NEXT STEPS
Objectives of the meeting - review
1. Orient key stakeholders about the context and implications of the recommendations of the Commission on Information and Accountability for Women's and Children's Health
2. Assess the current situation in terms of progress and plans, opportunities and challenges for implementing the recommendations, and identity priority actions
3. Building on existing plans and frameworks, develop a country roadmap for enhancing accountability for the next 4 years, outlining how the gaps and priorities will be addressed and implemented.
4. Establish a shared understanding of the work required and the roles and responsibilities of each partner to implement the roadmap.
Accountability framework 7 areas of action
1. Strengthening monitoring of results
2. Strengthening innovation through the use of ICT
3. Strengthening civil registration and vital statistics
4. Maternal death surveillance and response and quality of care assessments
5. National review and accountability mechanisms
6. Resource tracking and national health accounts
7. Advocacy and outreach
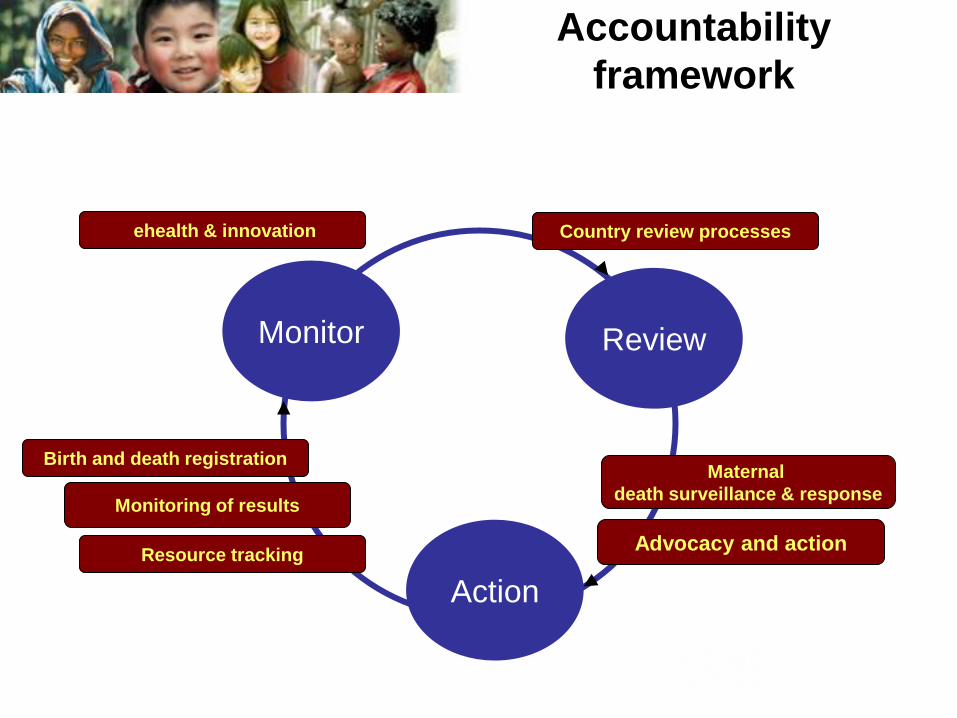
Accountability
framework
Monitor
Action
Review
Monitoring of results
Maternal
death surveillance & response
Resource tracking
ehealth & innovation Country review processes
Advocacy and action
Birth and death registration
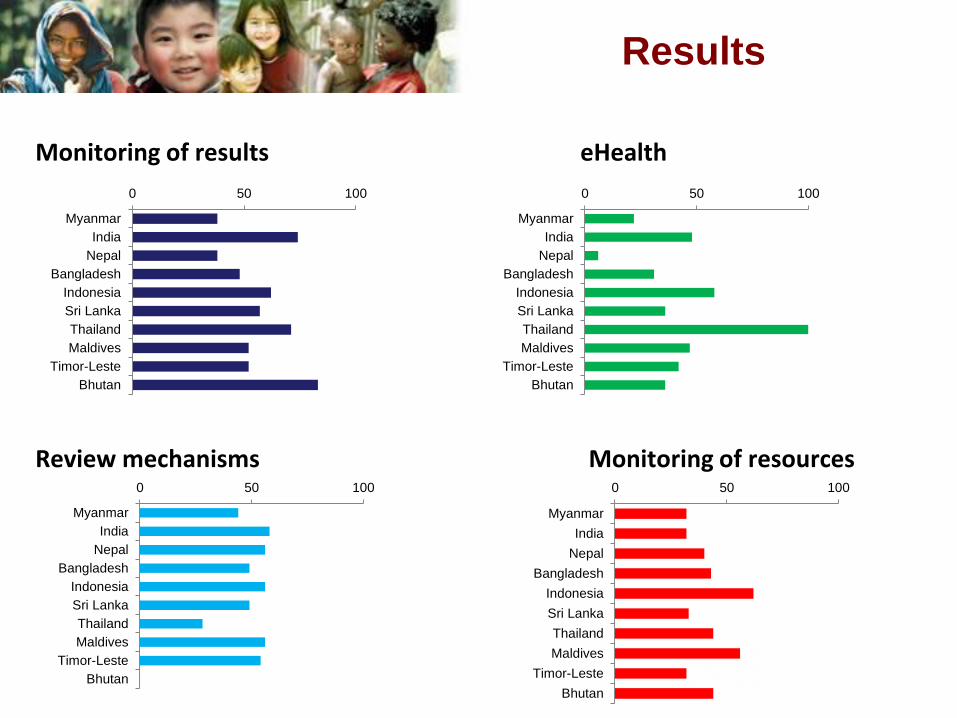
Results
0 50 100
Myanmar
India
Nepal
Bangladesh
Indonesia
Sri Lanka
Thailand
Maldives
Timor-Leste
Bhutan
0 50 100
Myanmar
India
Nepal
Bangladesh
Indonesia
Sri Lanka
Thailand
Maldives
Timor-Leste
Bhutan
0 50 100
Myanmar
India
Nepal
Bangladesh
Indonesia
Sri Lanka
Thailand
Maldives
Timor-Leste
Bhutan
0 50 100
Myanmar
India
Nepal
Bangladesh
Indonesia
Sri Lanka
Thailand
Maldives
Timor-Leste
Bhutan
Monitoring of results eHealth
Review mechanisms Monitoring of resources
Results
• Summary scores
• Assessment report
• Summary Roadmap development
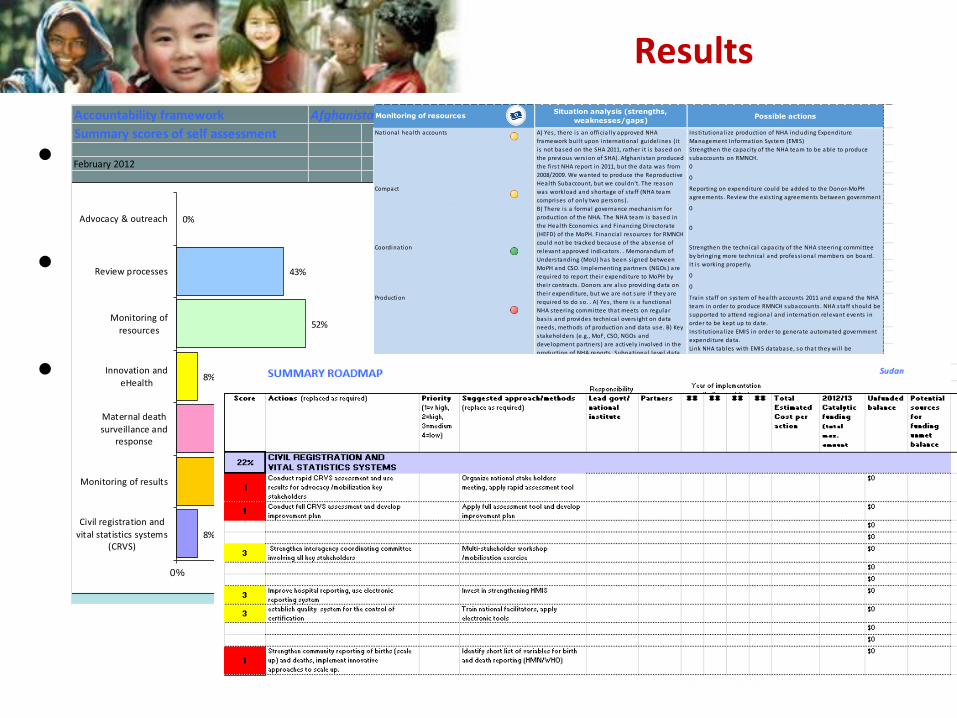
Accountability framework Afghanistan
Summary scores of self assessment
February 2012
Civil registration and vital statistics systems (CRVS) 8%
Monitoring of results 29%
Maternal death surveillance and response 26%
Innovation and eHealth 8%
Monitoring of resources 52%
Review processes 43%
Advocacy & outreach #DIV/0!
8%
29%
26%
8%
52%
43%
0%
0% 20% 40% 60% 80% 100%
Civil registration and
vital statistics systems(CRVS)
Monitoring of results
Maternal death
surveillance andresponse
Innovation and
eHealth
Monitoring of
resources
Review processes
Advocacy & outreach
Situation analysis (strengths,
weaknesses/gaps)Possible actions
National health accounts3
Insti tutional ize production of NHA including Expenditure
Management Information System (EMIS)
Strengthen the capaci ty of the NHA team to be able to produce
subaccounts on RMNCH.
0
0
Compact 3
Reporting on expenditure could be added to the Donor-MoPH
agreements . Review the exis ting agreements between government
and partners and improve mutual accountabi l i ty and transparancy 0
0
Coordination4
Strengthen the technica l capaci ty of the NHA steering committee
by bringing more technica l and profess ional members on board.
It i s working properly.
0
0
Production
2
Tra in s taff on system of health accounts 2011 and expand the NHA
team in order to produce RMNCH subaccounts . NHA staff should be
supported to attend regional and internation relevant events in
order to be kept up to date.
Insti tutional ize EMIS in order to generate automated government
expenditure data.
Link NHA tables with EMIS database, so that they wi l l be
populated automatica l ly once EMIS i s insti tutional ized.
0
0
Analys is 2 Produce analytica l summaries annual ly.
Use SHA 2011 for production of NHA tables after 2013. Diss iminate
the report widely to make i t accessable to publ ic access .
0
0
Data
Use2
Promote use of NHA data in pol icy making process .
0
0
Monitoring of resources
A) Yes , there i s an officia l ly approved NHA
framework bui l t upon international guidel ines (i t
i s not based on the SHA 2011, rather i t i s based on
the previous vers ion of SHA). Afghanis tan produced
the fi rs t NHA report in 2011, but the data was from
2008/2009. We wanted to produce the Reproductive
Health Subaccount, but we couldn't. The reason
was workload and shortage of s taff (NHA team
comprises of only two persons).
B) There i s a formal governance mechanism for
production of the NHA. The NHA team is based in
the Health Economics and Financing Directorate
(HEFD) of the MoPH. Financia l resources for RMNCH
could not be tracked because of the absense of
relevant approved indicators . . Memorandum of
Understanding (MoU) has been s igned between
MoPH and CSO. Implementing partners (NGOs) are
required to report their expenditure to MoPH by
their contracts . Donors are a lso providing data on
their expenditure, but we are not sure i f they are
required to do so. . A) Yes , there i s a functional
NHA steering committee that meets on regular
bas is and provides technica l overs ight on data
needs , methods of production and data use. B) Key
s takeholders (e.g., MoF, CSO, NGOs and
development partners ) are actively involved in the
production of NHA reports . Subnational level data
i s provided by NGOs. . A) We bel ieve that the
human capaci ty i s not adequate for production of
RMNCH subaccounts . B) Government expenditure
data i s not converted automatica l ly to NHA format
right now, but i t wi l l be poss ible once EMIS i s ful ly
functional . C) EMIS should serve as a centra l
database for production of automated s tandard
NHA table, including table by beneficiaries and
automated production of key RMNCH indicators . . A)
MoPH does not produce analytica l summaries , but
we have the ful l NHA report 2008/2009 in Engl ish
and Dari languages . We do not use SHA 2011, but
we use the previous vers ion of SHA. B) The NHA
report (which i s not produced according to SHA
2011) i s ava i lbe to publ ic access on
www.moph.gov.af and www.who.int.. Yes , i t i s an
Next steps
• Web publishing of draft assessment results (transparency!)
• National accountability framework workshop (suggested national workshop to be organized within 2-3 months)
• Finalize roadmap and submit to WHO
• Web publish the final roadmap (transparency!)
• Get catalytic funding
• IMPLEMENT
• Orient key country stakeholders about the context and implications of the recommendations of the Commission on Information and Accountability for Women's and Children's Health;
• Review the initial assessment (prepared by the country team in this workshop) and possible actions
• Take into consideration the results of the initial assessment results:
• Finalize the list of priorities
• Finalize the approach/methods
• Define responsibilities (government/partners)
• Indicate year of implementation (including catalytic actions for 2012-13)
• Estimate total per action and catalytic funding
What happens in a national
workshop?
What are the expected outputs of the national
workshop?
• Increased awareness and understanding by all stakeholders of the Commission recommendations and opportunities/challenges for country implementation;
• A completed review of the final draft of the accountability roadmap, identifying the priority actions and budget
• Group work on the identified priority areas – aim to identify the priority areas for strengthening during 2012-15, with cost implications for 2012-13.
• Catalytic US$ 250,000 potentially available from the CoIA
Further information
http://www.who.int/woman_child_accountability/en/
Accountability
Monitor
Action
Review
THANK YOU







