1
HIV Diagnostics:New Technologies and Strategies
Monica Parker, Ph.D.
Director, Bloodborne Viruses Laboratory
Wadsworth Center/NYSDOH
2
Objectives
• Review the principles of HIV diagnostic testing
• Describe technologies that aid in earlier and more accurate detection
• Present new testing strategies being proposed for HIV diagnostics

2
3
HIV
4
Virologic Markers of HIV Infection

3
5
Characteristics of HIV Infection
• Acute/Primary Infection– Ab to virus not detectable (window period)
– Viral RNA detectable by about day 10
– Viral Ag (p24) detectable 5-7 days after RNA
• Established Infection– Viral RNA levels decrease and level off
• May be undetectable, if antiretroviral treatment
– Ab detectable at 3 to 6 weeks post infection
– Ag (p24) may become undetectable due to immune complex formation
6
1989
• CDC released recommendations for a sequential, two-test algorithm for diagnosis of HIV-1 infection.
– Screen for antibodies to HIV using an enzyme immunoassay (EIA)
– If repeatedly reactive by EIA, conduct a more specific supplemental test
• Western blot (WB)
• Indirect immunofluorescence assay (IFA)
4
7
2010
• The CDC recommendation from 1989 is still the official stance
• Testing methods have moved forward
• More test options exist today
• Alternative strategies are under evaluation
Antibody Tests
The Standard for HIV Diagnostics

5
9
Antibody Screening Tests
• Enzyme Immunoassays (EIA, ELISA)
• Chemiluminescence Immunoassays (CIA)– Over time, sensitivity has increased
– Repeatedly reactive = reactive on at least two screening tests
– Supplemental testing is required to “confirm”infection
10
Enzyme Immunoassay (EIA)1st/2nd Generation
• Microwell plates coated with HIV antigens (Ag)
• Ag = Viral lysate, recombinant or peptide
• Serum/plasma -IgG + enzyme substrate color optical density (OD) reading
-IgG
IgG-HIV
HIV Ag

6
11
EIA: 3rd Generation
• Ag-Ab-Ag sandwich technique
• Multiple HIV Ag: HIV-1(envelope & core), HIV-2, group O
• Increased sensitivity, earlier detectionHIV Ab in
blood
IgG IgM
Ag-enzyme
+
HIV Ag on test surface
12
Random Access Platform
• Multiple analytes on the same instrument
• Reagents loaded and stored on board
• Controls run at the beginning of the day
• Load individual specimen tubes & get result in about 1 hr.
7
13
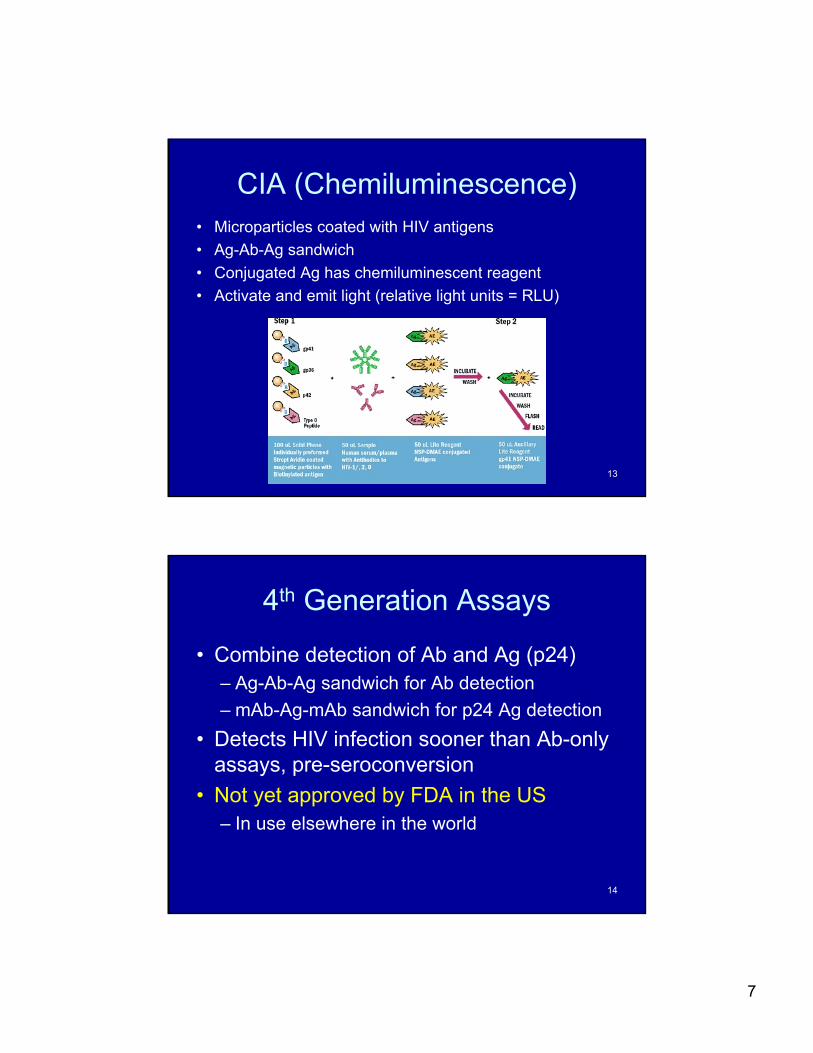
CIA (Chemiluminescence)• Microparticles coated with HIV antigens
• Ag-Ab-Ag sandwich
• Conjugated Ag has chemiluminescent reagent
• Activate and emit light (relative light units = RLU)
14
4th Generation Assays
• Combine detection of Ab and Ag (p24)– Ag-Ab-Ag sandwich for Ab detection
– mAb-Ag-mAb sandwich for p24 Ag detection
• Detects HIV infection sooner than Ab-only assays, pre-seroconversion
• Not yet approved by FDA in the US– In use elsewhere in the world
8
15
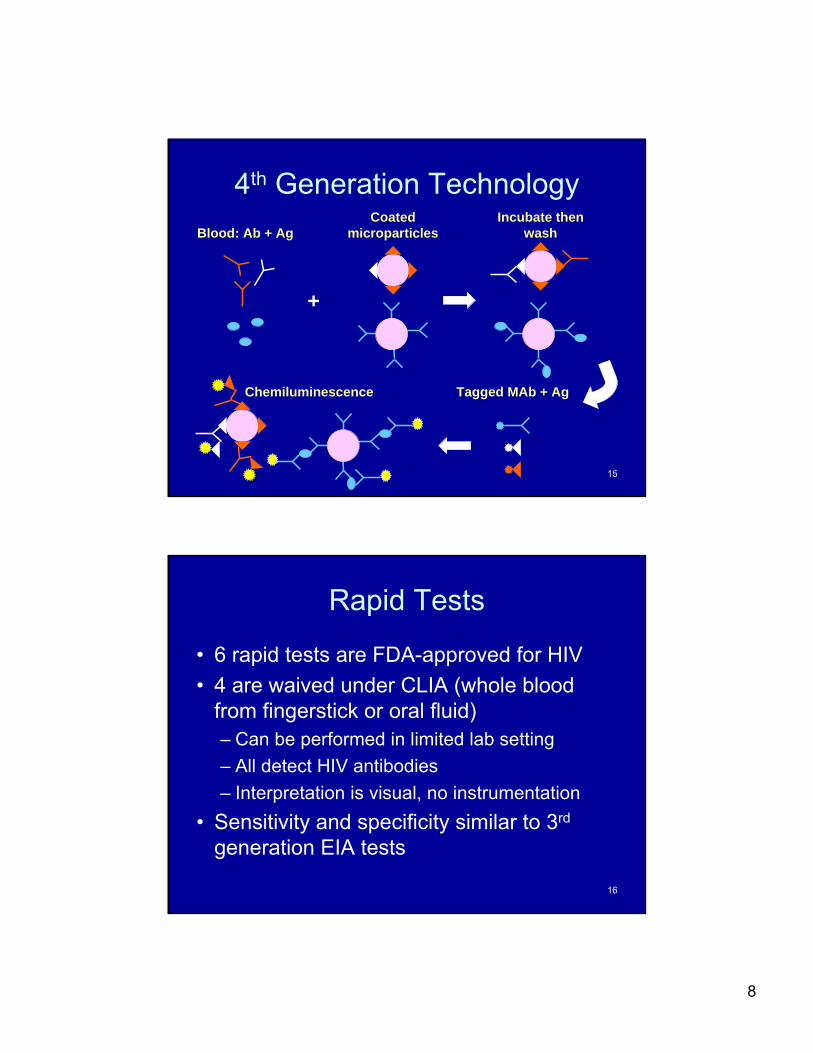
4th Generation Technology
Blood: Ab + Ag
+
Coated microparticles
Incubate then wash
Tagged MAb + AgChemiluminescence
16
Rapid Tests
• 6 rapid tests are FDA-approved for HIV
• 4 are waived under CLIA (whole blood from fingerstick or oral fluid)– Can be performed in limited lab setting
– All detect HIV antibodies
– Interpretation is visual, no instrumentation
• Sensitivity and specificity similar to 3rd
generation EIA tests

9
17
Uni-Gold Recombigen
Multispot HIV-1/HIV-2Reveal G3
OraQuick Advance Clearview Complete HIV 1/2
Clearview HIV 1/2 Stat Pak
HIV Rapid Tests
18
Uni-Gold Recombigen OraQuick Advance Clearview Complete HIV 1/2
Clearview HIV ½ Stat Pak
WAIVED(Low complexity)

10
19
Advantages/Disadvantages
• Clients get their results right away– When specimen was sent to lab, many clients
never returned for test results
– Post-test return rates: 70-85%
• Some clients get a preliminary positive result that turns out to be false positive
• Preliminary positive result requires supplemental testing to confirm
20
Supplemental Tests
• Supplemental tests are designed to be specific (confirmatory)
• Antibody screening tests have progressed and become more sensitive
• Supplemental tests for confirming HIV antibodies have changed little over the years
11
21
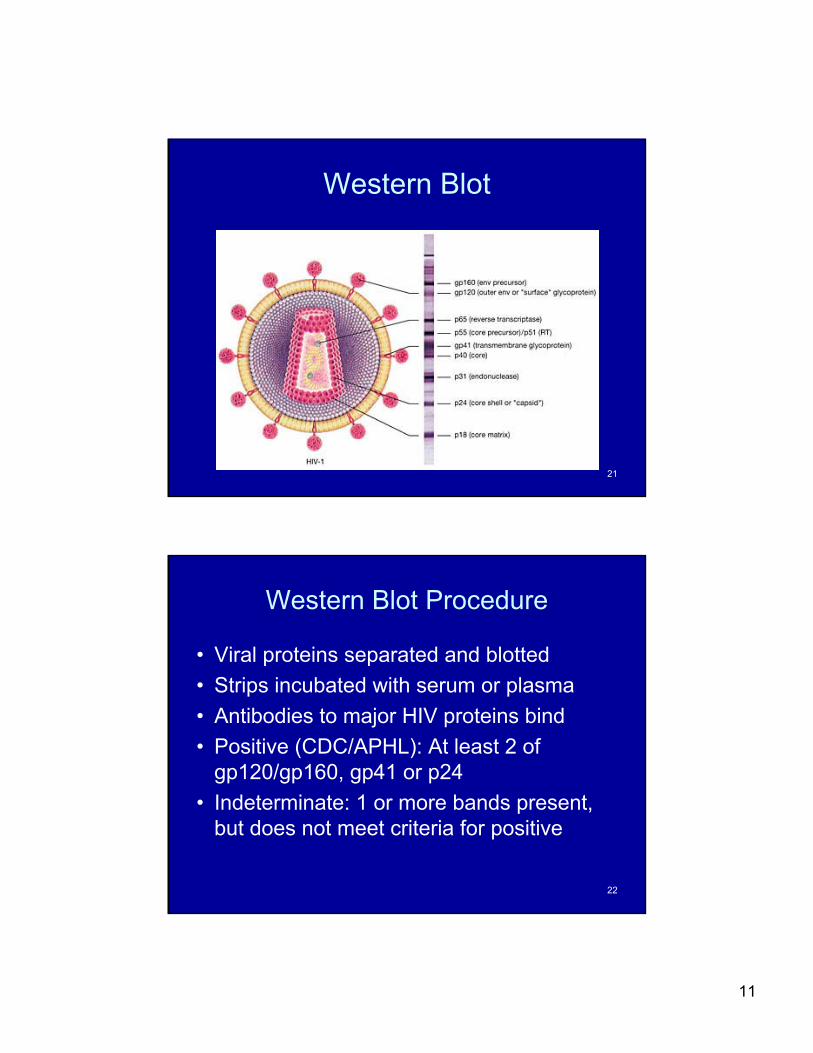
Western Blot
22
Western Blot Procedure
• Viral proteins separated and blotted
• Strips incubated with serum or plasma
• Antibodies to major HIV proteins bind
• Positive (CDC/APHL): At least 2 of gp120/gp160, gp41 or p24
• Indeterminate: 1 or more bands present, but does not meet criteria for positive

12
23
Interpretation is Subjective
24
Indeterminate Western Blot
• Reasons for indeterminate results:– Early infection– Late infection– HIV-2 infection– Other
• Some individuals may exhibit indeterminate results for long periods of time (years) and never seroconvert
• Most indeterminates show only weak reactions to the Gag proteins (mostly p17, p24 and/or p55)
13
25
HIV-2
• Lots of FDA-approved screening assays– Most are combo assays i.e. HIV-1/2
– Need to differentiate when reactive
• One FDA-approved HIV-2 ELISA test
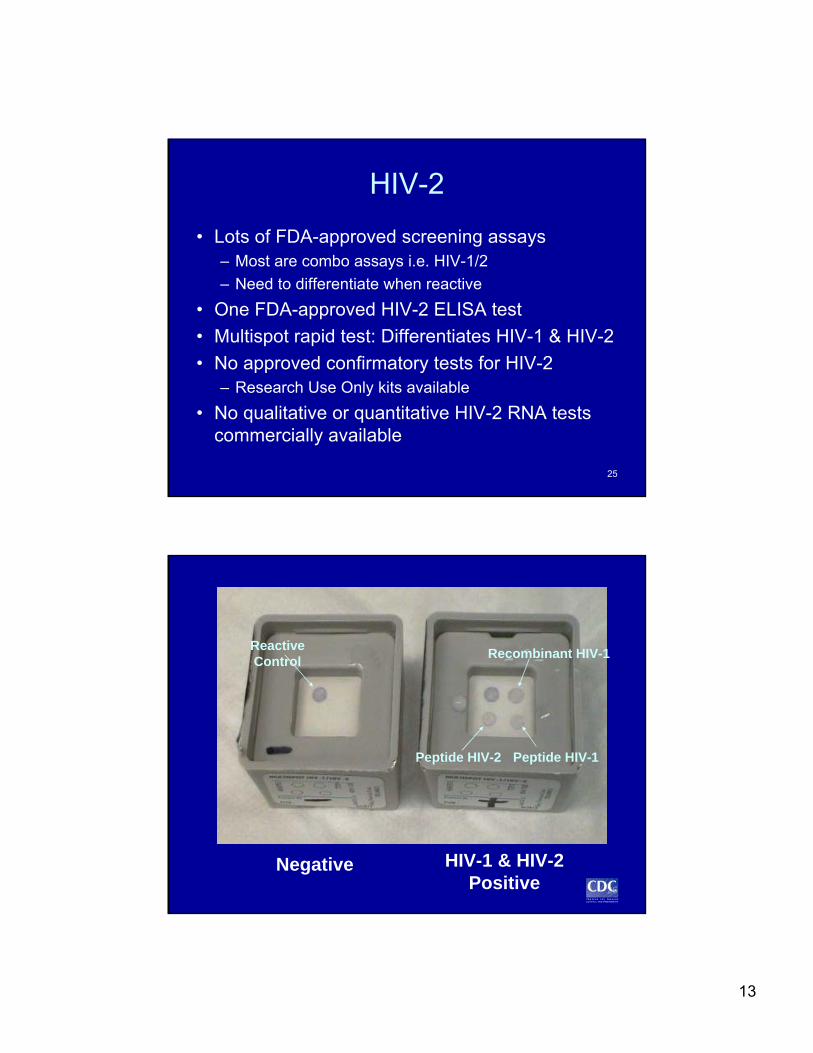
• Multispot rapid test: Differentiates HIV-1 & HIV-2
• No approved confirmatory tests for HIV-2– Research Use Only kits available
• No qualitative or quantitative HIV-2 RNA tests commercially available
26
Negative HIV-1 & HIV-2 Positive
Peptide HIV-2
Recombinant HIV-1
Peptide HIV-1
Reactive Control
14
27
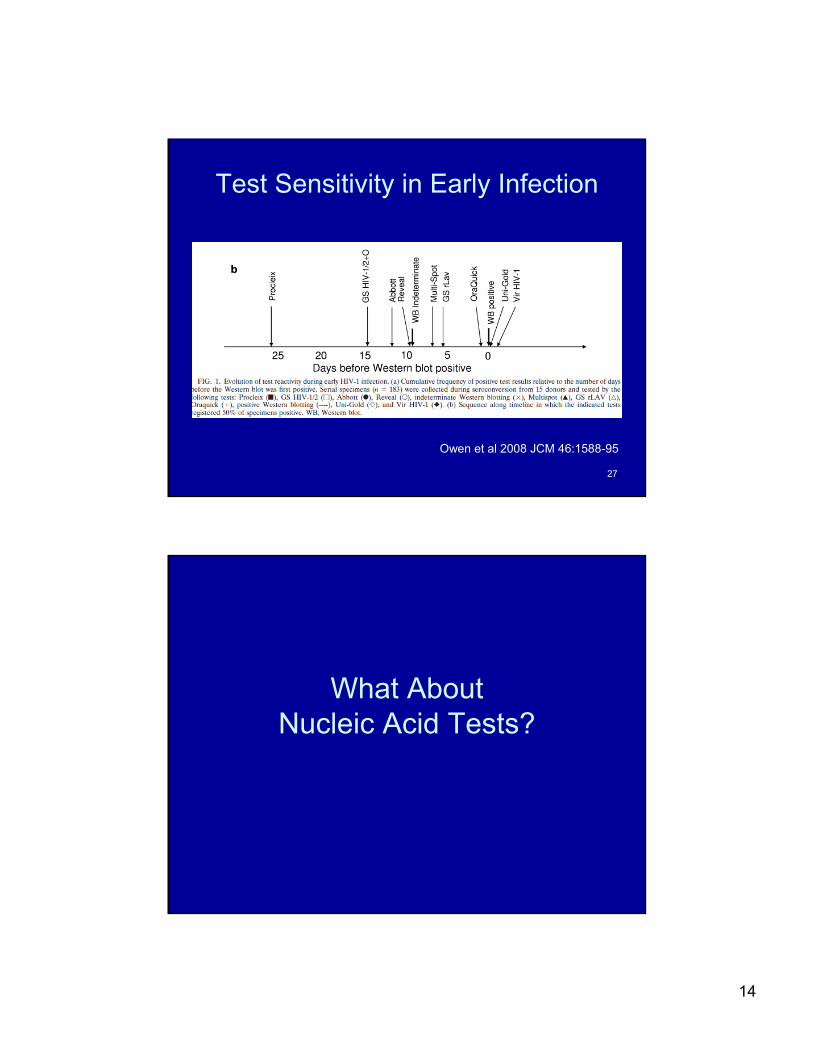
Test Sensitivity in Early Infection
Owen et al 2008 JCM 46:1588-95
What AboutNucleic Acid Tests?
15
29
HIV-1 RNA Testing
• Quantitative HIV-1 RNA tests (viral load)– Intended use (FDA): monitoring therapy, prognosis
– Alone, not intended for diagnosis
• Qualitative HIV-1 RNA test– Intended use ( One FDA approved):
– as an aid in the diagnosis of HIV-1 infection, including acute or primary infection
– to confirm HIV-1 infection in an individual whose specimen is repeatedly reactive for HIV-1 antibodies
30
Applications for RNA Testing
• Testing symptomatic or recently exposed individuals (AHI)
• Resolving discordant Ab test results:– EIA or rapid test reactive, WB neg or ind
• Screening pooled seronegative specimens (OFF-LABEL USE)
• Early infant diagnosis
16
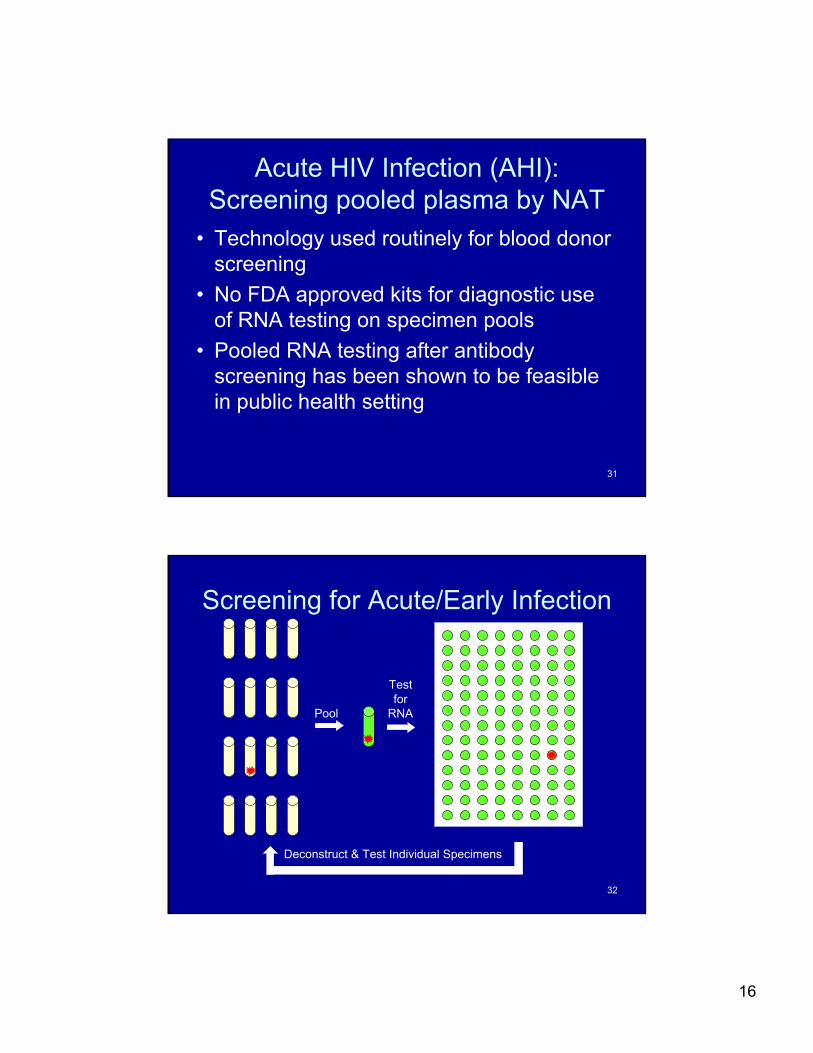
31
Acute HIV Infection (AHI):Screening pooled plasma by NAT
• Technology used routinely for blood donor screening
• No FDA approved kits for diagnostic use of RNA testing on specimen pools
• Pooled RNA testing after antibody screening has been shown to be feasible in public health setting
32
Pool
Testfor
RNA
Deconstruct & Test Individual Specimens
Screening for Acute/Early Infection
17
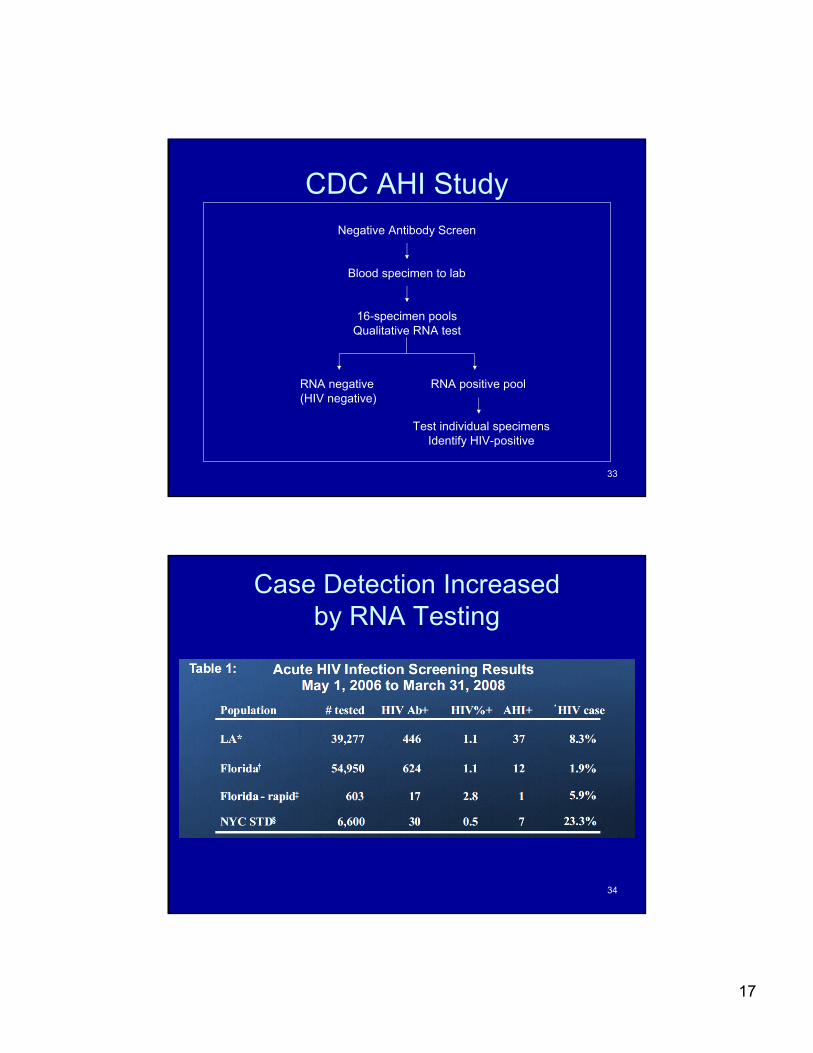
33
CDC AHI StudyNegative Antibody Screen
Blood specimen to lab
16-specimen poolsQualitative RNA test
RNA negative(HIV negative)
RNA positive pool
Test individual specimensIdentify HIV-positive
34
Case Detection Increasedby RNA Testing

18
35
Variable Yield with RNA Screening
• Parallel study was conducted with STD clinic in an upstate NY county
• 5722 HIV antibody-negative specimens screened by pooled RNA testing
• 1 EIA reactive/ WB indeterminate/RNA positive result
• No true AHIs detected
36
Recap on Testing Capabilities
• More FDA-approved tests available– Including several rapid tests
• Screening tests have increased sensitivity; Western blot has not
• Rapid tests get neg and prelim pos results to clients immediately; still need to confirm
• RNA tests may be used in the detection of acute/early infection

19
37
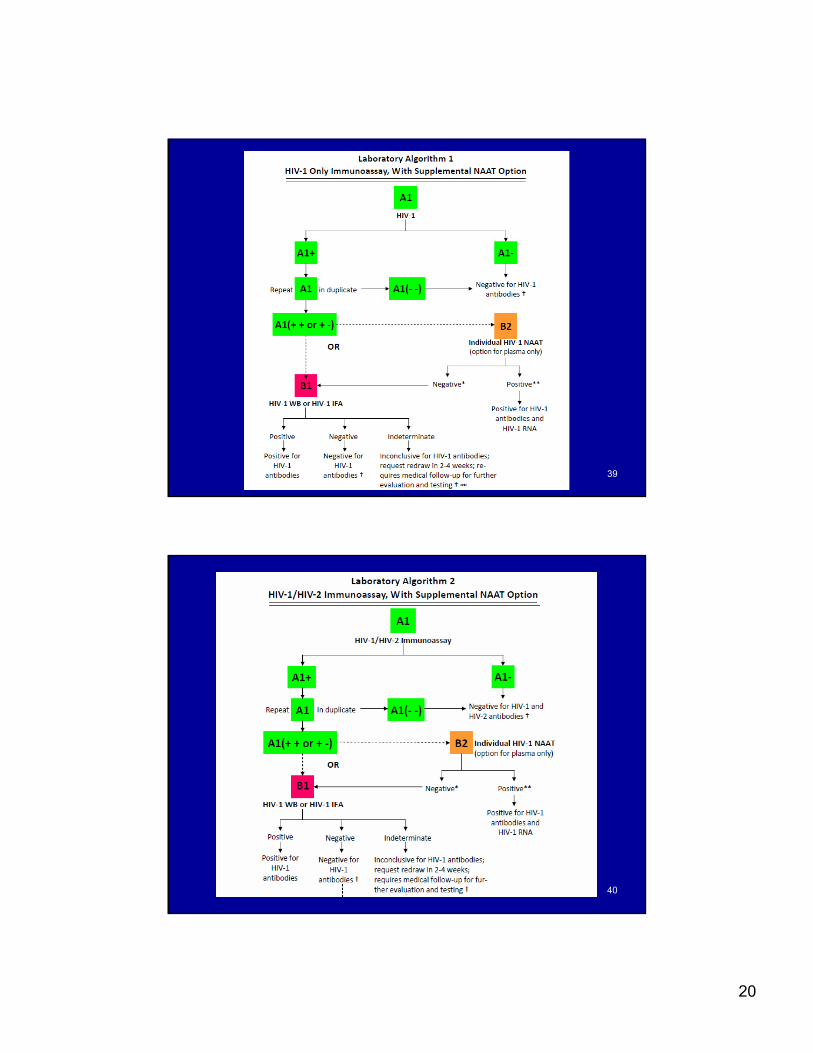
Updating the HIV Diagnostic Testing Strategies
• 2006: Two workgroups convened to develop proposals for the best combination of assays to determine HIV infection status in laboratory and point-of-contact (POC) settings
• Dec 2007:HIV Diagnostics Conference:– 5 laboratory testing strategies proposed
– 4 POC strategies proposed
Laboratory-based Testing Strategies
20
39
40

21
41
42
22
43
Status Report
• April 2009: HIV Testing Strategies, A Status Report released by CDC and APHL– http://www.aphl.org Infectious Diseases
• What are the false positive and false negative rates of these strategies?
• Are we ready to do away with the Western blot?
44
Moving Forward
• March 2010: HIV Diagnostics Conference– Progress was made towards developing a unified
laboratory algorithm– Consideration was given to early detection, accuracy
and cost– Proposed strategy:
• two different antibody screening tests• NAAT for discordant cases• No role for WB
• Implications for HIV case reporting and surveillance?

23
45
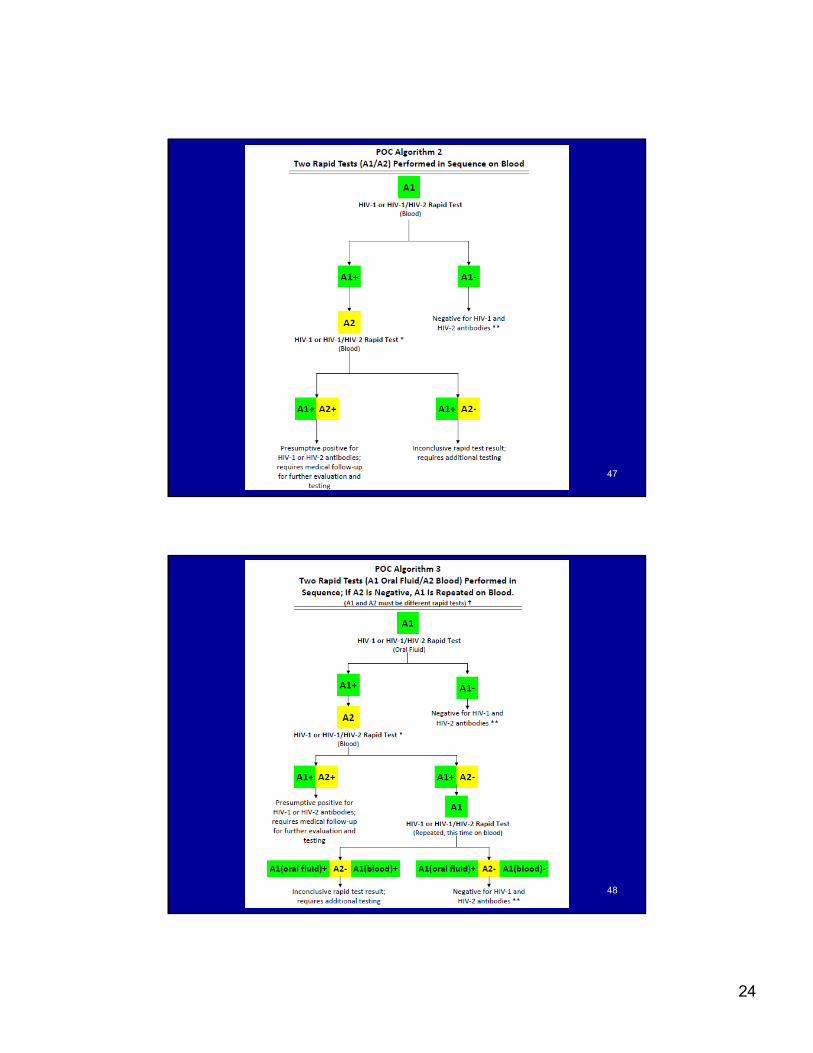
Point-of-Contact Strategies
• 2002: 1st HIV rapid test FDA approved for use at the POC
• CDC: Must confirm with WB or IFA– Intended use statements: “Suitable for use in multi-
test algorithms designed for statistical validation of rapid HIV tests”
• Multi-rapid test strategies are being evaluated
• Additional rapid test used to “verify” results of initial test, not “confirm” infection
46
24
47
48

25
49
50
Each Test is Different
•25 / box• 20 / box• 25 or 100 / box
• Finger stick only• Finger stick only• Oral or Finger stick sample
• Must be read by 20 minutes
• Must be read by 12 minutes
• Must be read by 40 minutes
•Test storage temp (46-86°F)
• Test storage temp (35-80°F)
• Test storage temp (35-80°F)
• 15 minutes• 10 minutes• 20 minutes
• HIV1 & HIV2• HIV1 Only• HIV1 & HIV2
ClearviewUni-GoldOraQuick

26
51
More Differences
• Clinic temperature to test (64 to 86°F)
• Clinic temperature to test (59 to 80.6°F)
• Clinic temperature to test (59 to 99°F)
• Controls good for 2 yrs (check expiration date)
• Controls good for 30 days after opening
• Controls good for 8 wks after opening
•Use test stand• Lay flat on table• Use blue stand
• If result invalid, retest with 1 device
• If result invalid, retest with 2 devices
• If result invalid, retest with 1 device
• Insert device into buffer vial
• Wash solution added to device
• Device added to developer solution
• Sampler tip collection• Pipette collection• Loop collection
ClearviewUni-GoldOraQuick
52
Questions
• Can multiple rapid tests be reliably performed in sequence at the POC?– Most data have been collected retrospectively
in a controlled lab setting
• What is the best sequence of rapid tests for multi-test algorithms?
• Collection of real-life data from rapid testing programs is underway
27
53
More Questions
• Rapid test → Preliminary positive → Refer to care– Many will go, some will not
• Lab confirmation = Lab reporting
• Will we see a decrease in case reports?
• Will active surveillance be needed
54
Summary
• The number and variety of HIV diagnostic tests have expanded greatly over time
• The capacity for early detection has improved
• New strategies are needed to fully take advantage of the testing options
• National recommendations are anticipated soon







