
Orientation to Surgical Technology & History of Surgery
ST210Concorde Career College
History
Objectives:
•Provide a timeline of events leading up to modern medical/surgical practice
•Understand the development of the role of the surgical technologist
•List and describe reasons for surgical intervention


History
Refer to Table 1-1 Pages 4-5 (ST4ST)
•Ancient Times•Dark Ages•Renaissance•Classical Period•Modern Age

Ancient Times4,000 BC
Cuneiform Script

Ancient Times• Imhotep
▫ Circa 2,500 BC▫ Considered the first
physician of recorded history
▫ Wrote one of the first surgical texts
▫ Considered divine due to his work
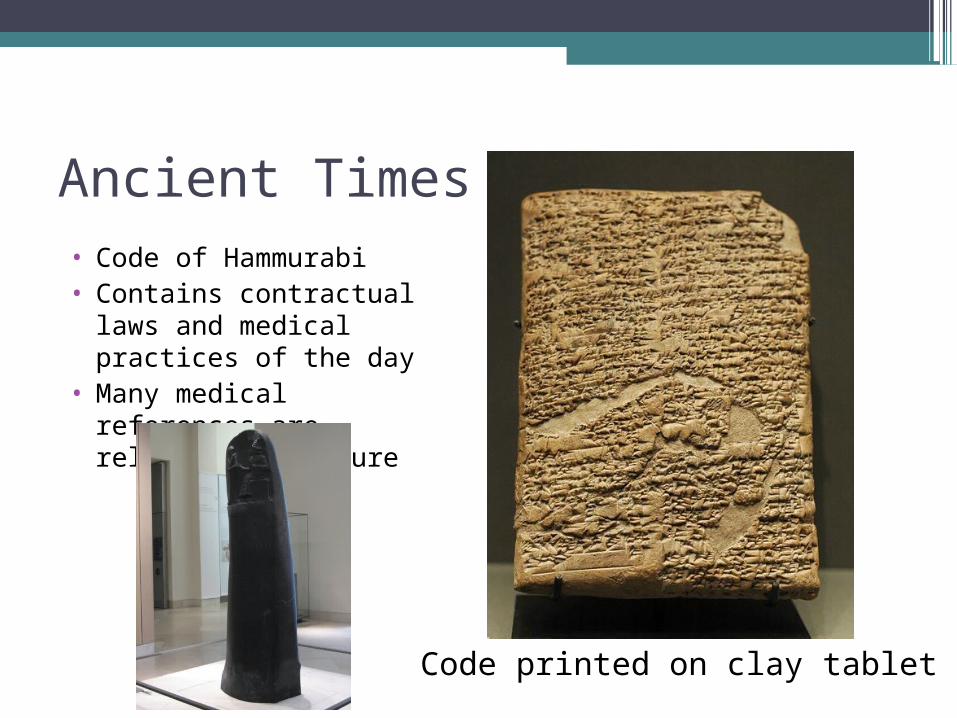
Ancient Times• Code of Hammurabi• Contains contractual laws
and medical practices of the day
• Many medical references are religious in nature
Code printed on clay tablet

Ancient Times• Moses
▫ Circa 2000 BC▫ Established laws for
cleanliness• Caduceus
▫ Numbers 21:4-9

Ancient Times• Circa 1500
▫ Ebers Papyrus▫ Egyptian Medical
hieroglyphs▫ Hindu Vedas

Ancient Times• Circa 1,000 BC
▫ Homer Early Greek historian
and mythologist Described military
medicine▫ Susruta
Father of Indian medicine

Classical Period (500 BC – 500 AD)• Hippocrates
▫ 460 – 370 BC▫ Greek physician▫ The Father of Medicine▫ Introduced the concept
that illness has a physical and rational explaination
Classical Period
• Aristotle▫ 384 – 322 BC▫ Established early
scientific mindset▫ Founder of comparative
anatomy

Classical Period• Herophilos
▫ 335 – 380 BC▫ Father of Anatomy▫ First to describe the
pulse as a diagnostic tool/vital sign

Classical Period• Aulus Cornelius Celsus
▫ 25 BC – 50AD ▫ Greek Encyclopaedist ▫ First to describe the
cardinal signs of inflammation

Classical Period• Aelius Galen
▫ 129 – 200AD▫ World’s first great
anatomist▫ Observations remained
unchallenged for over 1,500 years
▫ Believed that science was ruled by theology and adapted writings to reflect this viewpoint

Dark Ages (500 AD – 1100 AD)

Dark Ages• Avicenna
▫ 980 – 1037 AD▫ Persian philosopher▫ Wrote The Canon of
Medicine▫ Revived Aristotle’s
theories

Renaissance (1450 – 1600)• Paracelsus
▫ 1493 – 1541 AD▫ Swiss physician▫ Disagreed with Galen and
Avicenna, but could not prove his theories scientifically
▫ Called the Luther of Medicine
Renaissance• Ambroise Pare
▫ 1510 – 1590 AD▫ French barber surgeon▫ Greatest surgeon of the
16th century▫ Began ligating arteries
after amputation▫ Stopped cauterizing
wounds with hot irons and oils

Renaissance • Andreas Vesalius
▫ 1514 – 1564▫ Flemish anatomist▫ Father of Modern
Anatomy▫ Openly challenged Galen▫ Performed dissections on
human cadavers himself▫ Hired famous illustrators
to depict his anatomic findings
▫ Changed the world’s approach to anatomic discovery
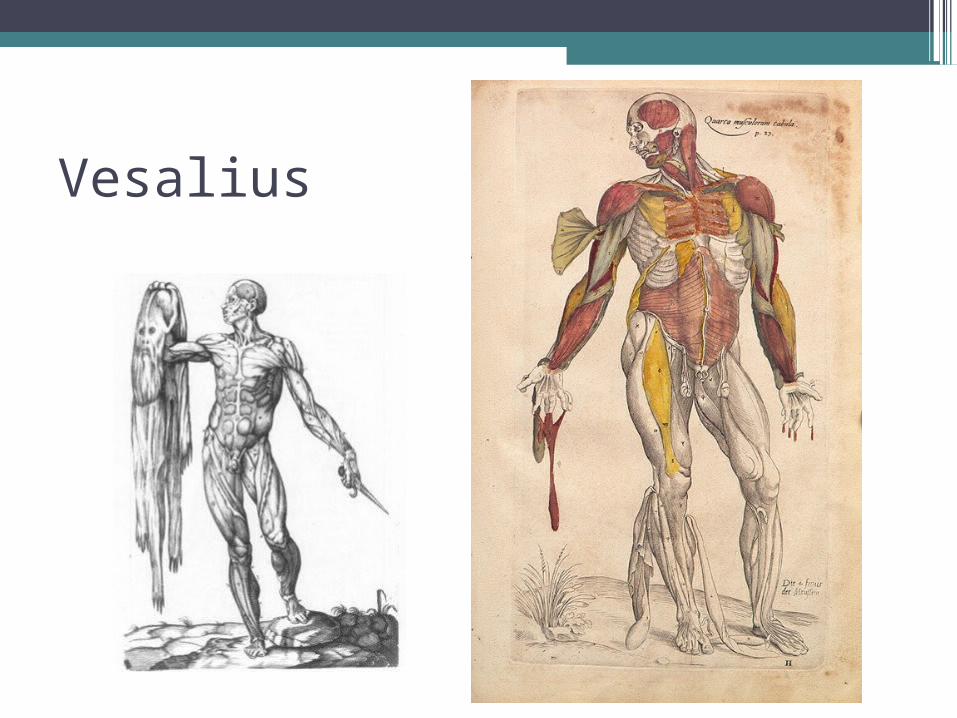
Vesalius
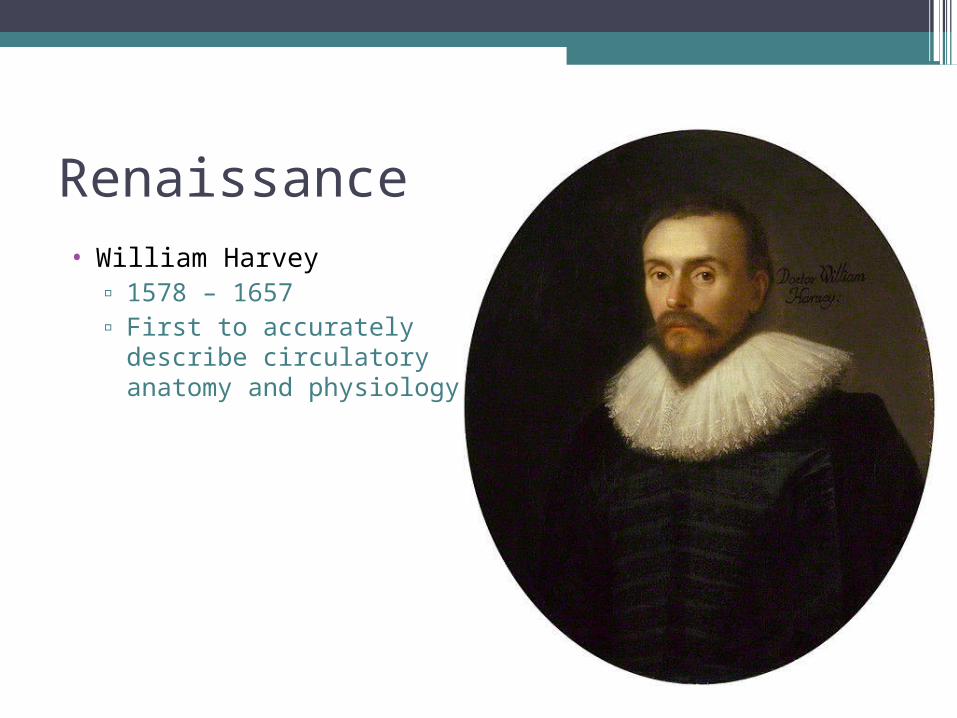
Renaissance• William Harvey
▫ 1578 – 1657▫ First to accurately
describe circulatory anatomy and physiology

Modern Age• Morgagni
▫ Developed modern-day clinical pathology
• Edward Jenner▫ 1749 – 1843 AD▫ Credited with discovering
the small pox vaccine▫ Father of Immunology▫ His work has saved more
lives than any other man
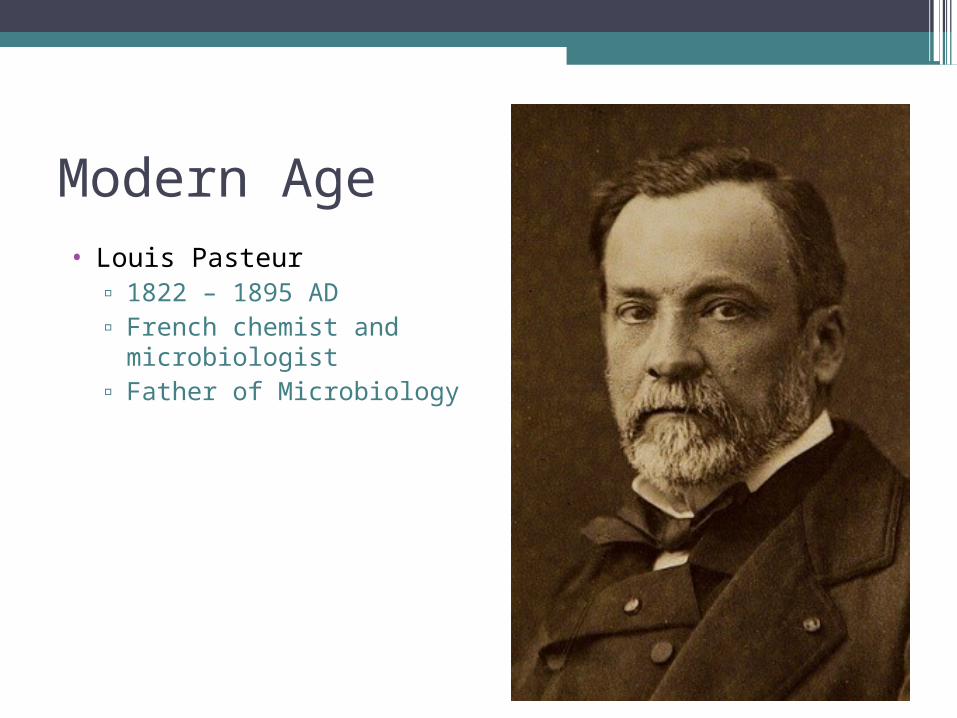
Modern Age• Louis Pasteur
▫ 1822 – 1895 AD▫ French chemist and
microbiologist ▫ Father of Microbiology

Modern Age• Joseph Lister
▫ 1827 – 1912 AD▫ Father of Asepsis▫ Used carbolic acid to
cleanse wounds and sterilize surgical instruments

Modern Age• William S. Halsted
▫ 1852 – 1922▫ Developed techniques for
meticulous wound closure
▫ Halsted’s Principles of Tissue Handling
▫ Developed sterile surgical gloves
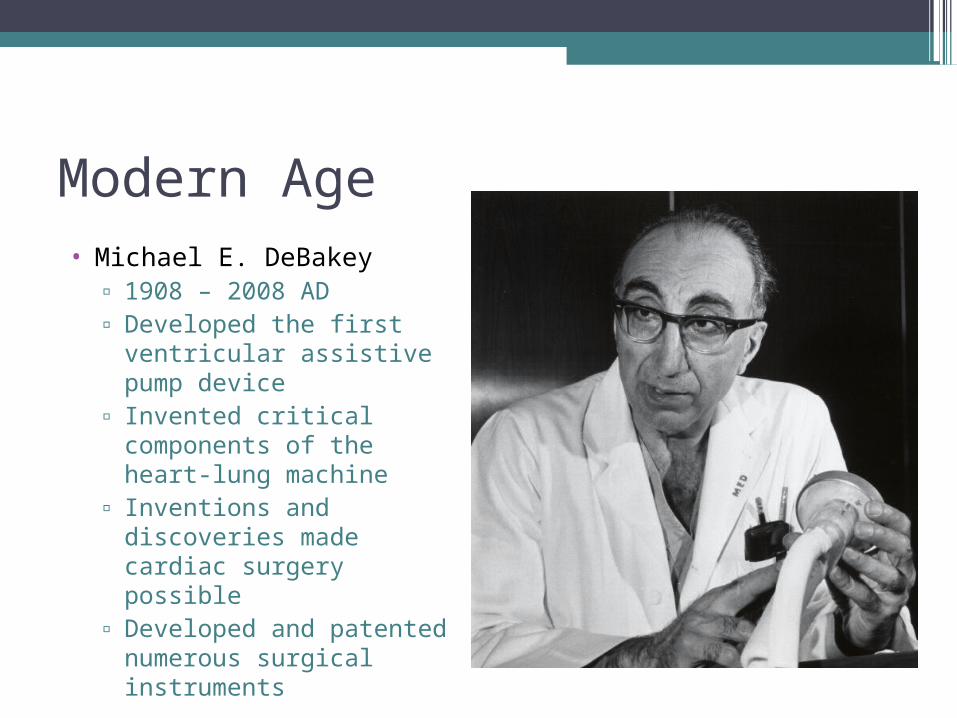
Modern Age• Michael E. DeBakey
▫ 1908 – 2008 AD▫ Developed the first
ventricular assistive pump device
▫ Invented critical components of the heart-lung machine
▫ Inventions and discoveries made cardiac surgery possible
▫ Developed and patented numerous surgical instruments

Modern Age• Denton Cooley
▫ Born 1920▫ Perfected the heart-lung
machine▫ Performed first US heart
transplant▫ Implanted first total
artificial heart
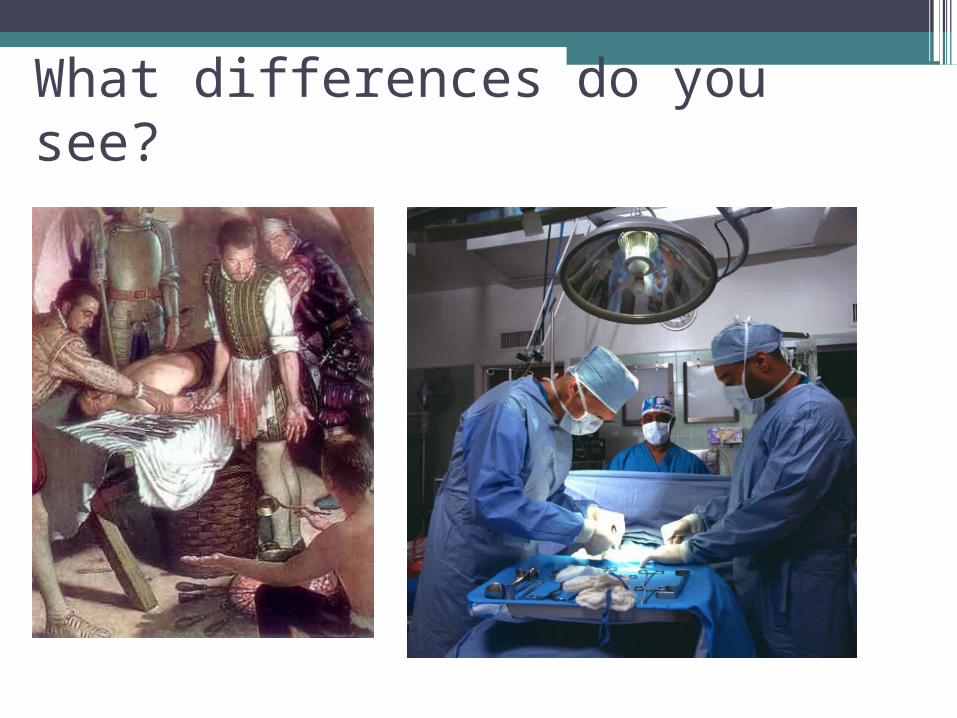
What differences do you see?

History
Once these three principles were identified and solutions found – modern medicine
could emerge!
1. Infection
2. Pain
3. Hemorrhage

History
Development of the Role of the Surgical Technologist
•How/why did the profession originate?•How has surgical technology education
evolved?•Why are you here?

History
Reasons for Surgical Intervention
•Trauma•Disease•Condition•Congenital Anomaly•Desire

History
Classifications of Surgical Intervention
• Emergent – Immediate threat to life or limb (requires immediate treatment)
• Urgent – Urgent threat to life or limb (requires treatment within a short period of time)
• Elective – Does not have to be performed within a short period of time (may be scheduled in the future)
• Optional – Not pathological in the traditional sense (not necessary)

History
Surgical Specialties• General Surgery (General)• Obstetric and Gynecologic Surgery (OB/GYN)• Ophthalmic Surgery (Eye)• Otorhinolaryngologic Surgery (ORL/ENT)• Oral and Maxillofacial Surgery (OMF)• Plastic and Reconstructive Surgery (Plastic)• Genitourinary Surgery (GU)• Orthopedic Surgery (Ortho)• Cardiothoracic Surgery (Hearts/Chest)• Peripheral Vascular Surgery (PV)• Neurosurgery (Neuro)

Workplace Management• CAAHEP: Commission on the Accreditation of
Allied Health Education Programs
• ARC/STSA: Accreditation Review Council on Education in Surgical Technology and Surgical Assisting
• NBSTSA: National Board of Surgical Technology and Surgical Assisting
• JC: Joint Commission, formerly known as the Joint Commission Accreditation of Health Care Organizations (JCAHO)

Phases of Surgical Care Management•Preoperative: prior to initiation of the
surgical procedure
•Intraoperative: while procedure is being performed
•Postoperative: when surgical procedure is terminated

PPEOR PreparationSterile field (creating, organizing, maintaining)OrganizingAssisting with gowning and glovingDraping
PREOPERATIVE CASE PREOPERATIVE CASE MANAGEMENTMANAGEMENT
Maintain the sterile fieldHandling of instruments, supplies, etc.Preparing medicationsCountingProper specimen identification and labelingDressing application
INTRAOPERATIVE CASE INTRAOPERATIVE CASE MANAGEMENTMANAGEMENT

Maintain the sterile field until the patient is out of the roomDisassemble the sterile fieldPatient transportationRoom turnover
POSTOPERATIVE CASE POSTOPERATIVE CASE MANAGEMENTMANAGEMENT

Surgical Team Members

NON-STERILE SURGICAL NON-STERILE SURGICAL TEAM MEMBERSTEAM MEMBERS
Circulator (RN, LPN, or Surgical Technologist)Anesthesia ProviderRadiology TechnologistPathologySurgical ObserversAnyone outside of the sterile field

Preparing the ORConducting pre-op patient interviewTransporting to and from the OR (Pre-op, PACU)Transporting the pt. to and from the OR tablePositioningPrepping the skinAssist with drapingAssist anesthesiaCounting, gathering suppliesVarious cord hook-upsMaintaining the OR recordSpecimensDressings
CIRCULATING DUTIESCIRCULATING DUTIES

Non-sterile Team Members

ANESTHESIA PROVIDER ANESTHESIA PROVIDER RESPONSIBILITIESRESPONSIBILITIES
MD, DO, CRNAPt. assessmentDetermining type of anesthesiaDiscussing the risks of anesthesiaMonitoring vital signsProviding supportive measures (airway, fluids)

STERILE TEAM MEMBERSSTERILE TEAM MEMBERS

WHO ARE THEY?WHO ARE THEY?
Surgical TechnologistSurgeon
MD, DO, DPM, DDS, DMD
Surgical AssistantCSFA, CSA, SA-C, CRNFA or RNFA, PA-C, OT-C or OPA-C, surgical resident, or other surgeonCST (limited scope)
The SurgeonThe Surgeon
•Assumes full responsibility for all medical acts of judgment and management of the surgical patient

Surgical First Assistant
Manual dexterity Manual dexterity and physical and physical stamina are stamina are requiredrequired
Acts as co-Acts as co-surgeonsurgeon
Responsible for Responsible for exposure and exposure and visualization of visualization of the woundthe wound

Why Surgical Technologists?

Personal Characteristics
•Ability to multi-task•Neat, accurate•Ability to stay focused in any situation•Stable temperament, patience•Manual dexterity, physical stamina•Ability to anticipate “what comes next”

Working Conditions
• Brightly lit, quiet, temperature controlled OR• Standing for long periods of time• Lifting heavy objects• Concentration• Unpleasant sites, odors, hazardous
materials, communicable diseases• 40 hour work-week plus “call rotation”
nights, holidays, and weekends







