Pathways Housing First!Program Philosophy and Practice
February 24, 2015
____________________________________________________________

This Morning’s Agenda• Welcome • Overview to the training • Introduction to Housing First program model• Housing operations• Support and treatment services• Treatment Philosophy• Harm Reduction/Peer Support• Research evidence: At Home/Chez Soi• Housing First as an Approach to Services • Open Forum Discussion (ongoing)

HPS Homeless-Services System Redesign
• Transformation: Change expectations and outcomes for local and regional systems for chronically homeless
• Redesign: Change ways of organizing and delivering services so that they appropriate to client needs
• Collaboration: Organizations working together towards the same goal of ending homelessness
• Tangible metrics: to determine program and system success, and examine how funds are expended

10% use 50% of system
resources
Homeless Population
5-10% chronically homeless
10-15% episodically homeless
80% transitionally homeless
WHO IS ELIGIBLE?Who are ‘the chronically homeless?’
• Living on the streets, shelters, drop-in center
• Mental health problems• Addiction and abuse• Health problems• Extreme Poverty• Isolation• Stigma• PTSD/Trauma
• Loyalty as a value (loyal brother and friend)
• Likes to cook, creative• Listens to country music• Follows sports teams• Protective, roots for the
underdog, sociable • Has a remarkable memory
for people and names• Opportunities to learn about
addiction
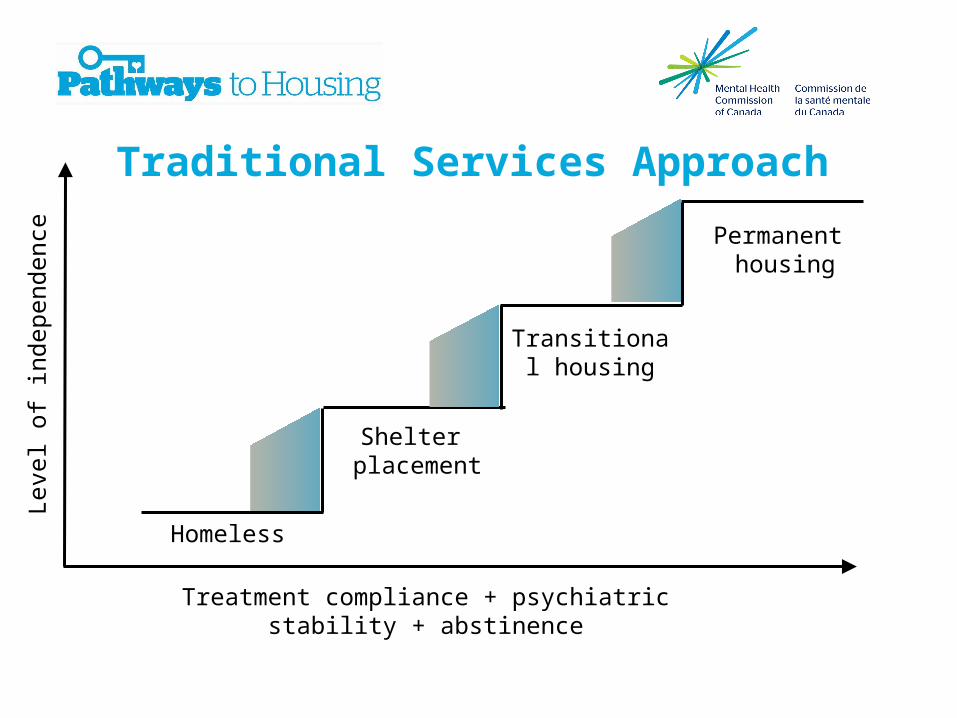
Traditional Services Approach
Leve
l of i
ndep
ende
nce
Treatment compliance + psychiatric stability + abstinence
Homeless
Shelter placement
Transitional housing
Permanent housing

Staircase Model is Based on Unrealistic Expectations

Intersection of Mental Illness, Addiction and Homelessness
Institutional Circuit

HOUSING FIRST
Is a Paradigm Shift_________________________________________________________________

Homeless
Shelter placement
Transitional housing
Permanent housing
Ongoing, flexible support
Harm Reduction
Housing First Model
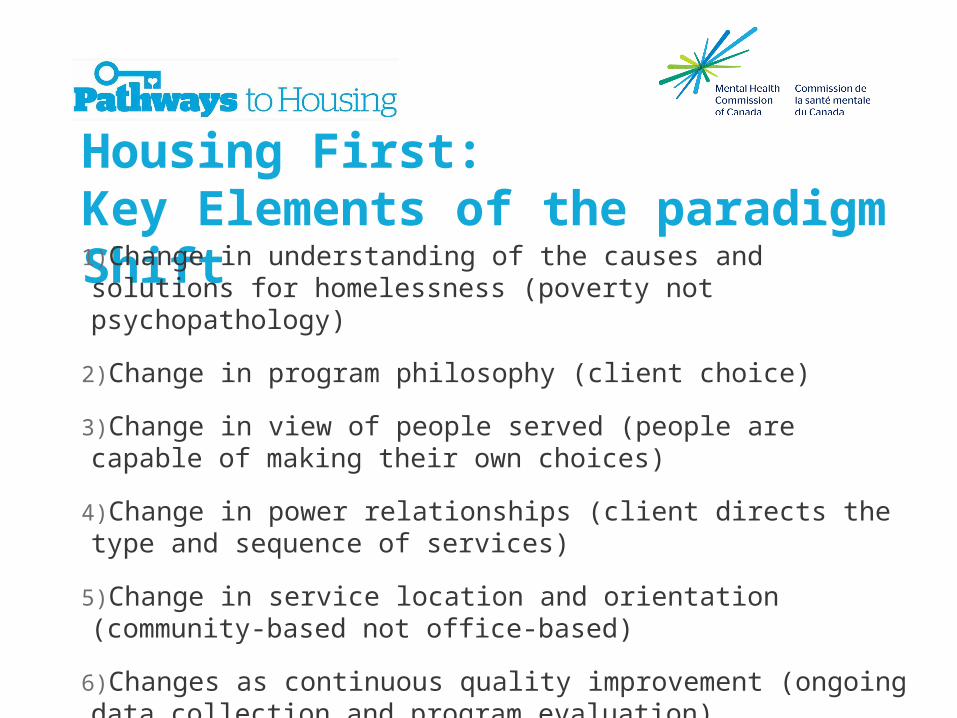
Housing First:Key Elements of the paradigm Shift1)Change in understanding of the causes and solutions for homelessness (poverty not psychopathology)
2)Change in program philosophy (client choice)
3)Change in view of people served (people are capable of making their own choices)
4)Change in power relationships (client directs the type and sequence of services)
5)Change in service location and orientation (community-based not office-based)
6)Changes as continuous quality improvement (ongoing data collection and program evaluation)

5 Dimensions of a Pathways’
Housing First Program Fidelity

Housing: Independent Apartments in Community
Settings (Rental and Social)• Most participants prefer own place in normal settings
• Independent apt• Scatter site (<20%)• Creates sense of home• Tenants Rights• Affordable (30%) +rent supp • Decent • Support services are off site

HF is Permanent Supportive Housing
IntegratedIndistinguishable
Support services are off site

Scatter site rural setting, Pathways VT
200 Tenants, 200 Apartments, 2 Counties, 6 Cities, 95 Landlords: Housing Retention Rate 90.5% (12 mo)

Landlords as Program Partners
Common GoalLandlord, agency and participant–
All want safe, decent, well-managed housing

Choice, Relocation and Limits to Choice• 2 Program requirements
• A) 30% of Income towards rent• B) Weekly apartment visits (change over time or crisis)
• Negotiation about apartment relocation is different than conversation about selecting first apartment
• Conditions that require additional support, e.g., mobile crisis, involuntary commitment

Clinical and Support Services• Consumers choose the type,
frequency and intensity of services
• Program requires home visit (and there are limits to choice)

Goals of Housing First• End Homelessness by providing immediate access to permanent housing and supports for people with behavioral health, addiction and other complex problems
• Build self-determination and mastery (recovery) by offering consumer-driven services
• Improve consumer’s quality of life and support recovery

Housing first, what’s second?
Health &Wellness/Chronic and Acute Health Problems
Finances/Budgeting/Money
Management
Alcohol/Drug -- Use Abuse
Mental Health Issues
job, training, education
Eviction preventi
on
legal
Choice is the foundation and driving force that directs clinical and housing services• Choice, self-determination and building towards graduation at the point of entry
• Practical limits of choice: real estate market, standard lease obligation, fixed incomes, and other real world constraints.
• Clinical issues and constraints to choice: psychiatric emergencies, relapse, social networks, and more.
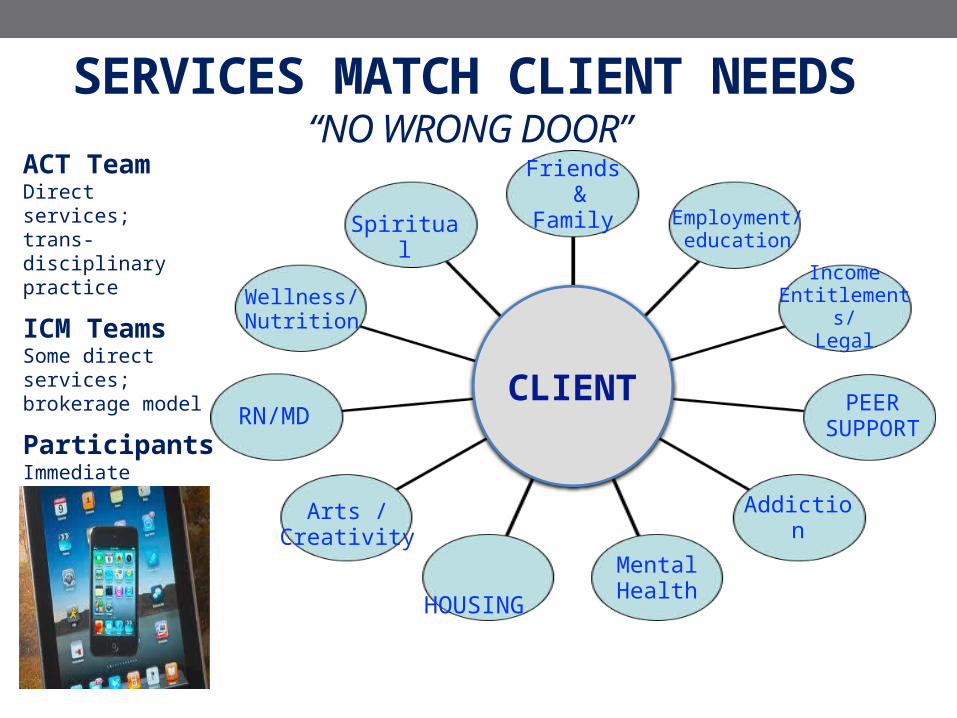
SERVICES MATCH CLIENT NEEDS “NO WRONG DOOR”
Spiritual
Wellness/Nutrition
Arts /Creativity
HOUSING
Addiction
PEERSUPPORT
Income Entitlements/
Legal
Employment/education
MentalHealth
Friends & Family
ACT Team Direct services; trans-disciplinary practice
ICM Teams Some direct services;brokerage model
ParticipantsImmediate access; client-directed RN/MD
CLIENT
iiiii

SERVICES: Matching the level of services to the person’s needs (rearrange existing service models)Intensive Case-management
• Moderate Need: ICM case management team provides support and brokers services
• Services provided in the participant’s home or community (group meetings offered at offices or other community settings)
• Off site and on-call services 7-24
• All teams use a recovery orientation
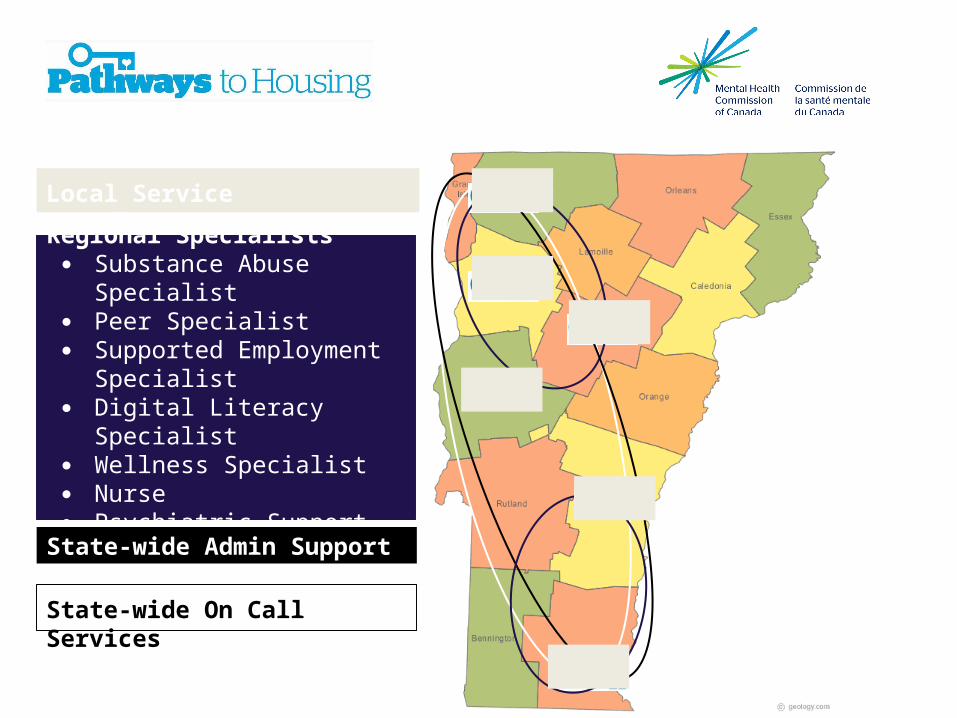
Regional Specialists● Substance Abuse Specialist● Peer Specialist● Supported Employment
Specialist● Digital Literacy Specialist● Wellness Specialist● Nurse● Psychiatric Support
State-wide Admin Support
State-wide On Call Services
Local Service Coordinators

Regional Service Specialists - 2 Team Leaders- 1 Supportive Employment Specialist- 1.5 Computer Literacy Specialist- .5 Nurse- .3 Psychiatrist
Franklin/Grand Isle- 1 Service Coordinator- .5 Substance Abuse Specialist
Chittenden- 3.5 Service Coordinators- .3 Substance Abuse Specialist
Washington- 2.5 Service Coordinators- .5 Substance Abuse Specialist
Windham- 2.5 Service Coordinators
Statewide- Medical Director- Project Manager- Intake Coordinator- Housing Director
- Administrative Staff
Red Clover Properties - 2 Housing Specialists
= Red Clover Properties (Housing Team)
Red Clover Properties- 1 Housing Specialist
Windsor - 1 Service Coordinator
Addison - 1 Service Coordinator- .5 Substance Abuse Specialist
Regional Service Specialists - 1 Team Leader- .5 Computer Literacy Specialist- .5 Substance Abuse Specialist- .5 Peer Specialist- .3 Nurse -. 1 Psychiatrist
Pathways HF Program Staff

SEPARATION OF HOUSING AND SERVICES_____________________________________________________________________________________________________________
Separated spatially, conceptually,and operationally

PRINCIPLE 3: HOUSING and SERVICESARE SEPARATE DOMAINS

Program Philosophy, Program Values
andProgram Practice

Philosophy
• Humanitarian: Psychological, Economic and Human Rights Integration
1) Positive view of human nature 2) Provide fundamental security and support3) Person is self-motivated
(program: housing as a human right)

Medicine Wheel
• Focus on Aboriginal homeless population• 3rd arm included traditional healing approaches (e.g., medicine wheel)

Person CenteredCapability focusInter-personal (you are an active agent in the treatment and outcome)
RECOVERY ORIENTATION

Relationship is the Foundation
Key Role for Peer Support

PATHWAYS HOUSING FIRST PROGRAM
What is Program Fidelity? How do you Measure it?Why does it matter?
____________________________________________________________________

Why Fidelity?

The case of Housing First… “It’s all about Housing & Choice”Pathways Housing First Fidelity Scale Results: Program Spectrum
“Participants can choose the housing they want regardless of whether they are
actively using.”
“Participants can choose to be clean and sober and they’ll get an apartment. Or they can choose to continue using and we’ll still give them housing in a room &
board”

Fidelity Site Visit• Before visit: collect basic info
o What types of housing do participants live ino How long did it take to get into housingo What percentage of participants have been discharged
• Team meeting observation
• Individual interviews with staffo All frontline providers; Each disciplineo Team Leadero Program Director, Administrators
• Focus group with program participants
• Chart review (random selection)
• Optional: home visits

Key Point

PATHWAYS HOUSING FIRST
Program Evaluation and Research Outcomes
__________________________________________________________________

MENTAL HEALTH COMMISSION OF CANADA (2009):AT HOME/CHEZ SOI -- 5 CITIES, RCT N=2,215

Homelessness and Mental Illness Homelessness is a significant social problem in
Canada(Estimates of 200,000 individuals per year)
Prevalence of mental illness and substance abuse/dependence is high and associated with poorer outcomes
Higher use of health, criminal and social services
At Home/Chez Soi Demonstration Project
• 2008 federal gov’t allocated $110 million over 5 years to the Mental Health Commission of Canada (www.mentalhealthcommission.ca)
• Action research on how to support people with severe mental illness to exit homelessness
• 85% funding for services and 15% for research
• Largest study of its kind in the world

Who Participated in At Home/Chez Soi?• 2148 participants
• 1158 in Housing First (HF)
• 990 in Treatment as Usual (TAU)
• Primarily middle-aged
• 32% of participants are women
• 22% of participants identified as being an Aboriginal person
• Typical total time lifetime homeless is nearly 5 years
• All have one or more serious mental health issue
• Majority have a concurrent disorder
• More than 90% had at least one chronic physical health problem

Housing: Stability – by ProgramPercentage of time housed

Summary of Fidelity Rating Results• 12 programs rated on 38 fidelity items in 5 domains
• Early implementation (Year 2) and one year later (Year 3)
• Overall, strong fidelity to the Housing First model (program ingredients rated above 3 on a 4-point scale)
• 71% Year 2; 78 % Year 3
• Higher fidelity in the 12 programs (5 ACT, 7 ICM) was related to:
- greater direct and indirect service time and more contacts with - participants (corr. = .55 to .60)
- greater housing stability (% of time in housing)- greater improvement in quality of life (d = .10) and
community functioning (d = .11)

Lessons Learned: 1. CAPABILITIES
• People are much more capable than we imagined possible.
• We have often confused functionality with capability

2. Need to Assume More Risk and Responsibility
Making progress requires a change in approach that involves taking some calculated risks for all of us (staff, board members, landlords, housing authority and policy makers, participants, family members, and the public).
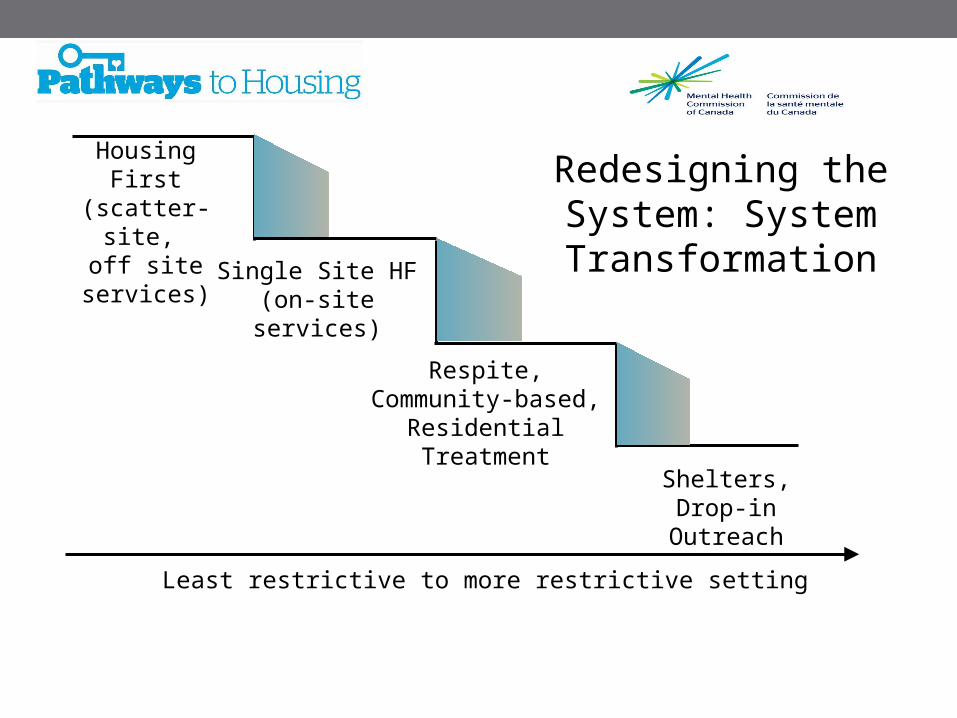
Respite, Community-based, Residential
Treatment
Single Site HF (on-site services)
Housing First (scatter-site,
off site services)Redesigning the System: System Transformation
Shelters, Drop-in Outreach
Least restrictive to more restrictive setting

3. Dissemination/Replication• High fidelity yield consistently high
results: 80%- 90%
• Need local champion
• Clear understanding of program model
• Compatible values in host agency culture
• Resources for Housing and Services

THANK YOU for your attentionContact us: [email protected]
Visit: www.Pathwaystohousing.org
Follow us:







