
Long-Term Comparison of Medical Treatment With Percutaneous Closure of Patent Foramen Ovale for SecondaryPrevention of Paradoxical Embolism:
A Propensity-Score Matched Comparison
Andreas Wahl*, Fabien Praz*, Bindu Kalesan†, Marie-Luise Mono#,
Laura Geister#, Krassen Nedeltchev#, Lorenz Räber*,
Heinrich P. Mattle#, Peter Jüni†, Stephan Windecker*, Bernhard Meier*
Departments of Cardiology* and Neurology# and Clinical Trials Unit†
Bern University Hospital, Switzerland

Conflicts of Interest
• Research grants• Lecture and consultation fees
– AGA Medical, Plymouth, MN, USA
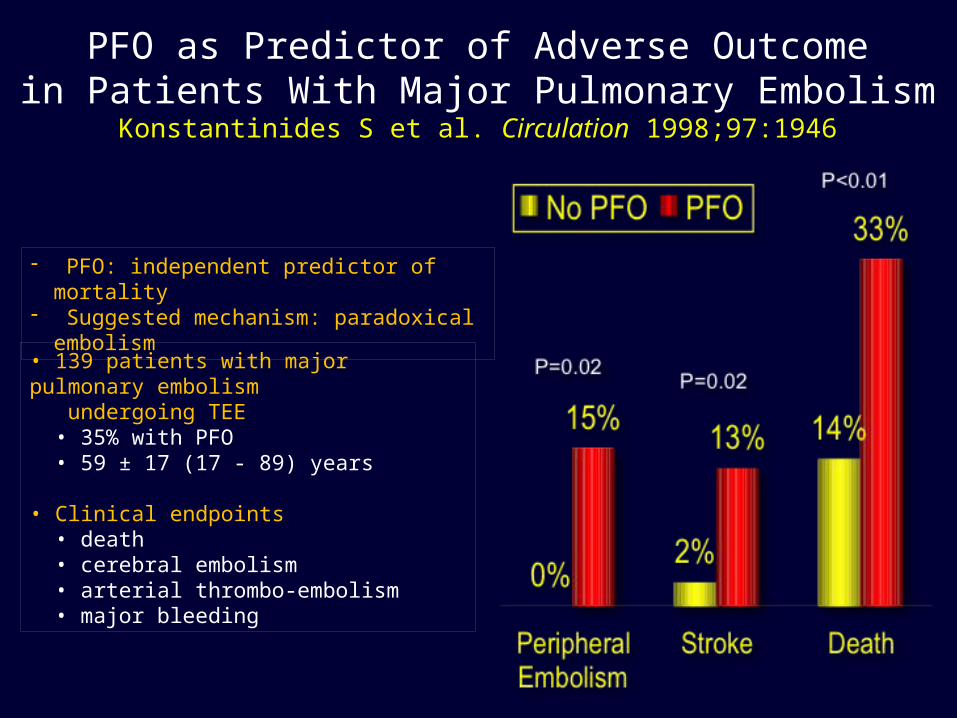
PFO as Predictor of Adverse Outcomein Patients With Major Pulmonary Embolism
Konstantinides S et al. Circulation 1998;97:1946
- PFO: independent predictor of mortality- Suggested mechanism: paradoxical
embolism
• 139 patients with major pulmonary embolism undergoing TEE • 35% with PFO • 59 ± 17 (17 - 89) years
• Clinical endpoints • death • cerebral embolism • arterial thrombo-embolism • major bleeding

Das RR, Stroke. 2008;39:2929-2935
Silent Cerebral Infarctions (by MR)2,040 Framingham Offsprings
(53% female; mean age, 62±9 years)

Prevalence of PFO According to Age
Age (years)
PFO in 263/965 autopsies (mean 27%)
Y=35-0.12xR2=0.6, p=0.008
Hagen PT, Mayo Clin Proc 1984; 59: 17-20
Selective mortality?
%
Percutaneous PFO Closure• Percutaneous PFO closure has been shown to be
safe and efficacious using several devices- Small procedural risk
- Minimal long-term risk
- Satisfactory closure rate
- Acceptable cost (outpatient procedure)
• Observational, non-randomized data suggest a lower risk of recurrence as compared to medical treatment alone
• No randomized trial published to date
• Limitations of ongoing randomized trials- High risk patients closed with device, not randomized
- Follow-up too short
Patient Population
Inclusion CriteriaAll patients with ischemic stroke or TIA, confirmed clinically or radiologically at the University Hospital of Bern Stroke Center between January 1994 and August 2000 were prospectively entered into the stroke/PFO registry if they had
- PFO ± atrial septal aneurysm (contrast TEE)
Exclusion CriteriaObvious other cardiac, aortic, or cerebrovascular cause
Treatment decisionBased on consensus among neurologist and patient

Patient Flow – Intention to Treat Analysis308 Patients
Jan. 1994 – Aug. 2000
Medical treatment alone158 patients
Percutaneous PFO closure150 patients
Medical treatment alone103 Patients
Percutaneous PFO closure103 Patients
Clinical Follow-upMedian 10.3 years
1,170 patient-years1,011 patient-years
After Propensity Score Matching 206 Patients
- 6 brands used- 42% Amplatzer occluders- 6% acute complications (no sequelae), no late
complications- 87% complete closure, 4% after 2nd intervention
- 50% antiplatelet therapy - 50% warfarin
- 27% PFO closure during follow-up
All neurovascular events adjudicated by neurologist
(Windecker S, JACC 44: 750-8, 2004)

PFO Closure150 Patients
Medical Treatment158 Patients
P
Age 50±12 51±13 0.55
Male , % 54 58 0.39
Diabetes mellitus, % 4 9 0.08
Hypertension, % 28 32 0.49
Hypercholesterolemia, % 45 29 0.003
Smoking, % 33 32 0.94
Cerebrovascular index event, % 0.022
- Ischemic stroke 65 77
- TIA 35 23
Mean number of CV events 1.8±1.1 1.5±1.0 0.025
More than 1 CV event, % 39 28 0.033
Patient Characteristics Before Propensity Score Matching (N=308)

PFO Closure103 Patients
Medical Treatment103 Patients
P
Age 49±12 50±13 0.65
Male , % 52 55 0.68
Diabetes mellitus, % 5 3 0.47
Hypertension, % 26 30 0.54
Hypercholesterolemia, % 29 35 0.37
Smoking, % 30 31 0.88
Cerebrovascular index event, % 0.44
- Ischemic stroke 75 70
- TIA 25 30
Mean number of CV events 1.5±1.0 1.5±0.9 0.88
More than 1 CV event, % 25 28 0.64
Patient Characteristics After Propensity Score Matching (N=206)

PFO Closure150 Patients
Medical Treatment158 Patients
P
Atrial septal anatomy, % 0.6
- PFO only 75 78
- PFO and atrial septal aneurysm 25 22
Interatrial shunt grade, % 0.001
- Small 3 11
- Moderate 17 28
- Large 79 61
Patient Characteristics Before Propensity Score Matching (N=308)

PFO Closure103 Patients
Medical Treatment103 Patients
P
Atrial septal anatomy, % 0.41
- PFO only 74 79
- PFO and atrial septal aneurysm 26 21
Interatrial shunt grade, % 0.40
- Small 4 9
- Moderate 11 21
- Large 74 70
Patient Characteristics After Propensity Score Matching (N=206)
0
5
10
15
20
25
30
Cum
ula
tive
inci
denc
e(%
)
103 96 94 89 87 85 84 82 82 54 28Medical103 103 100 98 98 98 98 97 96 60 29PFO closure
No. at risk
0 1 2 3 4 5 6 7 8 9 10Follow-up, years
__ PFO Closure- - - Medical
p=0.033
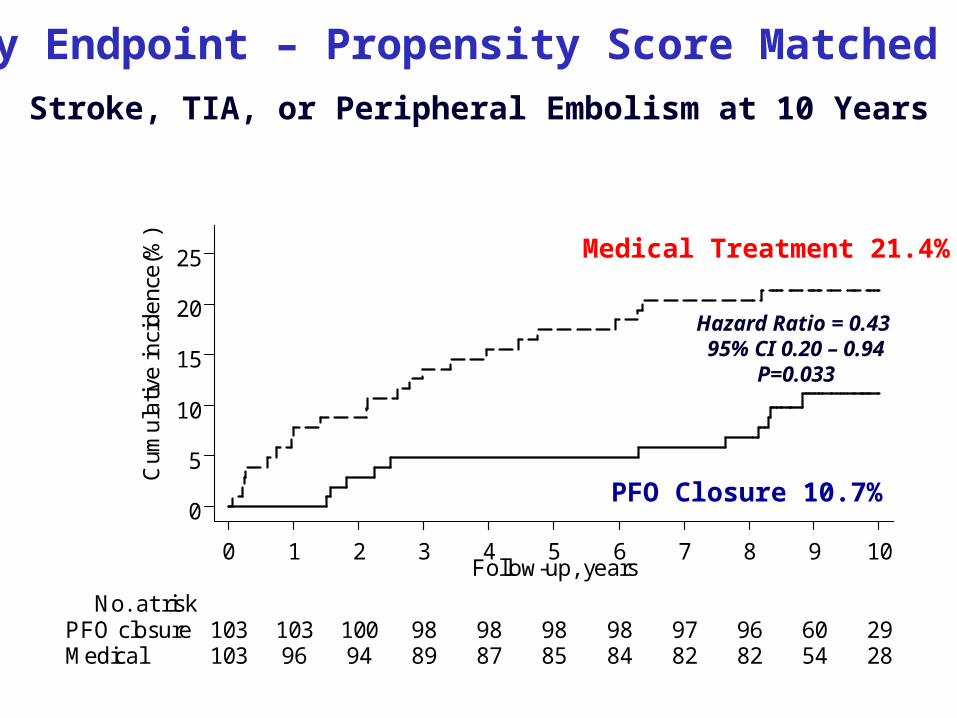
Stroke, TIA or Peripheral Embolism
Primary Endpoint – Propensity Score Matched Cohort
Hazard Ratio = 0.43 95% CI 0.20 – 0.94
P=0.033
Stroke, TIA, or Peripheral Embolism at 10 Years
PFO Closure 10.7%
Medical Treatment 21.4%
0
5
10
15
20
25
Cum
ula
tive
inci
denc
e(%
)
103 101 101 101 101 101 101 99 98 64 30Medical103 102 102 102 101 101 101 101 99 64 32PFO closure
No. at risk
0 1 2 3 4 5 6 7 8 9 10Follow-up, years
__ PFO Closure- - - Medical
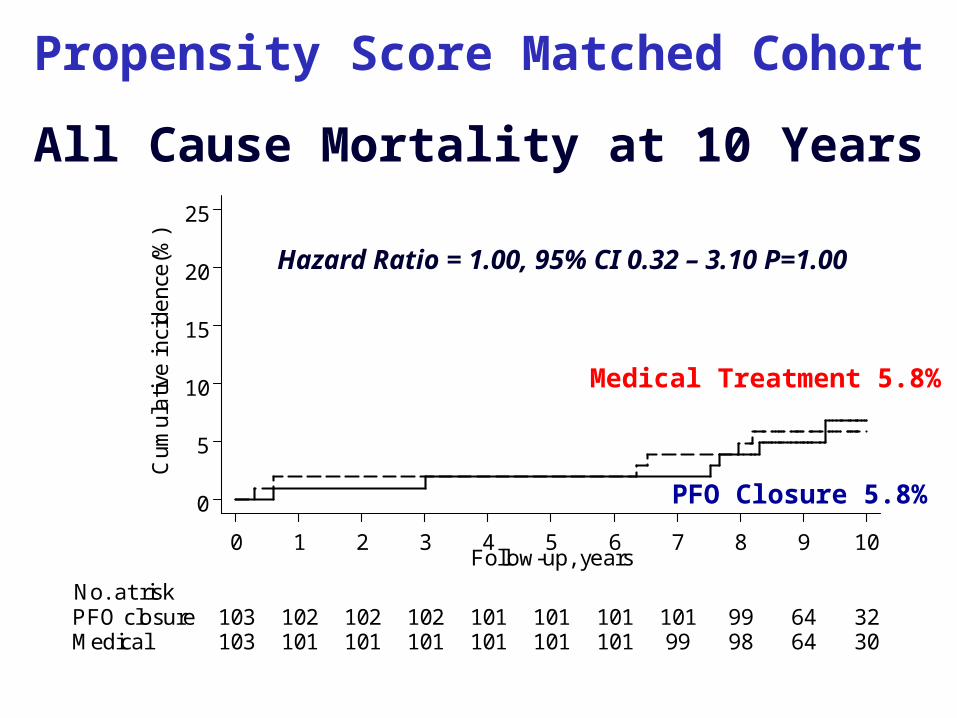
p=1.00
Death
Medical Treatment 5.8%
PFO Closure 5.8%
Hazard Ratio = 1.00, 95% CI 0.32 – 3.10 P=1.00
Propensity Score Matched Cohort
All Cause Mortality at 10 Years

0
5
10
15
20
25
Cum
ula
tive
inci
denc
e(%
)
103 101 100 98 97 97 97 96 96 65 31Medical103 103 102 102 102 102 102 101 100 65 31PFO closure
No. at risk
0 1 2 3 4 5 6 7 8 9 10Follow-up, years
__ PFO Closure- - - Medical
p=0.59
Stroke
Medical Treatment 7.8%
PFO Closure 5.8%
Hazard Ratio = 0.75, 95% CI 0.26 – 2.16, P=0.59
Ischemic Stroke at 10 Years
Propensity Score Matched Cohort

0
5
10
15
20
25
Cum
ula
tive
inci
denc
e(%
)
103 98 97 94 93 91 90 89 89 57 30Medical103 103 101 99 99 99 99 99 99 63 31PFO closure
No. at risk
0 1 2 3 4 5 6 7 8 9 10Follow-up, years
__ PFO Closure- - - Medical
p=0.039
TIA
Medical Treatment 13.6%
PFO Closure 4.9%
Hazard Ratio = 0.3195% CI 0.10 – 0.94
P=0.039
Transient Ischemic Attack at 10 Years
Propensity Score Matched Cohort

.1 .15 .2 .25 .5 1 2 4 6
PFO closure better Medical tr. better
0.43 (0.20-0.94)Overall 0.033
0.42 (0.15-1.18)PFO only0.61 (0.20-1.86)PFO and ASA
0.54
0.33 (0.09-1.23)Age <55 yrs0.690.50 (0.09-2.73)Age ≥55 yrs
0.14 (0.03-0.76)Female0.071.00 (0.29-3.45)Male
0.25 (0.03-2.24)No severe shunt 0.210.70 (0.27-1.84)Severe shunt
1.00 (0.35-2.85)≤1 event0.0740.22 (0.06-0.80)>1 event
0.04 (0.00-0.63)Index event TIA0.0390.86 (0.29-2.55)Index event stroke
HR (95% CI) PStroke/TIA/Periph. Embol.Propensity-Matched Cohort

0
5
10
15
20
25
30
Cu
mul
ativ
e in
cide
nce(
%)
158 149 144 137 135 131 130 128 127 126 124Medical150 148 144 142 142 142 142 141 140 136 136PFO closure
No. at risk
0 1 2 3 4 5 6 7 8 9 10Follow-up, years
__ PFO Closure- - - Medical
p=0.004
Stroke, TIA or Peripheral Embolism Primary Endpoint – Intention to Treat Population
PFO Closure 9.3%
Hazard Ratio = 0.4095% CI 0.22 – 0.75
P=0.004
Medical Treatment 21.5%
Ischemic Stroke, TIA, or Peripheral Embolism at 10 Years

0
5
10
15
Cu
mul
ativ
e in
cide
nce(
%)
158 155 154 153 153 153 152 149 146 145 145Medical150 149 149 149 147 147 147 147 145 144 143PFO closure
No. at risk
0 1 2 3 4 5 6 7 8 9 10Follow-up, years
__ PFO Closure- - - Medical
p=0.21
Death
Medical Treatment 8.2%
PFO Closure 4.7%
Hazard Ratio = 0.55, 95% CI 0.22 - 1.38, P=0.21
All Cause Mortality at 10 Years
Intention to Treat Population (N=308)
0
5
10
15
Cu
mul
ativ
e in
cide
nce(
%)
158 153 151 146 145 142 141 140 140 140 140Medical150 149 146 144 144 144 144 144 144 143 143PFO closure
No. at risk
0 1 2 3 4 5 6 7 8 9 10Follow-up, years
__ PFO Closure- - - Medical
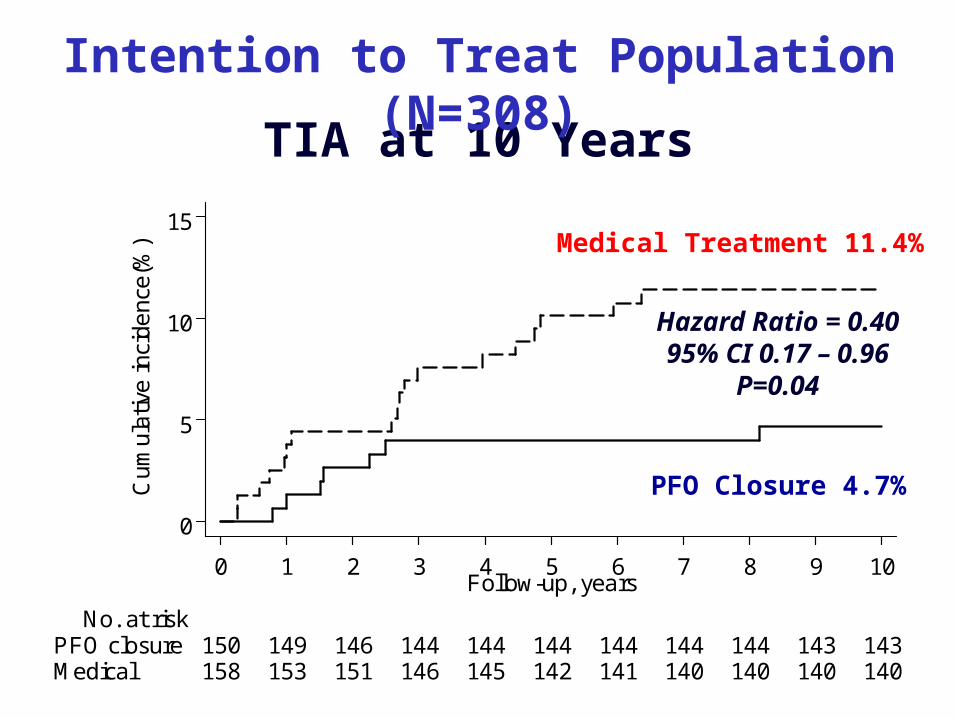
p=0.04
TIA
Medical Treatment 11.4%
PFO Closure 4.7%
Hazard Ratio = 0.4095% CI 0.17 – 0.96
P=0.04
TIA at 10 Years
Intention to Treat Population (N=308)
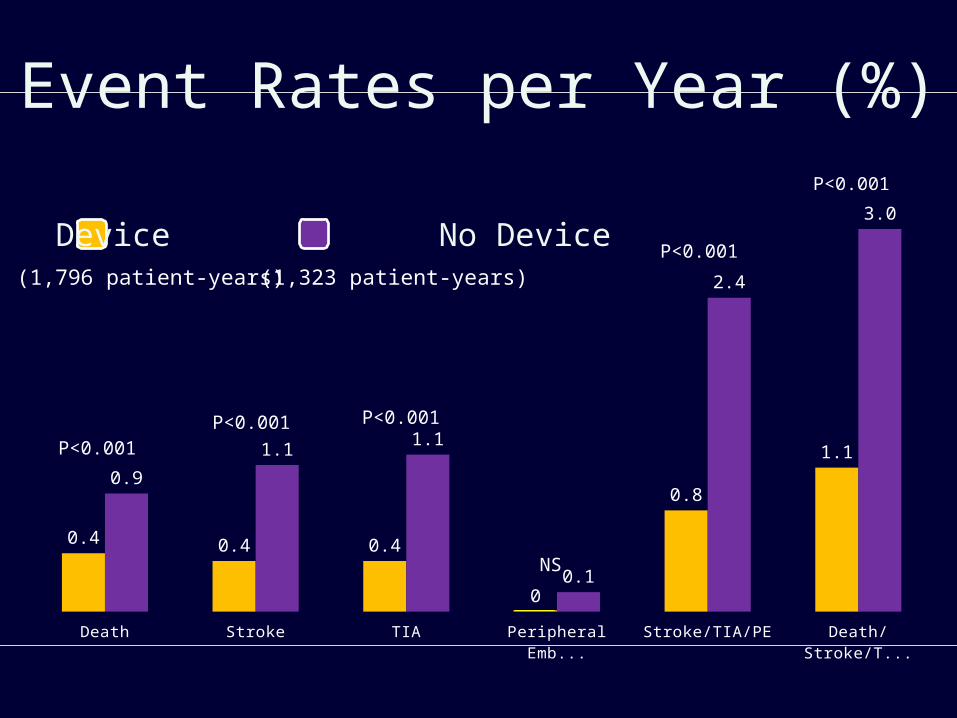
Death Stroke TIA Peripheral Embolism
Stroke/TIA/PE Death/Stroke/TIA/PE
0.4 0.4 0.4
0
0.8
1.1
0.9
1.11.1
0.1
2.4
3.0
P<0.001
P<0.001
P<0.001P<0.001 P<0.001
Event Rates per Year (%)
NS
(1,796 patient-years) (1,323 patient-years)
Device No Device
Conclusions• PFO closure appears more effective
than medical treatment for secondary prevention of recurrent cerebrovascular events among patients with stroke or TIA presumably related to PFO.
• Less death, stroke, or TIA with a PFO closure device than without.
• Results require confirmation in randomized clinical trials.







