Download - Legg calve perthes disease

LEGG CALVE PERTHES DISEASE
DR VANDANA G HARI RESIDENT KIMS TRIVANDRUM

Painful disorder of childhood characterised by avascular necrosis of femoral capital epiphysis.-Osteochondritis deformans juvenilis/Coxa plana-described 1910 independently by Legg, Calve, Perthes ,Waldenstrom
Legg Calve Perthes Disease

Pathogenesis
Precipitating cause unknown Predisposing factors-Genetic aspects 2-20%-Abnormal growth & development ,bone age
<1-3yrsPoor socio economic status
-Inherited thrombophilia-Males 4:1-Trauma

Cardinal cause ISCHEMIA OF FEMORAL HEAD
4-7yrs femoral head depend on lateral epiphyseal vessels(.upto 4 metphysea later ligamentum teres)
Epiphyseal vessels susceptible to stretching & pressure
Effusion
Venous flow blocked
Venous stasis
Intraosseous pressure rises Ischemia

Stages of Legg-Calves-Perthes (Waldenström
Initial -infarction produces a smaller, sclerotic epiphysis with medial joint space widening
-radiographs may remain occult for 3 to 6 mos

FragmentationDead marrow replaced with granulation
tissueBone revascularisedSome dead fragments replaced by fibrous
tissue Alternating areas of sclerosis &fibrosis –
Fragmentation of epiphysisHyperemic metaphysis-Rarefied / cystic in X-
ray-hip related symptoms are most prevalent-lateral pillar classification based on this stage
• Reossification -ossific nucleus undergoes reossification as new bone appears as necrotic bone is resorbed
-may last up to 18m
Healing or remodeling -femoral head remodels until skeletal maturity
-begins once ossific nucleus is completely reossified trabecular patterns return
Rapid &complete repair- architecture maintained
Tardy epiphysis collapse –Distorted growth of Head and Neck
Head Oval flattened head of mushroom
Neck shor t and broad

Clinical Features-Classical presentationPainless limp (4-8yr old boy)-Pain a/c or insidious –
vague ,ache in groin, thigh or knee, aggravated by hip movements

Signs1.Antalgic gait2.Muscle spasm3.Limited abduction & internal
rotation4.Proximal thigh atrophy5. Trendelenburg gait (head
collapse leads to decreased tension of abductors

Radiology
Decreased size of left femoral capital epiphysis
Linear translucency
.wide joint space

Subchondral fracture
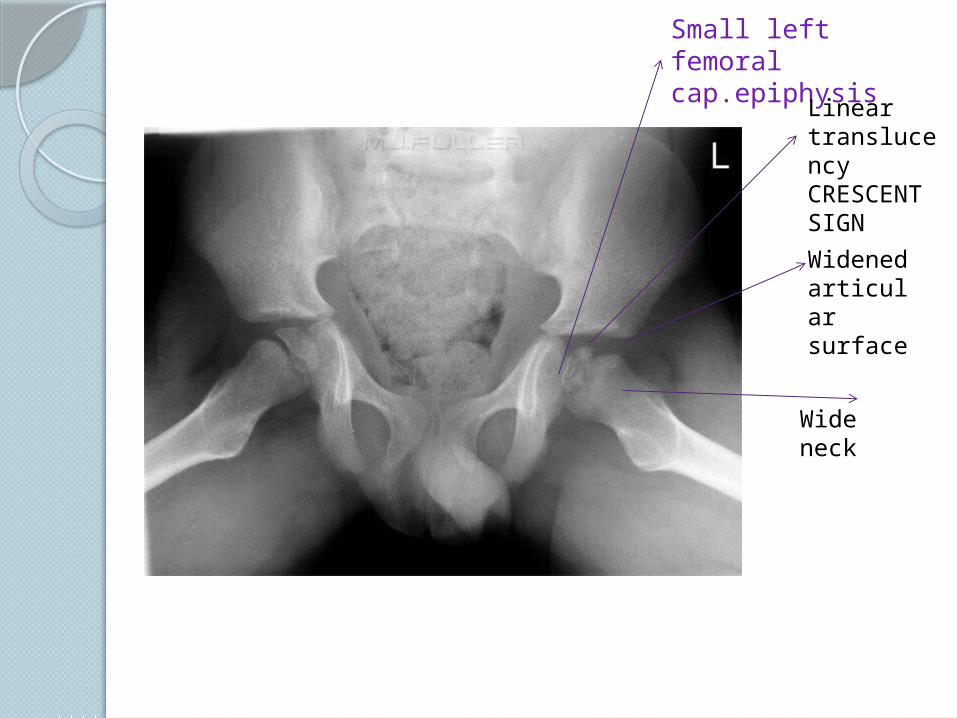
Small left femoral cap.epiphysis
Wide neck
Widened articular surface
Linear translucency CRESCENT SIGN
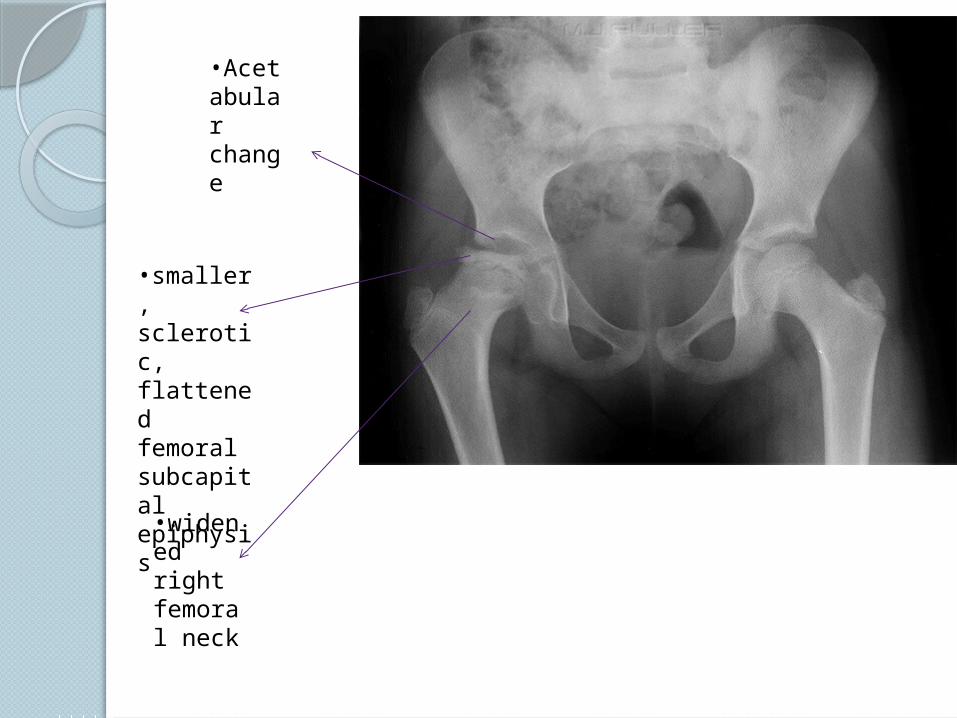
•Acetabular change
•widened right femoral neck
•smaller, sclerotic, flattened femoral subcapital epiphysis
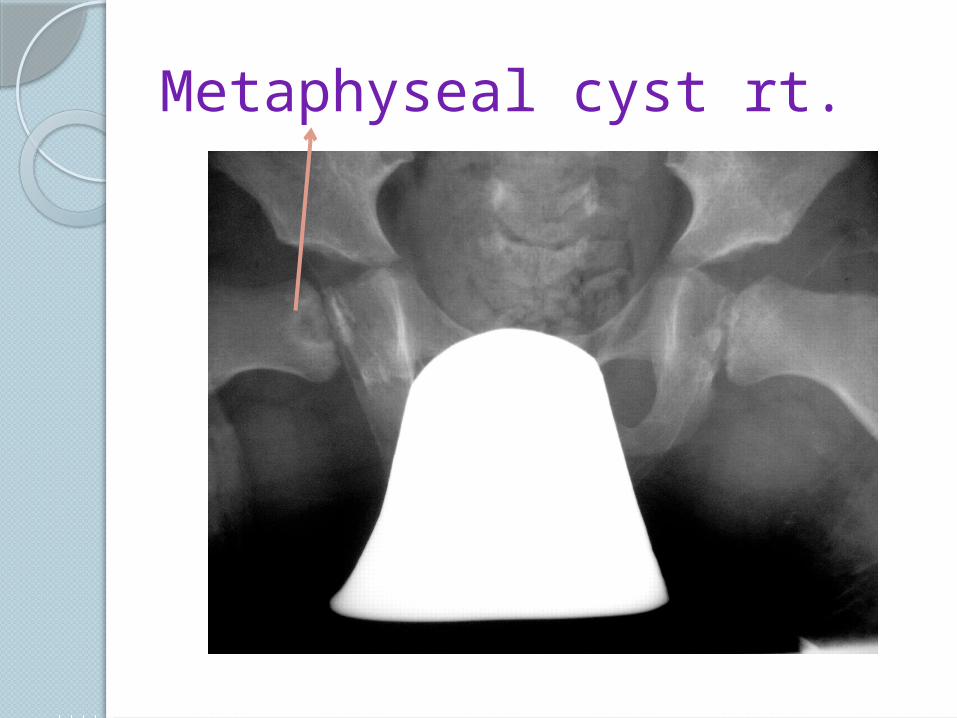
Metaphyseal cyst rt.

In group I there is involvement (hatched areas) of the anterior head only, no sequestrum, and no collapse of the
epiphysis. In group II, only the anterior head is involved, and there is a sequestrum with a clear junction. In group III only a small part of the epiphysis is not involved. In group IV there is total head involvement
CATERALL CLASSIFICATION
Gp 3 & 4
◦Head at risk signs (indicate a more severe disease course) Gage sign
V-shaped radiolucency in the lateral portion of the epiphysis and/or adjacent metaphysis
calcification lateral to the epiphysis lateral subluxation of the femoral head Horizontal growth plate
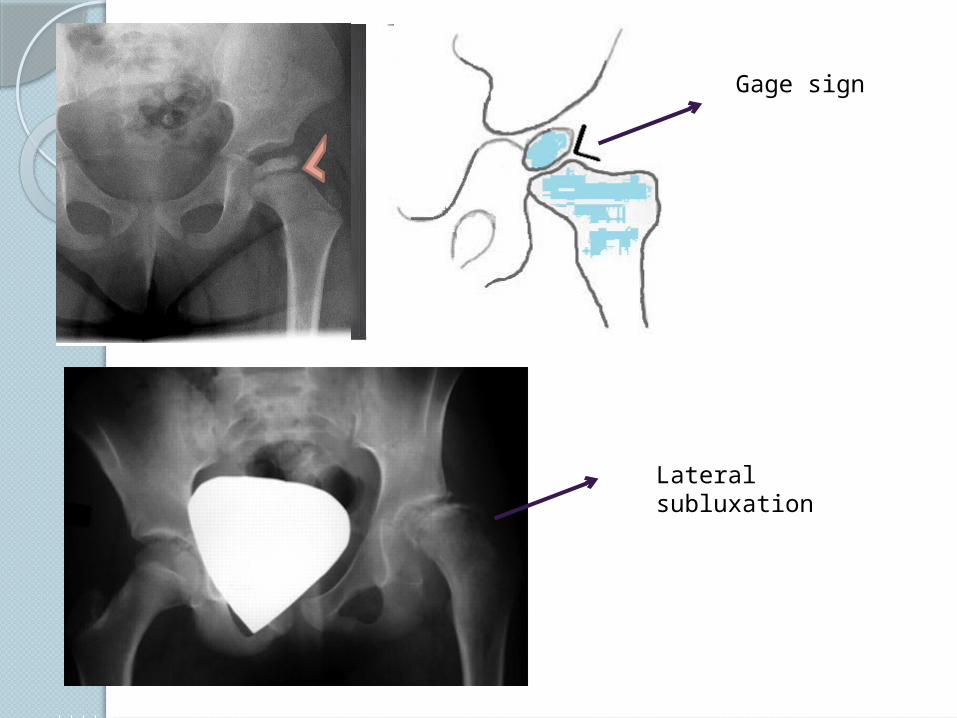
Gage sign
Lateral subluxation
Salter Thompson
GP A :<1/2 of capital femoral epiphysis involved
Gp B: >1/2 involved
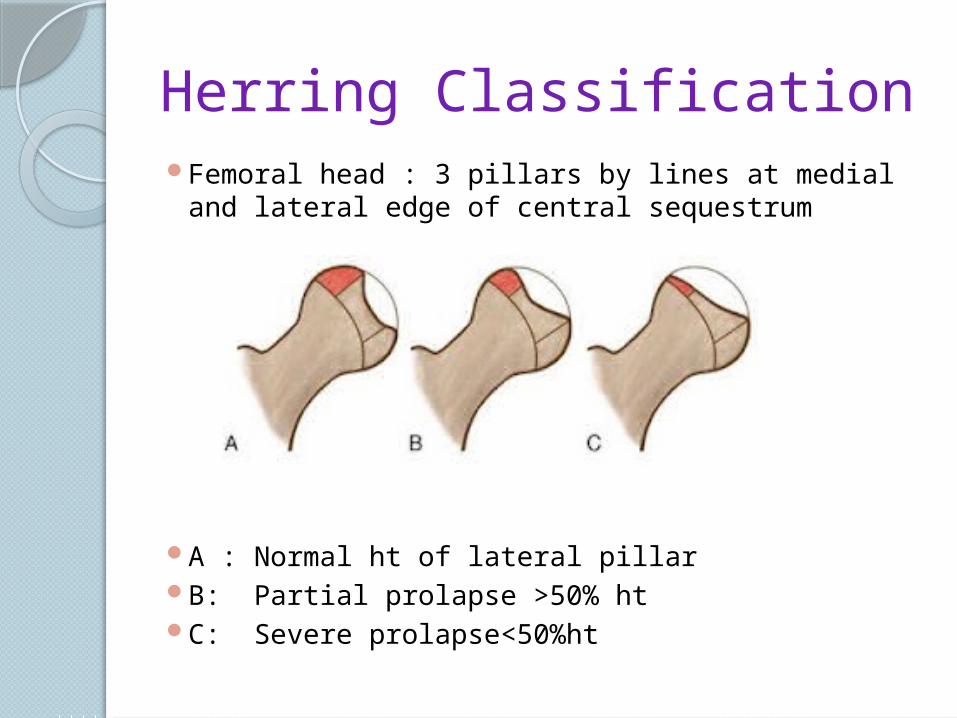
Herring ClassificationFemoral head : 3 pillars by lines at medial and
lateral edge of central sequestrum
A : Normal ht of lateral pillarB: Partial prolapse >50% htC: Severe prolapse<50%ht
Other investigationsBone scan ◦can confirm suspected case of LCP◦decreased uptake (cold lesion) can predate
changes on radiographsMRI ◦can provide early diagnosis revealing
alterations in the capital femoral epiphysis and physis
Arthrogram ◦a dynamic arthrogram can demonstrate
coverage and containment of the femoral head
Treatment
The primary aim Containment of head with in acetabulam
Initial management:1. analgesia2.modification of activities3.preservation of abductionReassess
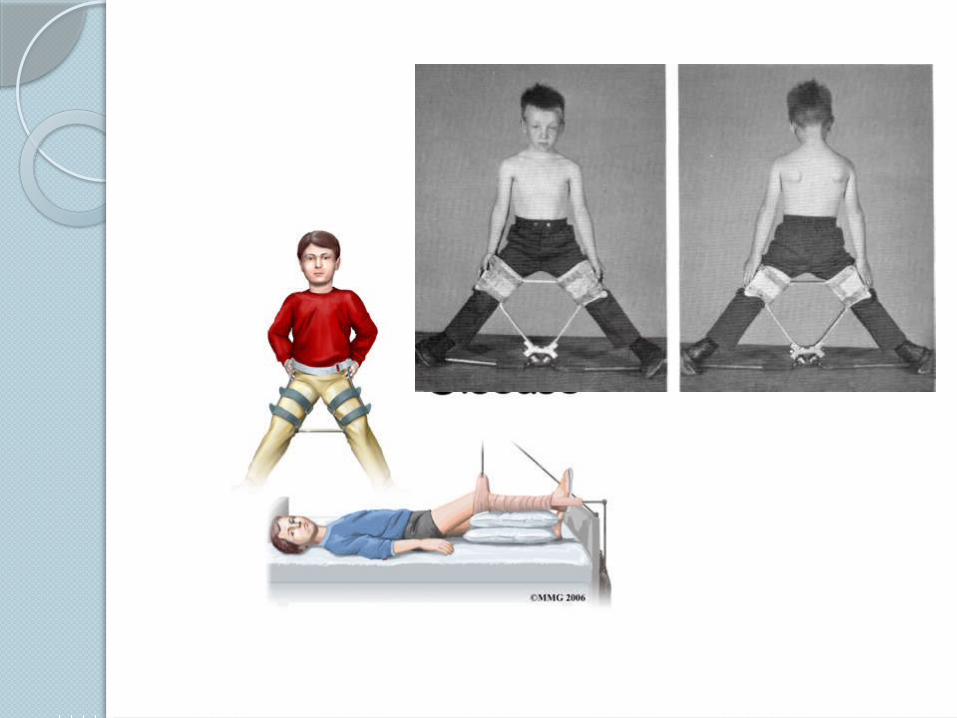
Containment
Holding hip widely abducted
• Newington brace,Toronto,Petri cast, Scottish Rite

Surgical procedures
VARUS DEROTATIONAL OSTEOTOMY –to provide containment
Reconstructive Procedures
Cheiloctomy –removal of protuberance
Chiari osteotomy-deepens acetabulam by medial displcement of distal pelvic fragment
Trocanteric advancement-distal transfer to normalise tension of trocanteric muscles

Guidelines
Children under 6Symptomatic treatment

6-8yrs
Bone age <=6yrs
LP A&B: symptomatic treatment
LP C:Ab.brace
>9yrsOperative containment

Thank u
THANK YOU







