Download - Nasal septum & its diseases

NASAL SEPTUM & ITS DISEASES
NAVAS SHAREEF .P .P
KMCT MED COLLEGE ; CALICUT ; INDIA
Email:[email protected]

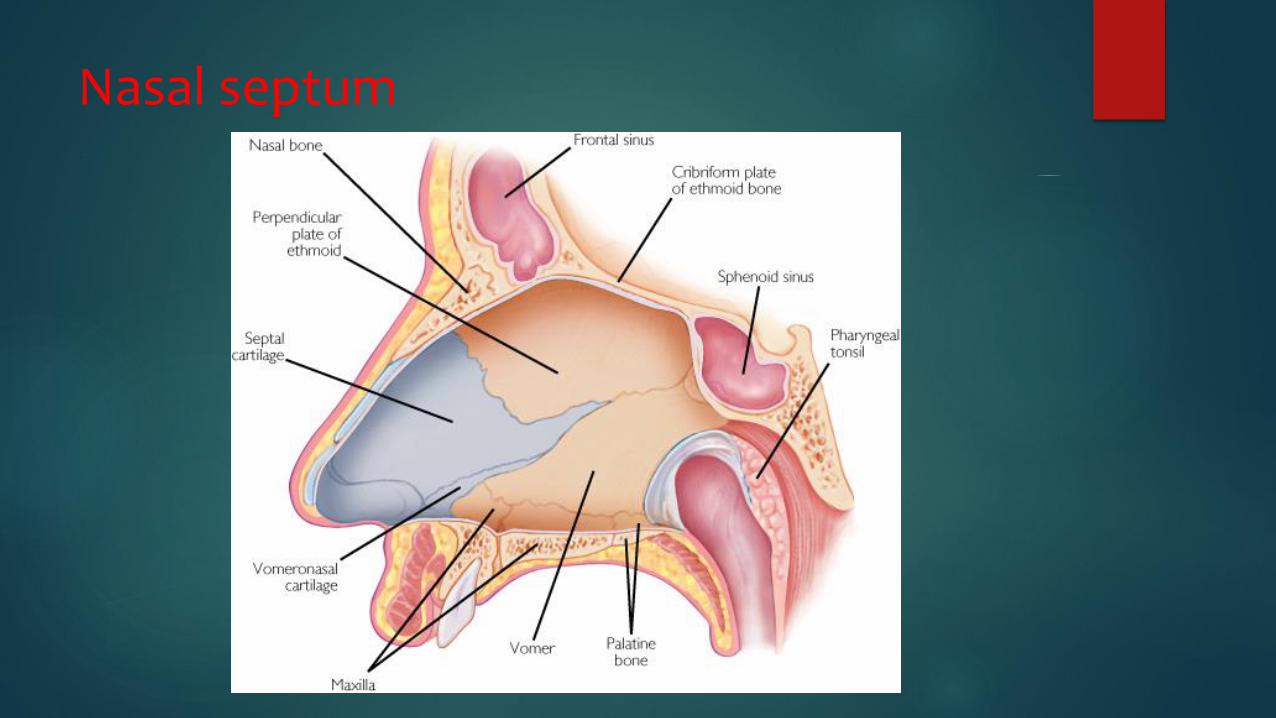
Nasal septum
Anatomy
3 parts
1)Columellar septum
2)Membranous septum
3)Septum proper
Nasal septum

1.Columellar septum
Formed of columella containing the
medial crura of alar cartilage united
together by fibrous tissue and covered
on either side by skin
2.Membranous Septum
Double layer of skin
No bony or cartilaginous support
Lies b/w columella & caudal border of septal
cartilage.
Both columella & membranous parts are freely
movable from side to side
3.Septum proper
Osteocartilagenous frame work
Covered with nasal mucous membrane
1.Perpendicular plate of ethmoid
2.The vomer
3.Large septal cartilage

Minor contributions from
-Crest of nasal bone
-Nasal spine of frontal bone
-Rostrum of sphenoid
-Crest of palatine bone
-Crest of maxilla
-Anterior nasal spine of maxilla

Septal cartilage
Partition b/w right&left nasal cavities.
Provides support to the tip & dorsum of cartilaginous part
of nose.
Its destruction ( in Septal abscess, injuries, tuberculosis,
excessive removal during septal surgery ) causes
depression of lower part of nose &drooping of nasal tip

Blood supply of nasal septum
Little’s area/Kiesselbach’s plexus
Vascular area in the anteroinferior part of nasal septum.
-Anterior ethmoidal artery
-Spheno palatine
-Greater palatine
-Septal branch of superior labial
+corresponding veins
Commonest site for epistaxis
Site for origin of “Bleeding polypus”(Hemangioma) of nasal
septum
Nerve supply
1)Nerves of common sensation
Anterior ethmoidal nerve.
Branches of sphenopalatine ganglion.
Branches of infra orbital nerve
2)Olfactory nerves.
3)Autonomic nerves.

Nerve supply

Fractures of nasal
septumAetiopathogenesis
Trauma
Fracture of septal cartilage or its
dislocation from vomerine groove
Septal injuries
with mucosal tear-profuse epistaxis
with intact mucosa-hematoma.
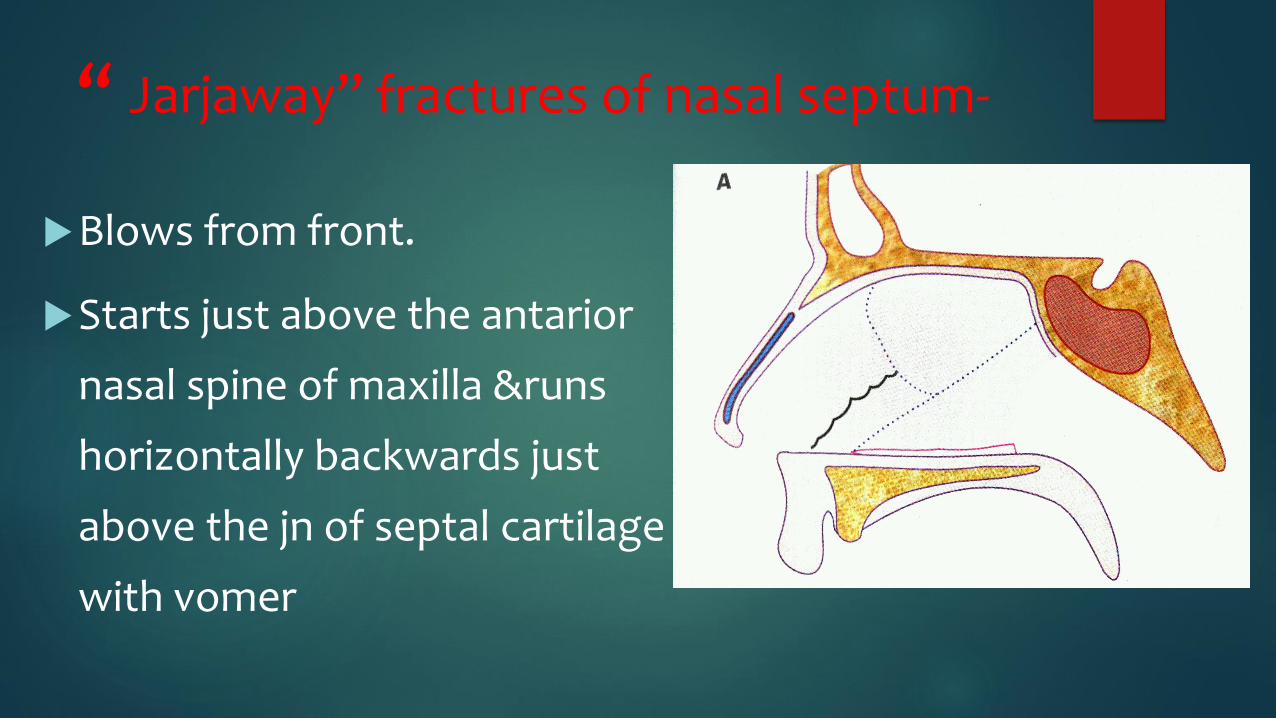
“ Jarjaway” fractures of nasal septum-
Blows from front.
Starts just above the antarior
nasal spine of maxilla &runs
horizontally backwards just
above the jn of septal cartilage
with vomer

“Chevallet” fractures of septal cartilage
Blows from below.
Runs vertically from antarior
nasal spine of maxilla upwards
to the jn of bony and
cartilaginous dorsum of nose.
Treatment of Fractures of nasal
septum
Hematoma should be drained
Dislocated or fractured septal fragments
should be repositioned& supported.


Complications of Fractures of nasal
septum
If injuries are ignored ,they would result in
deviation of cartilaginous nose
assymetry of nasal tip,columella
or the nostril.
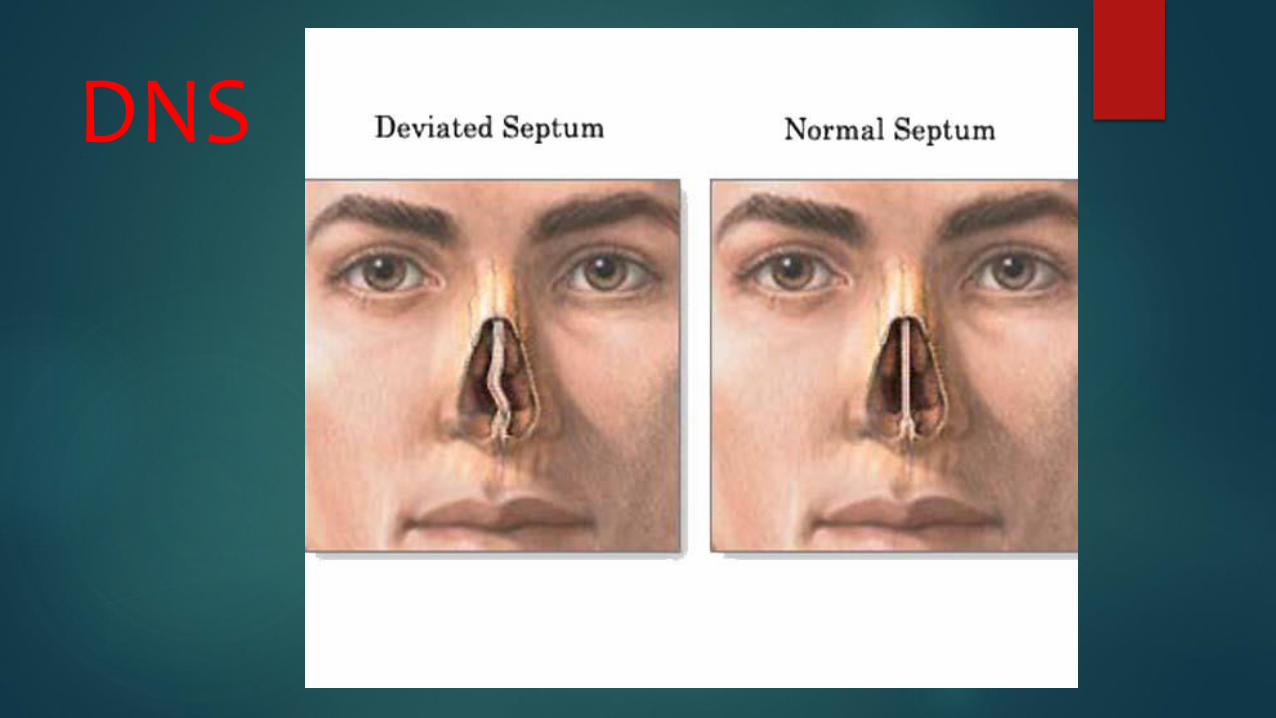
DNS
DEVIATED NASAL SEPTUMAetiology
1)Trauma
Lateral blow on nose:-displacement of septal
cartilage from the vomerine groove&maxillary
crest
Crushing blow from the front:-buckling or
twisting fractures
Trauma at birth during passage thru birth canal.
2)Developmental error
3)Racial factors
Caucasians affected more than negroes
4)Hereditary factors
Several members of the same family may have
deviated nasal septum.

Types of DNS
1)Anterior dislocation
Nasal septum dislocated to one of
the nasal chambers.
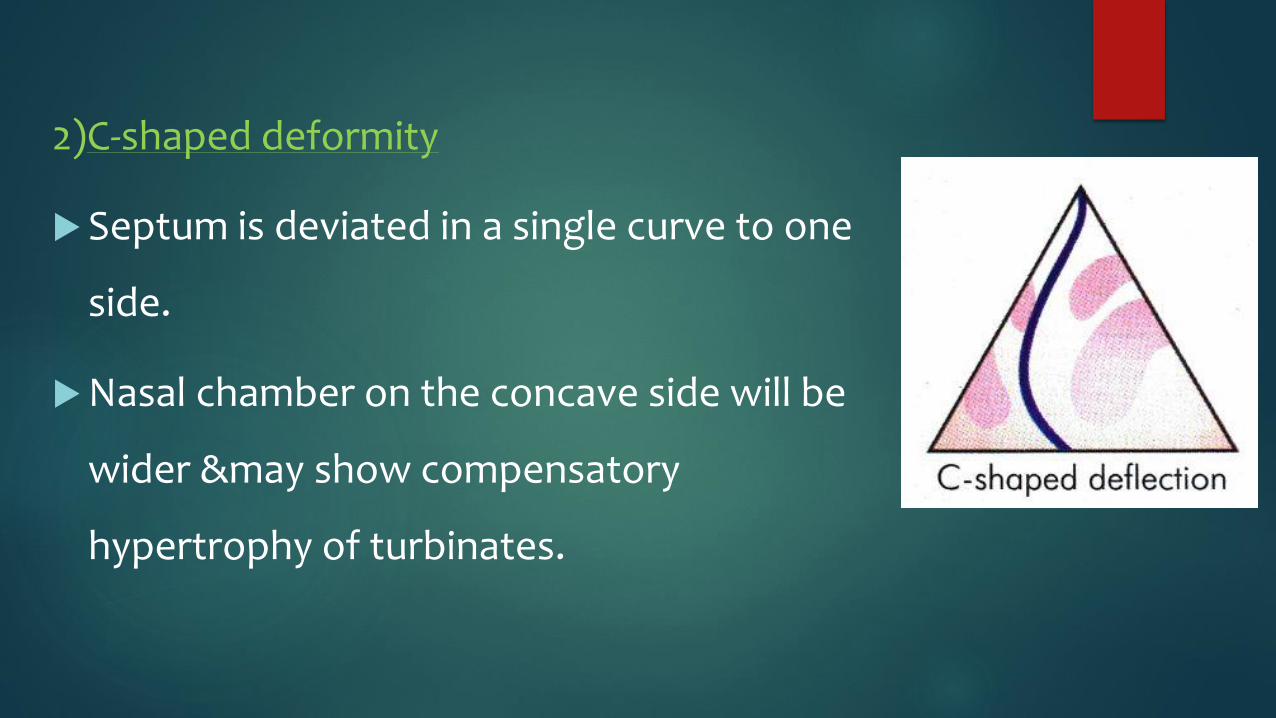
2)C-shaped deformity
Septum is deviated in a single curve to one
side.
Nasal chamber on the concave side will be
wider &may show compensatory
hypertrophy of turbinates.

3)S-shaped deformity
Septum may show an S-shaped
curve either in vertical or
anteroposterior plane.
Causes bilateral nasal
obstruction.
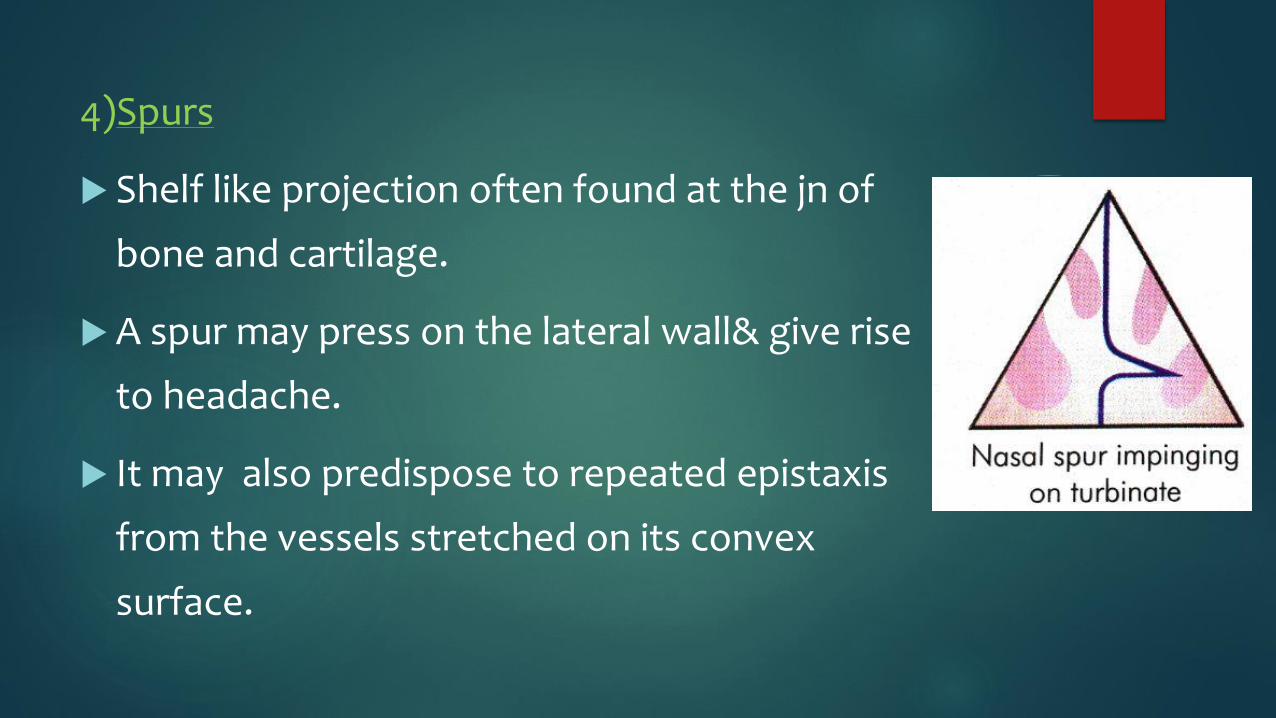
4)Spurs
Shelf like projection often found at the jn of
bone and cartilage.
A spur may press on the lateral wall& give rise
to headache.
It may also predispose to repeated epistaxis
from the vessels stretched on its convex
surface.

5)Thickening
Due to organised hematoma or
Overriding of dislocated septal
fragments.

Clinical features :DNS DNS can involve any age and sex
Males are affected more than females
1)Nasal obstruction Unilateral/bilateral
Site of obstuction
i. Vestibular
ii. At the nasal valve
iii. Attic
iv. Turbinal
v. Choanal
COTTLE TEST
Used to know whether nasal obstruction is due to
septal abnormality or not?
Cheek is drawn laterally while the patient breathes
quietly
If the nasal airway improves on the test side,test is +
ve
Indicates abnormality vestibular component of nasal
valve

COTTLE TEST
2)Headache
Deviated septum,esp. a spur may press on
lateral wall of nose giving rise to pressure
headache
3)Sinusitis
Deviated septum may obstruct sinus ostia
poor ventillation of sinus predispose or
perpetuate sinus infection.

4)Epistaxis
Mucosa over the deviated parts of
septum exposed to drying effects of
air currents formation of crusts which
when removed causes bleeding
Bleeding may occur from vessels over a
nasal spur

5)Anosmia
Failure of inspired air to reach the
olfactory region may result in total or
partial loss of sense of smell.
6)External deformity
7)Middle ear infection
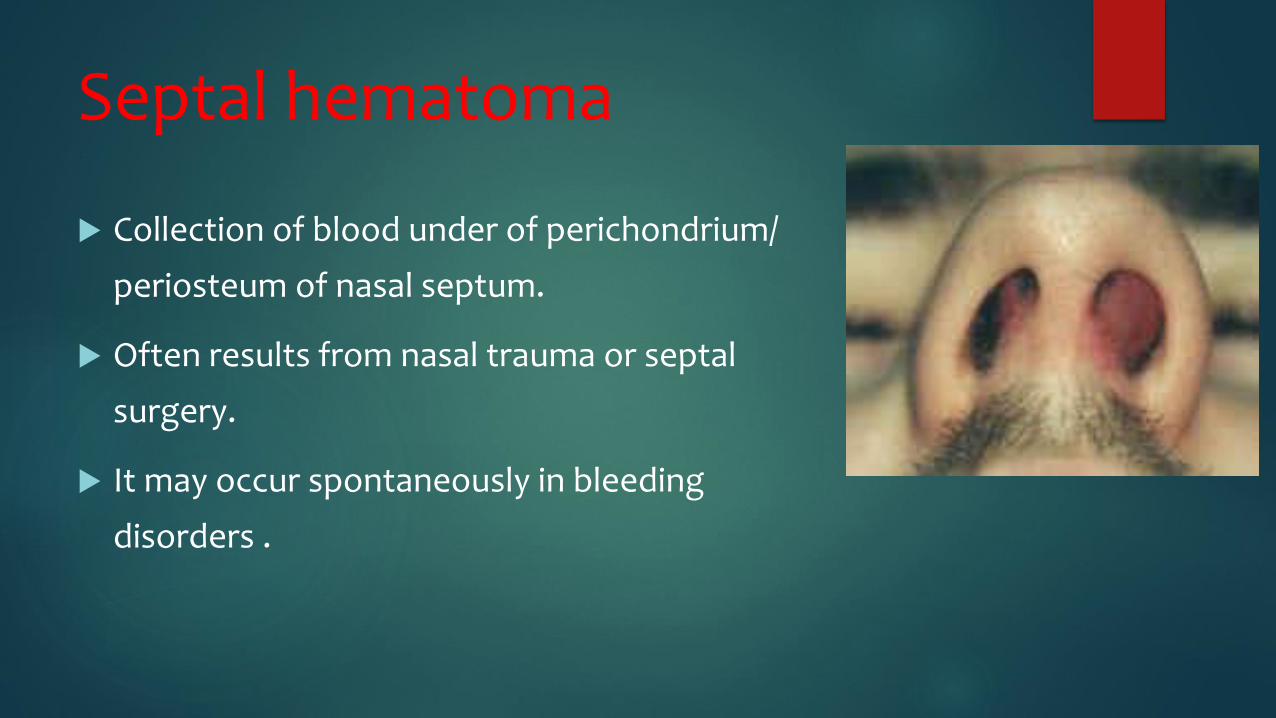
Septal hematoma
Collection of blood under of perichondrium/
periosteum of nasal septum.
Often results from nasal trauma or septal
surgery.
It may occur spontaneously in bleeding
disorders .
Clinical features :Septal hematoma
Bilateral nasal obstruction.
Frontal headache & sense of pressure over
nasal bridge.
Examn –smooth rounded swelling of the
septum in both the nasal fossa.
Palpation-mass soft & fluctuant.

Treatment :Septal hematoma
Small hematomas aspirated with a wide
bore sterile needle.
Large hematomas incised and drained.
Following drainage nose is packed on
both sides to prevent reaccumulation.
Systemic antibiotics should be given to
prevent septal abscess.

Complications :Septal hematoma
Septal hematoma if not
drainedorganise into fibrous tissue
leading to permanantly thickened septum
Secondary infection results in septal
abscess with necrosis of
cartilage&depression of nasal septum.

Septal abscess
Aetiology
Mostly from secondary infection of septal
hematoma.
Occassionally it follows furuncle of the nose or
upper lip.
It may follow a/c infection such typhoid or measles

Complications Septal abscess
Necrosis of septal cartilagedepression of
the cartilaginous dorsum.
Necrosis of septal flapsseptal
perforation.
Meningitis&cavernous sinus thrombosis-
rare &serious complication

Perforation of nasal septum
Aetiology
1)Traumatic perforation
Most common cause.
Common forms of trauma-injury to mucosal flaps during
SMR,cauterisation of septum with chemicals/galvanocautery
for epistaxis,habitual nose pricking.

2)Pathologic perforation
Septal abscess
Nasal myiasis
Rhinolith/neglected foreign body causing pressure
necrosis.
c/c granulomatous condn
lupus,TB,leprosy (perforation in cart. Part)
Syphilis (bony part)
Wegener’s granuloma-midline destructive lesion-
cause total septal perforation.

3)Drugs & chemicals
i. Prolonged use of steroid sprays in nasal allergy.
ii. Coccaine addicts.
iii. Workers in certain occupations,eg.Cr plating,dichromate/soda
ash(sod.carbonate) manufacture or those exposed to As.
4)Idiopathic
No h/o trauma,previous disease or Pt. may be unaware of
existence of perforation.

Clinical features:Perforation
Small ant.perforation-whistling sound
during inspiration/expiration.
Larger perforation-develop crusts
which obstruct the nose or may cause
severe epistaxis when removed

Treatment of septal perforation
Find the cause of perforation first
Inactive small perforation can be surgically closed by
plastic flaps.
Larger perforation difficult to close.
Their t/t is aimed to keep the nose crust free by alkaline
nasal douches&application of a bland oinment.
Thin sialistic button worn to get relief
from symptoms.
.....THANK U.....







