NONVERBAL LEARNING DISABILITY
& ASPERGER’S DISORDER
LINDA C. CATERINO, PH.D., ABPPARIZONA STATE UNIVERSITY
Objectives
� 1. Participants will learn the specific neuropsychological characteristics of individuals with Nonverbal Learning Disabilities (NLD).
� 2. Participants will learn the current status of the support for the diagnosis of NLD.
� 3. Participants will learn the specific diagnostic criteria for Asperger’s Syndrome (AS).
� 4. Participants will learn about differential diagnosis regarding NLD and AS.
History - Gerstmann Syndrome
� Josef Gerstmann- Austrian-American neurologist
� Wrote 1st published article on Gerstmann Syndrome
� Symptoms
� Finger agnosia
� Right-left orientation confusion
� Agraphia
� Acalculia
Johnson & Myklebust
� Proposed a nonverbal type of disability characterized by absence of serious
language problems and adequate or above skills in reading and writing,
� Higher verbal than performance IQ
� Problems in visual-spatial processing
� Spatial orientation, right-left orientation, body image, motor learning
� Difficulties in temporal perception
� Handwriting
� Mathematics
� Distractible
� Perseveration
� Disinhibition
� Deficiencies in social perception - “unable to comprehend the significance of
many aspects of his environment”
� (Myklebust, 1967;Johnson &Myklebust, 1975; Boshes & Myklebust, 1964)
Byron Rourke
� Neuropsychology of Learning Disabilities: Essentials of Subtype Analysis (1985)
� Syndrome of Learning Disabilities: Neurodevelopmental Manifestations (1995)
� Identified a group of children with a pattern of neuropsychological strengths and weaknesses
Rourke’s Description of NLD
� Neuropsychological assets in auditory perception, auditory attention, and auditory memory, especially for verbal material.
� Adequate skills in rote verbal memory & language, amount of verbal associations and language output.
� Poor visual-spatial organizational, psychomotor, tactile-perceptual, and concept formation skills, simple motor skills may be well developed
� Academic assets = single-word reading & spelling.
� Academic difficulties in (e.g., arithmetic, science)
� Difficulties in informal learning (e.g., as transpires during play and other social situations).
� Psychosocial deficits, primarily of the internalized variety, are usually evident by late childhood and adolescence and into adulthood.
Cognitive/Neuropsychological
� Strengths
� VIQ>PIQ by 10-15 pts or more
� Good receptive& expressive language , High in Similarities
� Verbal Recognition, Repetition, Associations, Storage, Output
� Auditory Perception
� Verbal Attention & Rote Memory
� Focus on Details
� Simple motor skills intact
� Grip strength normal
� Finger tapping average
� Deficiencies
� PIQ<VIQ, Block Design, Object Assembly, Picture Arrangement& Coding
� Bilateral Tactile Perception (more on left )
� Finger localization, fingertip number writing
� Tactile Form Recognition & Memory
� Bilateral Visual Perception
� Visual Memory (particularly as figures become more complex)
� Visual discrimination/Visual figure ground
� Visual spatial organizational abilities
� Perseveration
� Attention
� Selective attention
� Novel Material
� Understanding the big picture
� Concept Formation
� Nonverbal Problem Solving
Specific NLD Proposed Criteria � (1) Less than two errors on simple tactile perception and suppression vs. finger agnosia, finger
dysgraphesthesia, and astereognosis. Simple composite greater than 1 SD below the mean. Simple tactile-perceptual skills are superior to complex tactile-perceptual skills.(2) WRAT /WRAT -R standard score for Reading is at least 8 points greater than Arithmetic. Single word reading is superior to mechanical arithmetic.(3) Two of WISC/WISC- R Vocabulary, Similarities, and Information are highest of the Verbal scale. Straightforward and/or rote verbal skills are superior to those involving more complex processing (e.g., Comprehension).
� (4) Two of WISC/WISC -R subtests Block Design, Object Assembly, and Coding subtests are the lowest of the Performance scale. Complex visual-spatial-organizational skills and speeded eye-hand coordination are impaired.(5) Target Test at least 1 SD below the mean. Memory for visual sequences is impaired.(6) Grip strength within one standard deviation of the mean or above vs. Grooved Pegboard Test greater than one standard deviation below the mean. Simple motor skills are superior to those involving complex eye-hand coordination, esp. under speeded conditions. (7) Tactual Performance Test Right, Left, and Both hand times become progressively worse vis-à-vis the norms. Complex tactile-perceptual and problem-solving skills under novel conditions are impaired.(8) WISC/WISC -R VIQ > PIQ by at least 10 points. Verbal skills are superior to visual-spatial-organizational skills.
� The following criteria are currently under investigation:7 or 8 of criteria = definite NLD
� 5 o 6 of criteria = probable NLD
� 3 or 4 of these criteria - Questionable NLD
� 1 or 2 of these features: Low Probability of NLD
�
Drummond, C. R., Ahmad, S. A., & Rourke, B. P. (2005). Rules for the classification of younger children with Nonverbal Learning Disabilities and Basic Phonological Processing Disabilities. Archives of Clinical Neuropsychology, 20, 171-182.
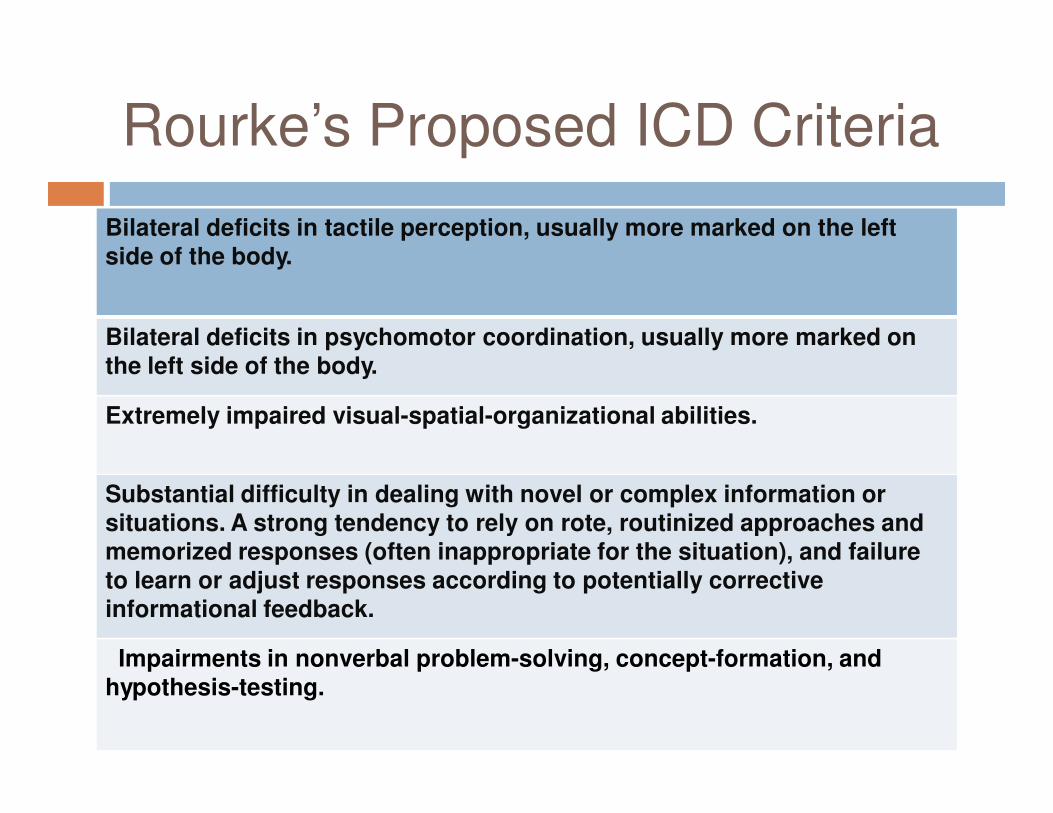
Rourke’s Proposed ICD Criteria
Bilateral deficits in tactile perception, usually more marked on the left side of the body.
Bilateral deficits in psychomotor coordination, usually more marked on the left side of the body.
Extremely impaired visual-spatial-organizational abilities.
Substantial difficulty in dealing with novel or complex information or situations. A strong tendency to rely on rote, routinized approaches and memorized responses (often inappropriate for the situation), and failure to learn or adjust responses according to potentially corrective informational feedback.
Impairments in nonverbal problem-solving, concept-formation, and hypothesis-testing.
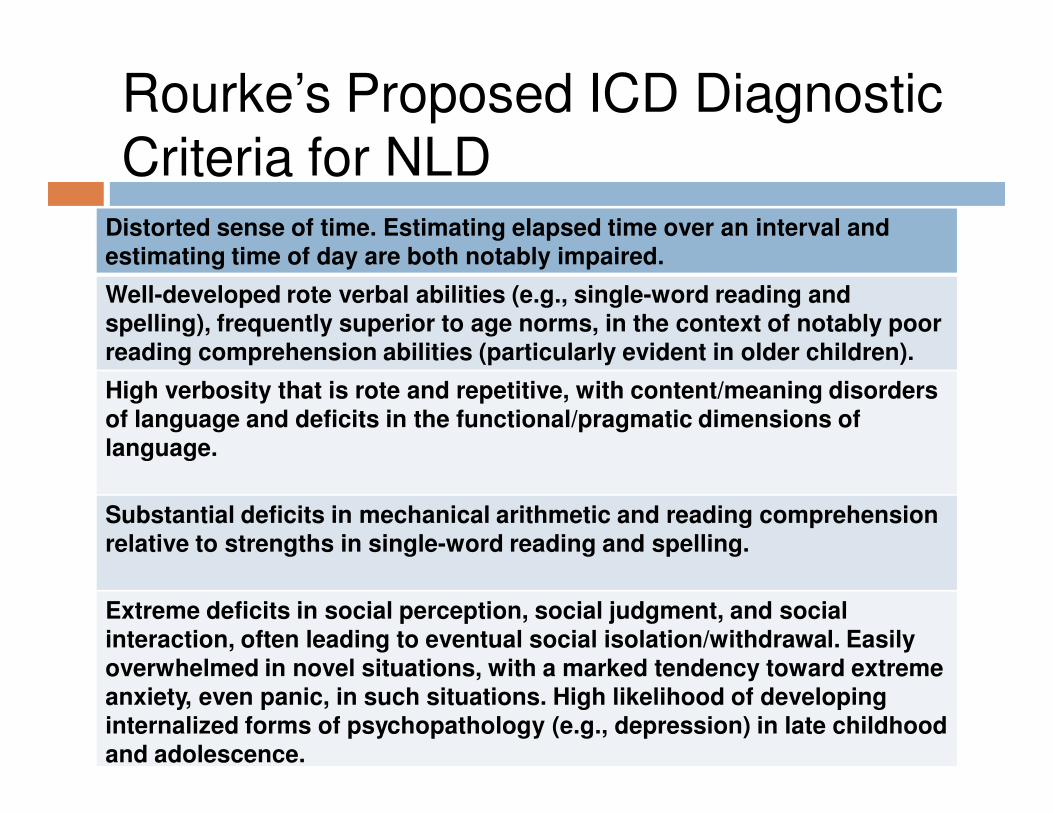
Rourke’s Proposed ICD Diagnostic Criteria for NLD
Distorted sense of time. Estimating elapsed time over an interval and estimating time of day are both notably impaired.
Well-developed rote verbal abilities (e.g., single-word reading and spelling), frequently superior to age norms, in the context of notably poor reading comprehension abilities (particularly evident in older children).
High verbosity that is rote and repetitive, with content/meaning disorders of language and deficits in the functional/pragmatic dimensions of language.
Substantial deficits in mechanical arithmetic and reading comprehension relative to strengths in single-word reading and spelling.
Extreme deficits in social perception, social judgment, and social interaction, often leading to eventual social isolation/withdrawal. Easily overwhelmed in novel situations, with a marked tendency toward extreme anxiety, even panic, in such situations. High likelihood of developing internalized forms of psychopathology (e.g., depression) in late childhood and adolescence.
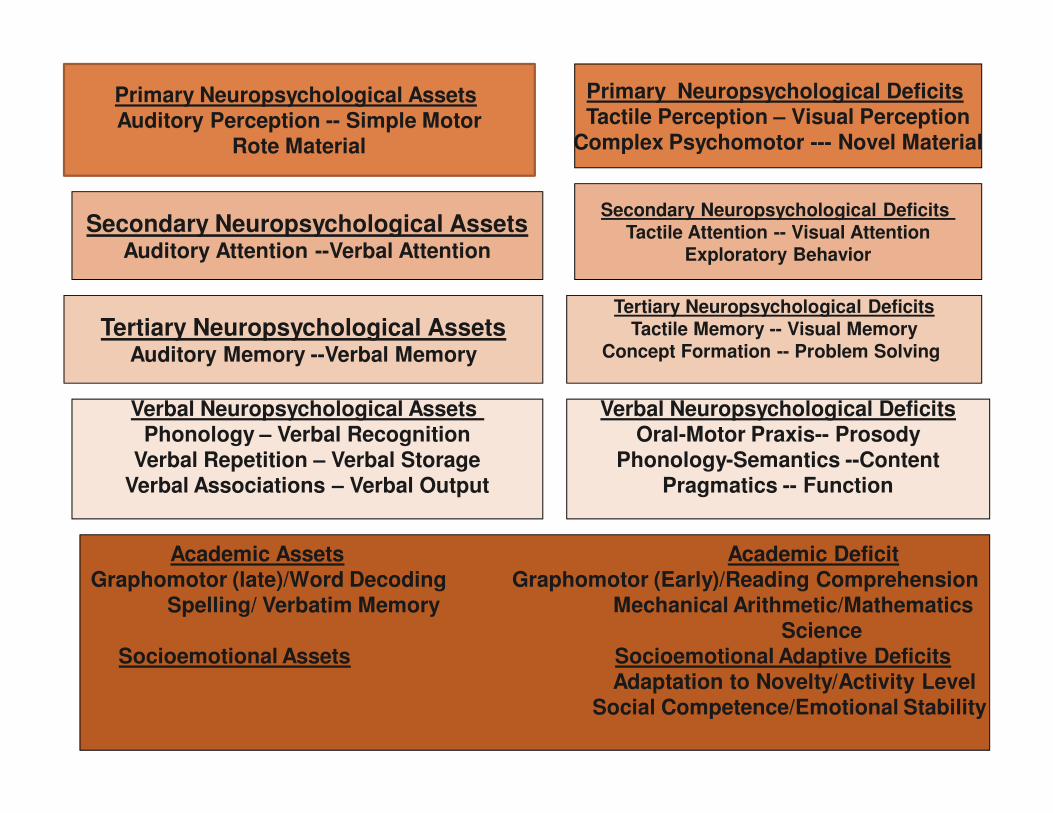
Primary Neuropsychological AssetsAuditory Perception -- Simple Motor
Rote Material
Tertiary Neuropsychological AssetsAuditory Memory --Verbal Memory
Secondary Neuropsychological AssetsAuditory Attention --Verbal Attention
Academic Assets Academic DeficitGraphomotor (late)/Word Decoding Graphomotor (Early)/Reading Comprehension
Spelling/ Verbatim Memory Mechanical Arithmetic/Mathematics Science
Socioemotional Assets Socioemotional Adaptive DeficitsAdaptation to Novelty/Activity Level
Social Competence/Emotional Stability
Verbal Neuropsychological Assets Phonology – Verbal Recognition
Verbal Repetition – Verbal StorageVerbal Associations – Verbal Output
Verbal Neuropsychological DeficitsOral-Motor Praxis-- Prosody
Phonology-Semantics --ContentPragmatics -- Function
Tertiary Neuropsychological DeficitsTactile Memory -- Visual Memory
Concept Formation -- Problem Solving
Primary Neuropsychological DeficitsTactile Perception – Visual Perception
Complex Psychomotor --- Novel Material
Secondary Neuropsychological Deficits Tactile Attention -- Visual Attention
Exploratory Behavior
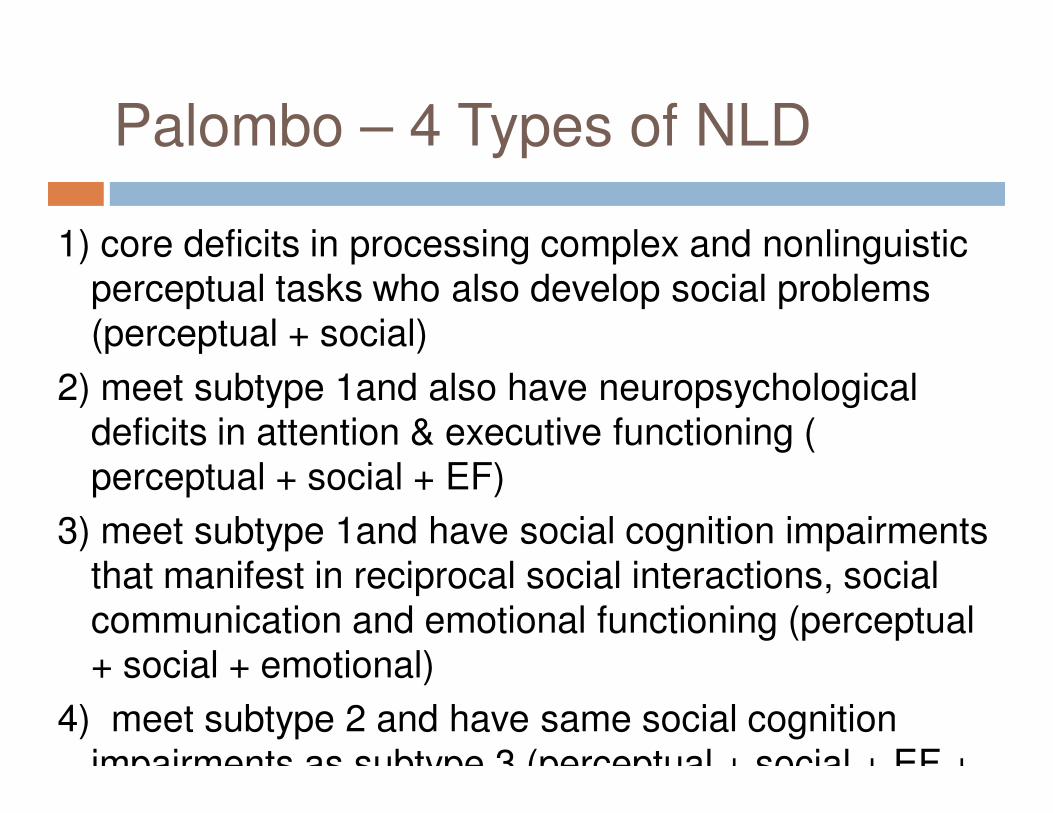
Palombo – 4 Types of NLD
1) core deficits in processing complex and nonlinguistic perceptual tasks who also develop social problems (perceptual + social)
2) meet subtype 1and also have neuropsychological deficits in attention & executive functioning ( perceptual + social + EF)
3) meet subtype 1and have social cognition impairments that manifest in reciprocal social interactions, social communication and emotional functioning (perceptual + social + emotional)
4) meet subtype 2 and have same social cognition impairments as subtype 3 (perceptual + social + EF +
4 Subtypes of NLD
� Davis & Broitman (2011)
� All children with NLD have significant visual-spatial and executive function difficulties
� 1st Core subtype have visual-spatial executive functioning, mild social and academic difficulties
� 2nd Children with visual & executive functioning difficulties that significantly impact their social functioning
� 3rd Children with visual & executive functioning difficulties and significant academic problems
� 4th Children with visual-spatial, executive functioning, social and academic difficulties where all areas are functionally impaired
Davis & Broitman
4. All areas impaired
3. Visual-spatial
Executive
Functioning
Significant Academic Problems
1. Visual –Spatial
Executive functioning
Mild social & Academic
Difficulties
2. Visual-Spatial
Executive Functionin
g that significantl
y impact social
functioning
Hale & Fiorello (2004)
� 2 types
� Executive novel problem solving - frontal
� Posterior visual-spatial holistic problem solving- right hemisphere
Specific Characteristics -
Cognitive
� WISC-III - VIQ greater than PRI by 10 standard score points or more
� 80% have highest standard scores on Information, Similarities or Vocabulary
� 90% had lowest scores on Block Design, Object Assembly, Coding (Drummond, et al., 2005)
� Deficits in:
� Perceptual and Quantitative Reasoning,
� Theory of Mind
Attention
� Attentional Problems – maybe due to Visual Perceptual and tactile difficulties (Rourke, 2000)
� Auditory verbal attention intact
� Problems with Sustained Visual & Divided Attention
� Tend to be diagnosed with ADHD: Predominately Inattentive type (ADHD–PI) but may not be true ADHD (Semrud-Clikeman, 2007).
Executive Functioning
� Hypothesis generation
� Flexible problem solving;
� Self-monitoring;
� Behavior regulation;
� Integration of emotion with context
Speed and Efficiency of
Processing
� Assets -- auditory verbal including sustained auditory attention, reading speed for simple words, and rapid oral word association
� Deficits -- visual attention, tracking, matching, decision making speed, verbal-visual naming, color naming and writing speed
Memory & Learning
� Assets - auditory verbal learning and memory
� Deficits - in visual-visual verbal learning, visual immediate, visual spatial working memory, delayed and long term recall of visual information, Tactile-Kinesthetic Learning and Memory; Location Memory
Visual Processing Deficits
� Visual Perception;
� Scanning-Tracking;
� Figure-ground disturbance
� Visual-spatial
� Constructional
Sensory-Motor Deficits
� Tactile-Kinesthetic;
� Tactile Defensiveness;
� Motor Sequencing,
� Strength
� Gross motor coordination (skipping, bike riding, jump roping)
� Fine Motor coordination (handwriting, coloring, cutting, tracing, fastening, fine motor speed & dexterity)
� Complex psychomotor tasks,
Language
� Asset - but language is pedantic, rote
� Poor prosody and high verbal production
NLD Communication Difficulties
Receptive
May
not under-stand social
Nuances
in conver-sation
(lack
of
tact)
Problems
decoding
prosodic
or
vocal intonation
s
Problems
reading
facial expressio
ns and
gestures
May
lack
sense
of
humor
Concrete interpretation
of
metaphors
Expressive
Good vocabular
y
Lack
of
gestures, facial
expressions or
vocal intonations
Social Deficits
� Facial recognition and emotional expression (visual
attention/memory) (Corbett & Constantine, 2006; Fine, Semrud-
Clikeman, Butcher, & Walkowiak, 2008; Rourke, 2000)
� Emotional nuancing in communication; poor receptivity to
feeling states and states of others;
� Poor prosody and high verbal production does not promote
positive social feed back
� Social judgment secondary to problems with reasoning &
concept formation
� Adaptation to novelty
� Comprehension of humor deficits observed in NLD group with
social perceptual difficulties (not in NLD group with just visual-
spatial difficulties)(Semrud-Clikeman et al., 2008)
NLD Social Difficulties
Limited peer interaction, prefer
one-to-one interaction,, prefer
younger peers
Problems
forming
friendships
Difficulty
reading
social cues
Socially
awkward &
inappropriate
May
withdraw
or
isolate
Rigid,
rule-bound
Disruptive
play
Bossy,
aggressive
& defensive
with peers
Problems
forming
close
personal
attachments
Problems
with
interpersonal
intimacy
Problems
with
adaptability
Emotional
� At risk for internalizing problems, e.g., anxiety & depression (Rourke, 1989; Little, 1993)
� Depression (Cleaver & Whitman, 1998) Children with sxs of right hemisphere white matter dysfunction had arithmetic difficulties and showed significant levels of depression
� Petti et al. (2003) found that children with NLD had a higher percentage of internalizing diagnoses among children at psychiatric treatment facilities.
� Higher risk for suicidal behavior as compared to other LDs (Rourke,1989; Bigler,1989; Fletcher, 1989; Kowalchuk & King,1989) -based on extremely small
Emotional
� Greenham (1999) – evidence not clear if emotional problems are cause
or consequence
� Most individuals with NLD do not develop psychological problems, and
very few commit suicide (Greenham 1999).
� Bloom & Heath (2010) compared 23 12- to 15-year olds with NLD with 23
matching children with “general learning disability” (GLD) and 23 typicals
Self-report scale, an adolescent depression scale,
Facial affect recognition measure,
Ability to make six different facial expressions
Understanding of facial expressions.
GLD did more poorly on recognition, expression, and understanding of
emotions
NLD group did not differ from the typical group
Co-morbidity- ADHD
� Higher rates of ADHD (e.g., Gross-Tur, Shaleve, Manor, &
Amir, 1995; Voeller, 1986)
NLD Emotional Difficulties
Lack of empathy
or compassion
Self critical, perfectionistic,
lack self-confidence
Anxious, worried
Increased risk
for depression
& suicide
Problems modulating
affect
Easily frustrated, loses
control
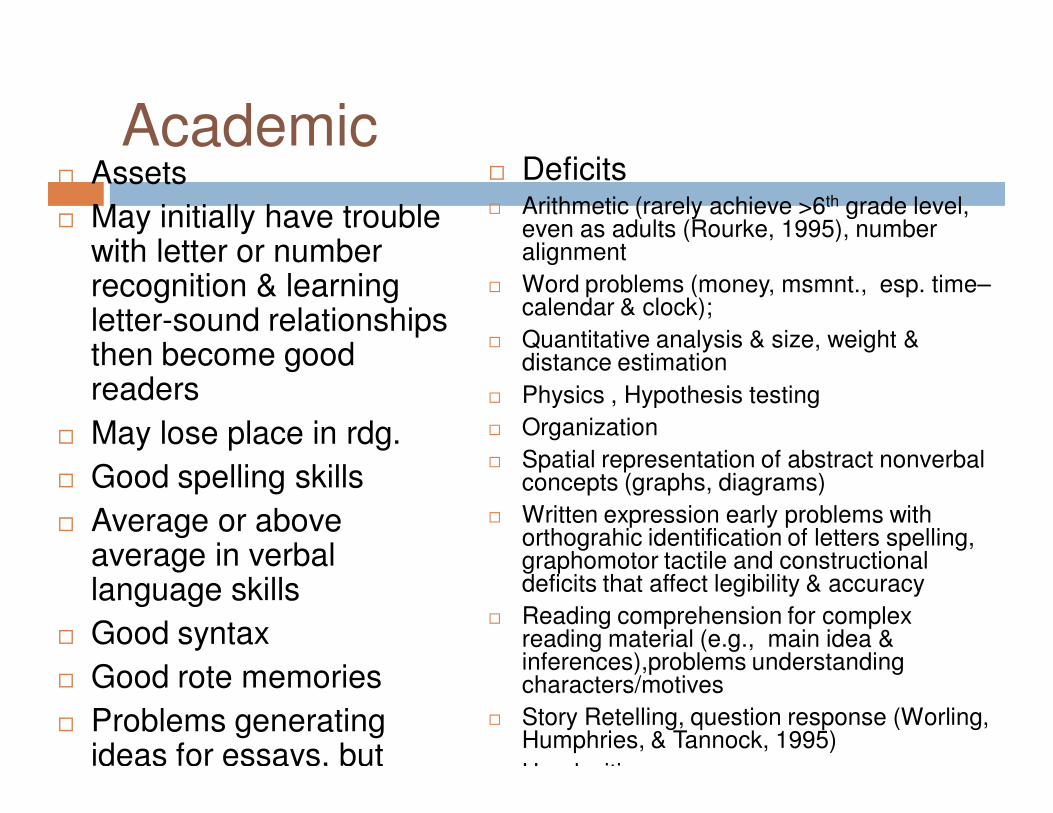
Academic� Assets
� May initially have trouble with letter or number recognition & learning letter-sound relationships then become good readers
� May lose place in rdg.
� Good spelling skills
� Average or above average in verbal language skills
� Good syntax
� Good rote memories
� Problems generating ideas for essays, but
� Deficits� Arithmetic (rarely achieve >6th grade level,
even as adults (Rourke, 1995), number alignment
� Word problems (money, msmnt., esp. time–calendar & clock);
� Quantitative analysis & size, weight & distance estimation
� Physics , Hypothesis testing
� Organization
� Spatial representation of abstract nonverbal concepts (graphs, diagrams)
� Written expression early problems with orthograhic identification of letters spelling, graphomotor tactile and constructional deficits that affect legibility & accuracy
� Reading comprehension for complex reading material (e.g., main idea & inferences),problems understanding characters/motives
� Story Retelling, question response (Worling, Humphries, & Tannock, 1995)
Handwriting
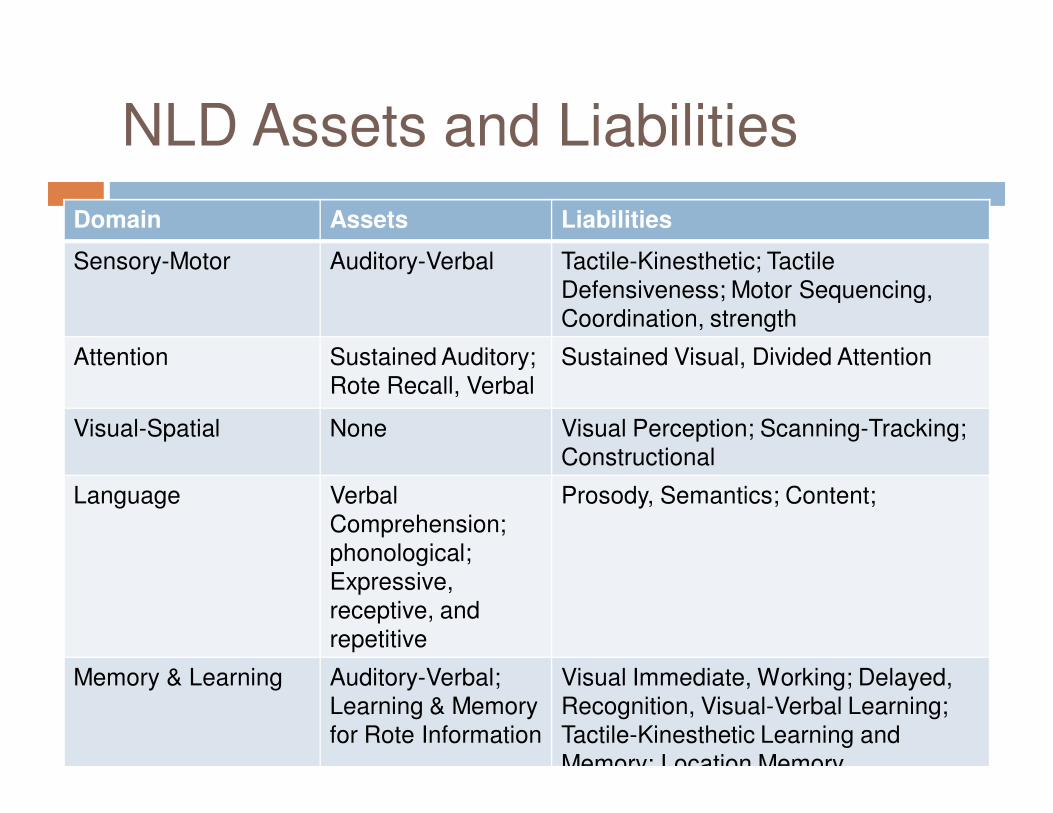
NLD Assets and Liabilities
Domain Assets Liabilities
Sensory-Motor Auditory-Verbal Tactile-Kinesthetic; Tactile
Defensiveness; Motor Sequencing,
Coordination, strength
Attention Sustained Auditory;
Rote Recall, Verbal
Sustained Visual, Divided Attention
Visual-Spatial None Visual Perception; Scanning-Tracking;
Constructional
Language Verbal
Comprehension;
phonological;
Expressive,
receptive, and
repetitive
Prosody, Semantics; Content;
Memory & Learning Auditory-Verbal;
Learning & Memory
for Rote Information
Visual Immediate, Working; Delayed,
Recognition, Visual-Verbal Learning;
Tactile-Kinesthetic Learning and
Memory; Location Memory
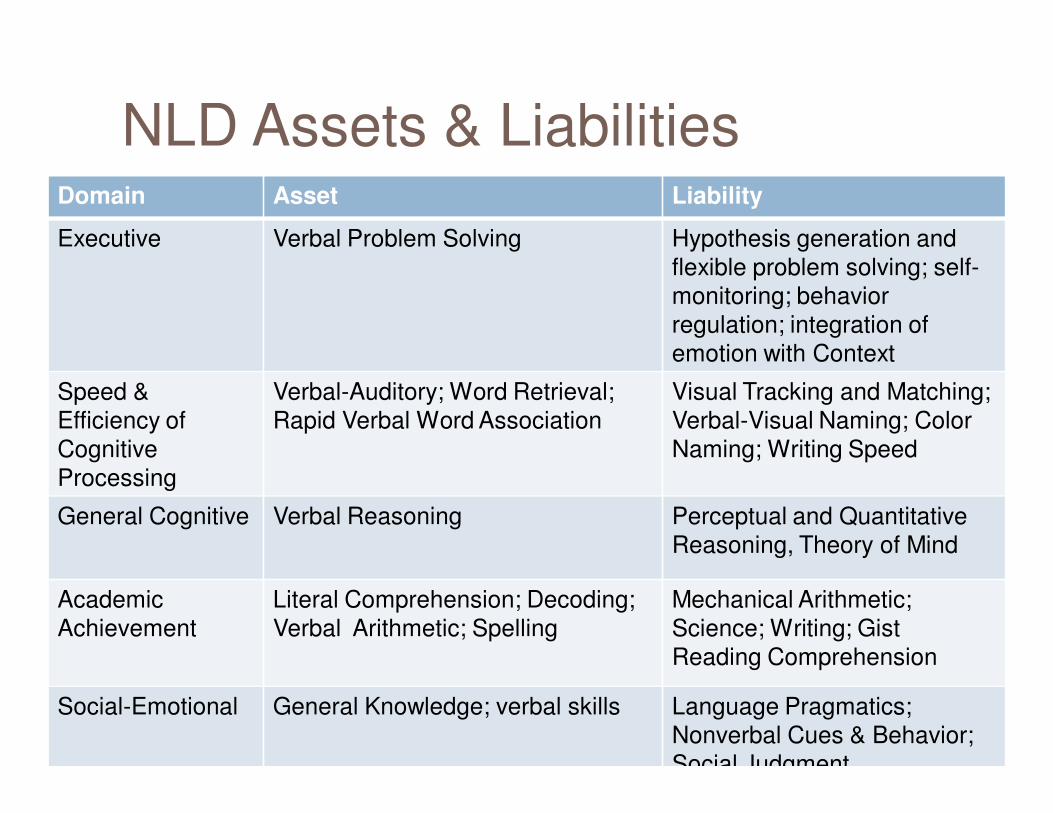
NLD Assets & LiabilitiesDomain Asset Liability
Executive Verbal Problem Solving Hypothesis generation and
flexible problem solving; self-
monitoring; behavior
regulation; integration of
emotion with Context
Speed &
Efficiency of
Cognitive
Processing
Verbal-Auditory; Word Retrieval;
Rapid Verbal Word Association
Visual Tracking and Matching;
Verbal-Visual Naming; Color
Naming; Writing Speed
General Cognitive Verbal Reasoning Perceptual and Quantitative
Reasoning, Theory of Mind
Academic
Achievement
Literal Comprehension; Decoding;
Verbal Arithmetic; Spelling
Mechanical Arithmetic;
Science; Writing; Gist
Reading Comprehension
Social-Emotional General Knowledge; verbal skills Language Pragmatics;
Nonverbal Cues & Behavior;
Social Judgment
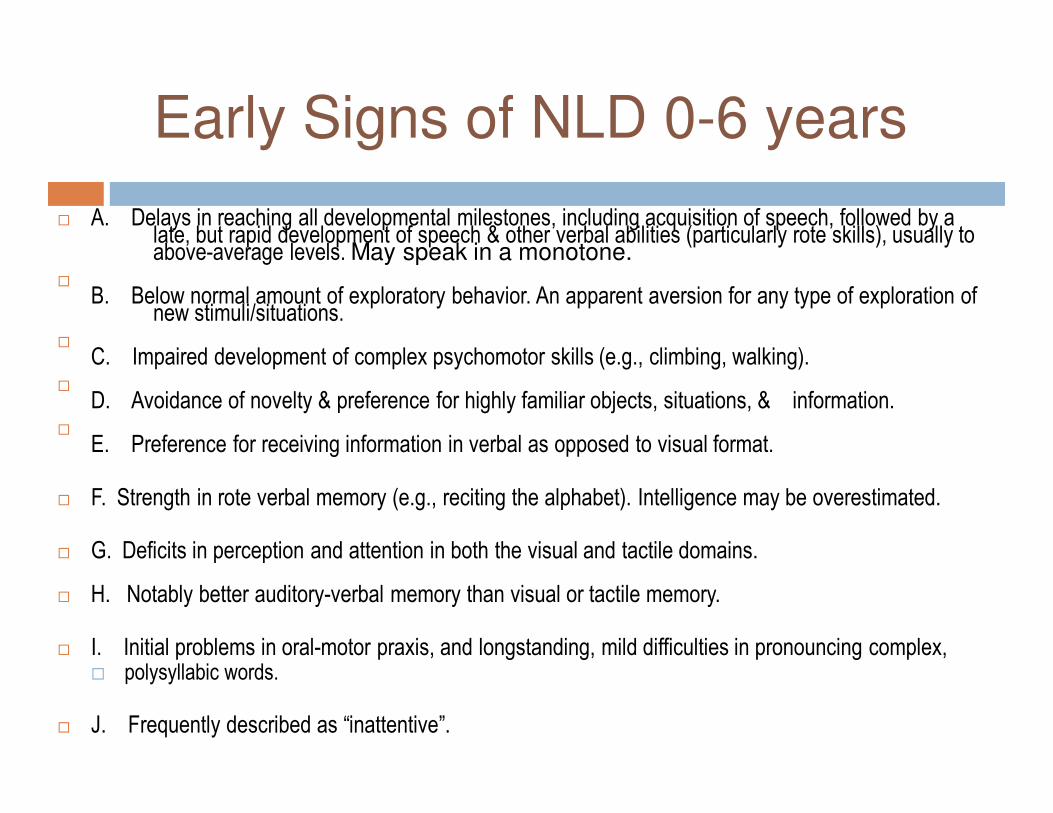
Early Signs of NLD 0-6 years
� A. Delays in reaching all developmental milestones, including acquisition of speech, followed by a late, but rapid development of speech & other verbal abilities (particularly rote skills), usually to above-average levels. May speak in a monotone.
�
B. Below normal amount of exploratory behavior. An apparent aversion for any type of exploration of new stimuli/situations.
�
C. Impaired development of complex psychomotor skills (e.g., climbing, walking).�
D. Avoidance of novelty & preference for highly familiar objects, situations, & information.�
E. Preference for receiving information in verbal as opposed to visual format.
� F. Strength in rote verbal memory (e.g., reciting the alphabet). Intelligence may be overestimated.
� G. Deficits in perception and attention in both the visual and tactile domains.
� H. Notably better auditory-verbal memory than visual or tactile memory.
� I. Initial problems in oral-motor praxis, and longstanding, mild difficulties in pronouncing complex, � polysyllabic words.
� J. Frequently described as “inattentive”.
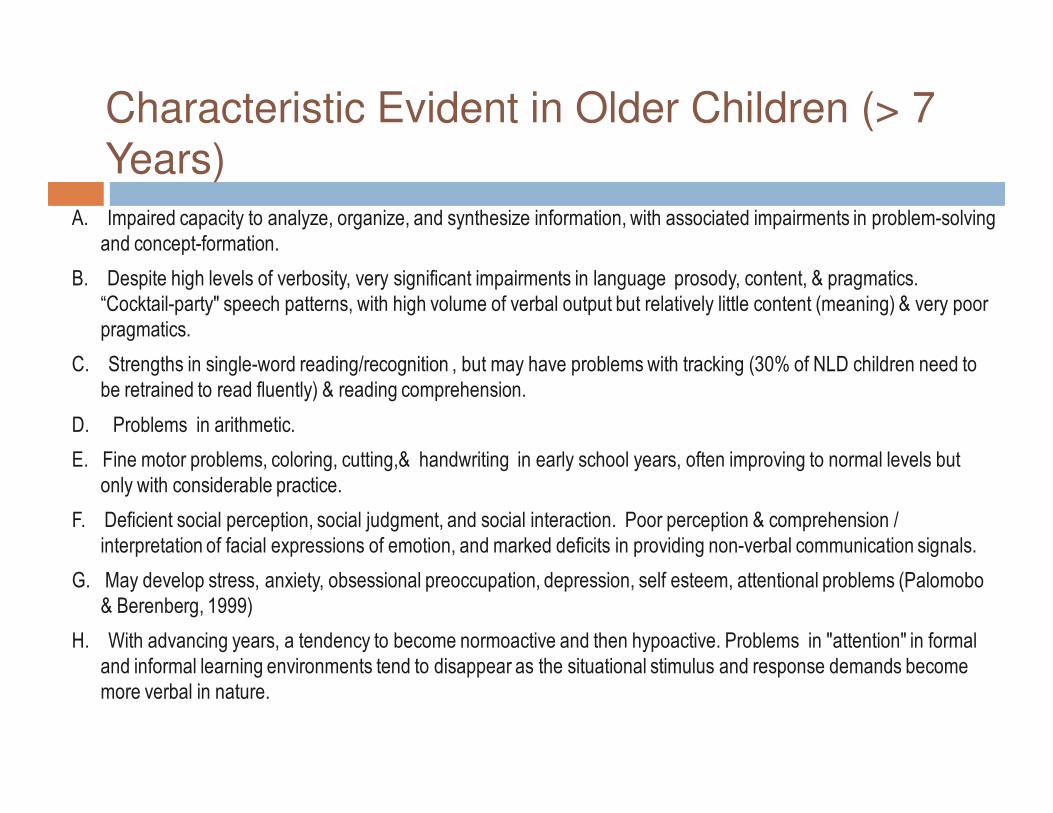
Characteristic Evident in Older Children (> 7
Years)
A. Impaired capacity to analyze, organize, and synthesize information, with associated impairments in problem-solving
and concept-formation.
B. Despite high levels of verbosity, very significant impairments in language prosody, content, & pragmatics.
“Cocktail-party" speech patterns, with high volume of verbal output but relatively little content (meaning) & very poor
pragmatics.
C. Strengths in single-word reading/recognition , but may have problems with tracking (30% of NLD children need to
be retrained to read fluently) & reading comprehension.
D. Problems in arithmetic.
E. Fine motor problems, coloring, cutting,& handwriting in early school years, often improving to normal levels but
only with considerable practice.
F. Deficient social perception, social judgment, and social interaction. Poor perception & comprehension /
interpretation of facial expressions of emotion, and marked deficits in providing non-verbal communication signals.
G. May develop stress, anxiety, obsessional preoccupation, depression, self esteem, attentional problems (Palomobo
& Berenberg, 1999)
H. With advancing years, a tendency to become normoactive and then hypoactive. Problems in "attention" in formal
and informal learning environments tend to disappear as the situational stimulus and response demands become
more verbal in nature.
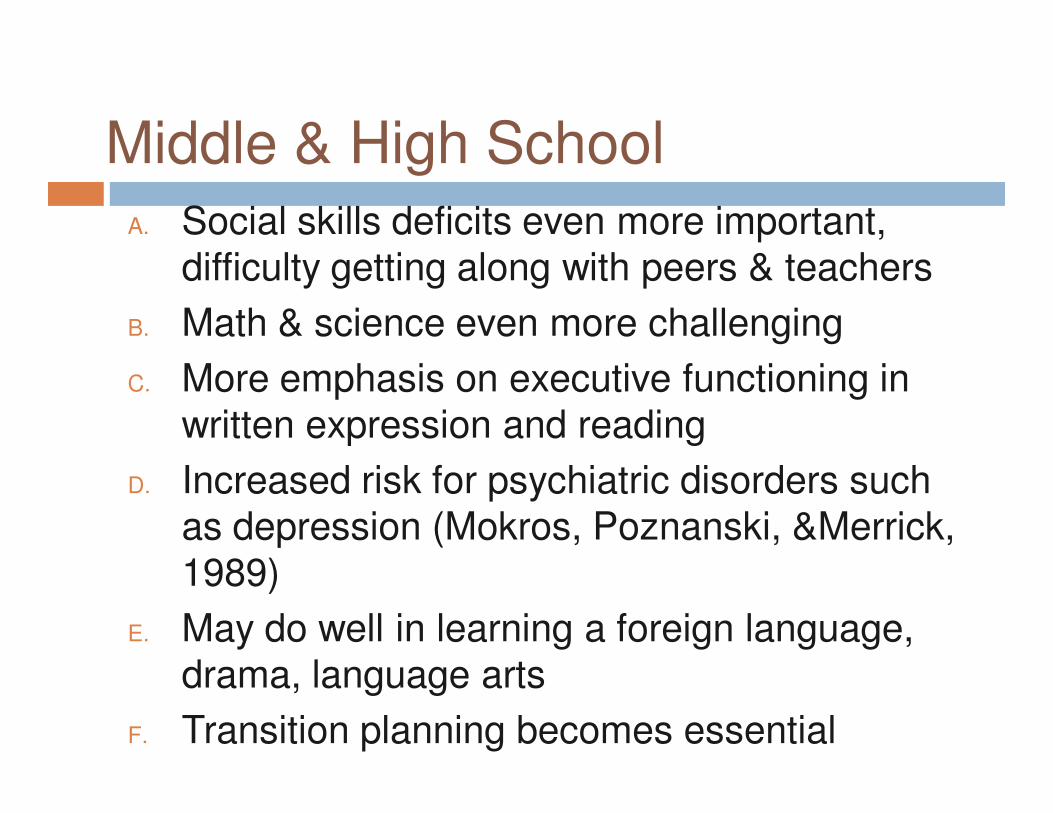
Middle & High School
A. Social skills deficits even more important, difficulty getting along with peers & teachers
B. Math & science even more challenging
C. More emphasis on executive functioning in written expression and reading
D. Increased risk for psychiatric disorders such as depression (Mokros, Poznanski, &Merrick, 1989)
E. May do well in learning a foreign language, drama, language arts
F. Transition planning becomes essential
Etiology
� NLD is the phenotype that may be due to various causes
� Hydrocephalus
� Agenesis of the Corpus callosum
� Turner’s Syndrome
� Fragile X
� Asperger’s Syndrome
� Williams Syndrome – similar strengths & weaknesses (Don,Schellenberg, &
Rourke, 1999) = WS lower cognitive
� Neurofibromatosis
� Velo-cardio-facial syndrome 22p-11q deletion (Lepach, A. C. & Peterman, F.
2011).
� leukomalacia
� spina bifida
Etiology
� Rourke presumed ‘right hemisphere’ dysfunction largely secondary to sub-cortical white matter differences and more association cortex
� Findings from existing neurological cases does suggest involvement of the right hemisphere and possibly of white matter (Voeller, 1995).
� Further study is needed to determine the validity of the right hemispheric white matter hypothesis in NLD.
Etiology
� Filley, 2001
� “the NLD syndrome remains a theoretical construct, and there is little documentation of right hemisphere damage in white (or gray) matter in children with this disability” (p. 262).
� “the relevance of the NLD syndrome to the behavioral neurology of white matter must remain conjectural” (p. 204).
� “careful correlation with neuroradiologic or neuropathologic data [is necessary] . . . to confirm or deny that white matter pathology is in fact present” (p. 262).
Etiology
� Semrud-Clikeman &Fine (2011) found greater number of cysts
on MRIs in children with NLD as compared to children with AS
& controls
� ¼ (7) of NLD had cysts or lesions, generally in the posterior
region--occipital/cerebellar or parietal regions (visual spatial
perception), equally in the right and left hemispheres and
bilateral in the cerebellum.
� Not found as frequently in children with Asperger’s syndrome or
with controls.
� One child w/Turner syndrome in the sample did not have a
cyst/lesion.
� May be a structural abnormality or a genetic disorder that
underlies the expression of nonverbal learning disability.
Asperger’s Syndrome
History
� Described in 1944 by a Viennese pediatrician, Hans Asperger (1906-1980), Asperger Syndrome (AS) “autistic psychopathy”
� Asperger identified a special group of children (4 boys aged 6 to 11) with normal cognitive & linguistic development, but poor social skills
� Impairment in nonverbal communication, vague facial expressions, limited gestures, limited, exaggerated or inappropriate language
� Verbal communication idiosyncratic, precise quality
� Misunderstanding of humor
� Intellectualization of affect
� Clumsiness & poor body awareness
� Special interests
� Conduct problems
� Familial patterns
� Gender patterns (more males)
� Increased anxiety & fear
Lorna Wing, MD
� British psychiatrist� Coined the term “Asperger’s syndrome” &
proposed formal diagnostic criteria� 1979 conducted an epidemiological study in
London�Triad of Impairments:
� Impairment of social interaction� Impairment of social communication
� Impairment of social imagination, flexible
thinking and imaginative play
DSM-IV-TR Diagnostic Criteria
� 299.80 Asperger’s Disorder� A. Qualitative impairment in social interaction, as manifested by at
least two of the following:
� 1. marked impairment in the use of multiple nonverbal behaviors such as eye-to-eye gaze, facial expression, body posture, and gestures to regulate social interaction
� 2. failure to develop peer relationships appropriate to developmental level
� 3. lack of spontaneous seeking to share enjoyment, interests, or achievements with other people
� 4. lack of social or emotional reciprocity
Diagnostic Criteria Continued…
� B. Restricted repetitive and stereotyped patterns of behavior, interests, and activities, as manifested by at least one of the following:
� 1. encompassing preoccupation with one or more stereotyped and restricted patterns of interest that is abnormal either in intensity or focus
� 2. apparently inflexible adherence to specific, nonfunctional routines or rituals
� 3. stereotyped and repetitive motor mannerisms
� 4. persistent preoccupation with parts of objects
Diagnostic Criteria
�C. The disturbance causes clinically significant impairment in social, occupational, or other important areas of functioning.
�D. No clinically significant general delay in language.
�E. No clinically significant delay in cognitive development or in the development of age appropriate self-help skills, adaptive behavior (other than in social interaction), and curiosity about the environment in childhood.
�F. Criteria are not met for another specific Pervasive Developmental Disorder or Schizophrenia.
AS - Social Impairments
May not like physical contact
Inability to engage in appropriate play
Extremely egocentric; self-
centered
Socially awkward Failure to develop developmentally appropriate peer
relationships
Lack of spontaneously
seeking enjoyment
Limited desire for social contact
Difficulty understanding other people’s expressions &
feelings
AS - Motor Impairments
Odd Motor Mannerisms
Delayed Acquisition of Motor Skills
Poor Manipulative
skills
Impaired mirror-image
imitation
Poor Coordination & Balance
AS - Sensory Impairments
Sensitivity to Pain and
Temperature
Sensitivity to taste and
texture of food
Tactile Sensitivity
Visual Sensitivity to
Certain Colors
Sound sensitivity- 3 types of noises:
• 1. sudden, unexpected noise (telephone ringing, dog barking, clicking of a pen)
• 2. high pitched, continuous noise (hair dryer, vacuum cleaner, mix-master)
• 3. confusing, multiple sounds (shopping centers, large classrooms)
Synaesthesia
• A sensation in one sensory system and as a result experiences a sensation in another modality• “Colored hearing” – seeing colors
when hearing a sound
AS – Language Impairments
Adult like speech/’little professors
May have no language delay; Well developed
speech but poor communication
Poor prosody, monotone, strange intonation, rate (too
fast), volume (too loud), poor fluency.
Poor ability to initiate and sustain
conversation with peers
Monologue type speech; egocentric
conversational style
Difficulty understanding metaphors/idioms/jokes
Lack of tact Echolalia
Emotional Co-morbidities
DepressionADHD
ODD Bipolar
Eating Disorders
Substance Use
Anxiety
(GAD, PTSD, Social Phobias, Phobias,
OCD, PTSD
Other Co-morbidities
Seizure
Disorders
Tourette’s
& Tics
Learning Disabilities
Developmental Coordination
DisorderHyperlexia
Other Characteristics
Rigidity in rituals & routines
Above Average Rote Memory
Executive Function Deficits
Intense Interest in circumscribed
subjects
� Nonverbal Learning Disability & Asperger’s Syndrome
NLD & AS
� NLD profile is often associated with AS (@80%), but AS is not always associated with NLD
� Individuals with AS present with virtually all characteristics of NLD (Rourke, 2000)
� Most children with AS have a NLD profile, but not all children
with NLD have AS
� Both NLD & AS have problems with social communication, and
reciprocity, nonverbal communication, pragmatic language,
and visual-spatial skills (Gunter, Ghaziuddin, & Ellis, 2002;
Voeller, 1995).
� Stronger verbal compared to performance skills on cognitive
testing were found for children with AS or NLD (Gillberg &
Billstedt, 2000; Klin et al., 1995).
NLD & AS
� Pennington (1991) –Rourke took 2 different groups & conflated them �1 group problems with spatial cognition�1 group problem with social emotional�only first group should be called NLD�Second group should be on autistic spectrum�Pennington (2009)reviewed NLD again
� “in sum, we do not have sufficient evidence to accept it as a valid learning disorder apart from either autism spectrum disorder (ASD), mathematics disorder (MD) or developmental coordination disorder (DCD) all of which are covered in the DSM-IV-TR (ASD in the category of PDDs)” (p. 248).
NLD vs. AS
� Palumbo (2001)- hypothesized that AS & NLD
could be 2 different subtypes of the same
syndrome
� Children with Asperger’s Syndrome have more
profound social difficulties than children with
developmental NLD (Thompson 1997).
� NLD & AS could be on a continuum of severity
ranging from NLD to Asperger’s and finally
autism (Roman, 1998)
NLD & AS (Klin, Sparrow,
Cicchetti, & Rourke, 1995).
� NLD & AD profiles share many characteristics
� Strong verbal skills
� Poor visual spatial ability
� Problems with executive functioning.
� NLD is evident in many with AS, but not in HFA
� The NLD profile is “an adequate model of neuropsychological assets and deficits encountered in individuals with AS (p. 1133)
� AS is one of several pathways including hydrocephalus, acquired brain injury and Williams Syndrome to the manifestation of NLD
NLD vs. AS
� Children with Asperger’s Syndrome typically
have “restricted interests,” where they
become obsessed with unusual interests
(Stein, Klin, & Miller 2004,
� The presence of stereotyped and restricted
patterns of interest and the need to adhere
to routines present in children with AS but
not NLD (Semrud-Clikeman, 2007).
NLD vs. AS
� Semrud-Clikeman, Walkowiak, Wilkinson, & Minne, 2010
� Compared 24 NLD, 52 AS, 27 ADHD 9- to 15-year-old children
� Found no significant differences in social perception between
the NLD & AS groups (both lower than controls)
� Differences between AS & NLD groups on calculations
� Differences on the Autism Diagnostic Interview–Revised,
particularly in the area of stereotyped and restricted behaviors.
� No significant difference for AS & NLD on Rey-Ostereith
Complex Figure test. Both lower than norms
NLD, AS & ADHD
� Semrud-Clikeman, Walkowiak, Wilkinson, & Christopher, 2010
� Compared NLD, AS, & ADHD-C & ADHD – PI
NLD & AS – No significant
differences
� Semi-structured interview (SIDAC)
� Behavioral Measures –BASC-2 Hyperactivity& Attention
� Social Skills – (SSRS)
� Math calculations
� Mathematics reasoning
� Reading recognition
� Fluid Reasoning (WJCOG-III) (Concept formation & Analysis & Synthesis)
� Motor Skills (Grooved Pegboard)
NLD & AS
� Visual-Spatial – NLD group significantly lower on
VMI than AS (Rey-Osterreith)
� Judgment of Line Orientation test (JLO) –NLD
lower than AS
� AS screener – AS group scored higher
� WASI –
� PIQ –NLD lower than AS
� VIQ - no significant difference among groups
� NLD group showing the largest split between VIQ & PIQ
NLD, AS, & ADHD
� 74% of NLDs had a V > P split of more than 15 SS points & 40% had a split of 25 SS points or higher (15-55)
� 63% of AS group had BIQ &PIQs within 15pts.
� But 37% of AS showed VIQ >PIQ in the AS group.
� While children with NLD are more likely to show a VIQ > PIQ split; there is a sizable minority of children who do not.
� Finding is not sufficient to provide a distinction between NLD & AS
� also found in Pelletier, Ahmad, & Rourke, 2001).
NLD vs. AS
• diagnosed from neuropsychological perspective
• Psychological test scores
• learning disability, discussion of how children learn
NLD
• diagnosed from psychiatric perspective
• observations
• developmental disorderAsperger’s
Prevalence
� .1 – 1%
� 10% (Ozols & Rourke, 1991
� 25% (Bender & Golden, 1990
� 29% (Van der Vluat, 1989)� Higher or equal rates in
females
� 1:1
� Recognized in 4th & 5th
grades
� 1-10 in 10,000
� Higher rates in Males
� Recognized around 3-4 yrs. of age
NLD AS
Neuropsychological
� VIQ > PIQ
� Weak visuospatial skills,
� Visual motor integration
� Right left confusion� Visual memory
deficits� Attentional problems� Hyperactivity as
child)
� May have Theory of Mind deficits
� VIQ>PIQ (X = 23.8 pts.) Ghaziuddin & Mountain-Kimchi (2004) found that only 82% of their AS group had VIQ > PIQ
� Weak visuospatial skills
� Visual motor integration
� Visual-spatial perception
� Nonverbal concept formation
� Visual memory deficits
� Attentional problems
� More likely to have Theory of Mind deficits
NLD AS
Visual Motor
� NLD� Psychomotor coordination
problems
� Clumsy, poor at sports
� Delayed Gross Motor Milestones
� Fine Motor difficulties, drawing, handwriting (Frankenberger, 2005)
� Avoidance of graphomotor tasks
� Difficulties dressing, problems with fasteners
� Poor organizational skills
� May not learn from diagrams, need verbal explanations (Fast, 2004)
� AS� Psychomotor
coordination problems
� Clumsy
� Fine and Gross Motor delays (Tantam, 1988; Gillberg,
1990)
� Stereotypic motor mannerisms (Mamen, 2007)
� Do not have visual issues & may be visual learners (Fast, 2004)
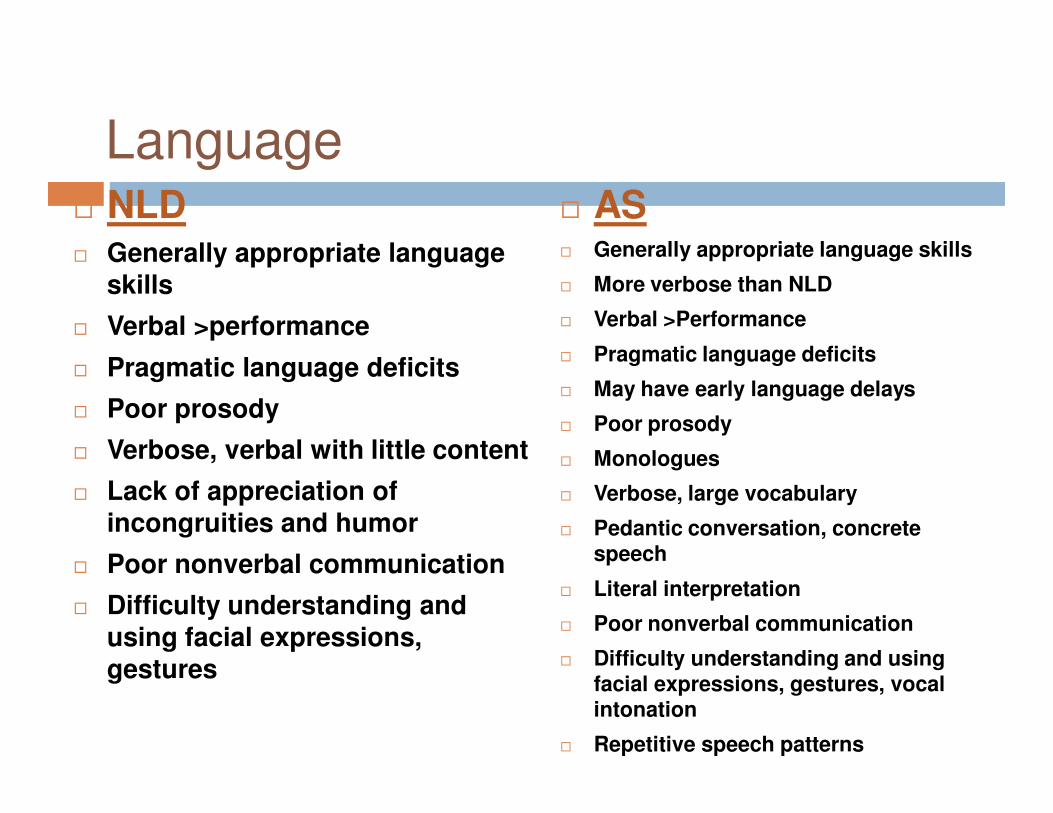
Language� NLD� Generally appropriate language
skills
� Verbal >performance
� Pragmatic language deficits
� Poor prosody
� Verbose, verbal with little content
� Lack of appreciation of incongruities and humor
� Poor nonverbal communication
� Difficulty understanding and using facial expressions, gestures
� AS� Generally appropriate language skills
� More verbose than NLD
� Verbal >Performance
� Pragmatic language deficits
� May have early language delays
� Poor prosody
� Monologues
� Verbose, large vocabulary
� Pedantic conversation, concrete speech
� Literal interpretation
� Poor nonverbal communication
� Difficulty understanding and using facial expressions, gestures, vocal intonation
� Repetitive speech patterns
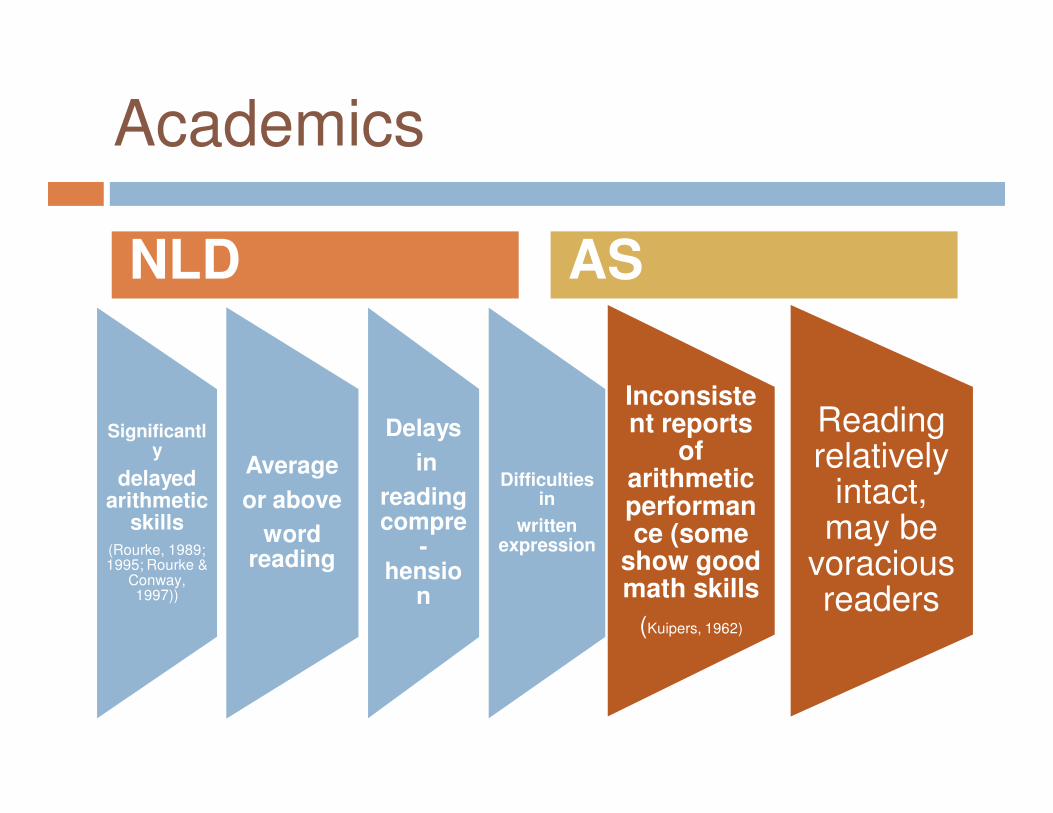
Academics
Significantly
delayed arithmetic
skills (Rourke, 1989; 1995; Rourke &
Conway, 1997))
Average
or above
word reading
Delays
in
reading compre
-hensio
n
Difficulties in
written expression
Inconsistent reports
of arithmetic performance (some
show good math skills
(Kuipers, 1962)
Reading relatively
intact, may be
voracious readers
NLD AS
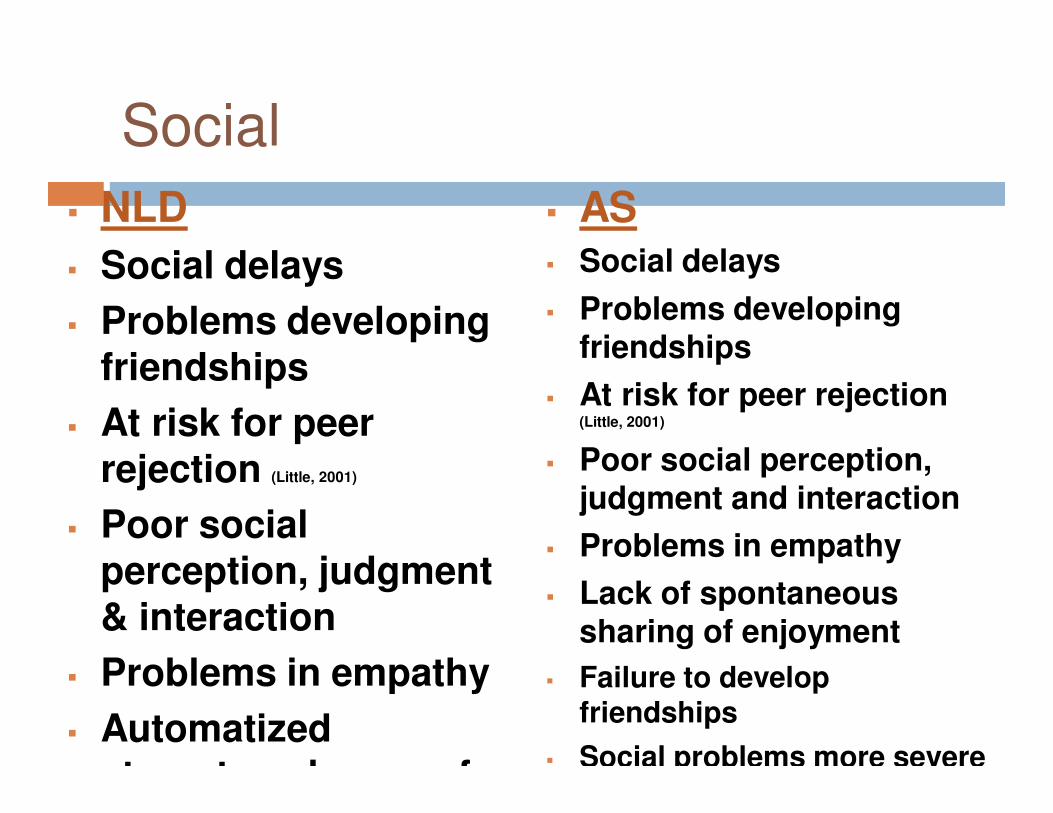
Social
� NLD
� Social delays
� Problems developing friendships
� At risk for peer rejection (Little, 2001)
� Poor social perception, judgment & interaction
� Problems in empathy
� Automatized stereotyped ways of
� AS� Social delays
� Problems developing friendships
� At risk for peer rejection (Little, 2001)
� Poor social perception, judgment and interaction
� Problems in empathy
� Lack of spontaneous sharing of enjoyment
� Failure to develop friendships
� Social problems more severe
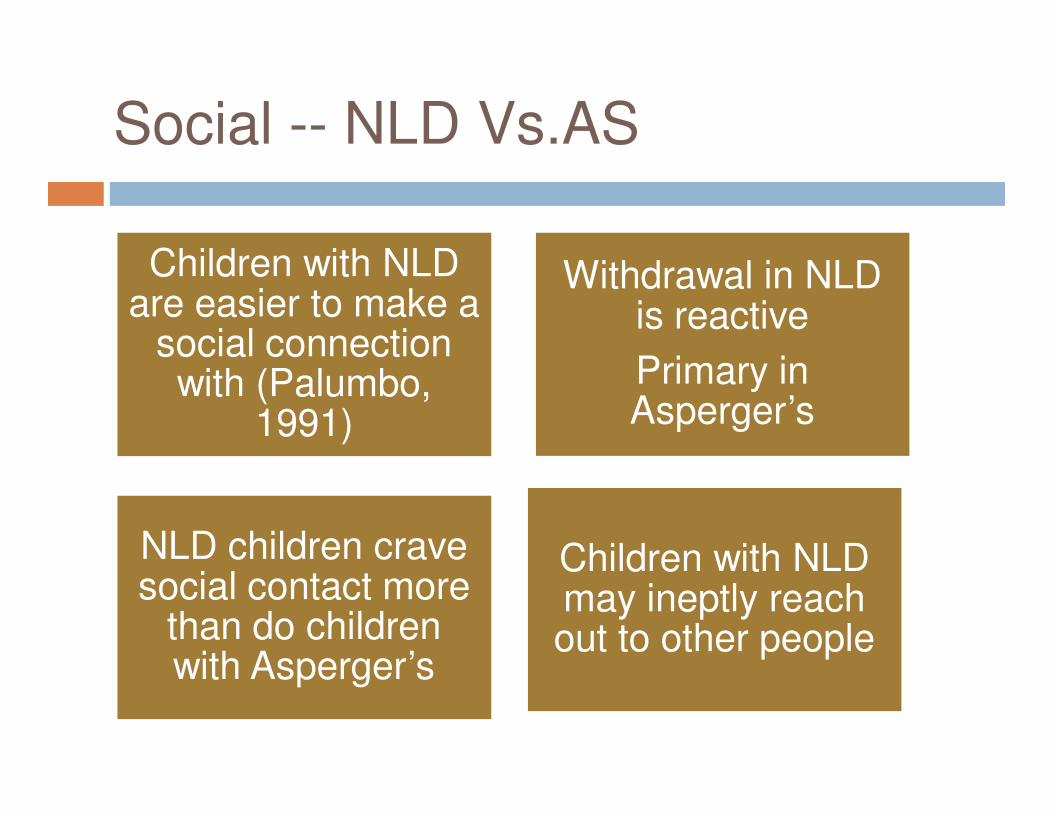
Social -- NLD Vs.AS
Children with NLD are easier to make a
social connection with (Palumbo,
1991)
Withdrawal in NLD is reactive
Primary in Asperger’s
NLD children crave social contact more
than do children with Asperger’s
Children with NLD may ineptly reach out to other people
Emotional
� Emotional problems (internalizing anxiety & depression) ( Petti, Voelker, Shore &
Hayman-Abello, 2003)
� MMPI - NLD group had no scores above 70 on clinical scales, (Waldo et al., 1999)
� High risk for suicide ( Bigler,
1989; Fletcher, 1989; Rourke, Young, & Lennars, 1989)
� Have normal emotions, but can’t express them or recognizing them in others (Fast, 2004)
� Anxiety (esp. in adolescence) (Klin, 2004)
� Potential of mood disorders is high ( Ellis, Ellis, Fraser,
& Deb, 1994; Gujikawa, Kobayashi, Koga, & Murata, 1987)
� MMPI -2 study with adults elevations on L and Depression, social introversion, social discomfort (Ozonoff, Garcia, Clark &
Lainhart,2005)
� Have flatter affects (Fast, 2004)
NLD AS
Repetitive Behaviors
Inability to Adapt to Change
Inability to adapt to change/novelty
Preoccupation with stereotyped and
established routines
Ritualistic
Focus on special interest
Amass factual information
NLD AS
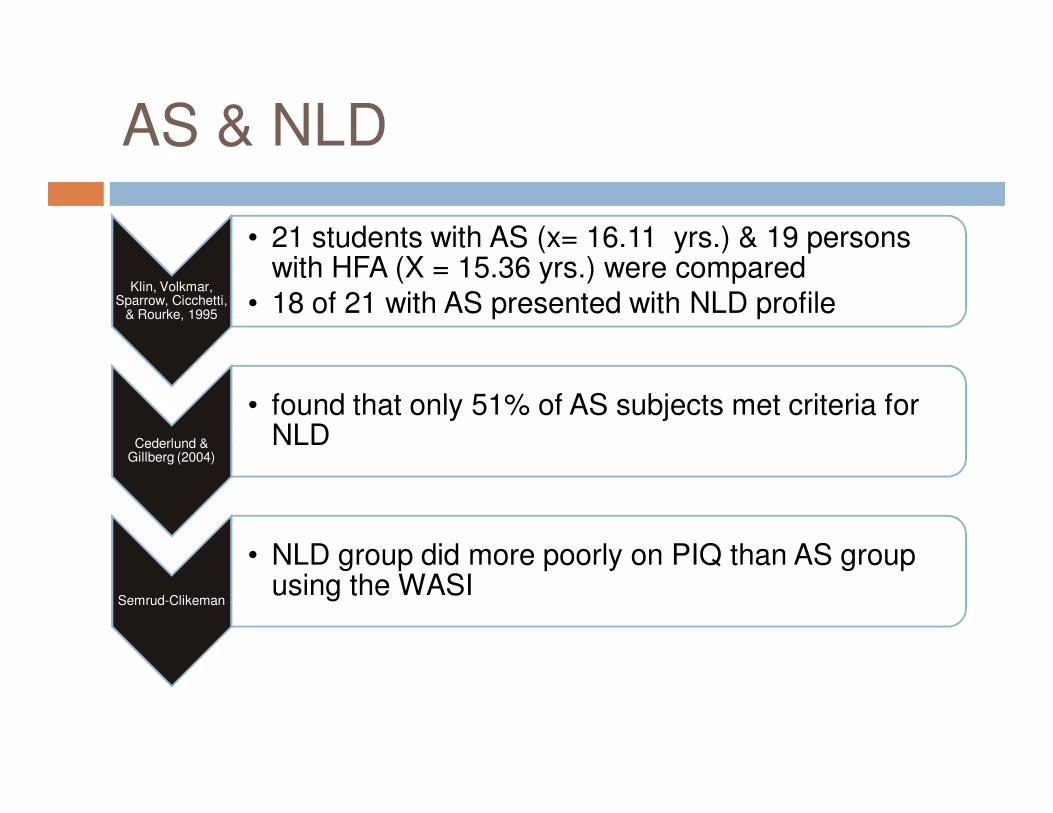
AS & NLD
Klin, Volkmar, Sparrow, Cicchetti,
& Rourke, 1995
• 21 students with AS (x= 16.11 yrs.) & 19 persons with HFA (X = 15.36 yrs.) were compared
• 18 of 21 with AS presented with NLD profile
Cederlund & Gillberg (2004)
• found that only 51% of AS subjects met criteria for NLD
Semrud-Clikeman
• NLD group did more poorly on PIQ than AS group using the WASI
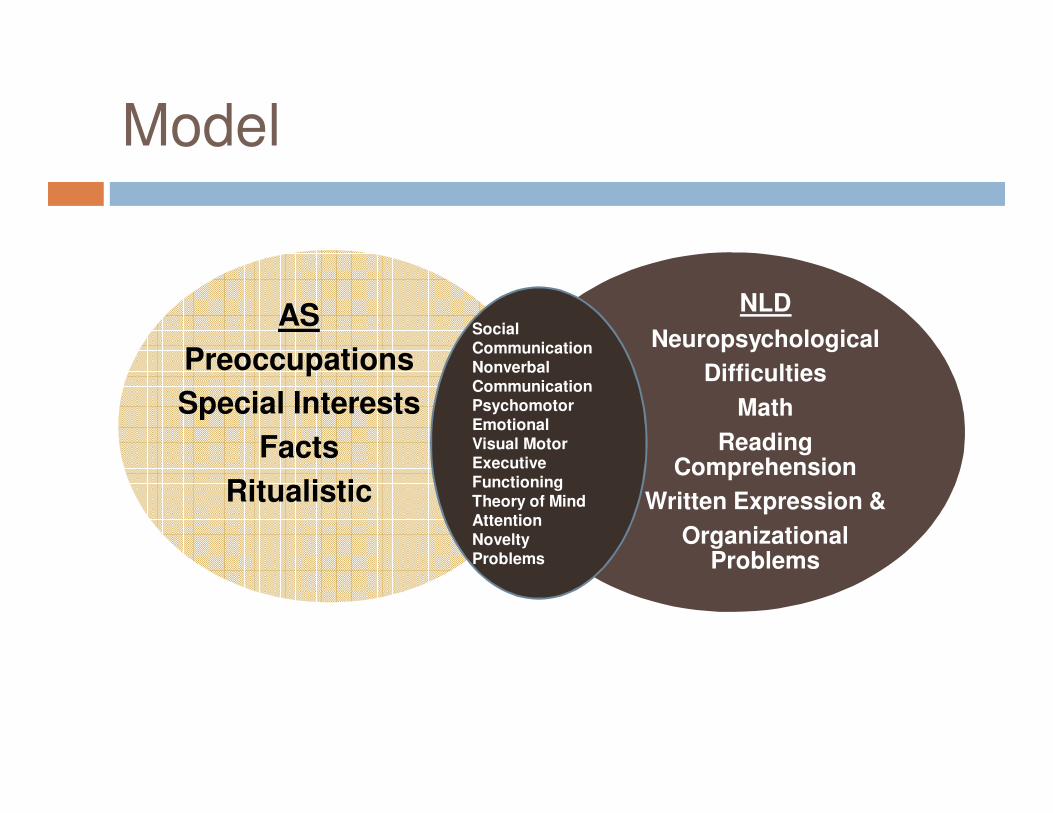
Model
AS
Preoccupations
Special Interests
Facts
Ritualistic
NLD
Neuropsychological
Difficulties
Math
Reading Comprehension
Written Expression &
Organizational Problems
SocialCommunicationNonverbal CommunicationPsychomotorEmotionalVisual Motor Executive FunctioningTheory of MindAttentionNovelty Problems
Assessment
� Cognitive Assessment
� Thinking &reasoning skills must be at least average
� Although IQ does not have to be average (e.g., average WJIII
Thinking ability or Cognitive Efficiency)
� There must be an impairment in at least one psychological
process related to learning
Neuropsychological
Assessment
� Impairment in at least one psychological process related to learning
� Visual/motor/spatial/tactile memory and attention
� Visual motor or fine motor processing
� Speed
� Pragmatic language
� Executive functioning (e.g., planning, monitoring, selective focusing, organization
Possible Assessment Measures
� WISC-IV
� Woodcock-Johnson Cognitive Battery III (WJ-Cog III) (Woodcock, McGrew, & Mather,2001a) – esp. Analysis & Synthesis & Concept Formation)
� KABC-2(Chow & Skuy, 1999) found that NLD children showed significantly higher successive than simultaneous processing
� WASI
Possible Assessment Measures
� NEPSY (e.g., Design copying, Arrows)
� Delis-Kaplan Visual Motor Integration
(Beery)
� Wisconsin Card Sort (Jing, Wang, Yang, &
Chen, 2004)
� Category Test (Strang & Rourke, 1983)
� The Children’s Category Test (Boll, 1993)
Ris et al. (2007) - good predictor of the NLD
group (Ris et al., 2007)
Possible Assessment
Instruments
� Rey-Osterreith Complex Figure (Osterreith,
1944)
� Grooved Pegboard (Klove, 1963).
� Finger Tapping Test (Reitan & Wolfson, 1985).
� Purdue Pegboard
� Judgment of Line Orientation (JLO) (Benton,
Sivan, Hamsher, Varney, & Spreen, 2004)-
(Semrud-Clikeman, yes, not Benton, Varney, &
Hamsher, 1978)
� VMI (Beery et al., 2006).
Possible Assessment
Instruments
� Children’s Auditory Verbal Learning Test – 2 (CAVLT-2)
� Children’s Memory Scale
Possible Assessment
Instruments� AS Screener (AS screener based on DSM-IV-TR Asperger syndrome criteria)
� ADI-R
� Asperger Syndrome Diagnostic Scale (ASDS)
� Autism Spectrum Rating Scales (ASRS)
� The Structured Interview for Diagnostic Assessment of Children (SIDAC) (Puig-
Antich & Chambers, 1978). (K-SADS)
� Behavior Assessment System for Children–2 (BASC–2) (Reynolds & Kamphaus,
2004).
� Social Skills Rating Scale (SSRS) (Gresham & Elliott, 1990)/SSIS
� Child and Adolescent Social Perception (1995) (Semrud-Clikeman & Glass,2008)
� CBCL
� Conners Parent/Teacher Rating Scales
� Behavior Rating Inventory of Executive Function (BRIEF)
� Children’s Depression Inventory
� NLD scale http://www.nldline.com/
Possible Assessment
Instruments
� WJ-Ach III (Woodcock et al., 2001b) Math calculations &
� Math reasoning (Forrest, 2004) didn’t find that poor
mathematical reasoning predicted NLD
� WIAT-III
� Key Math
� Gray Oral Reading-4
Is NLD a Valid Diagnosis?
� Spreen (2011) NLD remains a hypothesis, but it should not be used in clinical practice unless it is supported by solid research findings.
Selected References
Bloom, E., & Heath, N. (2010). Recognition, expression, and understanding facial expressions of emotion in adolescents with nonverbal and general learning disabilities. Journal of Learning Disabilities, 43, 180– 192.
Dehaene,S., & Cohen., L. (1997).Cerebral pathways for calculation double dissociation between
rote verbal and quantitative knowledge of arithmetic. Cortex, 33, 219-250.Davis, & Broitman, J. (2010). Nonverbal Learning disabilities in children. New York: Springer
DOI 10.1007/978-1-4419-8213-1Drummond, C., Ahmad, S., & Rourke, B. (2005). Rules for the classification of younger children
with Nonverbal Learning Disabilities and Basic Phonological Processing Disabilities. Archives of Clinical Neuropsychology, 20, 171-182.
Fast, Y. ( 2004). Individuals with Asperger’s syndrome or nonverbal learning disability: Stories and strategies. London: Jessica Kingsley Pub.
Filley, C. M. (2001). The behavioral neurology of white matter. New York, NY: Oxford.
Fisher, N. J., DeLuca, J. W., & Rourke, B. P. (1997). Wisconsin Card Sorting Test and Halstead Category Test performances of children and adolescents who exhibit the syndrome of Nonverbal Learning Disabilities. Child Neuropsychology, 3, 61-70.
Foss, J. (1991). Nonverbal learning disabilities and remedial interventions. Annals of Dyslexia, 41, 128-140.
Geary, D.C.(2000). From infancy to adulthood: The development of numeric abilities. European Child and Adolescent Psychiatry, 9, 11-16.
Ghaziuddin, M. & Mountain-Kimchi, K. (2004). Defining the intellectual profile of Asperger syndrome: Comparison with high functioning autism. Journal of Autism and Developmental Disorders, 34, 279-284.
Gilberg, C.(1989).Autism and Asperger Syndrome. Cambridge: Cambridge University Press.
Selected References
Hain, & Hale, J. B. (2010).”Nonverbal” learning disabilities or Asperger’s Syndrome? Clarification through cognitive hypothesis testing. (pp. 372-387). In N. Mather & L. Jaffe (Eds.) Comprehensive Evaluations: Case Reports for Psychologists, Diagnosticians. Hoboken, NJ.
Hale, J..B. & Fiorello, C.A.(2004). School neuropsychology. New York: Guilford Press.
Humphries, T., Cardy, J., Worling, D., & Peets, K. (2004). Narrative comprehension and retelling abilities
of children
with nonverbal learning disabilities. Brain & Cognition, 56, 77-88,.
Jing, J. Wang, Q., Yang, B., & Chen, X. (2004). Neuropsychological characteristics of selective attention in
children
with nonverbal learning disabilities. Journal of Chinese Medicine, 117, 1834-7.
Klin, A., Volkmar, F., Sparrow, S., Cicchetti, D., & Rourke, B.(1995). Validity and neuropsychological
characterization of Asperger syndrome.: Convergence with nonverbal learning disabilities. Journal of Child Psychology and Psychiatry, 36, 1127-1140.
Klin, A., Volkmar, F., & Sparrow, S. (Eds.) (2000). Asperger Syndrome. New York: Guilford Press.
Lepach, A. C. & Peterman, F. (2011). Nonverbal and verbal learning: A comparative study of children and
adolescents with 22q11 deletion syndrome, non-syndromal Nonverbal Learning Disorder and memory
disorder. Neurocase: The Neural Basis of Cognition, 17, 480-490.
DOI:10.1080/13554794.2010.536954
Little, S. (1993). Nonverbal Learning Disabilities and Socioemotional Functioning: A Review of Recent
Literature. Journal of Learning Disabilities, 26, 653-665. doi: 10.1177/002221949302601003
Selected References
Montgomery, J. M., Dyke, D. I., & Schwean, V.L. (Autism spectrum disorders: WISC-IV applications for clinical assessment and intervention in A. Prifitera, D. Saklofske & L.Weiss (Ed.). WISC-IV Clinical Assessment and Intervention (2nd. Ed.) , San Diego, CA: Academic Press, pp. 299-337.
Nicholls, C. (2011). The assessment of “nonverbal” learning disabilities. In N. Mather & L. Jaffe, (Eds.) (pp. 411-420. Comprehensive Evaluations: Case Reports for Psychologists, Diagnosticians. Hoboken, NJ.
Palombo, J. (2001). Learning disorders and disorders of the self in children and adolescents. New York:
W. W. Norton & Co.
Pelletier, P. M., Ahmad, S. A., & Rourke, B. P. (2001). Classification rules for Basic Phonological Processing Disabilities and Nonverbal Learning Disabilities: Formulation and external validity. Child Neuropsychology, 7, 84-98.
Pennington. B. (1991). Diagnosing learning disorders: A neuropsychologi9cal framework. New York: Guilford Press.
Pennington, B. F. (2009). Diagnosing learning disorders: A neuropsychological framework (2nd ed.).New York: Guilford.
Petti, V. L., Voelker, S. L., Shore, D. L., & Hayman-Abello, S. E. (2003). Perception of nonverbal emotion
cues by children with nonverbal learning disabilities: Formulation and external validity. Child Neuropsychology, 7, 84-98.
Ris, D. M., Ammerman, R.T., Waller, N., et al. (2007).Taxonicity of nonverbal learning
Selected References
Rourke, B. P. (1987). Syndrome of nonverbal learning disabilities: The final common
pathway of white-matter disease/dysfunction? The Clinical Neuropsychologist, 1, 209-234.
Rourke, B. P. (1988). The syndrome of nonverbal learning disabilities: Developmental manifestations in neurological disease, disorder, and dysfunction. The Clinical Neuropsychologist, 2, 293-330
Rourke, B. P. (1989). Nonverbal learning disabilities: The syndrome and the model. New York: The Guilford Press.
Rourke, B. P. (1995). Syndrome of nonverbal learning disabilities: Neurodevelpmental manifestations. (Ed.) New York: The Guilford Press..
Rourke, B. P., & Conway, J. A. (1997). Disabilities of arithmetic and mathematical reasoning: Perspectives from neurology and neuropsychology. Journal of Learning Disabilities, 30, 34-46.
Rourke, B. P., & Tsatsanis, K. D. (1996). Syndrome of Nonverbal Learning Disabilities: Psycholinguistic assets and deficits. Topics in Language Disorders, 16, 30-44.
Rourke, B. & Tsatsanis, K. (2000). Nonverbal learning disabilities and Asperger Syndrome in A. Klin, F. Volkmar, & S. Sparrow (Eds.) Asperger Syndrome. New York: Guilford Press. pp. 231-253.
Semrud-Clikeman, M., & Fine, J. (2011). Presence of Cysts on Magnetic Resonance Images (MRIs) in Children with Asperger Disorder and Nonverbal Learning Disabilities. Journal of Child Neurology , 26, 471-475 DOI: 10.1177/0883073810384264
Selected References
� Semrud-Clikeman, M., & Glass, K. L. (2008). Comprehension of humor in children with Nonverbal Learning
Disabilities, Verbal Learning Disabilities and without Learning Disabilities. Annals of Dyslexia, 58, 163–
180. DOI 10.1007/s11881-008-0016-3
Semrud-Clikeman, M. & Hynd, G. (1990). Right hemispheric dysfunction in non-verbal learning disabilities: Social, academic, and adaptive functioning in adults and children. Psychological Bulletin, 107, 196-209
Semrud –Clikeman, M., Walkowiak, J., Wilkinson, A., & Butcher, B. (2010). Executive Functioning in Children with Asperger's Syndrome, ADHD-Combined Type, ADHD-Predominately Inattentive Type, and Controls J ournal of Autism and Developmental Disorders, 40, 1017–1027 DOI 10.1007/s10803-010-0951-9.
Semrud –Clikeman, M., Walkowiak, J., & Wilkinson, A., Christopher, G. (2010). Neuropsychological Differences Among Children With Asperger's Syndrome, Nonverbal Learning Disabilities, Attention Deficit Disorder, and Controls. Developmental Neuropsychology, 35, 582–600. DOI: 10.1080/87565641.2010.494747
Semrud-Clikeman, M., Walkowiak, J., Wilkinson, A., & Minne, E. P. (2010). Direct and indirect measures of social perception, behavior, and emotional functioning in children with Asperger’s disorder, nonverbal learning disability, or ADHD. Journal of Abnormal Child Psychology, 38, 509–519.
Spreen, O. (2011). Nonverbal learning disabilities: A critical review: Child Neuropsychology, 17, 418- 443. DOI: 10.1080/09297049.2010.546778
Selected References
Stein, M. T., Klin, A., Miller, K., Coolman, R., & Snyder, D. M. (2004).When Asperger’s syndrome and
nonverbal learning disability look alike. Developmental and Behavioral Pediatrics, 25, S59–S64.
Stewart, K. Helping a child with nonverbal learning disorder or Asperger’s Syndrome: A parent’s guide.
London: New
Harbinger Publications.
Strang, J. D., & Rourke, B. P. (1983). Concept-formation/nonverbal reasoning abilities of children who exhibit
specific academic problems with arithmetic. Journal of Clinical Child Psychology, 12, 33–39
Strang, J. D., & Rourke, B. (1985). Arithmetic disabled subtypes: The neuropsychological significance of
specific arithmetical impairment in childhood. In B. Rourke (Ed.), Neuropsychology of learning disabilities:
Essentials of subtype analysis (pp. 167–185). New York, NY: Guilford.
Telzrow, F.. & Bonar, A., (2002). Responding to students with nonverbal learning disabilities. Teaching
Exceptional Children, 34, 8-133.
Volkmar, F. & Klin, A. (1998). Asperger syndrome and nonverbal learning disabilities in Schopler et al. (Eds.)
Asperger Syndrome or High-Functioning Autism? New York: Plenum Press. Pp. 107-121.
Williams, D., Goldstein, G., Kojkowski, N., & Minshew , N. (2008). Do individuals with high functioning autism
have the IQ profile associated with nonverbal learning disability? Research in Autism Spectrum
Disorders, 7, 353-361.
Worling, D.D., Humphries, T.,& Tannock, R. (1999). Spatial and emotional aspects of language interfering in
nonverbal learning disabilities. Brain and Language, 70, 220-239.
Yaloff, J. & McGrath, M. (2010). Assessing and intervening with children with Nonverbal learning disabilities.
(pp.579-598) In D. Miller, (ed.) Best Practices inSchool Neuropsychology: Guidelines for effective practice,







