When is HIV Treatment When is HIV Treatment requiredrequired for the woman’s own health?for the woman’s own health?
CD4 count <350 cells/mmCD4 count <350 cells/mm33
• Regardless of the WHO clinical stagingRegardless of the WHO clinical staging All with WHO clinical stage 3 or 4 All with WHO clinical stage 3 or 4
• Regardless of the CD4 countRegardless of the CD4 count

AIMS of ARV AIMS of ARV required for maternal health required for maternal health
Decrease maternal viral load to non-Decrease maternal viral load to non-detectable during pregnancydetectable during pregnancy
Provide drug to the baby in-utero and Provide drug to the baby in-utero and during labor and deliveryduring labor and delivery
Provide drug to the infant for 4-6 wks Provide drug to the infant for 4-6 wks if not BFif not BF
Provide drug to the mother during BF Provide drug to the mother during BF to keep her viral load as low as to keep her viral load as low as possiblepossible

Prevention MTCTPrevention MTCTMother requires treatment Mother requires treatment
Both maternal treatment & infant Both maternal treatment & infant prophylaxisprophylaxis
1.1. Start as soon as possibleStart as soon as possible
2.2. Regardless of gestational ageRegardless of gestational age
3.3. Through pregnancy, labor, delivery, Through pregnancy, labor, delivery, and thereafter DO NOT STOP and thereafter DO NOT STOP

Prevention MTCT Prevention MTCT mother requires treatmentmother requires treatmentRecommended regimens**Recommended regimens**
Mother recommended Mother recommended regimensregimens
AZT + 3TC + NVP orAZT + 3TC + NVP or AZT + 3TC + EFV* orAZT + 3TC + EFV* or TDF + 3TC (or FTC) + TDF + 3TC (or FTC) +
NVP orNVP or TDF + 3TC (or FTC) + TDF + 3TC (or FTC) +
EVF*EVF*
Infant-with or without Infant-with or without breast feedingbreast feeding
Daily NVP or twice Daily NVP or twice daily AZT till 4-6 wks daily AZT till 4-6 wks of ageof age
*avoid use in 1st trimester risk of neural tube defects
**WHO Guidelines 2010

MTCT & Maternal Viral Load MTCT & Maternal Viral Load
Despite appropriate antiretroviral drugs, MTCT can occur, though rare with a non-detectable viral load
Non-detectable does not mean no virus
Virus may be present in the vagina during delivery

Cesarean deliveryCesarean delivery
Scheduled CD has increased among Scheduled CD has increased among women with HIV infection since the women with HIV infection since the demonstration that delivery before demonstration that delivery before labor and membrane rupture can labor and membrane rupture can
reduce intrapartum HIV transmissionreduce intrapartum HIV transmission

Mode of DeliveryMode of Delivery
Cesarean – if viral load >1000 copies/mLCesarean – if viral load >1000 copies/mL Never been adequately studied on Never been adequately studied on
combination therapycombination therapy Women are given the optionWomen are given the option If C/D – done at 38 wks before onset of If C/D – done at 38 wks before onset of
laborlabor• Increased maternal risksIncreased maternal risks• Increased infant risks- increased respiratory Increased infant risks- increased respiratory
and jaundice complicationsand jaundice complications
Cesarean Delivery to Reduce Cesarean Delivery to Reduce Perinatal HIV TransmissionPerinatal HIV Transmission
Counsel: potential benefits and risks of scheduled C/D to reduce perinatal transmission
C/D reduces transmission associated with an unknown VL untreated or receiving only ZDV
May be effective in women with VL>1000 copies/mL
Unproven benefit in women on ART

Post C/S MorbidityPost C/S Morbidity
Emergency cesareanEmergency cesarean 12% (4.17)12% (4.17) Elective cesareanElective cesarean 6.4% (1.85) 6.4% (1.85) NSVDNSVD 4.0% 4.0%
• Postpartum feverPostpartum fever• DVT/PEDVT/PE• TransfusionTransfusion• Postpartum proceduresPostpartum procedures

Only use if discussion warrantsOnly use if discussion warrants

Safety and Toxicity of ART in Safety and Toxicity of ART in Pregnant Women: PIsPregnant Women: PIs
Concern for increased risk of Concern for increased risk of hyperglycemia: monitor closelyhyperglycemia: monitor closely
Conflicting data re preterm delivery in Conflicting data re preterm delivery in women receiving PIswomen receiving PIs
Mitochondrial Toxicity and Mitochondrial Toxicity and Nucleoside Analogue DrugsNucleoside Analogue Drugs
Nucleoside analogs known to induce Nucleoside analogs known to induce mitochondrial dysfunction (neurologial effects mitochondrial dysfunction (neurologial effects most French data, very rare in US data)most French data, very rare in US data)
Lactic acidosis/hepatic steatosis reported Lactic acidosis/hepatic steatosis reported Pregnant women on nucleoside analogues Pregnant women on nucleoside analogues
should have liver enzymes and electrolytes should have liver enzymes and electrolytes monitored in 3monitored in 3rdrd trimester trimester

Combination Therapy with Combination Therapy with Protease Inhibitor ? RisksProtease Inhibitor ? Risks
No increase in No increase in preterm preterm delivery, low delivery, low birth weight or birth weight or stillbirthstillbirth
5% on PI vs 2% 5% on PI vs 2% very low birth very low birth weightweight
Tuomala et al, NEJM 2002Tuomala et al, NEJM 2002
33% risk PTD33% risk PTD Lorenzi et al, AIDS Lorenzi et al, AIDS
19981998
increased PTD increased PTD (p=0.0001) OR (p=0.0001) OR 2.4, 95% CI 1.3 - 2.4, 95% CI 1.3 - 4.44.4
Cotter et al J Infect Dis 2006Cotter et al J Infect Dis 2006

ARV & PTD : Another Clue?ARV & PTD : Another Clue? In the absence of clinically evident In the absence of clinically evident
chorioamnionitischorioamnionitis
Combination therapy +PI was a/w Combination therapy +PI was a/w evidence of histological chorioamnionitis evidence of histological chorioamnionitis
This increased the risk of PTD (p=0.001)This increased the risk of PTD (p=0.001)

Four Hour RuleFour Hour Rule
Protective effect of CD in setting Protective effect of CD in setting of HSV lesionsof HSV lesions

Duration of ruptured membranes & Duration of ruptured membranes & vertical transmission of HIVvertical transmission of HIV
The risk increased by 2% for every one The risk increased by 2% for every one hour increase in duration of hour increase in duration of membrane rupturemembrane rupture
A diagnosis of AIDS may potentiate A diagnosis of AIDS may potentiate this effect this effect
AIDS 2001AIDS 2001

Duration of Membrane Duration of Membrane Rupture & Perinatal Rupture & Perinatal Transmission of HIV:Transmission of HIV:
Does the Four Hour Rule Does the Four Hour Rule Still Apply?Still Apply?
cotter IDSOG cotter IDSOG Seattle 2008Seattle 2008

PNT RatePNT Rate
Membrane rupture < 4 hours Membrane rupture < 4 hours 0.9%0.9%
Membrane rupture Membrane rupture ≥≥ 4 hours 4 hours 2.1%2.1%
MTCT RateMTCT Rate
VL<1000 copies/mL on combination VL<1000 copies/mL on combination ARTART
n=429n=429
Membrane rupture < 4 hours 0%Membrane rupture < 4 hours 0% Membrane rupture Membrane rupture ≥≥ 4 hours 0% 4 hours 0%
up to 25 hoursup to 25 hours

MTCT RateMTCT Rate
VL VL ≥≥1000 on combination ART1000 on combination ART
Membrane rupture < 4 hours Membrane rupture < 4 hours 2.9%2.9%
Membrane rupture Membrane rupture ≥≥ 4 hours 4 hours 1.1%1.1%
ConclusionConclusion
Duration of membrane rupture Duration of membrane rupture ≥4 hours is not a risk factor for ≥4 hours is not a risk factor for MTCT of HIV in women with a MTCT of HIV in women with a VL<1000/mL on combination VL<1000/mL on combination ARTART

Missed Opportunities for HIV Missed Opportunities for HIV MTCT Prevention in the USAMTCT Prevention in the USA
Review of 5054 HIV-exposed Review of 5054 HIV-exposed deliveries at 6 sites in the USA from deliveries at 6 sites in the USA from 19961996––20002000
423 HIV-infected infants423 HIV-infected infants Perinatal HIV transmission ratePerinatal HIV transmission rate
• 2.5% for maternal combination therapy2.5% for maternal combination therapy
• 5.4% for maternal AZT alone (both with 5.4% for maternal AZT alone (both with intrapartum and neonatal AZT)intrapartum and neonatal AZT)
• 28% with no treatment28% with no treatment
Peters VB et al. XIV IAC; Barcelona, 2002: Abstract #1429.

How can MTCT be further How can MTCT be further reduced?reduced?
Early prenatal careEarly prenatal care Re-test at 32 weeks, especially Re-test at 32 weeks, especially
those at high risk those at high risk Rapid HIV testing of Rapid HIV testing of allall women women
presenting to the hospital without presenting to the hospital without documented HIV statusdocumented HIV status

Rapid Testing at Delivery toRapid Testing at Delivery toLate-Presenting WomenLate-Presenting Women
High risk of perinatal transmission High risk of perinatal transmission in women without antenatal care in women without antenatal care
Rapid testing in labor can make it Rapid testing in labor can make it possible to initiate ARV prophylaxis possible to initiate ARV prophylaxis
ARV prophylaxis should be initiated ARV prophylaxis should be initiated as soon as possible after a positive as soon as possible after a positive rapid HIV test rapid HIV test







