Download - Marissa Conrad, MS, PT, NCS, CBIS
BPPV
September 27, 2018
Marissa Conrad, MS, PT, NCS, CBIS

1
Objectives
• Describe BPPV including risk factors, signs and symptoms
• Accurately assess the various forms of BPPV
• Differential Diagnosis
• Perform appropriate canalith repositioning maneuvers for the various
forms of BPPV

2
Benign Paroxysmal Positional Vertigo
Benign – it is not life-threatening
Paroxysmal – it comes in sudden, brief spells
Positional – it gets triggered by certain head positions or movements
Vertigo – a false sense of rotational movement

3
Benign Paroxysmal Positional Vertigo
• Benign paroxysmal positional vertigo (BPPV) is a peripheral
vestibular disorder that manifests as sudden, short-lived episodes of
vertigo elicited by specific head movements.
• BPPV is one of the most common causes of vertigo.
• It is often self-limited, but can become chronic and relapsing, with
considerable effects on a patient's quality of life.
• Results from the migration of free-floating calcium carbonate crystals
into one of the semicircular canals, rendering them sensitive to
gravity and causing a spinning sensation.

4
Epidemiology
One recent large epidemiological study estimates that as many as
35% of adults aged 40 years or older in the United States—
approximately 69 million Americans—have experienced some form
of vestibular dysfunction
Benign paroxysmal positional vertigo (BPPV) is the most common
cause of vestibular vertigo accounting for approximately 20–30% of
diagnoses in specialized dizziness clinics.

5
Cost of BPPV
• It is estimated that it costs approximately $2,000 to diagnose BPPV
and that greater than 65 percent with this condition will undergo
potentially unnecessary diagnostic testing or therapeutic
interventions.
• Healthcare costs associated with the diagnosis of BPPV alone
approach $2 billion per year
• In 86% of affected individuals, BPPV led to medical consultation,
interruption of daily activities or sick leave.
• In total, only 8% of affected participants received effective treatment.

6
BPPV Risk Factors
• Increasing age
• Female gender
• Head trauma
• Vestibular neuronitis
• Meniere’s Disease
• Post surgical

7
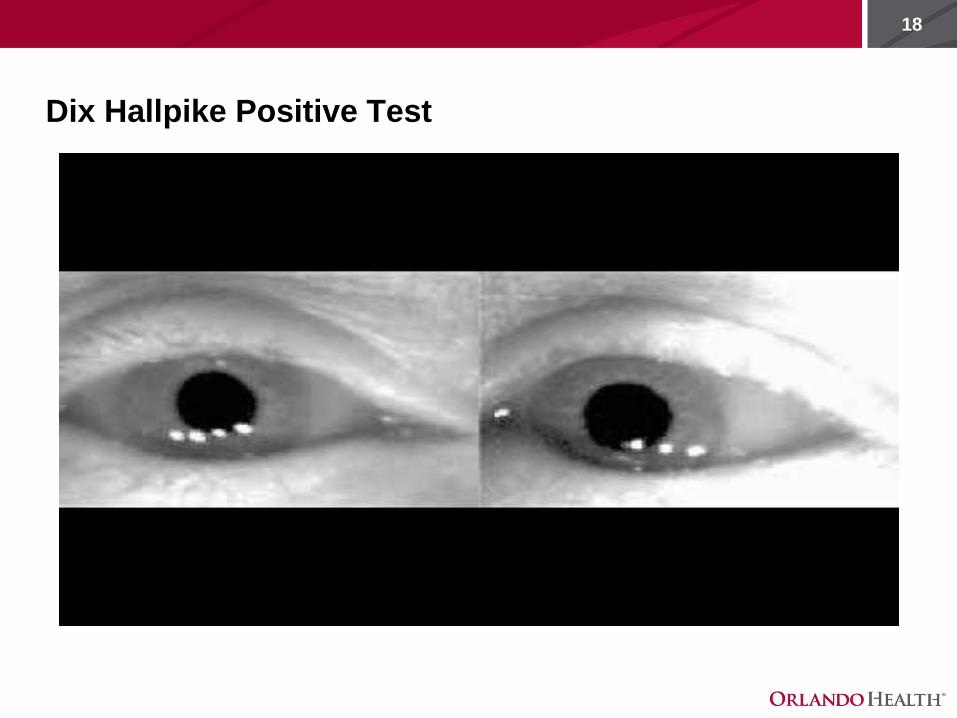
BPPV - Signs and Symptoms
• Symptoms
• Sudden onset, vertigo sensation (intense spinning)
• Lasts only seconds, usually at night or morning, when rolling
over in bed or getting out of bed
• Induced by head positional changes (rolling in bed, bending
over, looking up)
• May have balance disturbance
• Signs
• Visible nystagmus with Dix Hallpike, Sidelying Test or Roll Test
• Short duration (canalithiasis) or long duration (cupulolithiasis)
• Fatigability – response diminishes with repeated maneuvers
• May see a reversal of nystagmus upon sitting: normal response

8
BPPV treatment
• Symptoms remit with one treatment in approximately 85% of the
cases
• BPPV has been reported in adults of all ages
• Rare for children

9
BPPV Canalithiasis Mechanism
• Canalithiasis (most common)
• Dislodged otoconia in the semicircular canals
• Short duration: nystagmus less than 60 seconds
• A latency between 5-30 seconds
• The direction of the burst is about the axis of the canal
containing the debris
• A reversal of nystagmus on sitting
• Fatiguability
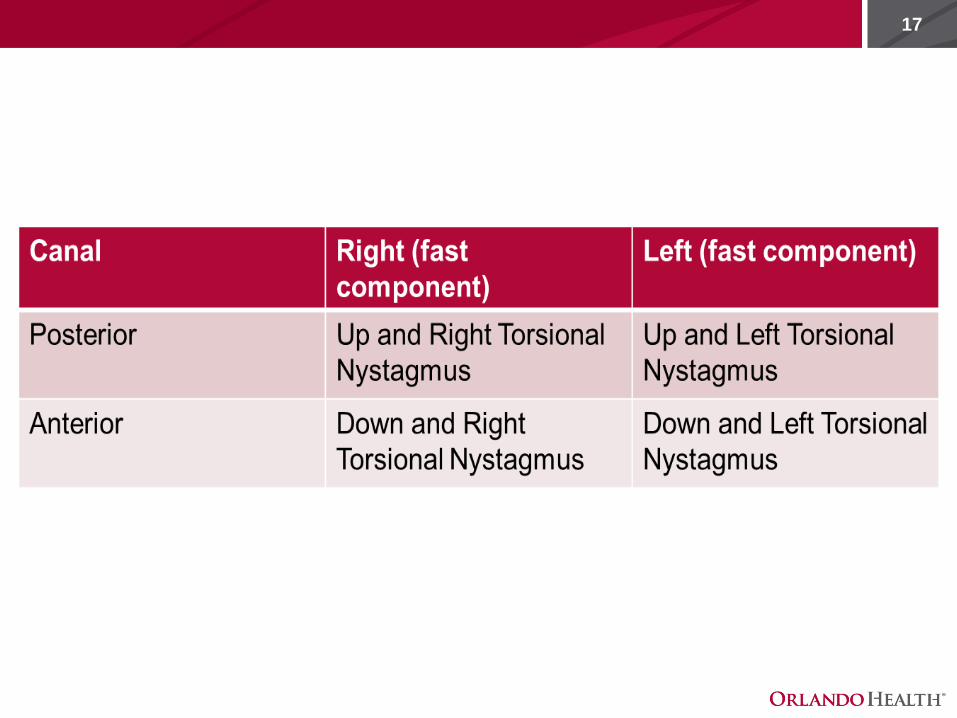
• In posterior canalithiasis, you will see upbeating and torsional
nystagmus
• In Horizontal/lateral Canalithiasis, you will see geotropic
nystagmus (toward the ground)

10
BPPV Cupulolithiasis Mechanism
• Otoconia are attached to the cupula, situated in the ampulla
• Prolonged duration of nystagmus > 60 seconds
• Symptoms tend to persist
• No latency
• Posterior canal -- upbeating and torsional in dix-hallpike position
• Anterior canal – downbeating and torsional when in Dix Hallpike
position
• Horizontal/Lateral canal -- nystagmus that beats to the opposite side
that is down ("ageotrophic").
• Up with the Cup
• Less common than canalithiasis

11
BPPV
• Canal involvement
• Posterior canal – 80-90%
• Horizontal canal – 10-20%
• Anterior canal – 3%
• Need to correctly identify direction of nystagmus to diagnose
involved canal and ensure appropriate treatment
• Direction of nystagmus – named for quick phase (upbeating and
torsional??)
• Monitor duration of nystagmus
12
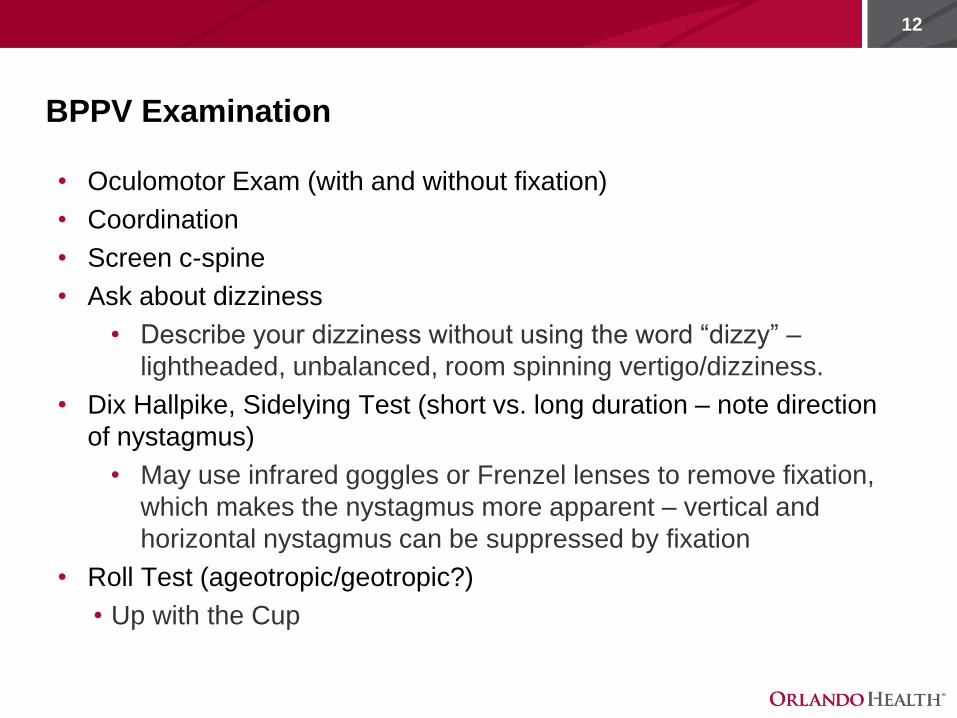
BPPV Examination
• Oculomotor Exam (with and without fixation)
• Coordination
• Screen c-spine
• Ask about dizziness
• Describe your dizziness without using the word “dizzy” –
lightheaded, unbalanced, room spinning vertigo/dizziness.
• Dix Hallpike, Sidelying Test (short vs. long duration – note direction
of nystagmus)
• May use infrared goggles or Frenzel lenses to remove fixation,
which makes the nystagmus more apparent – vertical and
horizontal nystagmus can be suppressed by fixation
• Roll Test (ageotropic/geotropic?)
• Up with the Cup

13
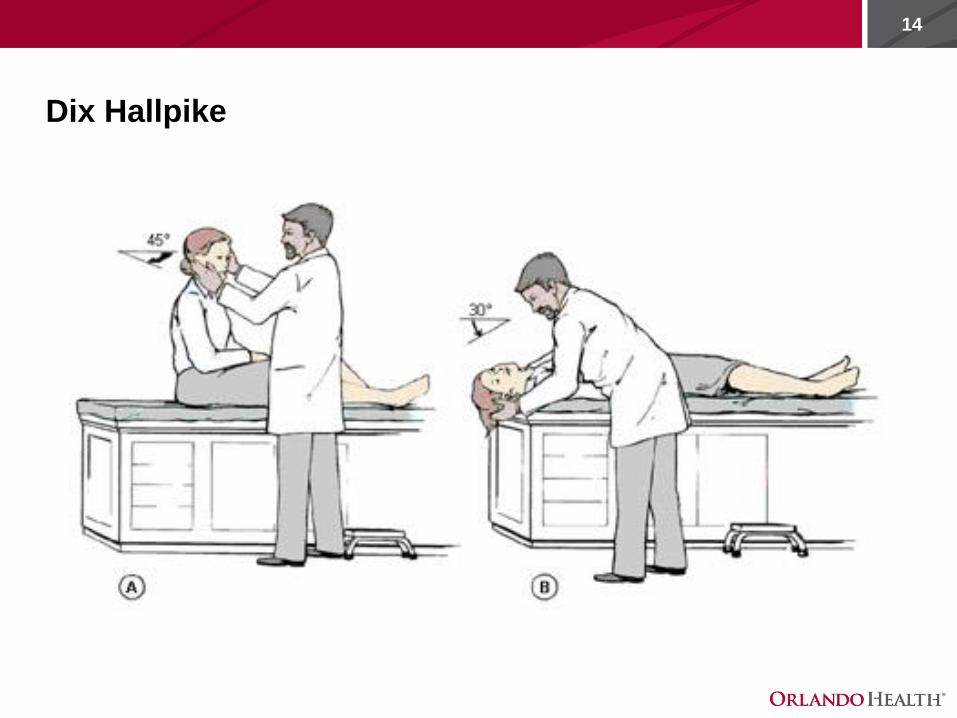
Dix Hallpike
• Explain beforehand
• Instruct the patient to keep eyes open
• Reassure the patient that the dizziness/vertigo will stop or
decrease shortly.
• Test the presumed unaffected side first to minimize nausea

15
Dix Hallpike

16
Test Series
1. Perform the Dix Hallpike test on the left side (suspected
asymptomatic side)
2. Perform the Dix Hallpike test on the right side
3. If the patient has no vertigo: before sitting the patient up for the right
side, perform a roll test by having them turn the head quickly to the
left.
4. After 60 seconds, have the patient quickly turn the head back to the
right
5. After 60 seconds, have the patient sit up.
17
18
Dix Hallpike Positive Test

19
20
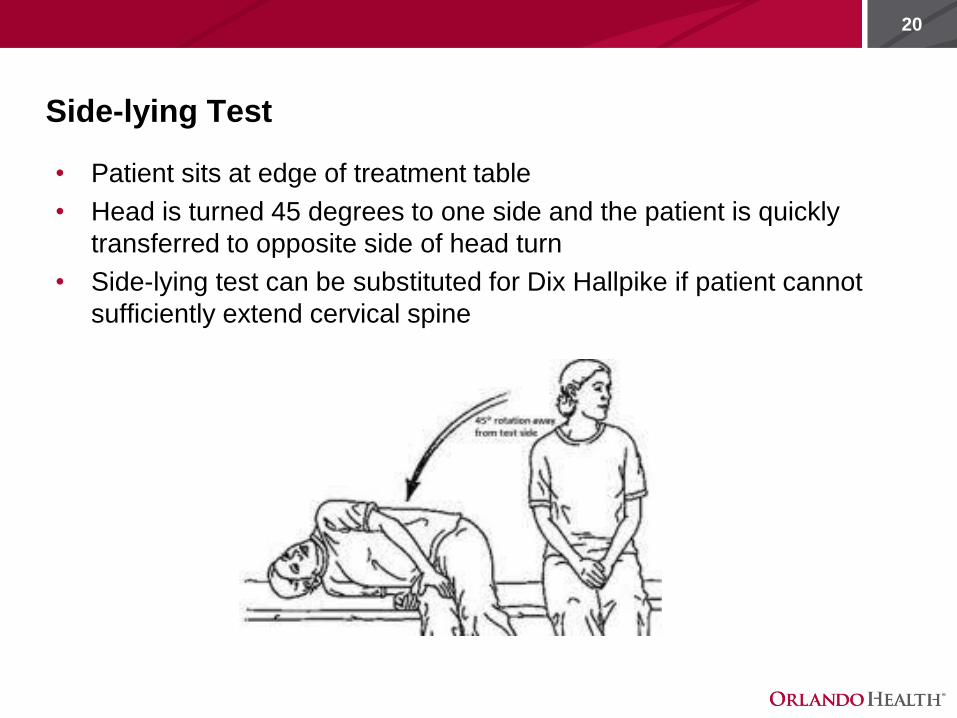
Side-lying Test
• Patient sits at edge of treatment table
• Head is turned 45 degrees to one side and the patient is quickly
transferred to opposite side of head turn
• Side-lying test can be substituted for Dix Hallpike if patient cannot
sufficiently extend cervical spine

21
Modifications
• If unable to achieve appropriate cervical extension:
• Testing: sidelying test
• Treatment: tilt table, wedge
• Don’t be afraid to ask for help/extra hands for larger people
22
(Supine or Head) Roll Test
Lateral (horizontal) Canal BPPV
• Patient is positioned supine with cervical spine flexion 30 degrees
and the head is then quickly turned to one side—held for 30‐60 sec
then return to start position. Then turn the head quickly to opposite
side for 30‐60 sec.
• Look for symptoms and horizontal nystagmus

23
Supine Roll Test

24

25
Peripheral vs. Central
Interpretation of Dix Hallpike/Sidelying/Horizontal Roll Tests
• Consider central problem if atypical:
• Non-rotatory nystagmus
• No latency
• Direction changing nystagmus
• No fatigability
• No habituation

26
TREATMENTS!
27
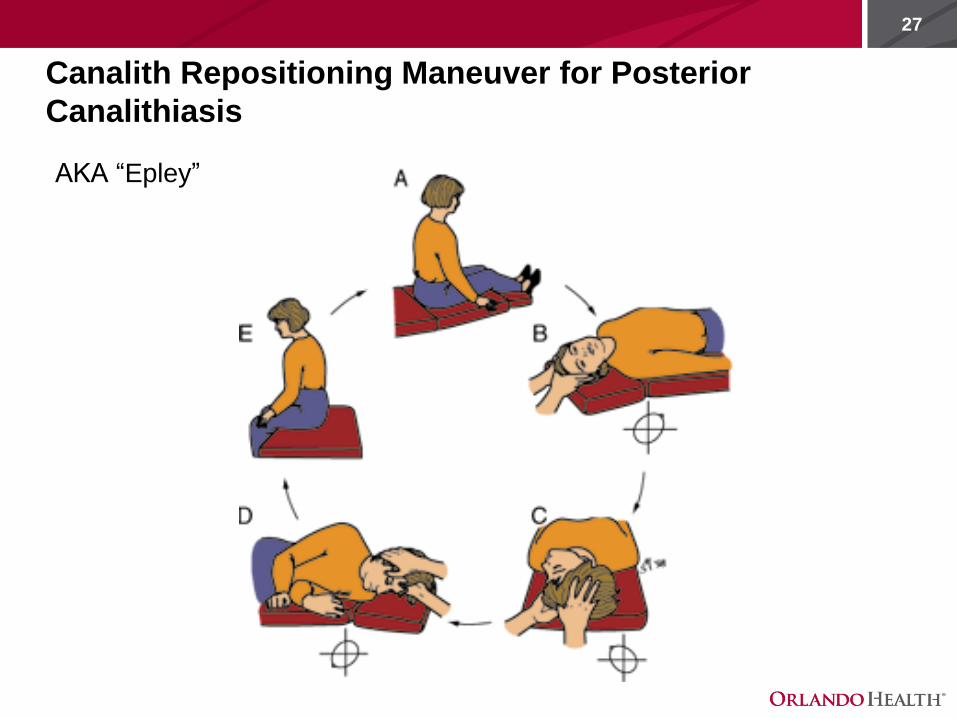
Canalith Repositioning Maneuver for Posterior
Canalithiasis
AKA “Epley”

28
Videos – CRM for Posterior canalithiasis

29

30
CRM for Posterior Cupulolithiasis
31
Lateral (Horizontal) Canal BPPV
Two types of BPPV involving the horizontal canal
• Geotropic nystagmus:
• Otoconia situated in the lateral canal (canalithiasis)
• More intense when the head is turned toward the affected ear
• Apogeotropic (Ageotropic) nystagmus:
• Otoconia attached to the cupula (cupulolithiasis)
• More intense when the head is turned toward the healthy ear.

32
CRM for Horizontal Canalithiasis/BBQ Roll Technique

33
CRM for Horizontal Canalithiasis
• AKA Gufoni
First described in 1998.
Geotropic nystagmus
• Patient quickly lies down on the side of the unaffected ear and
remains in this position until the evoked nystagmus subsides plus 60
seconds. The head is then quickly rotated 45 degrees toward the
floor and kept in this position for another 2 minutes, after which the
patient resumes an upright position

34
CRM for Horizontal Canalithiasis

35
Home Treatment Option
Forced, prolonged positioning maneuver for Horizontal Canalithiasis –
Vannuchi
• Start on the involved side (30-60 seconds) – roll to supine – roll
onto unaffected side, remain there for 12 hours.

36
CRM for Horizontal Cupulolithiasis
For ageotropic nystagmus
Casani – long duration nystagmus
• Lie patient down quickly onto affected side holding head in neutral.
Have patient rotate head quickly down (nose toward mat) and hold 2
minutes.

37
Ageotropic – long duration nystagmus

38
CRM Horizontal Cupulolithiasis (ageotropic) BPPV

39Canal Description of Maneuver
PC/AC Canalithiasis • Rotate head 45 degrees toward affected side.
• Rapidly lie supine with head hanging over edge of mat
• Hold for 30-60 seconds after symptoms subside
• Rotate head 90 degrees to opposite side, hold 30-60 seconds
• Roll on side, head facing the ground, tuck chin
• Return to sit, stay with the patient
PC Cupulolithiasis • Rotate Head 45 degrees toward unaffected side
• Rapidly move onto affected side (nose up to ceiling). Hold for 1 minute
• Rapidly move through starting position to opposite side holding head turned
toward unaffected side (nose down to mat/floor). Hold for 1 minute
• Slowly return to sitting position
AC Cupulolithiasis • Rotate Head 45 degrees towards affected side
• Rapidly move onto affected side (nose down to mat). Hold 1 minute
• Rapidly move through starting position to opposite side holding head turned
toward unaffected side (nose up to ceiling). Hold 1 minute
• Slowly return to sitting position
Horizontal Cupulolithiasis
(Positive side is considered
that which is least
symptomatic)
• For ageotropic of prolonged duration
• 1. Lie Patient down quickly onto affected side holding head in neutral
• 2. Quickly rotate head down 45 degrees
• 3. Hold for 2 minutes
Horizontal Canalithiasis
(Positive side is considered
that which is most
symptomatic/has more
nystagmus)
• For geotropic nystagmus of short duration – 3 options
• 1. BBQ Roll
• 2. Forced Prolonged Positioning: start sidelying on affected side. Roll to
unaffected side and remain there for 12 hours. If need to get up at night, repeat
maneuver and continue countdown
• 3. CRM for horizontal canalithiasis/Appiani: Lie patient down quickly onto
unaffected side holding head in neutral. Have patient rotate head quickly down
(nose toward mat) and hold 2 minutes.

40
Post Treatment
• Depending on symptoms, can repeat maneuver until nystagmus is
not observed (1-3 repetitions)
• Follow up: 2-7 days
• Reoccurrence: 30%

41
Summary and Conclusion
• BPPV is the mechanical displacement of otoconia from the utricle
into one of the SCCs
• Idiopathic or traumatic
• Occurs spontaneously in many patients but may follow head
trauma, labyrinthitis/neuritis, post surgery, Meniere's disease or
ischemia in the distribution of the anterior vestibular artery
• Disease of the peripheral vestibular system
• The most common cause of vertigo
• Very Treatable
• LAB to practice CRM
42
References
• Thomas Brandt, Doreen Huppert, Joachim Hecht, Cornelia Karch &
Michael Strupp (2006) Benign paroxysmal positioning vertigo: A long-
term follow-up (6–17 years) of 125 patients, Acta Oto-Laryngologica,
126:2, 160-163, DOI: 10.1080/00016480500280140
• Von Brevern M, Radtke A, Lezius F, et al. Epidemiology of benign
paroxysmal positional vertigo: a population based study. Journal of
Neurology, Neurosurgery, and Psychiatry. 2007;78(7):710-715.
doi:10.1136/jnnp.2006.100420.
• Herdman, S. J. Vestibular Rehabilitation 3rd edition. Philadelphia: F. A.
Davis Company; 2007.
• Lee S-H, Kim JS. Benign Paroxysmal Positional Vertigo. Journal of
Clinical Neurology (Seoul, Korea). 2010;6(2):51-63.
doi:10.3988/jcn.2010.6.2.51.
• M. Riga, A. Bibas, J. Xenellis, and S. Korres, “Inner Ear Disease and
Benign Paroxysmal Positional Vertigo: A Critical Review of Incidence,
Clinical Characteristics, and Management,” International Journal of
Otolaryngology, vol. 2011, Article ID 709469, 7 pages, 2011.
https://doi.org/10.1155/2011/709469.







