
ESPEN Congress Madrid 2018
Nutrition In Solid Organ Transplant Patients
Obesity In Transplant PatientsM. I. Correia (BR)

Obesity in transplant patients
M.Isabel T. D. Correia, MD, PhD
Brazil

Disclosures
• Abbott
• Baxter
• Danone
• Fresenius
• Nestlé
Outline
• The transplant patient
• Bebore transplantation• Malnutrition
• Obesity
• After transplantation• Weight gain/obesity
• Associated factors
• Complications
• Conclusions– What can be done?
The transplant patient

Outline
• The transplant patient
• Bebore transplantation• Obesity
• Malnutrition
• After transplantation• Weight gain/obesity
• Associated factors
• Complications
• Conclusions– What can be done?

Obesity worldwide


% n

Nutrition 29 (2013) 1252–1258

Nutrition 29 (2013) 1252–1258

Nutrition 29 (2013) 1252–1258

Obesity - preoperatively
• Global estimates of NAFLD approach 25%
– 30% prevalence in the US
• Nonalcoholic steatohepatitis (NASH) is 5%
– 20% of these patients progressing to end stage liver disease
– NASH is projected to become the leading indication for LT
• in the next decade in the United States
Diwan TS et al.
Liver Transpl. 2018 Aug 6

Dietary intake vs nutritional status
• Inadequate
– Alcoholic
– Eating habits
• Anorexia
• Ascitis
• Many restrictions
– Doctors
– Dietitians
– Others
Ribeiro H et al
Nutrition 29 (2013) 1252–1258
Physical Activity vs nutritional status
Outline
• The transplant patient
• Bebore transplantation• Malnutrition
• Obesity
• After transplantation• Weight gain/obesity
• Associated factors
• Complications
• Conclusions– What can be done?

The operation

Obesity – risk factor for surgical
complications

Obesity and surgical complications
• Wound infection
• Wound quality
– Fistula
– Dehiscence
• Thrombosis
• Cardiovascular events
• Pneumonia
• Graft function

Nutritional status - perioperatively
Ribeiro H et al
Submitted, 2018

Nutritional status - perioperatively
Ribeiro H et al
Submitted, 2018

Morbidity after liver transplant
Cardiovascular diseases
• General population• Girman et al. Am J Cardiol 2004; 193: 136-41.
• Kip et al. Circulation 2004; 109: 706-13.
• Post liver transplant population• Laryea et al. Liver Transpl 2007; 13: 1109-14.
Liver injury
• General population• Marceau et al. J Clin Endocrinol Met 2009; 84: 1513-17.
• Marchesini et al. Cur Opin Lipidol 2005; 16: 421–27.
• Post liver transplant population• Hanouneh et al. Liver Transpl 2008; 14: 1287-93.
• Angelico et al. Eur J Gastroenterol Hepatol 2003; 15: 99-102.

Metabolic disorders after liver
transplantation (LTx)
• Obesity: 41%• Stegall et al. Transplantation 1995: 60; 1057-60.
• Diabetes: 38%• Khalili et al. Liver Transpl 2004: 10; 349-55.
• Hypertension: 77%• Neal et al. Transplantation 2004; 77: 93-9.
• Hypertriglyceridemia: 69%• Gisbert et al. Liver Transpl Surg 1997; 3: 416-22.
• Low HDL levels: 52%• Muñoz et al. Transplantation Proc 1991; 23: 1480-3.

Metabolic disorders after liver
transplantation.
Obesity
Hypertension
HDL Triglycerides
InsulinResistance
Laryea et al. Liver Transpl 2007; 13: 1109-14
Bianchi et al. Liver Transpl 2008; 14: 1648-54

Metabolic syndrome (MetS) after LTx
• .
• High prevalence
•From 44.5% to 58%• Mindikoglu et al. Transpl Proc 2006; 38: 1440-44.
• Laryea et al. Liver Transpl 2007; 13: 1109-14.
• Bianchi et al. Liver Transpl 2008; 14: 1648-54.
• Hanouneh et al. Liver Transpl 2008; 14: 1287-93.
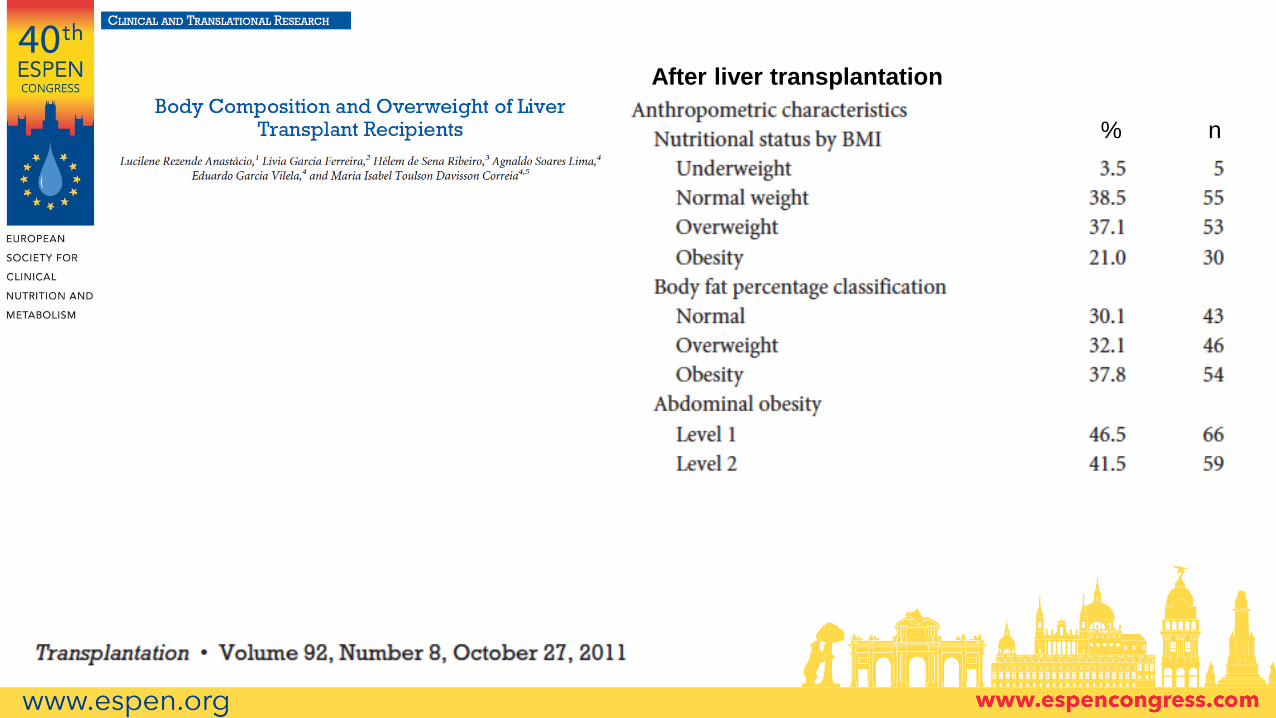
After liver transplantation
% n

Weight variation
2.5%
18.8%
1.3% 0.0% 1.3%
48.1%
52.4%
49.9% 48.7% 42.4%
49.4%
28.8%
48.8% 51.3% 56.3%
0%
50%
100%
Before liver disease 1º time after LTx 1 y after LTx 2 y after LTx 3 y after LTx
Underweight Normal weight Excessive weight


Patient’s perception on risk factors for
weight gain
48.9%
28.6%
24.8%
20.3%
10.5% 9.8%
5.3%8.3%
Aumento da ingestãoalimentar
Melhora da saúde Redução do nível deatividade física
Medicamentos Ansiedade Prednisona Fim das restriçõesalimentares
OutrosNo foodrestriction
OtherIncreased diet
intakeHealth impro. Decreased PA Medication Anxiiety
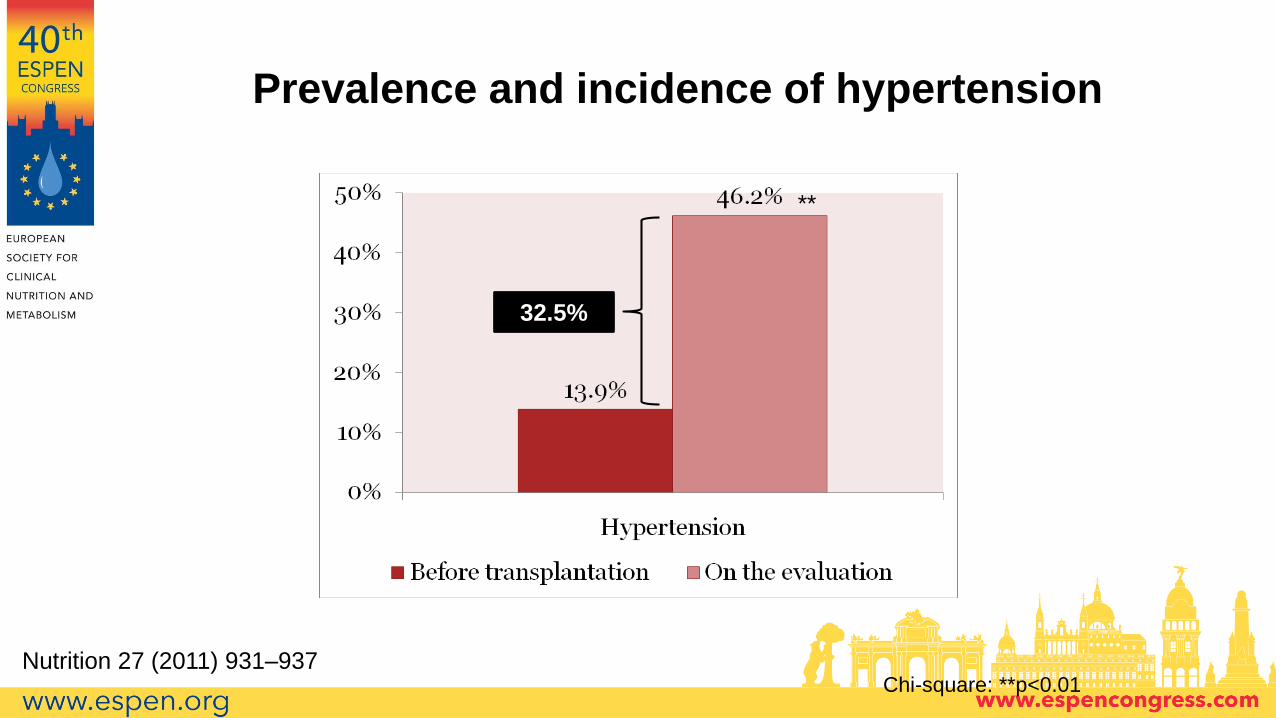
Chi-square: **p<0.01
**
32.5%
Prevalence and incidence of hypertension
Nutrition 27 (2011) 931–937
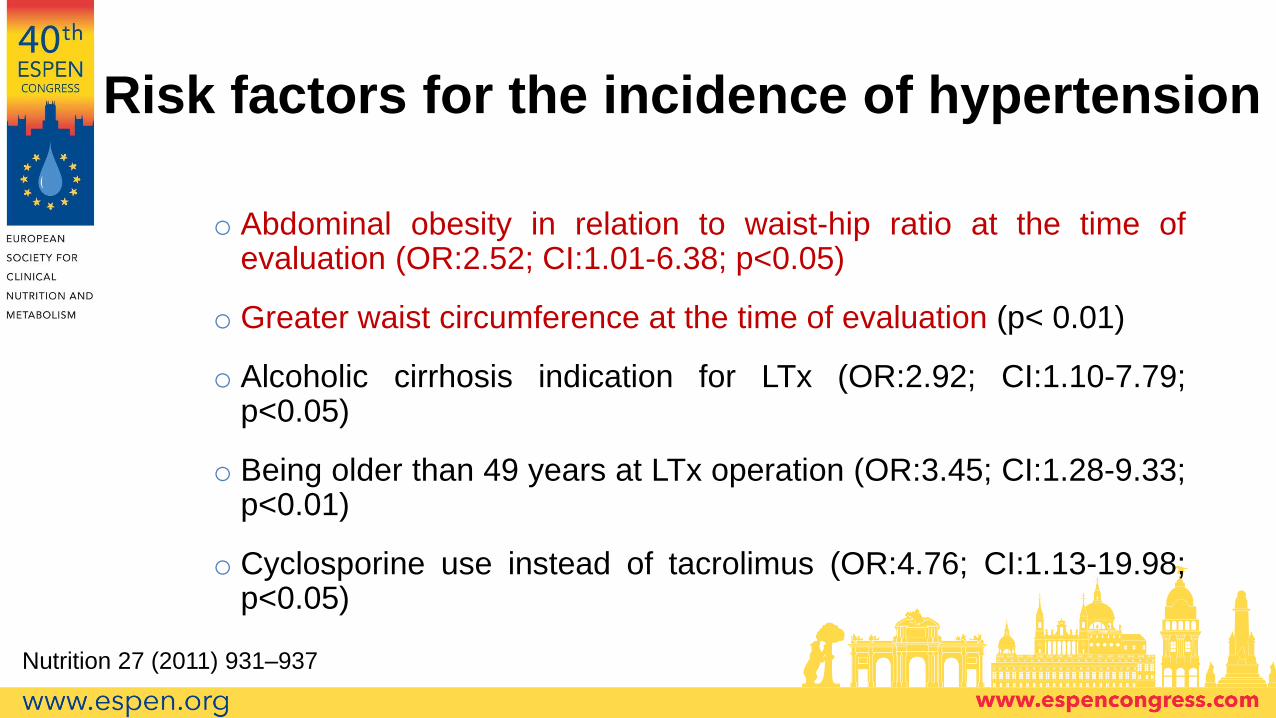
Risk factors for the incidence of hypertension
o Abdominal obesity in relation to waist-hip ratio at the time ofevaluation (OR:2.52; CI:1.01-6.38; p<0.05)
o Greater waist circumference at the time of evaluation (p< 0.01)
o Alcoholic cirrhosis indication for LTx (OR:2.92; CI:1.10-7.79;p<0.05)
o Being older than 49 years at LTx operation (OR:3.45; CI:1.28-9.33;p<0.01)
o Cyclosporine use instead of tacrolimus (OR:4.76; CI:1.13-19.98;p<0.05)
Nutrition 27 (2011) 931–937

Chi-square: **p<0.01
**
15%
Prevalence and incidence of diabetes
Nutrition 27 (2011) 931–937
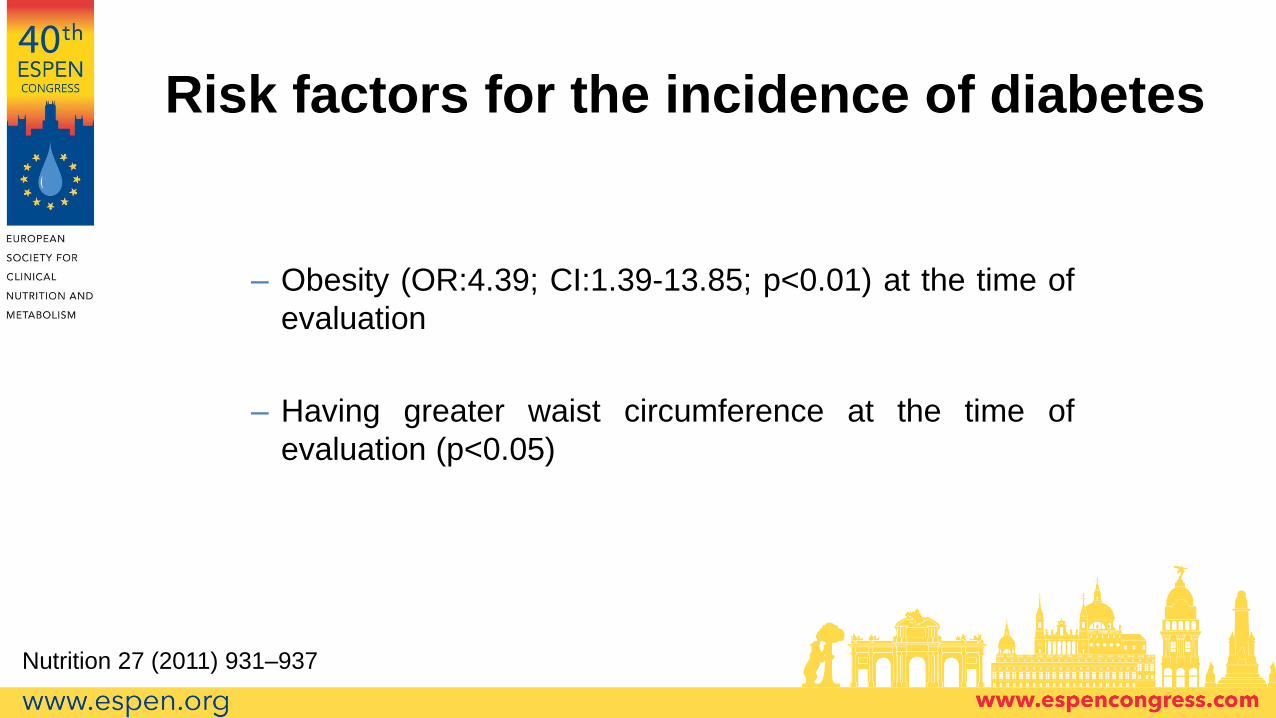
– Obesity (OR:4.39; CI:1.39-13.85; p<0.01) at the time of
evaluation
– Having greater waist circumference at the time of
evaluation (p<0.05)
Risk factors for the incidence of diabetes
Nutrition 27 (2011) 931–937

RESULTS
• 148 patients assessed
– Median age: 53 years (21 – 75 years)
– 61.8% men
– Median time since Tx: 3 years and 8 months (4 m – 14 y)
– Tacrolimus use: 88.5% / Cyclosporine use: 11.5%
– Steroids
• Median time on use: 4 months (1.5 m – 11 y and 8 m)
• Cumulative dose: 2.35 g (0.57 – 39.38)
Nutrition 27 (2011) 931–937
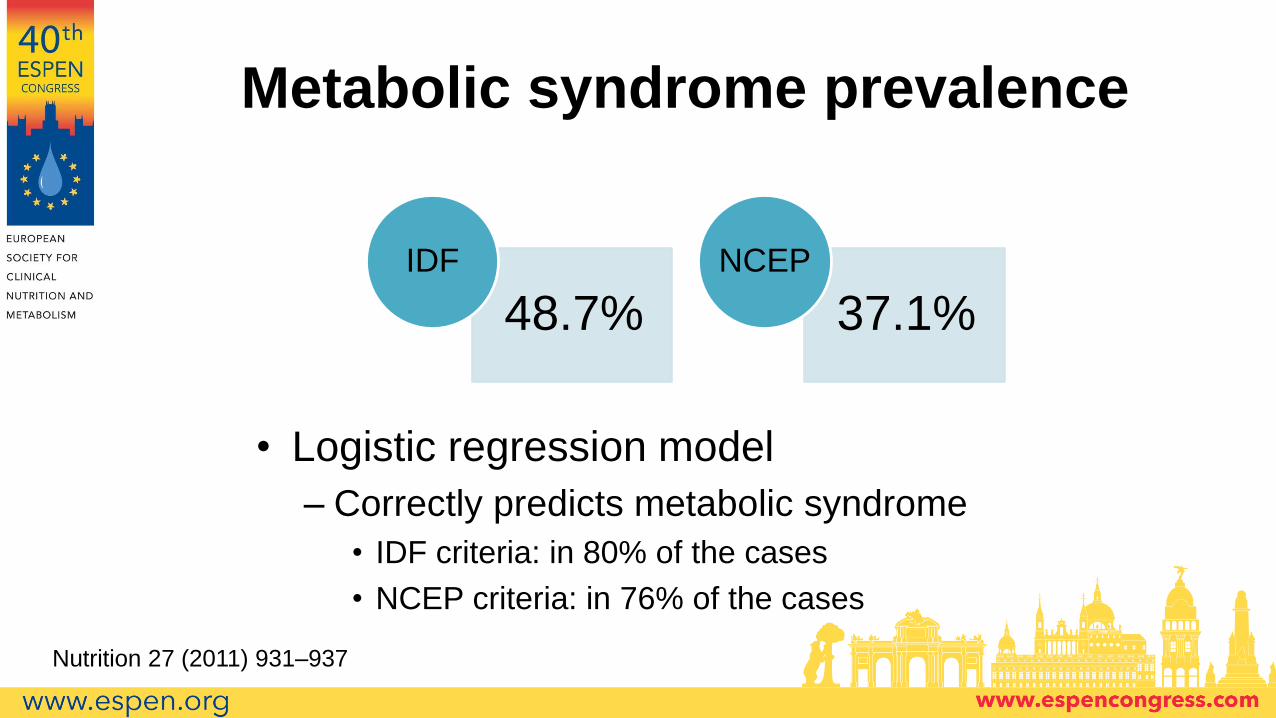
Metabolic syndrome prevalence
• Logistic regression model
– Correctly predicts metabolic syndrome
• IDF criteria: in 80% of the cases
• NCEP criteria: in 76% of the cases
48.7%
IDF
37.1%
NCEP
Nutrition 27 (2011) 931–937

Nutrition 27 (2011) 931–937



Uncontrolled eating and cognitive restraint are associated
with excessive weight gain after liver transplantation
53.5
19.4 16.2
53.1
16.4 12.8
55
28.3 26.9
0
20
40
60
80
100
Cognitive Restraint UncontrolledEating
Emotional Eating
Eating behavior scores based on weight gain
All Weight gain < 14kg Weight gain > 14kg
Ferreira S et al.
Submitted

• Alcoholic liver disease predicted new‐onset obesity (HR,
3.37; P = 0.025)
• Female sex was protective (HR, 0.39; P = 0.034).

Outline
• The transplant patient
• Bebore transplantation• Malnutrition
• Obesity
• After transplantation• Weight gain/obesity
• Associated factors
• Complications
• Conclusions– What can be done?




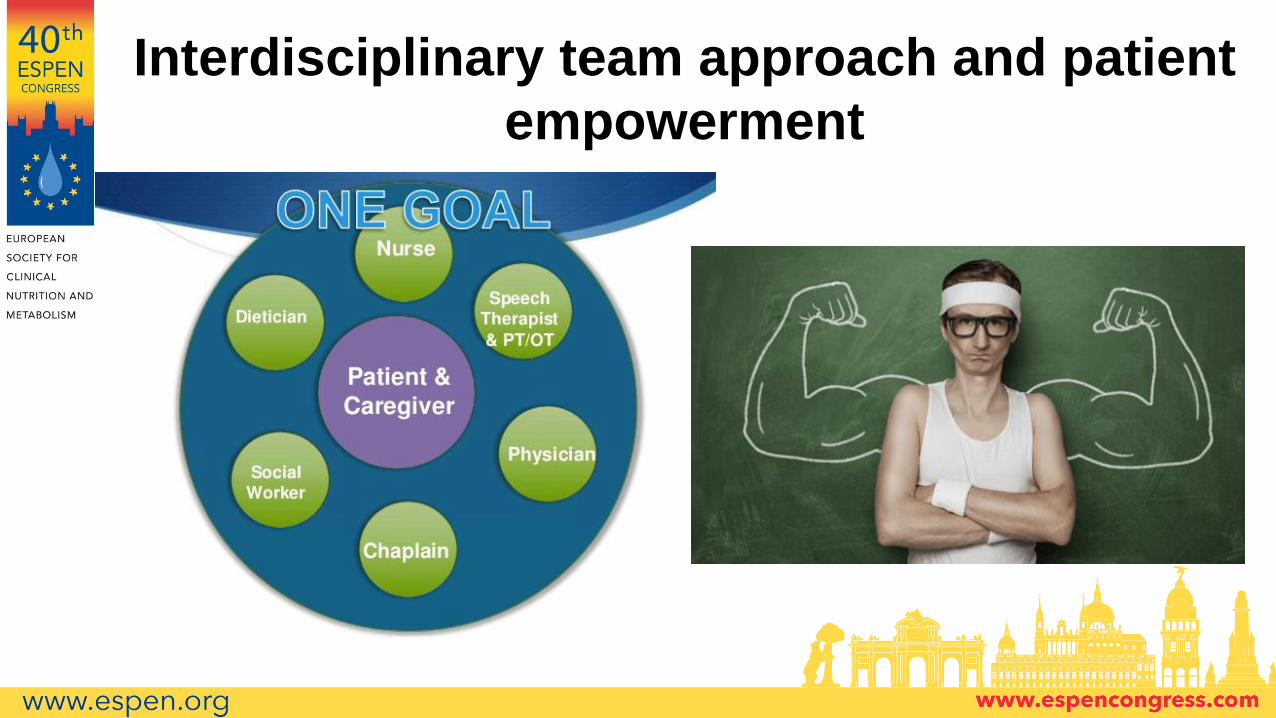
Interdisciplinary team approach and patient
empowerment








