Management of Multiple Myeloma: The Changing Paradigm
Relapsed/Refractory Disease

Patient Case• A 64-yr-old woman comes with relapsed
myeloma. Her history is as follows:
– Initial studies 3 years ago showed 55% plasma cells in the bone marrow, hyperdiploidy, IgGκ 3.5 g/dL, and multiple lytic lesions
– Initially treated with RVD, followed by high-dose melphalan and peripheral blood stem cell transplantation
– She achieved a CR and was on observation
– 3 yrs later, M-protein reappears to 1.5 g/dL
• What is the right choice of therapy for her?
– Carfilzomib/lenalidomide/dex
– Ixazomib/lenalidomdie/dex
– Elotuzumab/lenalidomide/dex
– Evaluation for clinical trial
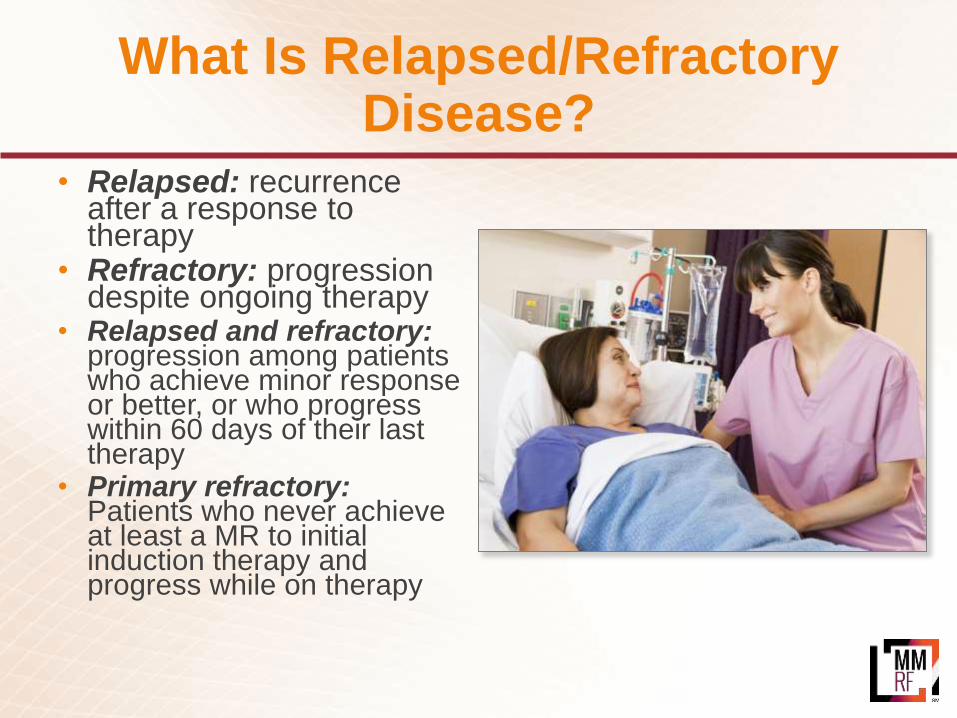
What Is Relapsed/Refractory Disease?
• Relapsed: recurrence after a response to therapy
• Refractory: progression despite ongoing therapy
• Relapsed and refractory: progression among patients who achieve minor response or better, or who progress within 60 days of their last therapy
• Primary refractory: Patients who never achieve at least a MR to initial induction therapy and progress while on therapy
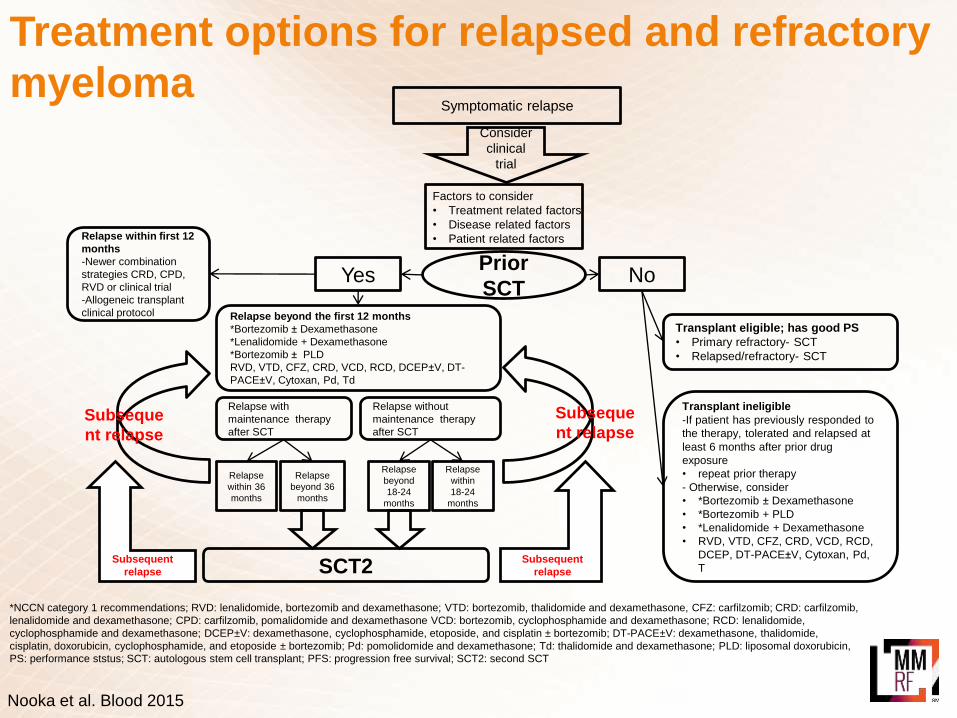
Treatment options for relapsed and refractory
myelomaConsider
clinical
trial
Prior
SCT
Transplant eligible; has good PS
• Primary refractory- SCT
• Relapsed/refractory- SCT
Transplant ineligible
-If patient has previously responded to
the therapy, tolerated and relapsed at
least 6 months after prior drug
exposure
• repeat prior therapy
- Otherwise, consider
• *Bortezomib ± Dexamethasone
• *Bortezomib + PLD
• *Lenalidomide + Dexamethasone
• RVD, VTD, CFZ, CRD, VCD, RCD,
DCEP, DT-PACE±V, Cytoxan, Pd,
T
Relapse within first 12
months
-Newer combination
strategies CRD, CPD,
RVD or clinical trial
-Allogeneic transplant
clinical protocol
Symptomatic relapse
Yes No
Relapse with
maintenance therapy
after SCT
Relapse without
maintenance therapy
after SCT
Factors to consider
• Treatment related factors
• Disease related factors
• Patient related factors
Subseque
nt relapse
*NCCN category 1 recommendations; RVD: lenalidomide, bortezomib and dexamethasone; VTD: bortezomib, thalidomide and dexamethasone, CFZ: carfilzomib; CRD: carfilzomib,
lenalidomide and dexamethasone; CPD: carfilzomib, pomalidomide and dexamethasone VCD: bortezomib, cyclophosphamide and dexamethasone; RCD: lenalidomide,
cyclophosphamide and dexamethasone; DCEP±V: dexamethasone, cyclophosphamide, etoposide, and cisplatin ± bortezomib; DT-PACE±V: dexamethasone, thalidomide,
cisplatin, doxorubicin, cyclophosphamide, and etoposide ± bortezomib; Pd: pomolidomide and dexamethasone; Td: thalidomide and dexamethasone; PLD: liposomal doxorubicin,
PS: performance ststus; SCT: autologous stem cell transplant; PFS: progression free survival; SCT2: second SCT
SCT2
Relapse
within 36
months
Relapse
beyond 36
months
Relapse
beyond
18-24
months
Relapse
within
18-24
months
Subsequent
relapse
Subsequent
relapse
Subseque
nt relapse
Relapse beyond the first 12 months
*Bortezomib ± Dexamethasone
*Lenalidomide + Dexamethasone
*Bortezomib ± PLD
RVD, VTD, CFZ, CRD, VCD, RCD, DCEP±V, DT-
PACE±V, Cytoxan, Pd, Td
Nooka et al. Blood 2015
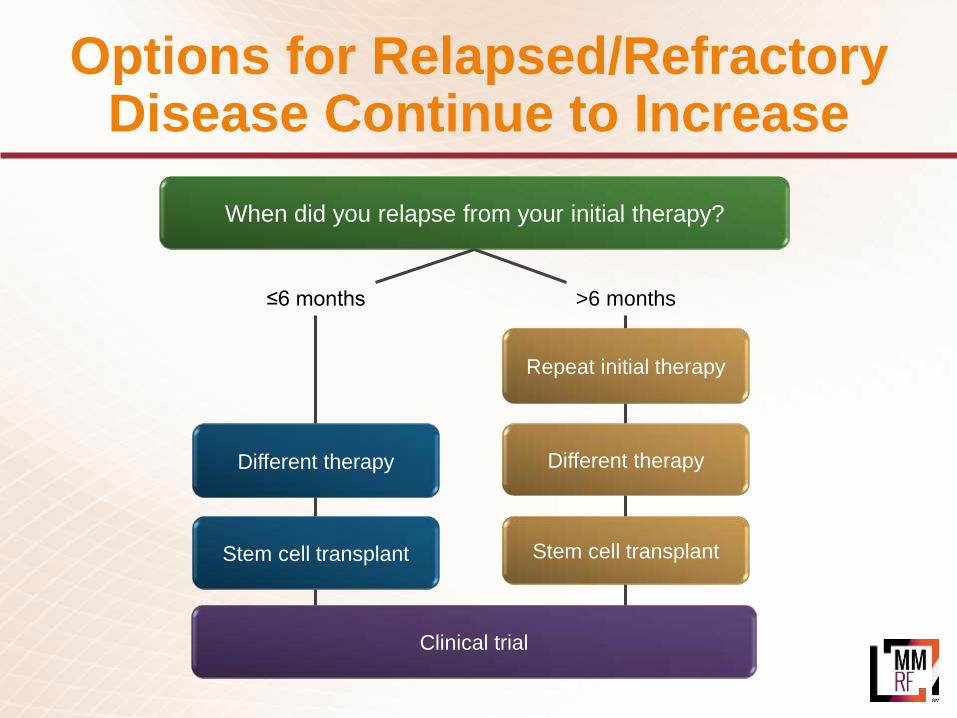
Options for Relapsed/Refractory Disease Continue to Increase
When did you relapse from your initial therapy?
≤6 months
Different therapy
Stem cell transplant
>6 months
Stem cell transplant
Different therapy
Repeat initial therapy
Clinical trial

Factors to Consider in Treatment Selection
DISEASE-RELATED
• DOR to initial therapy• FISH/cytogenetics/genomics profile
PRIOR TREATMENT–RELATED
• Prior drug exposure• Toxicity of regimen• Mode of administration• Previous SCT
PATIENT-RELATED
• Pre-existing toxicity• Presence of other conditions• Age• General health• Personal lifestyle and preferences
DOR, duration of response; FISH, fluorescence in situ hybridization; SCT, stem cell transplantLonial S. Hematology Am Soc Hematol Educ Program. 2010;303.

Options at First Relapse

Proteasome Inhibitor:Kyprolis (carfilzomib)
*Overall response rate = complete response (CR) + very good partial response (VGPR) + partial response (PR) + minimal response (MR)
• Used alone (after two or more therapies):
− 23% overall response rate (CR + VGPR + PR + MR)
− On average, responses last 7.8 months
• In patients who have never received Velcade:
− 42% overall response rate
− On average, responses last 13 months
How effective is it?
• In combination with dex or with Revlimid + dex for the treatment of patients with relapsed or refractory MM who have received one to three lines of therapy
• As a single agent for the treatment of patients with relapsed or refractory MM who have received one or more lines of therapy
FDA-approved indication
• Standard: Kyprolis used alone or in combination with dex or in combination with Revlimid and dex
• Under investigation: combinations with Farydak, IMiDs such as Revlimid and Pomalyst, experimental therapies (for example, SAR650984, filanesib)
What combinations are used?
• High-risk features (for example, t(4;14) or 17p13 del or elevated β2-microglobulin)
• History of previous neuropathy
• Safe for patients with reduced kidney function
Who should take it?
Kyprolis (carfilzomib)
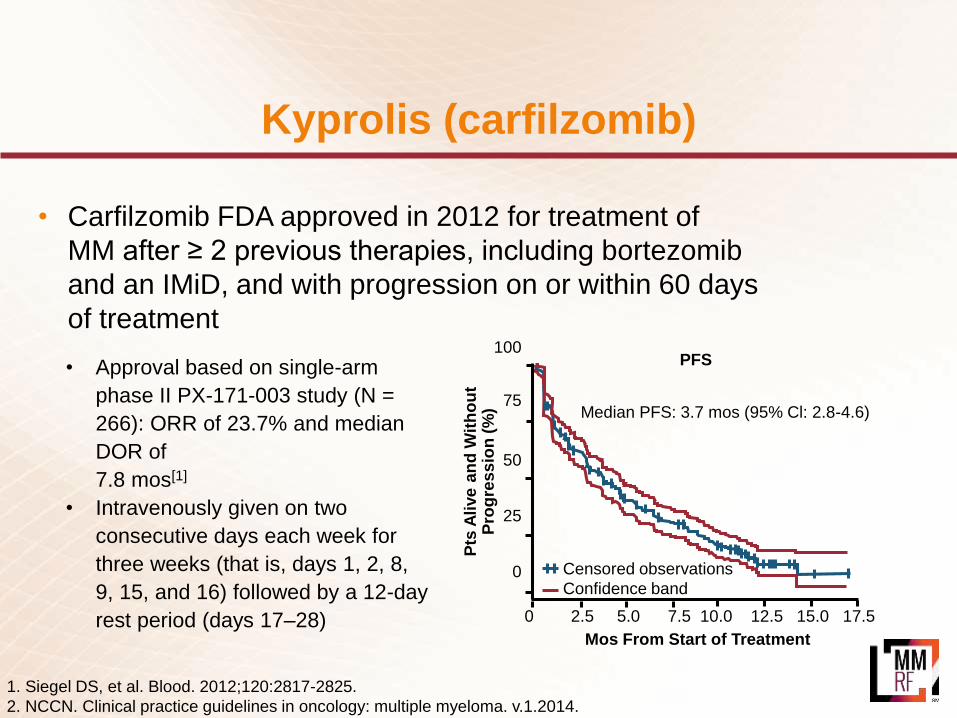
• Carfilzomib FDA approved in 2012 for treatment of
MM after ≥ 2 previous therapies, including bortezomib
and an IMiD, and with progression on or within 60 days
of treatment
1. Siegel DS, et al. Blood. 2012;120:2817-2825.
2. NCCN. Clinical practice guidelines in oncology: multiple myeloma. v.1.2014.
PFS
0 2.5 5.0 7.5 10.0 12.5 15.0 17.5
100
75
50
25
0
Median PFS: 3.7 mos (95% Cl: 2.8-4.6)
Mos From Start of Treatment
Pts
Alive a
nd
Wit
ho
ut
Pro
gre
ssio
n (
%)
Censored observations
Confidence band
• Approval based on single-arm
phase II PX-171-003 study (N =
266): ORR of 23.7% and median
DOR of
7.8 mos[1]
• Intravenously given on two
consecutive days each week for
three weeks (that is, days 1, 2, 8,
9, 15, and 16) followed by a 12-day
rest period (days 17–28)
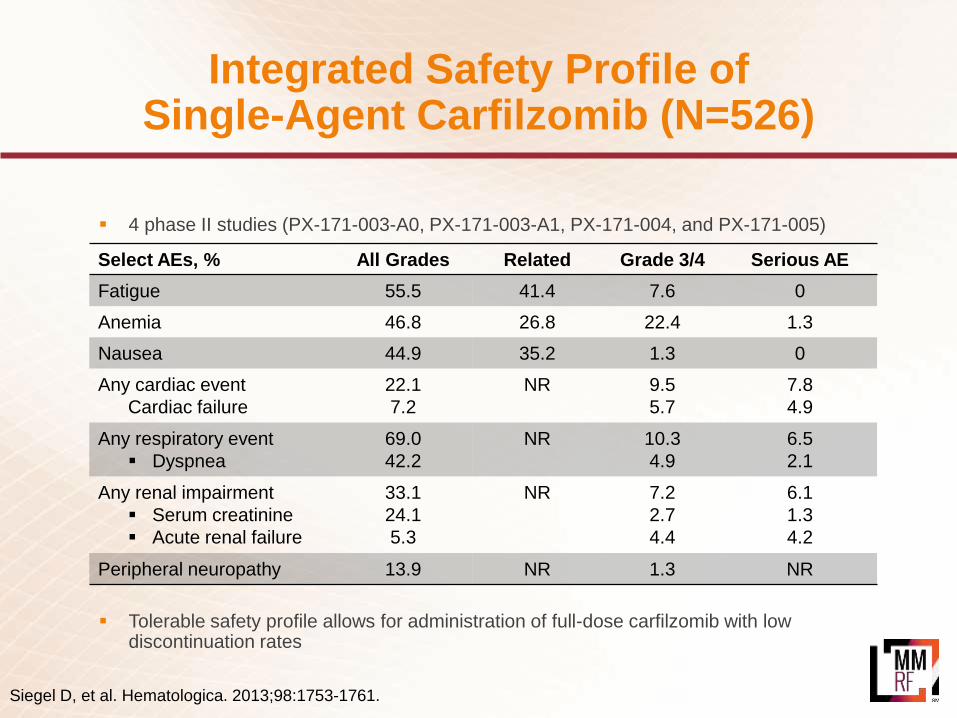
Integrated Safety Profile of Single-Agent Carfilzomib (N=526)
4 phase II studies (PX-171-003-A0, PX-171-003-A1, PX-171-004, and PX-171-005)
Tolerable safety profile allows for administration of full-dose carfilzomib with low discontinuation rates
Siegel D, et al. Hematologica. 2013;98:1753-1761.
Select AEs, % All Grades Related Grade 3/4 Serious AE
Fatigue 55.5 41.4 7.6 0
Anemia 46.8 26.8 22.4 1.3
Nausea 44.9 35.2 1.3 0
Any cardiac event
Cardiac failure
22.1
7.2
NR 9.5
5.7
7.8
4.9
Any respiratory event
Dyspnea
69.0
42.2
NR 10.3
4.9
6.5
2.1
Any renal impairment
Serum creatinine
Acute renal failure
33.1
24.1
5.3
NR 7.2
2.7
4.4
6.1
1.3
4.2
Peripheral neuropathy 13.9 NR 1.3 NR

Berenson J, ASH 2015 Abst 373
CarfilzomibDays 1, 8, and 15
Duration of infusion: 30 minutes
and
Dexamethasone IV or PODays 1, 8, 15, and 22 (day 22 omitted for cycles 9+)
Both drugs given until PD or unacceptable toxicity
IV, intravenous; MTD, maximum tolerated dose; PD, progressive disease: PO, per oral.
Treatment Schedule (Phase 1 and 2)
Carfilzomib (mg/m2)a Dexamethasone (mg)
Phase 1 (3+3 dose-escalation schema)
Dose level 1 45 40
Dose level 2 56 40
Dose level 3 70 40
Dose level 4 88 40
Phase 2 MTD from phase 1 40aCarfilzomib 20 mg/m2 was administered to all patients on only cycle 1 day 1.
Dosing
28 day cycles:
CHAMPION-1 Study Design
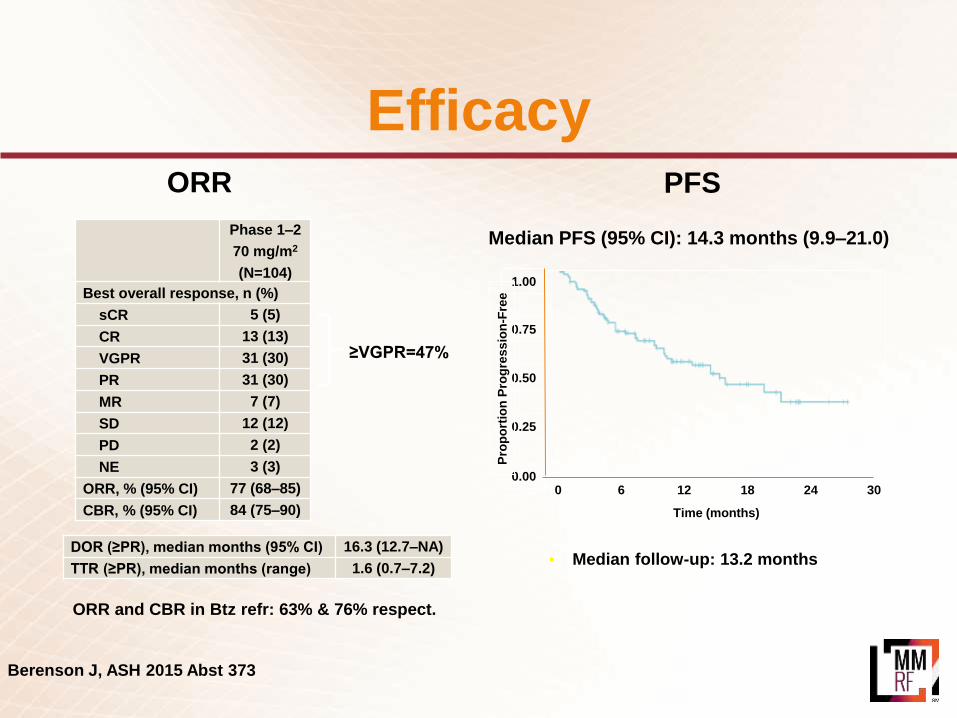
• Median follow-up: 13.2 months
Median PFS (95% CI): 14.3 months (9.9–21.0)
1.00
0.75
0.50
0.25
0.00
Pro
po
rtio
n P
rog
ressio
n-F
ree
0 6 12 18 24
Time (months)
30
PFS ORR
Phase 1–2
70 mg/m2
(N=104)
Best overall response, n (%)
sCR 5 (5)
CR 13 (13)
VGPR 31 (30)
PR 31 (30)
MR 7 (7)
SD 12 (12)
PD 2 (2)
NE 3 (3)
ORR, % (95% CI) 77 (68–85)
CBR, % (95% CI) 84 (75–90)
≥VGPR=47%
DOR (≥PR), median months (95% CI) 16.3 (12.7–NA)
TTR (≥PR), median months (range) 1.6 (0.7–7.2)
ORR and CBR in Btz refr: 63% & 76% respect.
Berenson J, ASH 2015 Abst 373
Efficacy
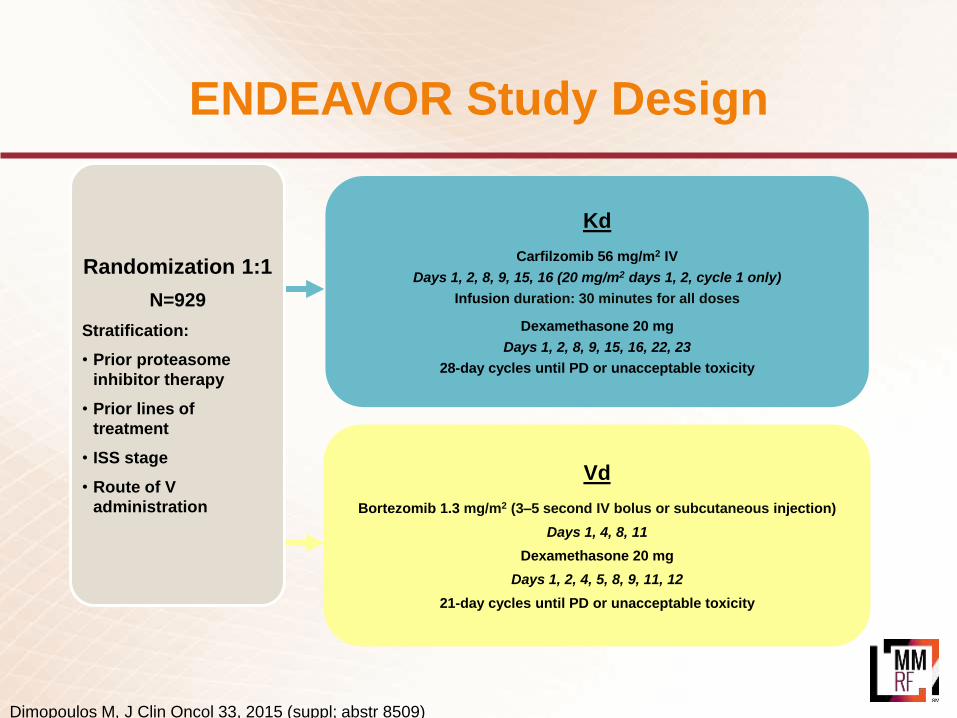
ENDEAVOR Study Design
Vd
Bortezomib 1.3 mg/m2 (3–5 second IV bolus or subcutaneous injection)
Days 1, 4, 8, 11
Dexamethasone 20 mg
Days 1, 2, 4, 5, 8, 9, 11, 12
21-day cycles until PD or unacceptable toxicity
Kd
Carfilzomib 56 mg/m2 IV
Days 1, 2, 8, 9, 15, 16 (20 mg/m2 days 1, 2, cycle 1 only)
Infusion duration: 30 minutes for all doses
Dexamethasone 20 mg
Days 1, 2, 8, 9, 15, 16, 22, 23
28-day cycles until PD or unacceptable toxicity
Randomization 1:1
N=929
Stratification:
• Prior proteasome
inhibitor therapy
• Prior lines of
treatment
• ISS stage
• Route of V
administration
Dimopoulos M, J Clin Oncol 33, 2015 (suppl; abstr 8509)

Primary End Point: Progression-Free SurvivalIntent-to-Treat Population (N=929)
1.0
0.8
0.6
0.4
0.2
0
Pro
port
ion S
urv
ivin
g
Without P
rogre
ssio
n
0
Months Since Randomization
Kd
Vd
Kd
(n=464)
171 (37)
18.7
Vd
(n=465)
243 (52)
9.40.53 (0.44–0.65); 1-sided P<0.0001
Disease progression or death – n (%)
Median PFS – months
HR for Kd vs Vd (95% CI)
• Median follow-up: 11.2 months
6 12 18 24 30
Dimopoulos M, J Clin Oncol 33, 2015 (suppl; abstr 8509)

ASPIRE Study Design
Rd
Lenalidomide 25 mg Days 1–21
Dexamethasone 40 mg Days 1, 8, 15, 22
KRd
Carfilzomib 27 mg/m2 IV (10 min)
Days 1, 2, 8, 9, 15, 16 (20 mg/m2 days 1, 2, cycle 1 only)
Lenalidomide 25 mg Days 1–21
Dexamethasone 40 mg Days 1, 8, 15, 22
Randomization
N=792
Stratification:
• β2-microglobulin
• Prior bortezomib
• Prior lenalidomide
After cycle 12, carfilzomib given on days 1, 2, 15, 16
After cycle 18, carfilzomib discontinued
28-day cycles
Stewart K, et al. N Engl J Med 2015; 372:142-152
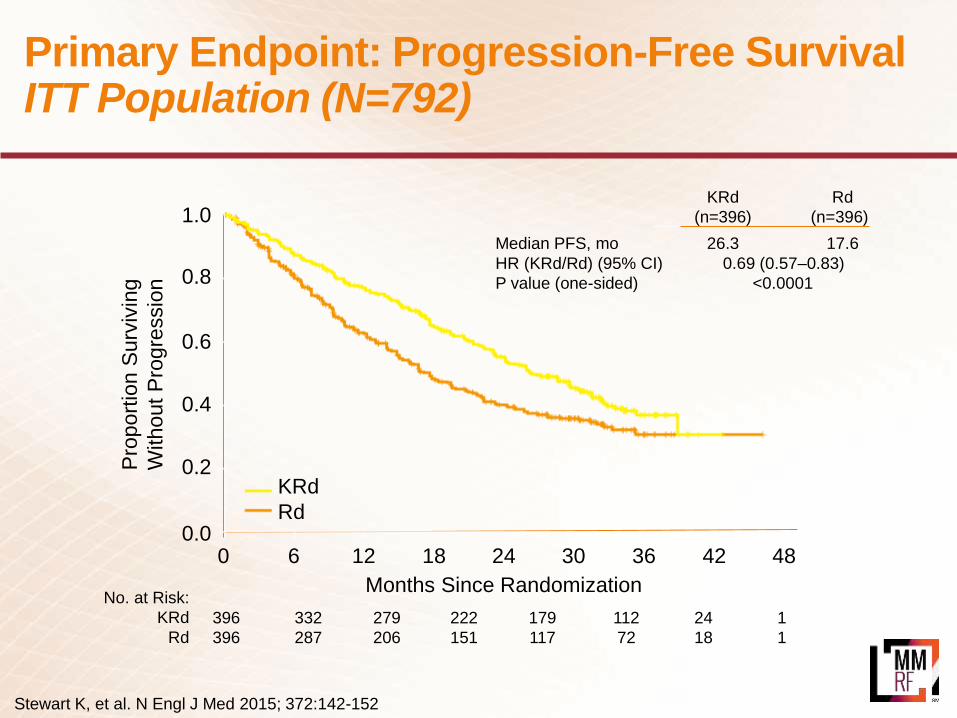
Primary Endpoint: Progression-Free SurvivalITT Population (N=792)
1.0
0.8
0.6
0.4
0.2
0.0
Pro
port
ion S
urv
ivin
g
Without
Pro
gre
ssio
n
KRd
Rd
0 6 12 18 24 30 36 42 48
Months Since Randomization
KRd Rd
(n=396) (n=396)
Median PFS, mo 26.3 17.6
HR (KRd/Rd) (95% CI) 0.69 (0.57–0.83)
P value (one-sided) <0.0001
No. at Risk:
KRd
Rd
396 332 279 222 179 112 24 1
396 287 206 151 117 72 18 1
Stewart K, et al. N Engl J Med 2015; 372:142-152

Proteasome Inhibitor:Ninlaro (ixazomib)
• 78% overall response rate (PR or better)How effective is it?
• In combination with Revlimid and dex for the treatment of patients with MM who have received at least one prior therapy
FDA-approved indication
• Standard: With Revlimid and dex
• Under investigation: with Treanda or Pomalyst in RR patients or with Revlimid in newly diagnosed patients
What combinations are used?
• Relapsed or relapsed/refractory following at least one prior therapy Who should take it?
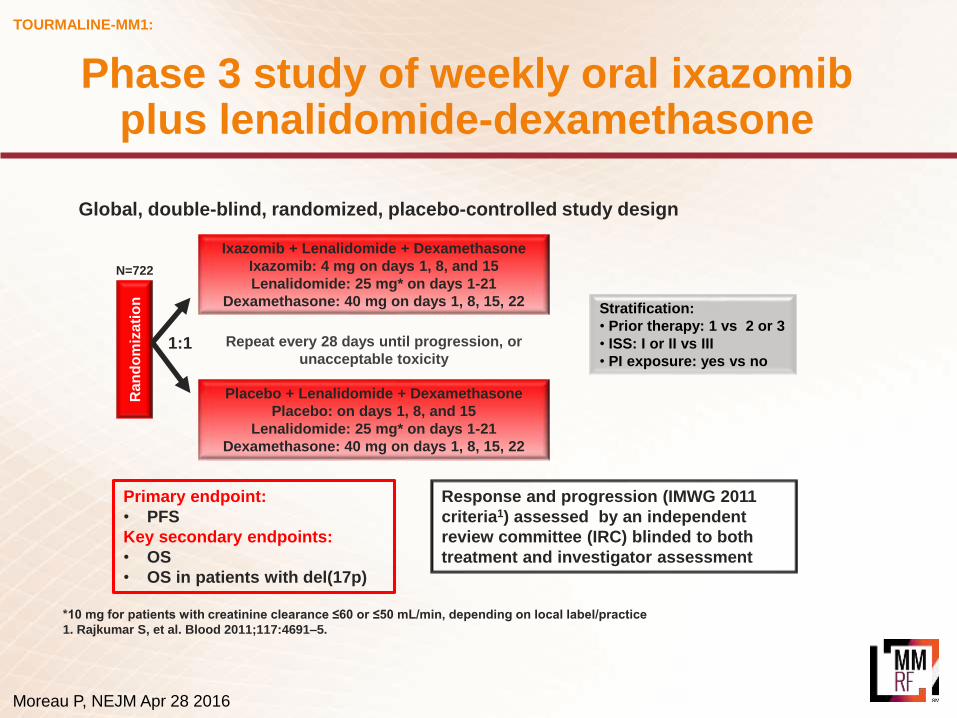
TOURMALINE-MM1:
Ra
nd
om
iza
tio
n
Ixazomib + Lenalidomide + Dexamethasone
Ixazomib: 4 mg on days 1, 8, and 15
Lenalidomide: 25 mg* on days 1-21
Dexamethasone: 40 mg on days 1, 8, 15, 22
N=722
1:1
Placebo + Lenalidomide + Dexamethasone
Placebo: on days 1, 8, and 15
Lenalidomide: 25 mg* on days 1-21
Dexamethasone: 40 mg on days 1, 8, 15, 22
Repeat every 28 days until progression, or
unacceptable toxicity
Stratification:
• Prior therapy: 1 vs 2 or 3
• ISS: I or II vs III
• PI exposure: yes vs no
Global, double-blind, randomized, placebo-controlled study design
*10 mg for patients with creatinine clearance ≤60 or ≤50 mL/min, depending on local label/practice
1. Rajkumar S, et al. Blood 2011;117:4691–5.
Response and progression (IMWG 2011
criteria1) assessed by an independent
review committee (IRC) blinded to both
treatment and investigator assessment
Primary endpoint:
• PFS
Key secondary endpoints:
• OS
• OS in patients with del(17p)
Moreau P, NEJM Apr 28 2016
Phase 3 study of weekly oral ixazomibplus lenalidomide-dexamethasone

TOURMALINE-MM1:
A significant, 35% improvement in PFS with IRd vs placebo-Rd
Number of patients at risk:
IRd
Placebo-Rd
360 345 332 315 298 283 270 248 233 224 206 182 145 119 111 95 72 58 44 34 26 14 9 1 0
362 340 325 308 288 274 254 237 218 208 188 157 130 101 85 71 58 46 31 22 15 5 3 0 0
1.0
0.8
0.6
0.4
0.2
0.0
0 1 2 3 4 5 6 7 8 9 1
0
1
1
1
2
1
3
1
4
1
5
1
6
1
7
1
8
1
9
2
0
2
1
2
2
2
3
2
4
Pro
bab
ilit
y o
f p
rog
ressio
n-f
ree s
urv
ival
Time from randomization (months)
Log-rank test p=0.012
Hazard ratio (95% CI): 0.742 (0.587, 0.939)
Number of events: IRd 129; placebo-Rd 157
Median PFS:
IRd: 20.6 months
Placebo-Rd: 14.7 months
Median follow-up: ~15 months
Interim OS analysis @ 23 months of FU: 81 and 90 deaths in ixazomib and placebo, respectively
Moreau P, NEJM Apr 28 2016
Final PFS analysis
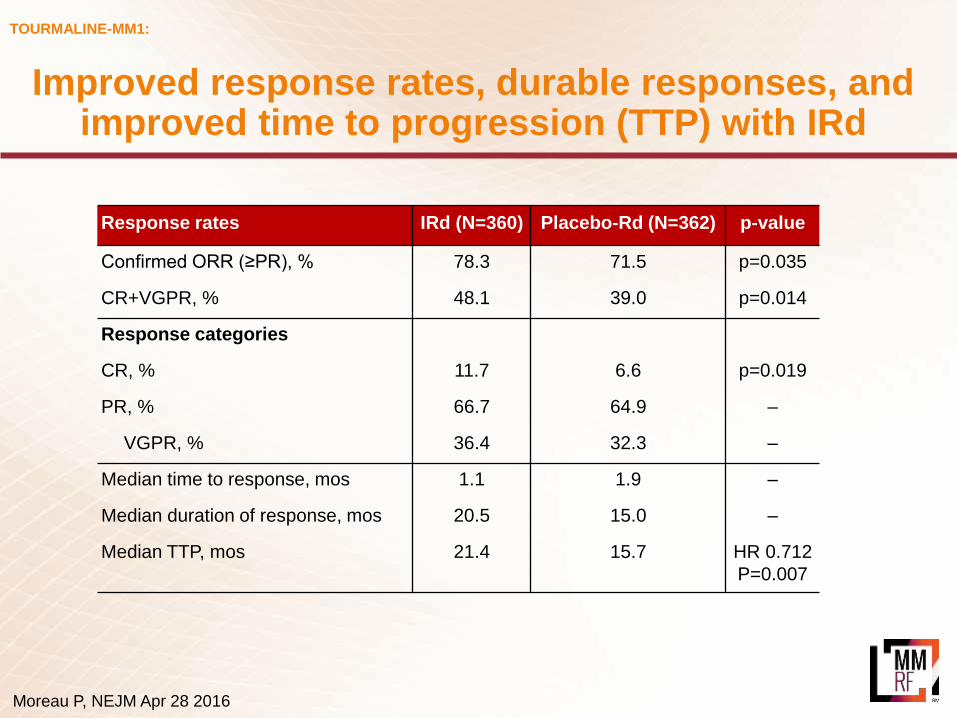
TOURMALINE-MM1:
Response rates IRd (N=360) Placebo-Rd (N=362) p-value
Confirmed ORR (≥PR), % 78.3 71.5 p=0.035
CR+VGPR, % 48.1 39.0 p=0.014
Response categories
CR, % 11.7 6.6 p=0.019
PR, % 66.7 64.9 –
VGPR, % 36.4 32.3 –
Median time to response, mos 1.1 1.9 –
Median duration of response, mos 20.5 15.0 –
Median TTP, mos 21.4 15.7 HR 0.712
P=0.007
Moreau P, NEJM Apr 28 2016
Improved response rates, durable responses, and improved time to progression (TTP) with IRd
Proteasome Inhibitor:Ninlaro (ixazomib)
• Common side effects include:
− Diarrhea
− Constipation
− Thrombocytopenia
− Peripheral neuropathy
− Nausea
− Peripheral edema
− Vomiting
− Back pain
What are the possible side effects?
• Oral
• Days 1, 8, and 15 of a 28-day cycle
How is Ninlaro administered?
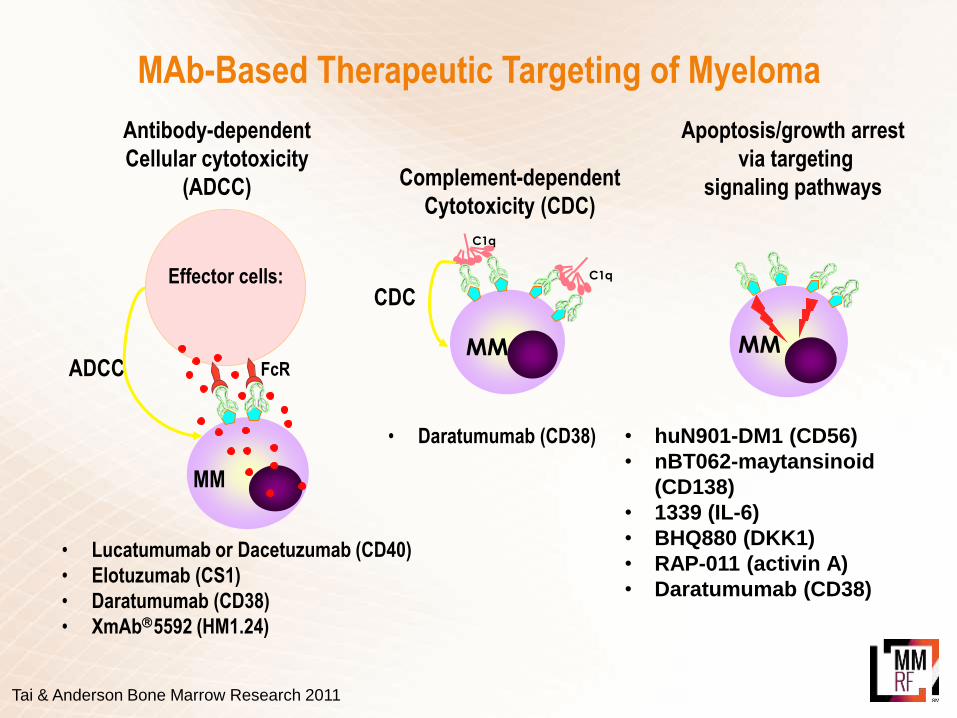
Antibody-dependent
Cellular cytotoxicity
(ADCC)
ADCC
Effector cells:
MM
FcR
Complement-dependent
Cytotoxicity (CDC)
CDC
MM
C1q
C1q
Apoptosis/growth arrest
via targeting
signaling pathways
MM
• Lucatumumab or Dacetuzumab (CD40)
• Elotuzumab (CS1)
• Daratumumab (CD38)
• XmAb5592 (HM1.24)
• huN901-DM1 (CD56)
• nBT062-maytansinoid
(CD138)
• 1339 (IL-6)
• BHQ880 (DKK1)
• RAP-011 (activin A)
• Daratumumab (CD38)
• Daratumumab (CD38)
MAb-Based Therapeutic Targeting of Myeloma
Tai & Anderson Bone Marrow Research 2011
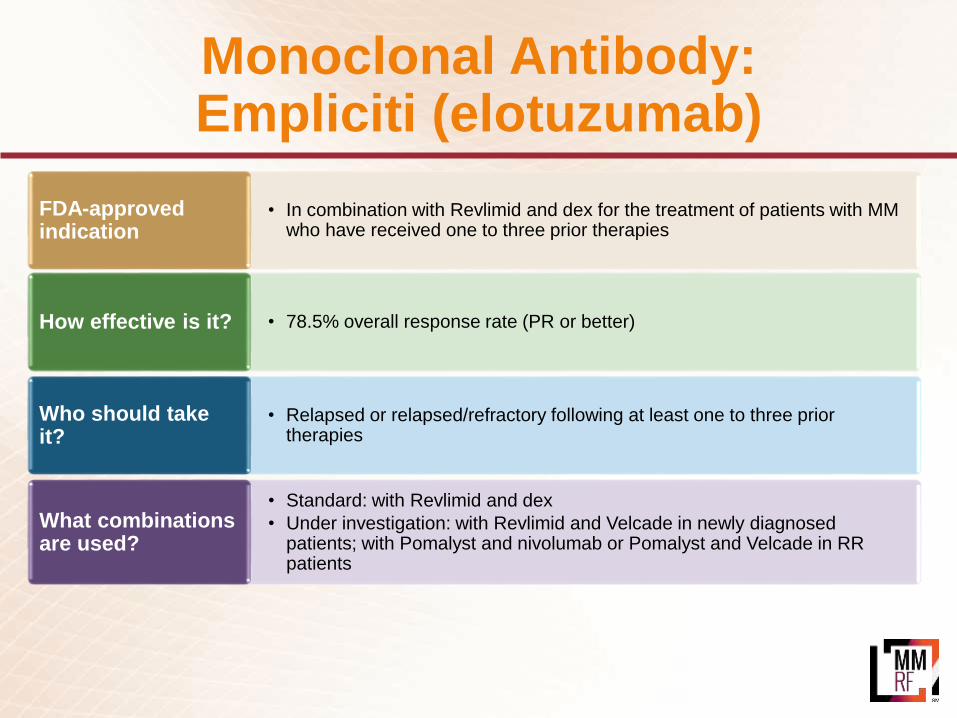
Monoclonal Antibody:Empliciti (elotuzumab)
• 78.5% overall response rate (PR or better)How effective is it?
• In combination with Revlimid and dex for the treatment of patients with MM who have received one to three prior therapies
FDA-approved indication
• Standard: with Revlimid and dex
• Under investigation: with Revlimid and Velcade in newly diagnosed patients; with Pomalyst and nivolumab or Pomalyst and Velcade in RR patients
What combinations are used?
• Relapsed or relapsed/refractory following at least one to three prior therapies
Who should take it?
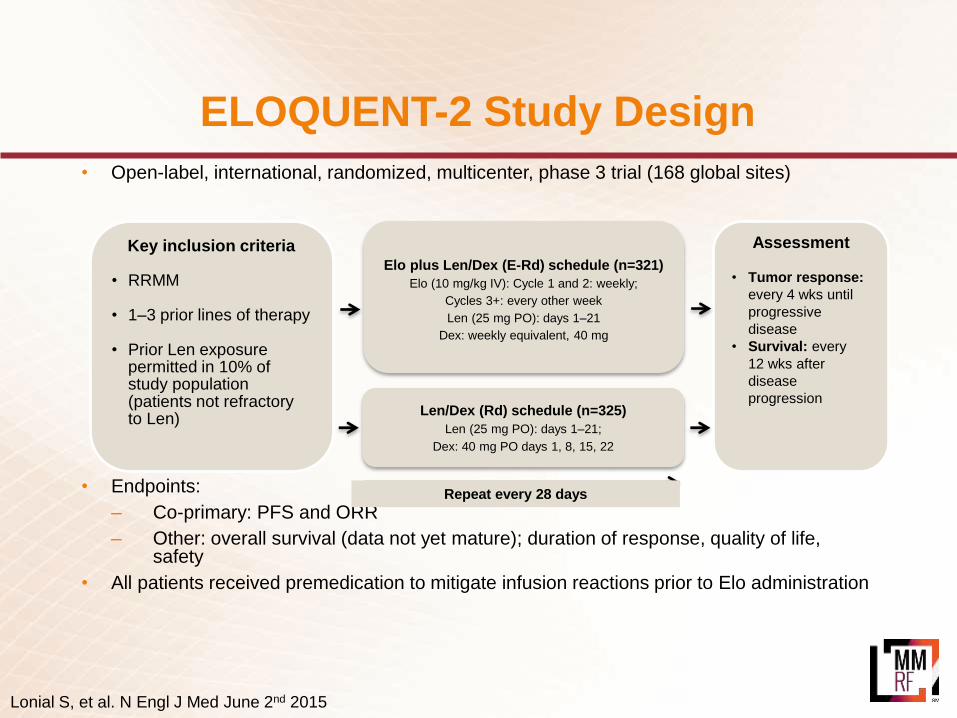
ELOQUENT-2 Study Design
• Open-label, international, randomized, multicenter, phase 3 trial (168 global sites)
• Endpoints:
– Co-primary: PFS and ORR
– Other: overall survival (data not yet mature); duration of response, quality of life, safety
• All patients received premedication to mitigate infusion reactions prior to Elo administration
Key inclusion criteria
• RRMM
• 1–3 prior lines of therapy
• Prior Len exposure permitted in 10% of study population (patients not refractory to Len)
Elo plus Len/Dex (E-Rd) schedule (n=321)
Elo (10 mg/kg IV): Cycle 1 and 2: weekly;
Cycles 3+: every other week
Len (25 mg PO): days 1–21
Dex: weekly equivalent, 40 mg
Len/Dex (Rd) schedule (n=325)
Len (25 mg PO): days 1–21;
Dex: 40 mg PO days 1, 8, 15, 22
Repeat every 28 days
Assessment
• Tumor response:
every 4 wks until
progressive
disease
• Survival: every
12 wks after
disease
progression
Lonial S, et al. N Engl J Med June 2nd 2015
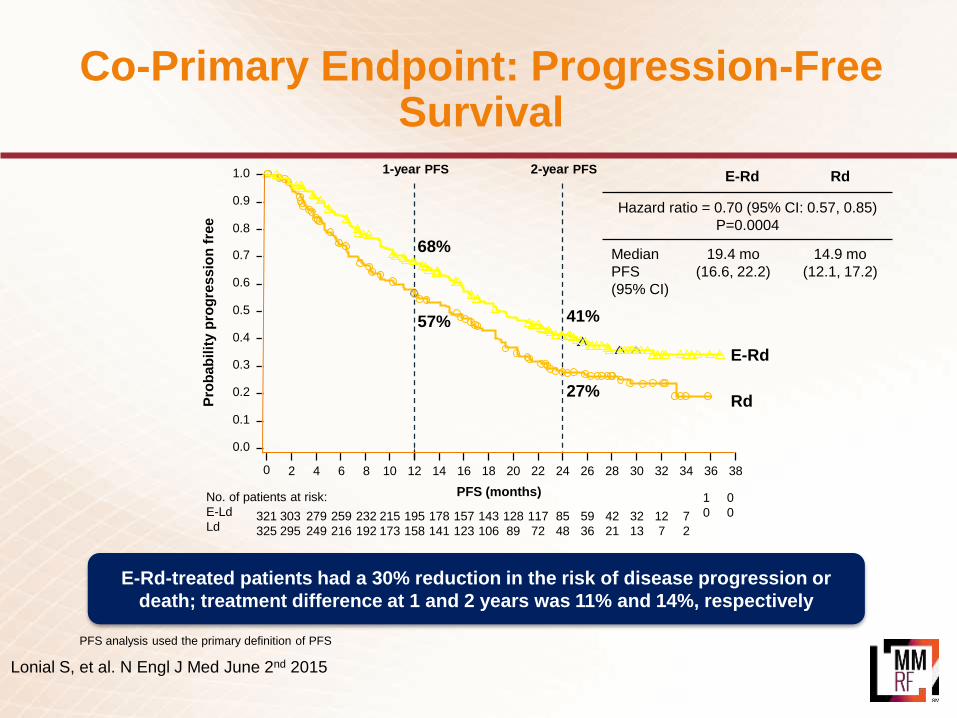
Co-Primary Endpoint: Progression-Free Survival
PFS analysis used the primary definition of PFS
E-Rd-treated patients had a 30% reduction in the risk of disease progression or
death; treatment difference at 1 and 2 years was 11% and 14%, respectively
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
380 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36
No. of patients at risk:
E-Ld
Ld321
325
303
295
279
249
259
216
232
192
215
173
195
158
178
141
157
123
143
106
128
89
117
72
85
48
59
36
42
21
32
13
12
7
7
2
57%
68%
27%
41%
1-year PFS 2-year PFS
PFS (months)
Pro
bab
ilit
y p
rog
ressio
n f
ree
E-Rd
Rd
0
0
1
0
E-Rd Rd
Hazard ratio = 0.70 (95% CI: 0.57, 0.85)
P=0.0004
Median
PFS
(95% CI)
19.4 mo
(16.6, 22.2)
14.9 mo
(12.1, 17.2)
Lonial S, et al. N Engl J Med June 2nd 2015

E-Ld Ld
HR 0.73 (95% CI 0.60, 0.89); p=0.0014
Median PFS
(95% CI)
19.4 mos
(16.6, 22.2)
14.9 mos
(12.1, 17.2)
PFS benefit with E-Ld was maintained over time (vs Ld):
• Overall 27% reduction in the risk of disease progression or death
• Relative improvement in PFS of 44% at 3 years
0.0
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
480 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45
No. of patients at risk:
E-Ld
Ld
321
325
293
266
259
215
227
181
171
130
144
106
125
80
107
67
94
60
85
51
59
36
34
15
19
7
8
3
PFS (months)
Pro
bab
ilit
y p
rog
res
sio
n f
ree
3
0
195
157
E-LdLd0.1
1-year PFS 2-year PFS 3-year PFS
0
0
68%
41%
26%
57%
27%
18%
ELOQUENT-2
Dimopoulos M, ASH 2015 Abst 28
Extended Progression-Free Survival
Monoclonal Antibody:Empliciti (elotuzumab)
• Common side effects include:
− Fatigue
− Diarrhea
− Pyrexia
− Constipation
− Cough
− Peripheral neuropathy
− Nasopharyngitis
− Upper respiratory tract infection
− Decreased appetite
− Pneumonia
What are the possible side effects?
• IV
• Every week for the first 2 cycles and every 2 weeks thereafter
How is Empliciti administered?

Options at Second Relapse and Beyond
IMiD: Pomalyst (pomalidomide)
*Overall response rate = complete response (CR) + very good partial response (VGPR) + partial response (PR) + minimal response (MR)
• Patients who received two or more prior therapies, including Velcade and an IMiD
− 29% overall response rate*
− On average, responses lasted 7.4 months
How effective is it?
• For MM patients who have received at least two prior therapies including Revlimid and Velcade and have demonstrated disease progression on or within 60 days of completion of the last therapy
FDA-approved indication
• Standard: Pomalyst + dex
• Under investigation: combinations with Vel-dex, Kyprolis-dex; experimental drugs (for example, SAR650984, Filanesib, Ixazomib)
What combinations are used?
• Received two or more prior therapies, including Velcade and Revlimid
• High-risk myeloma with DNA alterations, including t(4;14); preliminary data indicates effectiveness in 17p13del
• Safe for patients with reduced kidney function
• Patients of all ages
Who should take it?

Pomalidomide + Low-Dose Dex in RRMM
• Pomalidomide + low-dose dexamethasone FDA approved in 2013 for treatment after ≥ 2 previous therapies (including lenalidomide and bortezomib) and progression during or within 60 days of treatment
– Approval based on phase II MM-002 study (N = 221) [1]: ORR of 33% with Pom + LoDexvs 18% with Pom[2]
– DoR of 8.3 mos with Pom + LoDex; 10.7 mos with Pom[2]
– Low rates of discontinuations due to AEs[2]
PFS[2]
Median PFS, Mos
4.2
2.7
Jagannath S, et al. ASH 2012. Abstract 450.
Richardson PG, et al. Blood. 2014;123:1826-1832.
Pom + LoDex
Pom
100
80
60
40
20
0
Pati
en
ts (
%)
0 2010 30
PFS (Mos)
HR: 0.68
P = .003
0.2
0.4
0.6
0.8
1.0
0.00.0
0.2
0.4
0.6
0.8
1.0
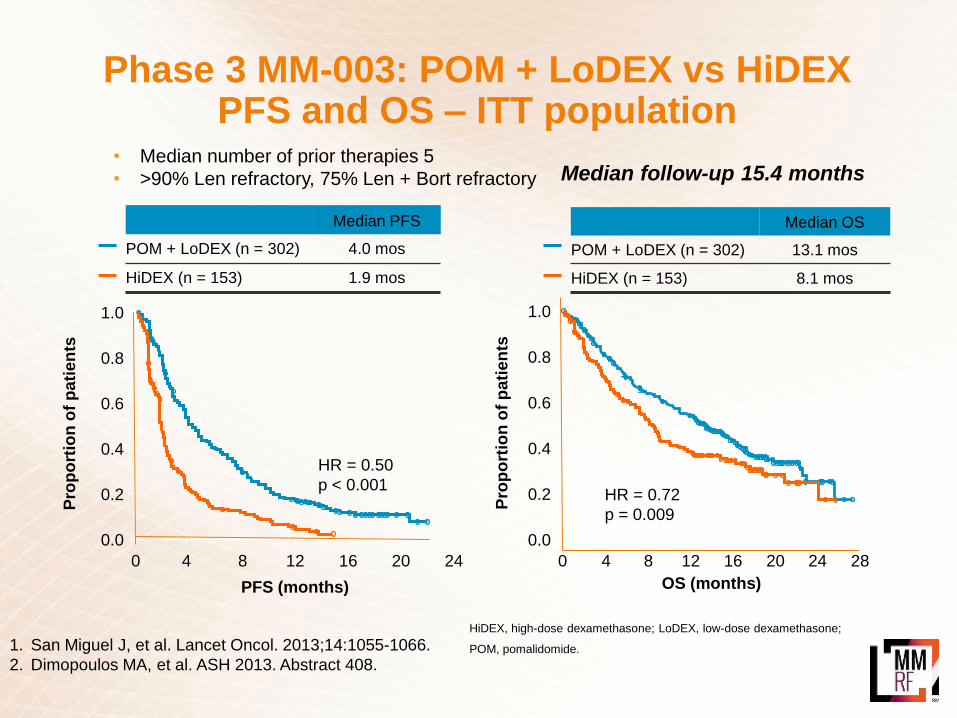
Phase 3 MM-003: POM + LoDEX vs HiDEXPFS and OS – ITT population
HiDEX, high-dose dexamethasone; LoDEX, low-dose dexamethasone;
POM, pomalidomide.
PFS (months)
Median PFS
POM + LoDEX (n = 302) 4.0 mos
HiDEX (n = 153) 1.9 mos
HR = 0.50
p < 0.001
4 8 12 16 20 240
Pro
po
rtio
n o
f p
ati
en
ts
OS (months)
Pro
po
rtio
n o
f p
ati
en
tsHR = 0.72
p = 0.009
4 8 12 16 20 24 280
Median OS
POM + LoDEX (n = 302) 13.1 mos
HiDEX (n = 153) 8.1 mos
Median follow-up 15.4 months• Median number of prior therapies 5
• >90% Len refractory, 75% Len + Bort refractory
1. San Miguel J, et al. Lancet Oncol. 2013;14:1055-1066.
2. Dimopoulos MA, et al. ASH 2013. Abstract 408.
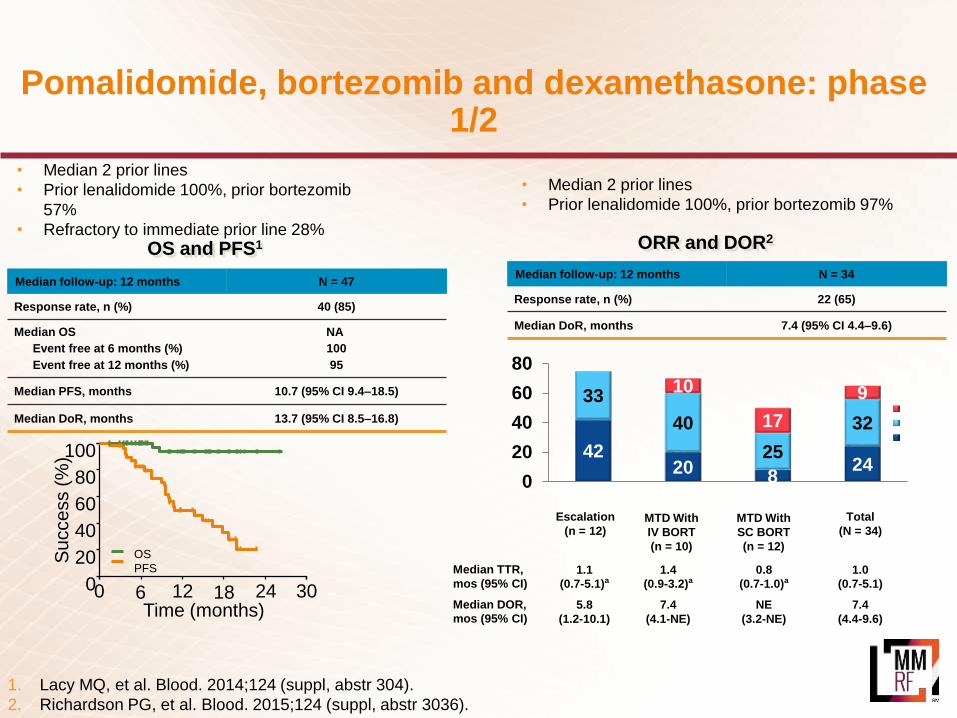
Pomalidomide, bortezomib and dexamethasone: phase 1/2
Time (months)
100
80
40
20
0
60
Success (
%)
0 12 24 306 18
OS
PFS
OS and PFS1
1. Lacy MQ, et al. Blood. 2014;124 (suppl, abstr 304).
2. Richardson PG, et al. Blood. 2015;124 (suppl, abstr 3036).
Median follow-up: 12 months N = 47
Response rate, n (%) 40 (85)
Median OS
Event free at 6 months (%)
Event free at 12 months (%)
NA
100
95
Median PFS, months 10.7 (95% CI 9.4–18.5)
Median DoR, months 13.7 (95% CI 8.5–16.8)
• Median 2 prior lines
• Prior lenalidomide 100%, prior bortezomib
57%
• Refractory to immediate prior line 28%
Median follow-up: 12 months N = 34
Response rate, n (%) 22 (65)
Median DoR, months 7.4 (95% CI 4.4–9.6)
• Median 2 prior lines
• Prior lenalidomide 100%, prior bortezomib 97%
4220
824
33
40
25
32
10
17
9
0
20
40
60
80
sCR/CRVGPRPR
Escalation
(n = 12)MTD With
IV BORT
(n = 10)
Total
(N = 34)MTD With
SC BORT
(n = 12)
Median TTR,
mos (95% CI)
Median DOR,
mos (95% CI)
1.1
(0.7-5.1)a
5.8
(1.2-10.1)
1.4
(0.9-3.2)a
7.4
(4.1-NE)
0.8
(0.7-1.0)a
NE
(3.2-NE)
1.0
(0.7-5.1)
7.4
(4.4-9.6)
ORR and DOR2

Phase 1/2, pomalidomide, cyclophosphamide and dexamethasone: PFS
Median PFS: 9.5 vs 4.4 months (p = 0.1078)
Median OSa: not reached vs 16.8 months (p = 0.1308)
• Median number of prior therapies 4
• Must have been refractory to lenalidomide
• Refractory to bortezomib 71%
Pro
po
rtio
n
Progression-free survival (months)
1.0
0.8
0.6
0.4
0.2
0.0
Arm N Event Censored Median (95% CI)
POM-LoDEX 36 30 (83%) 6 (17%) 4.4 (2.3, 6.0)
POM-LoDEX + cyclo 34 26 (76%) 8 (24%) 9.5 (4.6, 13.6)
0 3 6 9 12 15 18 21 24 27
POM-LoDEX
POM-LoDEX + cyclo
Log-rank p =
0.1078
Baz R, et al. Blood. 2016.

IMiD: Pomalyst (pomalidomide)
*Reduced risk when taken with blood thinners
• Common side effects include:
− Fatigue and weakness
− Low white blood cell counts
− Anemia
− Gastrointestinal effects (constipation, nausea, or diarrhea)
− Shortness of breath
− Upper respiratory infection
− Back pain
− Fever
− Blood clots*
What are the possible side effects?
• Capsule taken once daily for 21 days out of a 28-day cycle (3 weeks on, 1 week off)
• Blood thinners (for example, aspirin or low-molecule-weight heparin) are given along with Pomalyst to reduce the risk of blood clots
How is Pomalyst administered?
Histone Deacetylase Inhibitor:Farydak (panobinostat)
• 61% overall response rate (PR or better)How effective is it?
• In combination with Velcade and dex, treatment of MM patients who have received at least two prior regimens including Velcade and an IMiD (for example, Thalomid, Revlimid)
FDA-approved indication
• Standard: with Velcade and dex
• Under investigation: with Kyprolis and experimental drugs (for example, ixazomib)
What combinations are used?
• Relapsed or relapsed/refractory following at least two prior regimens including Velcade and an IMiD
Who should take it?
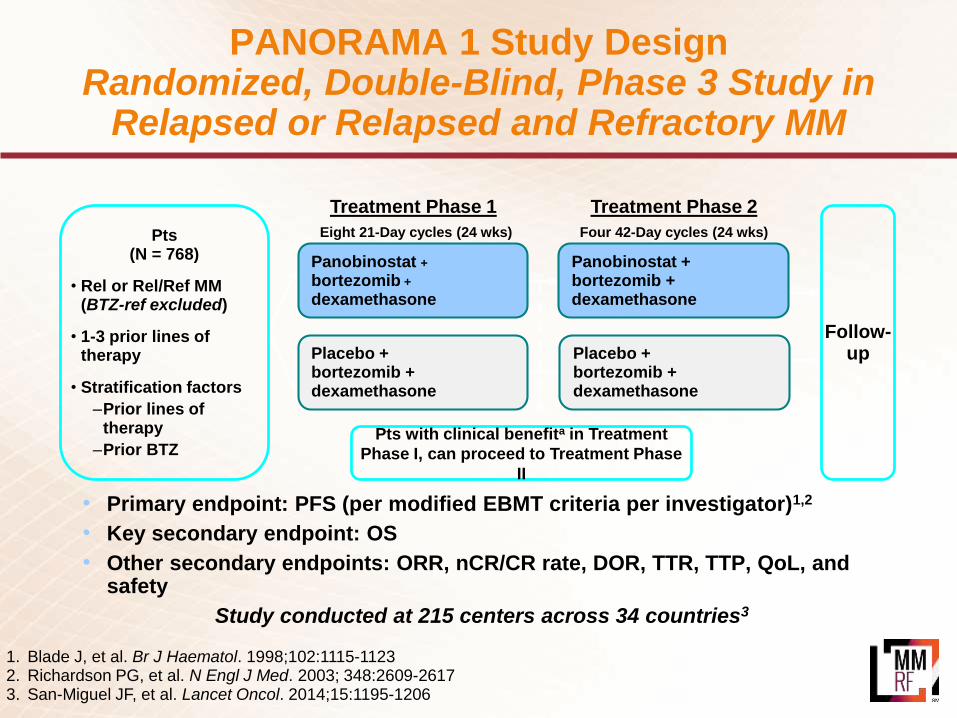
Follow-up
Treatment Phase 1 Treatment Phase 2
Eight 21-Day cycles (24 wks) Four 42-Day cycles (24 wks)
Panobinostat +
bortezomib +
dexamethasone
Placebo + bortezomib + dexamethasone
Panobinostat + bortezomib + dexamethasone
Placebo + bortezomib + dexamethasone
Pts with clinical benefita in Treatment
Phase I, can proceed to Treatment Phase
II
• Primary endpoint: PFS (per modified EBMT criteria per investigator)1,2
• Key secondary endpoint: OS
• Other secondary endpoints: ORR, nCR/CR rate, DOR, TTR, TTP, QoL, and safety
Study conducted at 215 centers across 34 countries3
Pts(N = 768)
• Rel or Rel/Ref MM (BTZ-ref excluded)
• 1-3 prior lines of therapy
• Stratification factors
–Prior lines of therapy
–Prior BTZ
1. Blade J, et al. Br J Haematol. 1998;102:1115-11232. Richardson PG, et al. N Engl J Med. 2003; 348:2609-26173. San-Miguel JF, et al. Lancet Oncol. 2014;15:1195-1206
PANORAMA 1 Study Design Randomized, Double-Blind, Phase 3 Study in
Relapsed or Relapsed and Refractory MM

PANORAMA Trial: Pan-Bor-Dex in Relapsed MM
Panobinostat 20 mg orally d 1,3,5,8,12 in 21-day cycles
Bortezomib 1.3mg/m2
Dexamethasone 20 mg
PFS OS
Median OS
Pan-Bor-Dex 33.64 mos
Pbo-Bor-Dex 30.39 mos
PAN-Bor-Dex
Pbo-Bor-Dex
HR 0.87
P =0.259
Months
San-Miguel JF, et al. Blood. 2014;124: Abstract 4742.
PAN-Bor-Dex
Pbo-Bor-Dex
80
60
40
20
0
0 4 8 12 16 20 2
4
28 32 36
HR 0.63
P
<0.0001
Months
Median PFS
Pan-Bor-Dex 12.0 mos
Pbo-Bor-Dex 8.1 mos
100
Histone Deacetylase Inhibitor:Farydak (panobinostat)
• Common side effects include:
− Diarrhea
− Peripheral neuropathy
− Asthenia/fatigue
− Nausea
− Peripheral edema
− Decreased appetite
− Vomiting
What are the possible side effects?
• Oral
• Taken once every other day for three doses per week of weeks 1 and 2 of a 4-week cycle (that is, on days 1, 3, 5, 8, and 12)
How is Farydak administered?
Monoclonal Antibody:Darzalex (daratumumab)
• 29% to 36% overall response rate (PR or better)How effective is it?
• Treatment of patients with MM who have received at least three prior lines of therapy including a proteasome inhibitor (PI) and an immunomodulatory agent or who are double-refractory to a PI and an immunomodulatory agent
FDA-approved indication
• Standard: as monotherapy
• Under investigation: with Revlimid or Velcade in newly diagnosed patients
What combinations are used?
• Relapsed or relapsed/refractory following at least three prior lines of therapy including a PI and an immunomodulatory agent or who are double-refractory to a PI and an immunomodulatory agent
Who should take it?

Daratumumab in monotherapy: Two studies: GEN501 & SIRIUS
• ≥18 years of age, ECOG status ≤21,2
• GEN5011
– Open-label, multicenter, phase 1/2, dose-escalation and dose-expansion study
– Relapsed from or refractory to ≥2 prior lines of therapy including PIs and IMiDs
• SIRIUS2
– Open-label, multicenter, phase 2 study
– Patients had received ≥3 prior lines of therapy, including a PI and an IMiD, or were double refractory to a PI and an IMID
• DARA was approved by the FDA on November 16, 2015, based on these studies
16 mg/kg(n = 16)
8 mg/kg(n = 18)
16 mg/kg(n = 106)
Response evaluated
Randomization
Additional 90 patientsenrolled at DARA 16 mg/kg
SIRIUS
Safety and response evaluated
Dose-escalation
Doses from 0.005-24 mg/kg
(n = 32)
Dose-expansion
GEN501
16 mg/kg(n = 42)
8 mg/kg(n = 30)
1. Usmani S, ASH 2015 Abst 29
2. Lokhorst HM, et al. N Engl J Med. 2015;373(13):1207-1219.
3. Lonial S, et al. Lancet. 2015. In press.
16 mg/kgN = 148

18%
10%
1%2%
0
5
10
15
20
25
30
35
16 mg/kgO
RR
, %
PR VGPR CR sCR
ORR = 31%
16 mg/kg (N = 148)
n (%) 95% CI
Overall response rate (sCR+CR+VGPR+PR)
46 (31) 23.7-39.2
Best responsesCRCRVGPRPRMRSDPDNE
3 (2)2 (1)
14 (10)27 (18)
9 (6)68 (46)18 (12)
7 (5)
0.4-5.80.2-4.8
5.3-15.412.4-25.42.8-11.2
37.7-54.37.4-18.51.9-9.5
VGPR or better (sCR+CR+VGPR) 19 (13) 7.9-19.3
CR or better (sCR+CR) 5 (3) 1.1-7.7
• ORR = 31%
• ORR was consistent in subgroups including age, number of prior lines of therapy, refractory status, or renal function
3%CR or better
13%VGPR or better
N = 148
Daratumumab in monotherapy: Two studies: GEN501 & SIRIUS – Efficacy in the combined analysis
Usmani S, ASH 2015 Abst 29

• For the combined analysis, median OS = 19.9 (95% CI, 15.1-NE) months
• 1-year overall survival rate = 69% (95% CI, 60.4-75.6)
Daratumumab in monotherapy: Two studies: GEN501 & SIRIUS – PFS and OS analysis
PD/NE: 3.7 (1.7-7.6) months
Responders: NE (7.4, NE)
MR/SD: 3.2 (2.8-3.7) months
PD/NE: 0.9 (0.9-1.0) months
0
Pat
ien
ts p
rogr
ess
ion
-fre
e an
d a
live
, %
2 6 8 12 14 18 20
Time from first dose, monthsPatients at risk
RespondersMR/SDPD/NE
0
25
50
75
100
4 10 16
RespondersMR/SDPD/NE
467725
46450
35130
2730
1310
500
300
000
41210
1420
300
0
Pat
ien
ts a
live
, %
2 6 8 12 14 18 22
Time from first dose, monthsPatients at risk
RespondersMR/SDPD/NE
0
25
50
75
100
4 10 16
MR/SD
467725
467416
456311
44577
42475
29374
310
000
466712
43537
15101
20
1351
Responders: NE (19.9, NE)
MR/SD: 17.5 (15.1-NE) months
PD/NE: 3.7 (1.7-7.6) months
Responders
PD/NE
Progression-free survival Overall Survival
Usmani S, ASH 2015 Abst 29

Monoclonal Antibody:Darzalex (daratumumab)
• Common side effects include:
− Infusion reactions
− Fatigue
− Nausea
− Back pain
− Pyrexia
− Cough
− Upper respiratory tract infection
What are the possible side effects?
• IV
• Weekly for weeks 1 to 8 then every 2 weeks for weeks 9 to 24 and then every four weeks for weeks 25 onwards
How is Darzalex administered?

MMY-1001 (Dara + Pom-Dex arm)
• ORR = 71%
• ORR in double-refractory patients = 67%
• Clinical benefit rate (ORR + minimal response) = 73%
DARA + POM-D
(N = 75)
n (%) 95% CI
Overall response rate
(sCR+CR+VGPR+PR)53 (71) 59.0-80.6
Best response
sCR
CR
VGPR
PR
MR
SD
PD
4 (5)
3 (4)
25 (33)
21 (28)
2 (3)
17 (23)
3 (4)
1.5-13.1
0.8-11.2
22.9-45.2
18.2-39.6
0.3-9.3
13.8-33.8
0.8-11.2
VGPR or better
(sCR+CR+VGPR)32 (43) 31.3-54.6
CR or better (sCR+CR) 7 (9) 3.8-18.3
ORR = 71%
43%
VGPR or
better
9%
CR or
better
28%
33%
4%
5%
0
10
20
30
40
50
60
70
80
16 mg/kg
OR
R, %
PR VGPR CR sCR
N = 75
Chari A, ASH 2015 Abst 508
ORR to Dara + Pom-Dex
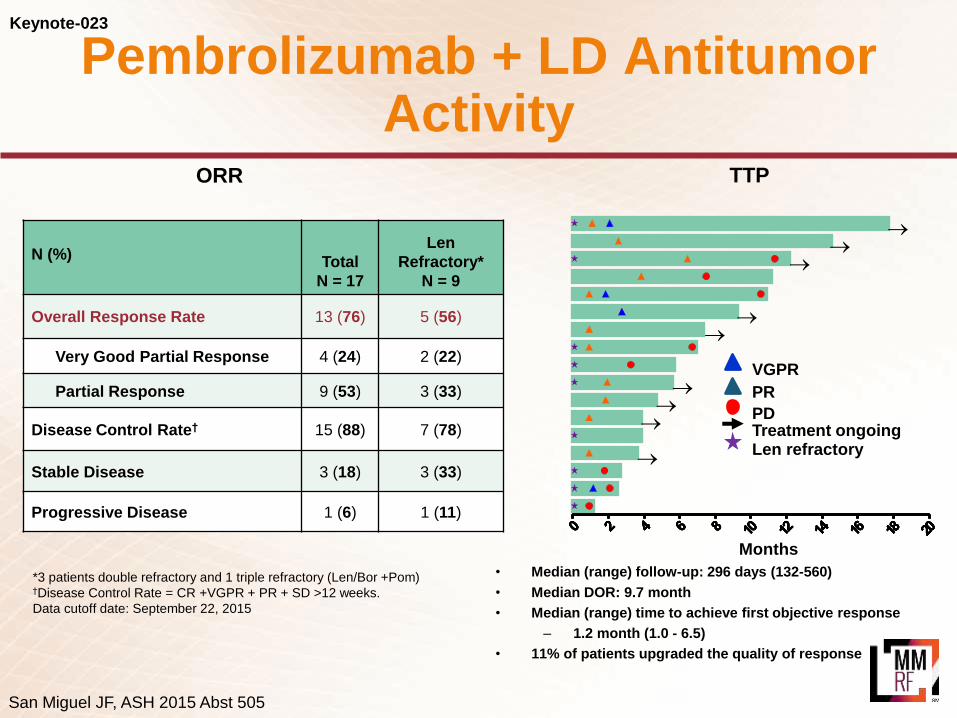
Keynote-023
N (%)Total
N = 17
Len
Refractory*
N = 9
Overall Response Rate 13 (76) 5 (56)
Very Good Partial Response 4 (24) 2 (22)
Partial Response 9 (53) 3 (33)
Disease Control Rate† 15 (88) 7 (78)
Stable Disease 3 (18) 3 (33)
Progressive Disease 1 (6) 1 (11)
*3 patients double refractory and 1 triple refractory (Len/Bor +Pom)†Disease Control Rate = CR +VGPR + PR + SD >12 weeks.
Data cutoff date: September 22, 2015
• Median (range) follow-up: 296 days (132-560)
• Median DOR: 9.7 month
• Median (range) time to achieve first objective response
– 1.2 month (1.0 - 6.5)
• 11% of patients upgraded the quality of response
VGPR
PR
PD
Len refractory
Treatment ongoing
Months
ORR TTP
San Miguel JF, ASH 2015 Abst 505
Pembrolizumab + LD Antitumor Activity
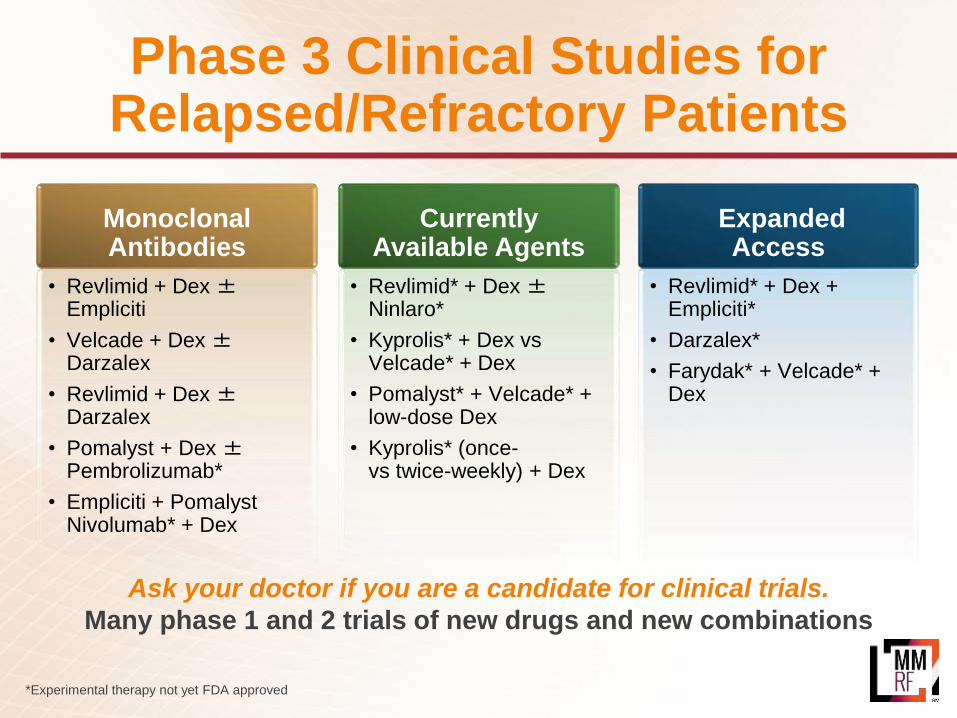
Phase 3 Clinical Studies for Relapsed/Refractory Patients
*Experimental therapy not yet FDA approved
Ask your doctor if you are a candidate for clinical trials.
Many phase 1 and 2 trials of new drugs and new combinations
• Revlimid + Dex±Empliciti
• Velcade + Dex±Darzalex
• Revlimid + Dex±Darzalex
• Pomalyst + Dex ±Pembrolizumab*
• Empliciti + PomalystNivolumab* + Dex
Monoclonal Antibodies
• Revlimid* + Dex ±Ninlaro*
• Kyprolis* + Dex vs Velcade* + Dex
• Pomalyst* + Velcade* + low-dose Dex
• Kyprolis* (once-vs twice-weekly) + Dex
CurrentlyAvailable Agents
• Revlimid* + Dex + Empliciti*
• Darzalex*
• Farydak* + Velcade* + Dex
ExpandedAccess
Conclusion: Example Patient Case
• A 64-yr-old woman comes with relapsed myeloma. Her history is as follows:
– Initial studies 3 years ago showed 55% plasma cells in the bone marrow, hyperdiploidy, IgGκ 3.5 g/dL, and multiple lytic lesions
– Initially treated with RVD, followed by high-dose melphalan and peripheral blood stem cell transplantation
– She achieved a CR and was on observation
– 3 yrs later, M-protein reappears to 1.5 g/dL
• All choices are optimal. Though she had multiple combination options available, she chose to go on combination daratumumab, lenalidomide and dexamethasone clinical trial and she remains in CR 20 months later. Other than IRR with 1st infusion, she tolerated regimen well currently has a great QOL.

NCCN guidelines 2016
NCCN guidelines V2.2016 and V3.2016

Summary: Relapsed/Refractory Myeloma
Relapsed/refractory multiple myeloma is treatable
Patients typically receive multiple lines of therapy
Treatment may sometimes be continued for an extended period of time
Six new drugs (Kyprolis, Pomalyst, Farydak, Darzalex, Empliciti, Ninlaro) introduced in last 4 years
With the introduction of each new drug, potential for additional combinations
Many promising new drugs/new combinations in clinical development—consider a clinical trial
![THE EMERGEN] PARADIGM: CHANGING PATTERNS OF …](https://cdn.vdocument.in/doc/165x107/623c64932f120923b20805b9/the-emergen-paradigm-changing-patterns-of-.jpg)






