

Hughes Stovin SyndromeMorning Report
January 19th, 2010Jason Kidd

HemoptysisDefinition: Expectoration of blood from the
respiratory tractMassive hemoptysis: >100 ml/24 hoursEstimation of blood loss is unreliable
Harrison’s

Hemoptysis: DDxAirway Disease
Inflammatory: bronchitis, bronchiectasisNeoplasmsForeign bodyTraumaFistula formation

Hemoptysis: DDx contPulmonary parenchymal disease
Infection: PNA, TB, Aspergilloma, abscessAutoimmune: Goodpasture’s, hemosiderosis,
lupus, Wegener’sGenetic: Ehlers-DanlosCocaine inducedMedication induced: Bevacizumab

Hemoptysis: DDx contPulmonary Vascular Disorders
PEA-V malformationsElevated pulmonary pressure (LV failure)

Hemoptysis: Evaluation
Adapted from Harrison’s

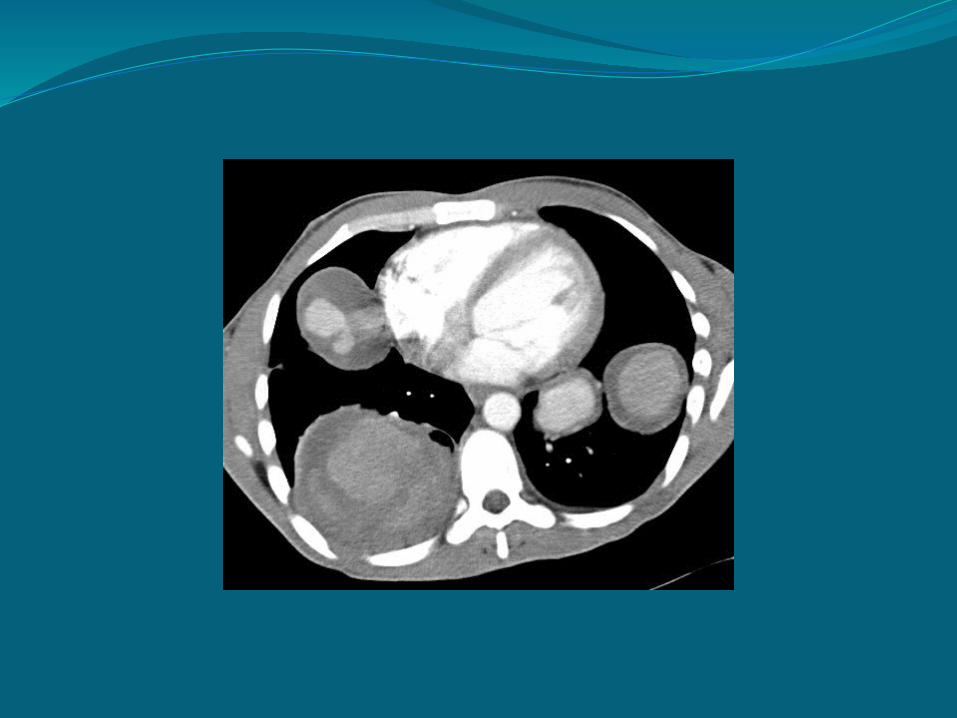
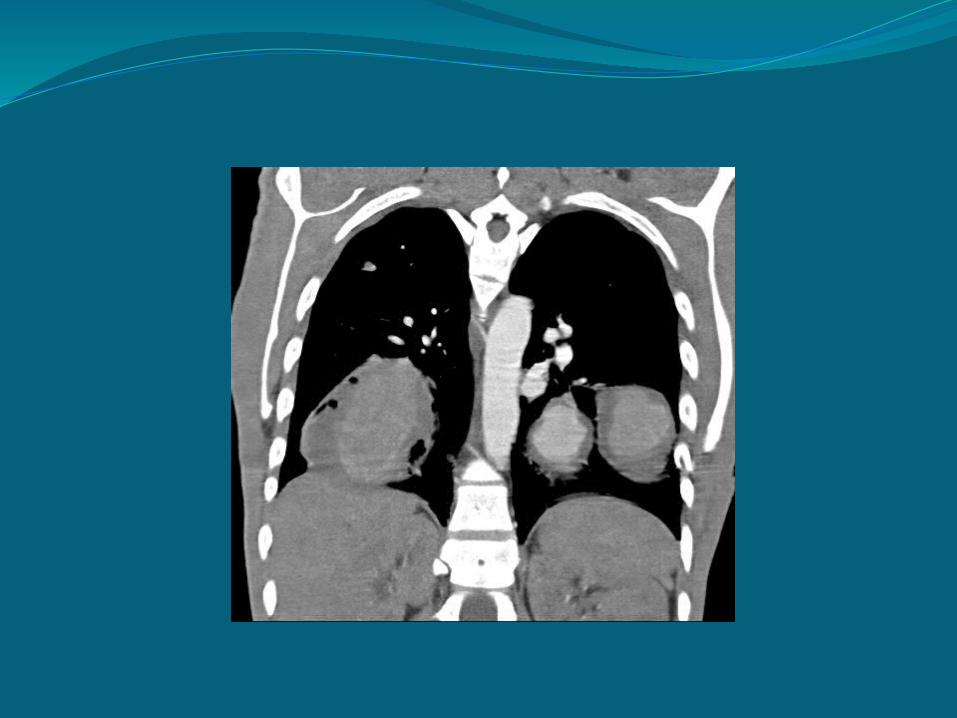
BackgroundFirst described by Hughes and Stovin in 1959
4 cases of multiple pulmonary artery aneurysms associated with venous thrombosis


Hughes Stovin SyndromeMostly men, age 12-40Present with hemoptysis, cough, dyspnea,
chest pain.Can present with fever, elevated ICP

Kinderman et al

PathogenesisUnknownAneurysms thought to be related to
weakening of the vessel wall due to inflammation
Related to Behcet’s disease?

Behcet’s diseaseChronic inflammatory diseaseManifestations are due to vasculitisCharacterized by recurrent oral ulcers and
systemic manifestations including: Genital ulcers, ocular disease, skin disease, vascular disease, arthritis
More common along ancient silk road Turkey: (80 to 370 per 100,000)Japan, China: (13 to 20 per 100,000)North America: (6 per 100,000)

Behcet’s disease: contNo pathognomonic tests, Dx based on clinical
findings
Criteria for diagnosisRecurrent oral ulcers (3x per year) plus 2 of
the following Recurrent genital ulcers Eye lesions (uveitis, retinal vasculitis) Skin lesions (erythema nodosum) Positive pathergy test
International Study Group for Behcet’s Disease


Behcet’s DiseaseVascular disease
Involves blood vessels of all sizesCan involve both arterial and venous sides of
circulationLarge vessel involvement in 1/3 patients
Thrombus, stenosis, aneurysm formationPulmonary arterial involvement in
characteristic Hemoptysis is the most common presenting
symptom
UpToDate

Association with Behcet’s? Similarities between the pulmonary involvement of Behcet’s disease
(BD) and Hughes-Stovin syndrome (HSS) Gender
Mostly young males
Common clinical manifestations Fever Arthralgia Thrombosis
Pulmonary artery aneurysm (PAA) Association with thrombosis HSS: 100% BD: 80%
Common histopathologic findings of PAA: Perivascular inflammation Arterial wall destruction
Treatment of choice Cyclophosphamide or azathioprine and corticosteroids
Prognosis of HSS and BD (in the presence of PAA) Usually fatal due to the rupture of PAA
Adapted from Erkan et al

TreatmentImmunosuppresionSurgical resection of high risk lesions
Limited to 1 segment of 1 lungTranscatheter embolization
No specific treatment guidelines

TreatmentLee et al describe a case similar to ours
48 yo male p/w fever, dyspnea, wt loss CT showed multiple pulmonary arteries Underwent embolization and later R lobectomy Aneurysms returned, L lobectomy performed Discharged on prednisolone 5 mo later, new aneurysms Started on cytoxan CXR at 3 monthsno aneurysms

What happened?Received high dose solumedrol x 3 daysHad right thoracotomy and lobectomyPath: No active vasculitisStarted on Imuran and Prednisone

Works CitedChalazonitis et al, Hughes Stovin Syndrome: a case report
and review of the literature, Cases Journal 2009, 2:98Criteria for diagnosis of Behcet’s disease. International Study
Group for Behcet’s Disease. Lancet 1990; 335:1078Erkan et al, Is Hughes Stovin Syndrome Behcet’s disease?,
Clin Exp Rheumatol 2004; 22(Suppl 34): 564-568Kinderman M, Wilkens H, Hughes Stovin Syndrome,
Circulation 2003;108;e156Lee et al, Successful cyclophosphamide therapy with
complete resolution of pulmonary artery aneurysm in Hughes-Stovin syndrome patient, Clin Rheumatol (2008) 27: 1455-1458
Harrison’s Internal MedicineUptodate.com

Questions?







