Download - Pediatric Endocrinology

Pediatric Endocrinology
Sarah LawrenceDivision of EndocrinologyCHEO

Outline
Growth/short stature Puberty – precocious and delayed Disorders of Sex Development Diabetes Thyroid

Short Stature

Predicted Height
155 cm168 cm177 cm
3 boys age 10 128 cm
BA 8 BA 10 BA 12
Which will be taller as an adult?

Midparental [target] height: males
Mother
Father
Target Height
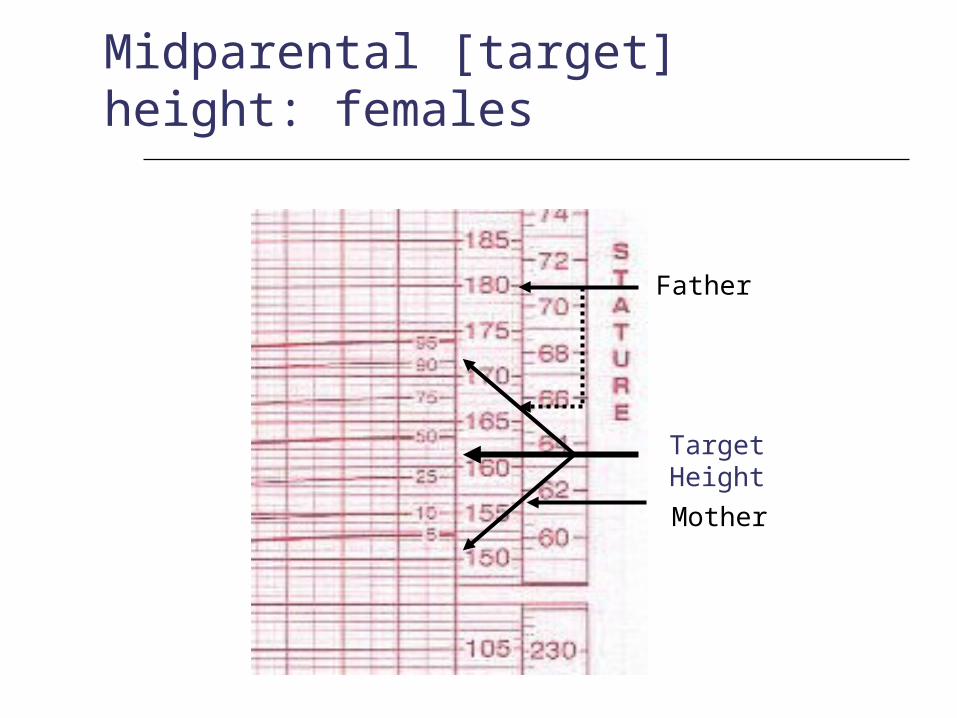
Midparental [target] height: females
Mother
Father
Target Height
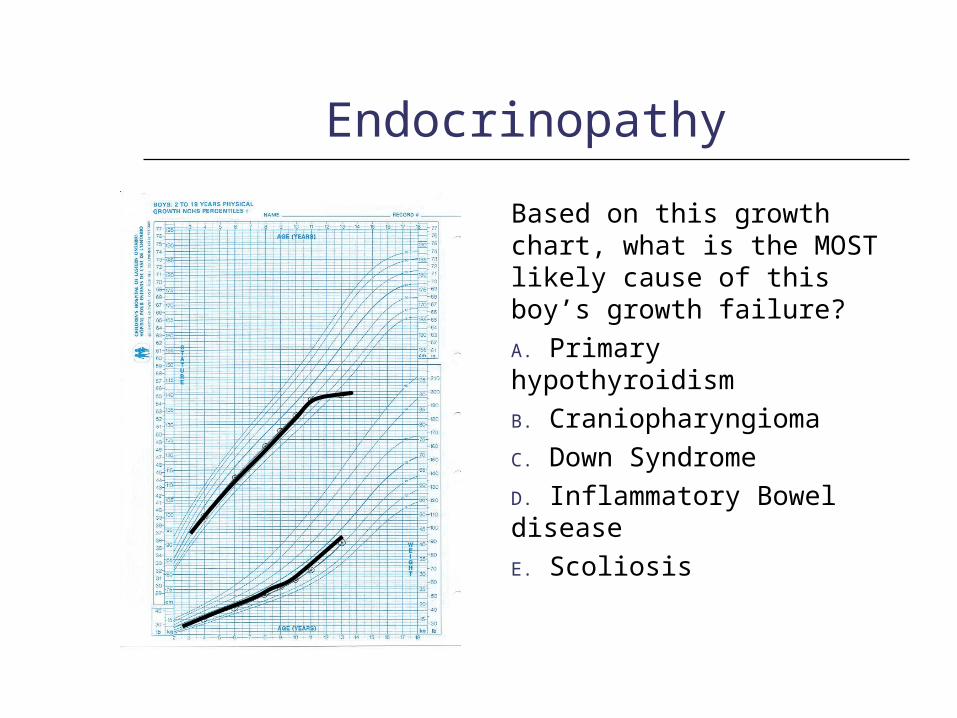
Endocrinopathy
Based on this growth chart, what is the MOST likely cause of this boy’s growth failure?A. Primary hypothyroidismB. CraniopharyngiomaC. Down SyndromeD. Inflammatory Bowel diseaseE. Scoliosis

Chronic Disease
Based on this growth chart, what is the MOST likely cause of this boy’s growth failure?A. Primary hypothyroidismB. CraniopharyngiomaC. Down SyndromeD. Inflammatory Bowel diseaseE. Scoliosis

Approach to Short Stature
Growth velocity
Target Height
Familial Short Stature Constitutional Delay
Normal Variant
IUGR
Dysmorphic syndromes
Chromosomal disorders
Prenatal
Medications
Chronic disease
Endocrine
Postnatal
Proportionate Disproportionate
Pathologic
Short Stature
Idiopathic Short Stature
Precocious Puberty
Presence of secondary sexual development by age:
8 in a girl
9 in a boy

Puberty Sequence: Girls

Puberty Sequence: Males

Approach to Precocious Puberty
Growth Velocity
Bone Age
Premature Thelarche
Estrogen
Premature Adrenarche
Androgens
Normal variant
Normal
Central
Androgens Estrogen
Peripheral
Pathological
Increased
Precocious Puberty
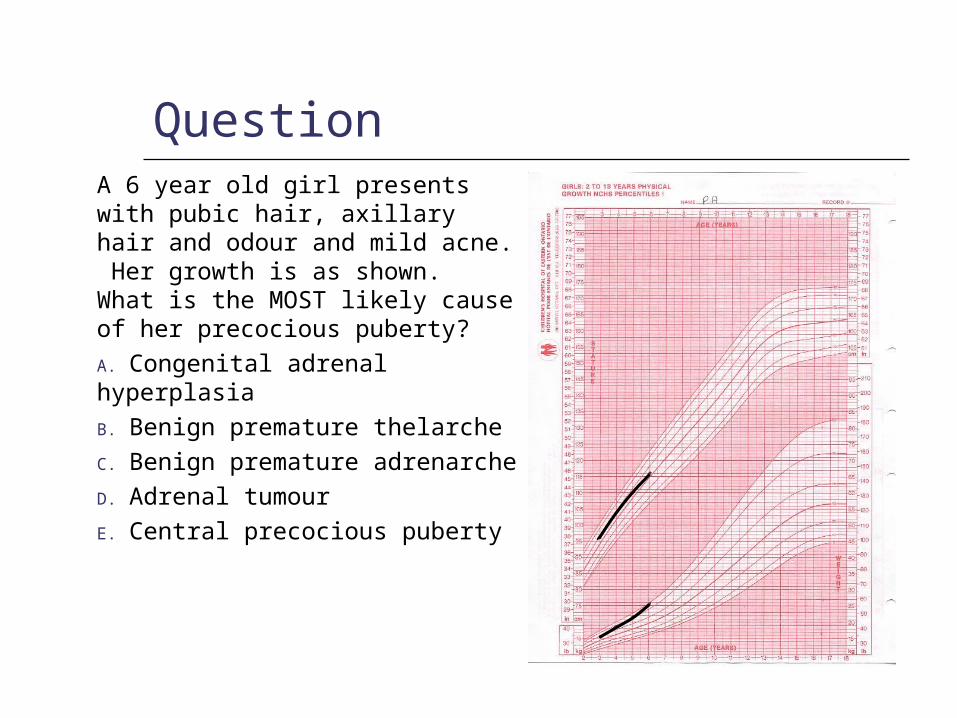
QuestionA 6 year old girl presents with pubic hair, axillary hair and odour and mild acne. Her growth is as shown. What is the MOST likely cause of her precocious puberty?A. Congenital adrenal hyperplasiaB. Benign premature thelarcheC. Benign premature adrenarcheD. Adrenal tumourE. Central precocious puberty
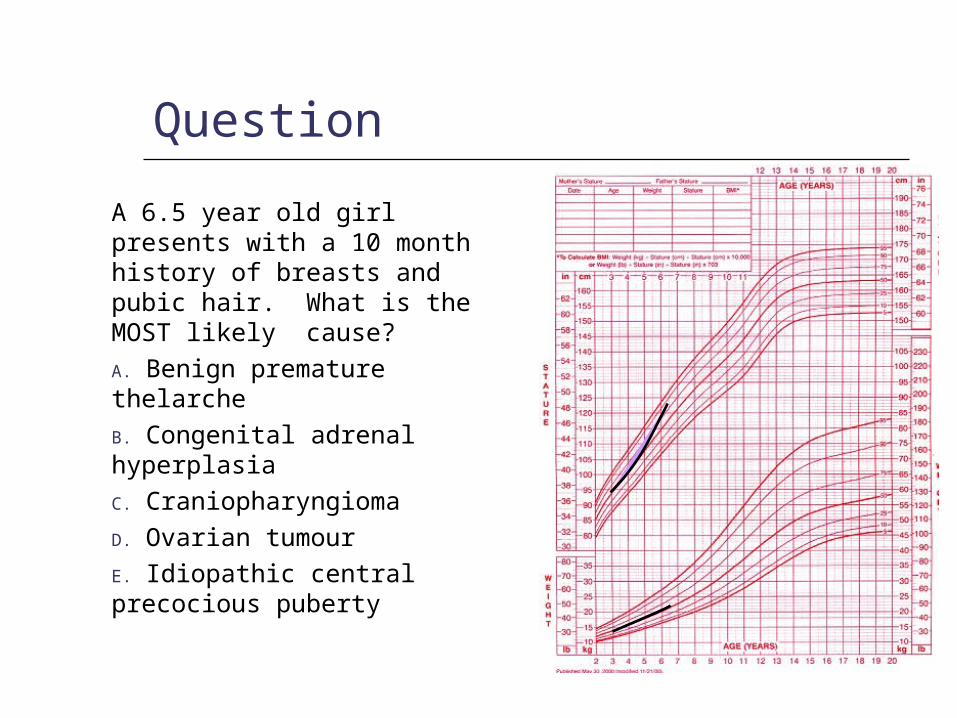
Question
A 6.5 year old girl presents with a 10 month history of breasts and pubic hair. What is the MOST likely cause?A. Benign premature thelarcheB. Congenital adrenal hyperplasiaC. CraniopharyngiomaD. Ovarian tumourE. Idiopathic central precocious puberty

Approach to Precocious Puberty: Females
Premature
Thelarche
Estrogen
Premature
Adrenarche
Androgens
Normal Variant
Normal
Estrogen
+/- androgens
Central
Ovary
Adrenal
Other
Estrogen
Ovary
Adrenal
Other
Androgens
Peripheral
Pathological
Increased
Bone age, GV

x
CAH 29/01/92
QuestionA 5 year old boy presents with pubic hair, growth acceleration. He has Tanner 4 pubic hair and genitalia with 2 ml testes. What is the MOST likely diagnosis?
A. Idiopathic central pubertyB. Congenital adrenal hyperplasiaC. Hypothalamic tumourD. Testicular tumour
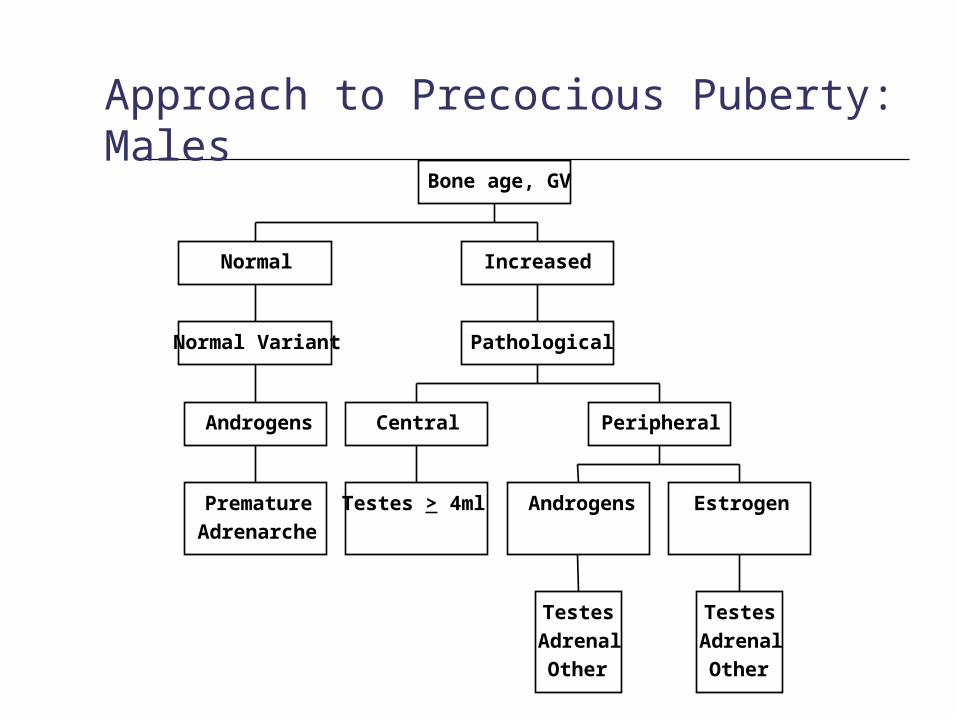
Approach to Precocious Puberty: Males
Premature
Adrenarche
Androgens
Normal Variant
Normal
Testes > 4ml
Central
Testes
Adrenal
Other
Androgens
Testes
Adrenal
Other
Estrogen
Peripheral
Pathological
Increased
Bone age, GV

Delayed Puberty
Absence of secondary sexual development by age:
13 in a girl
14 in a boy
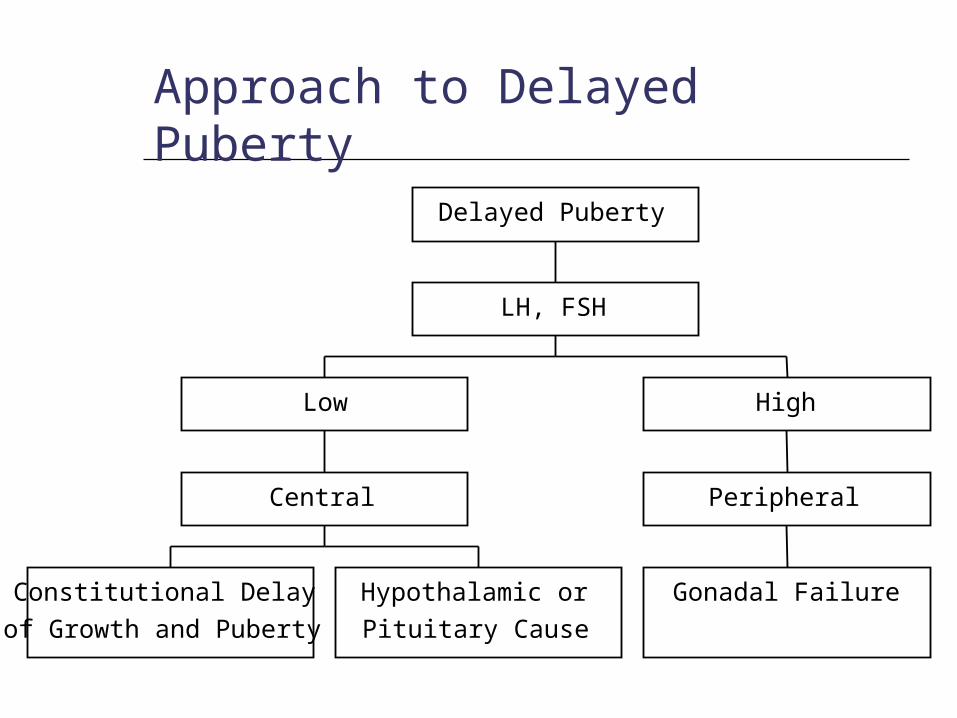
Constitutional Delay
of Growth and Puberty
Hypothalamic or
Pituitary Cause
Central
Low
Gonadal Failure
Peripheral
High
LH, FSH
Delayed Puberty
Approach to Delayed Puberty

Delayed Puberty: Investigations
Growth records
Bone age
LH, FSH
Sex hormone levels - not needed
Other hormones as clinically indicated (T4, TSH, GH, Prolactin, Cortisol)

Delayed Puberty: Treatment
Hyper / Hypogonadotropic Hypogonadism
Boys: Testosterone intramuscular injection, transdermal
patch/gel or orally, gradually increasing to adult doses
Girls: Start with low dose estrogen, increasing over 1-2 years,
then begin cycling with estrogen and progesterone
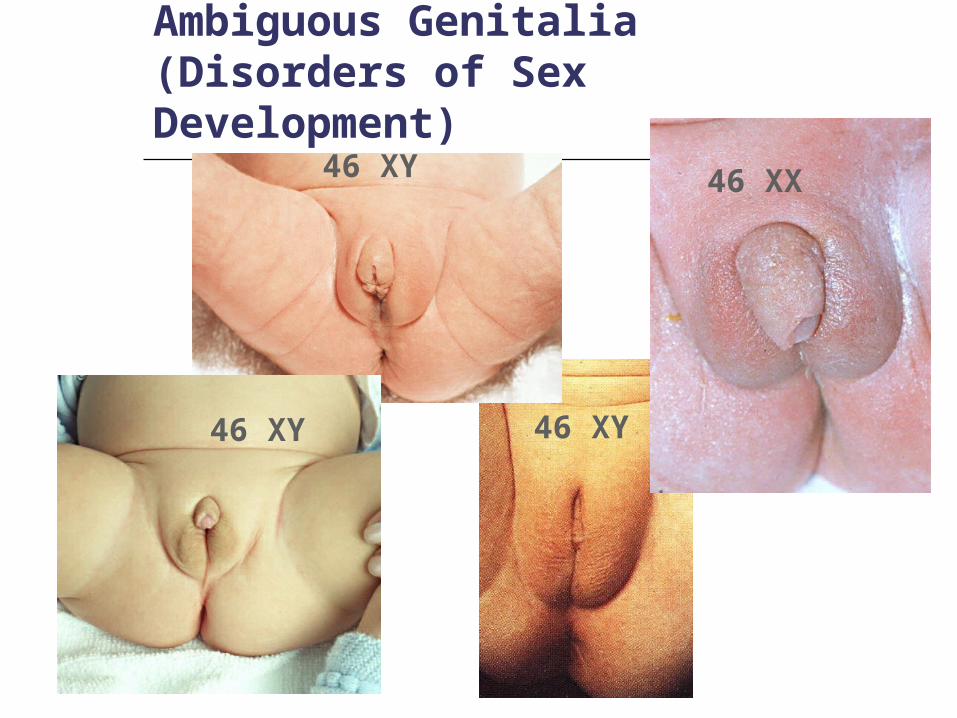
Ambiguous Genitalia (Disorders of Sex Development)
46 XY
46 XY 46 XX
46 XY
Development of Internal and External Genitalia
http://www.aboutkidshealth.ca/En/HowTheBodyWorks/SexDevelopmentAnOverview/Pages/default.aspx
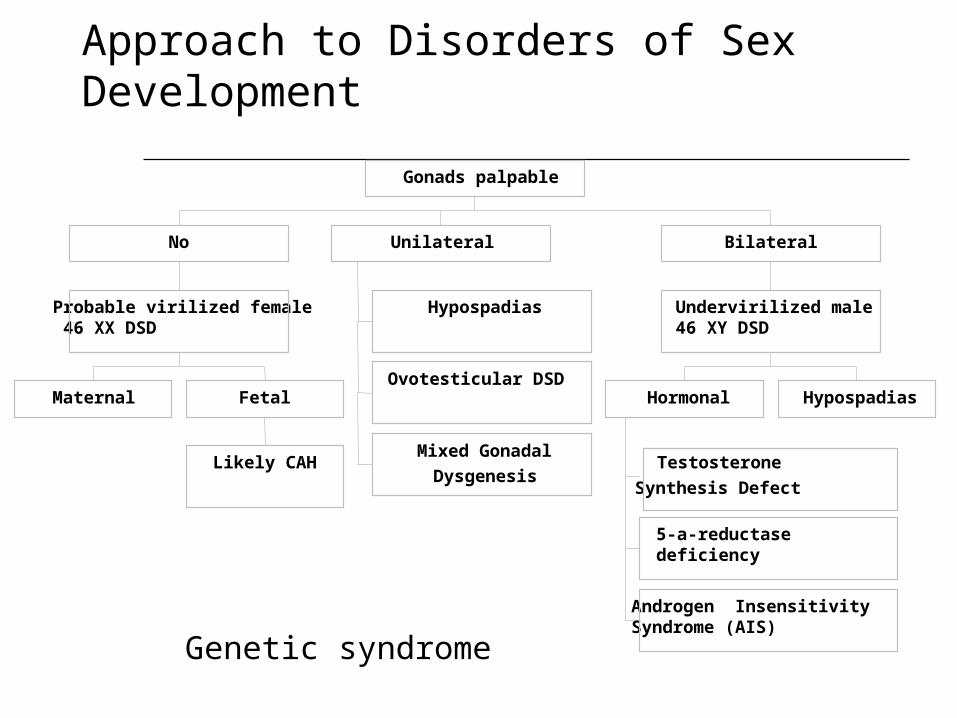
Approach to Disorders of Sex Development
Maternal
Likely CAH
Fetal
Probable virilized female 46 XX DSD
No
Hypospadias
Ovotesticular DSD
Mixed Gonadal
Dysgenesis
Unilateral
Testosterone
Synthesis Defect
5-a-reductase deficiency
Androgen Insensitivity Syndrome (AIS)
Hormonal Hypospadias
Undervirilized male46 XY DSD
Bilateral
Gonads palpable
Genetic syndrome
Type 1 Diabetes

Epidemiology of Type 1
Prevalence 0.4% of individuals < 18 years
Increased risk to family membersSibling 5%Father with diabetes 6-8%Mother with diabetes 2-3%Identical twin 30-50%

Diagnostic Criteria FBG > 7.0 mmol/L OR
Casual BG > 11.1 with symptoms OR
2 hour BG in OGTT of > 11.1
Pediatrics: do not need confirmatory sample on another day in the presence of unequivocal hyperglycemia and symptoms.

BG Targets
Age (years) Premeal target
(mmol/L)
HbA1c Target (%)
< 5 6-12 < 8.5%
6-12 4-10 < 8.0%
>12 4-7 < 7.0%
DKA: How common is it?
At diagnosis of diabetes 15-67% present with DKA
Established diabetes 1-10% of patients/year
Cerebral edema 0.4-1% of episodes of DKA 25% mortality, up to 35% with severe
neurologic deficits

Cerebral Edema in DKA
Who is at risk? Increased risk in new onset DM, more
dehydrated and acidotic patients ?treatment factors – rapid infusion of hypo-
osmolar fluids, use of bicarbonate
Treatment – early intervention is key Raise HOB, + intubate, reduce fluids hypertonic saline, mannitol

DKA: What you need to remember
The best way to prevent CE-DKA is to prevent DKA
How do you prevent cerebral edema once child presents in DKA? By remembering a few guiding principles:
The younger the child, the greater the risk
No insulin bolus No fluid bolus, unless in shock (max 10
cc/kg over 20-30 minutes)
Question:
An 8 yo girl is diagnosed with Type 1 diabetes. At what age should you begin screening for:
a) Microalbuminuria b) Retinopathyc) Hypothyroidismd) Hyperlipidemiae) Celiac disease
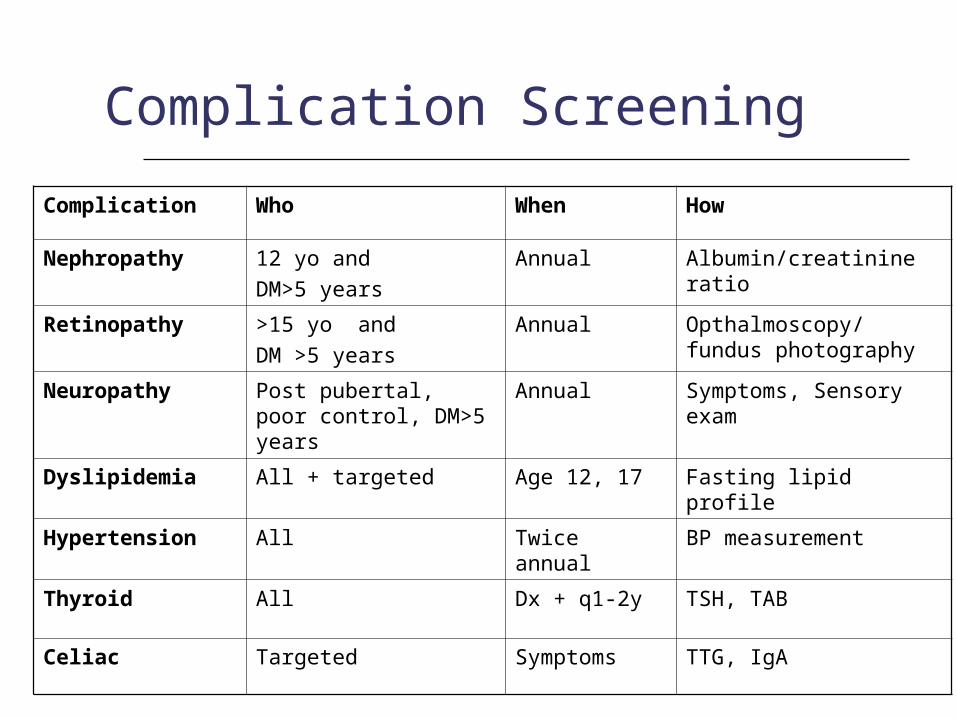
Complication Screening
Complication Who When How
Nephropathy 12 yo and DM>5 years
Annual Albumin/creatinine ratio
Retinopathy >15 yo and DM >5 years
Annual Opthalmoscopy/ fundus photography
Neuropathy Post pubertal, poor control, DM>5 years
Annual Symptoms, Sensory exam
Dyslipidemia All + targeted Age 12, 17 Fasting lipid profile
Hypertension All Twice annual BP measurement
Thyroid All Dx + q1-2y TSH, TAB
Celiac Targeted Symptoms TTG, IgA
Type 2 Diabetes in Children and Youth
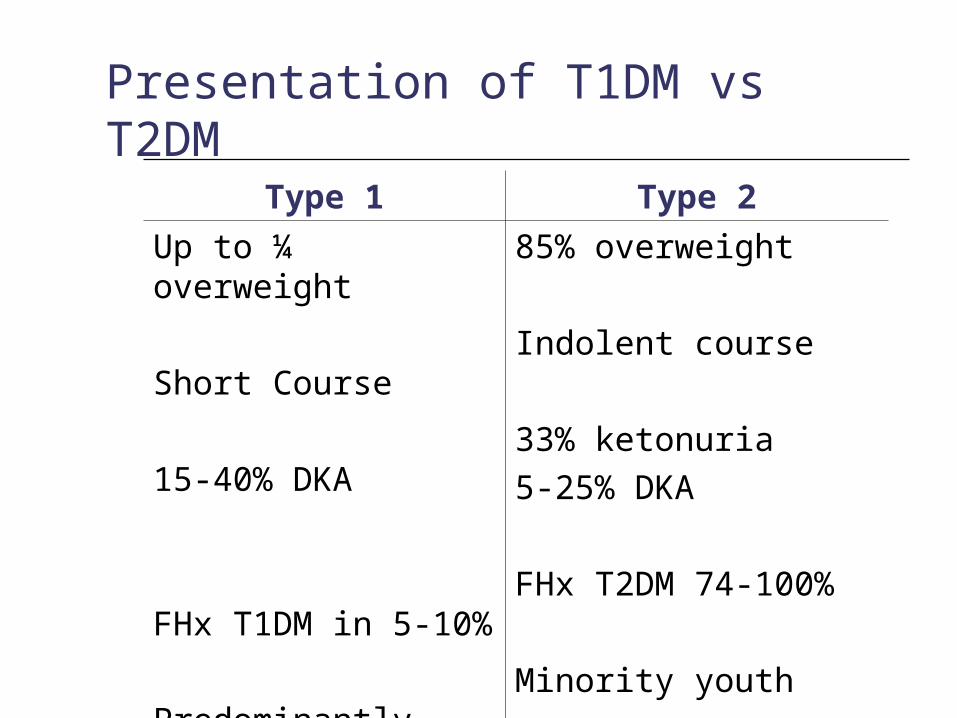
Presentation of T1DM vs T2DM Type 1 Type 2
Up to ¼ overweight
Short Course
15-40% DKA
FHx T1DM in 5-10%
Predominantly white
85% overweight
Indolent course
33% ketonuria5-25% DKA
FHx T2DM 74-100%
Minority youth
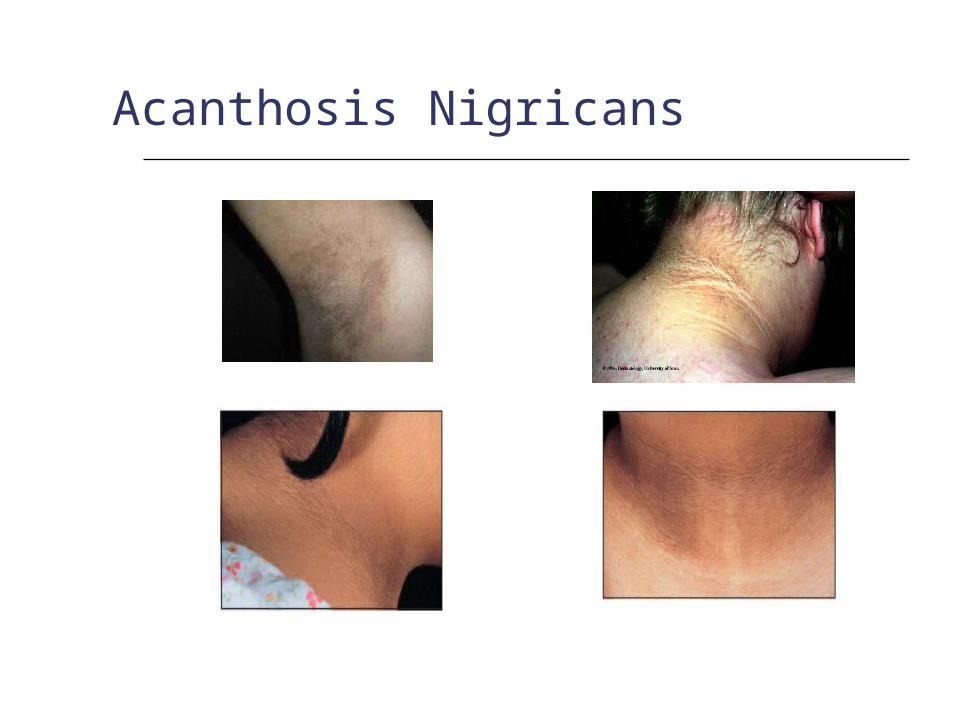
Acanthosis Nigricans
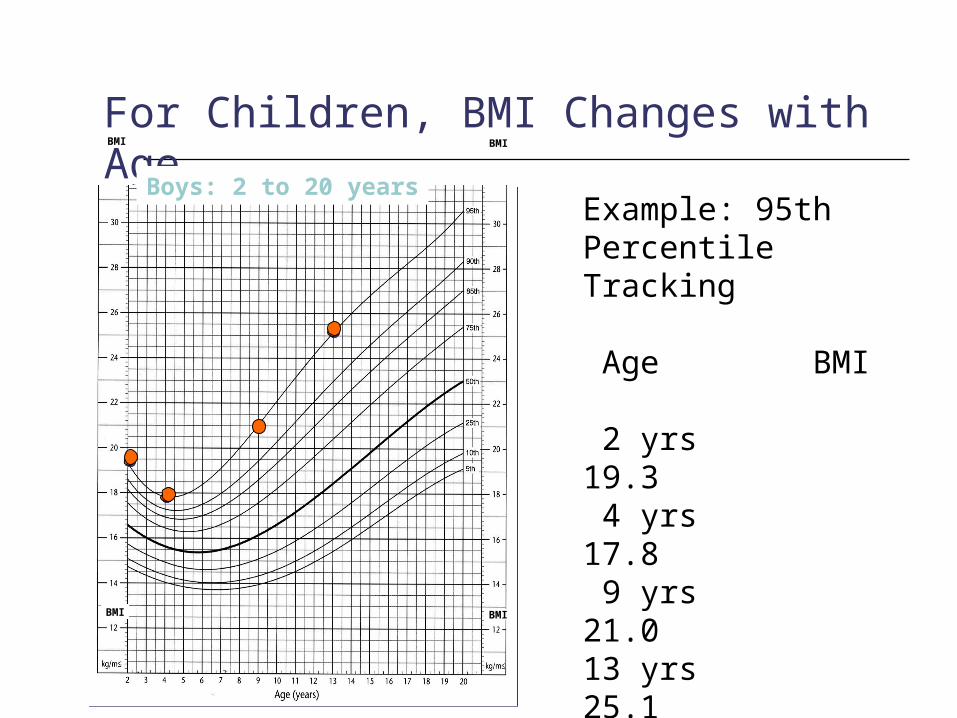
Example: 95th Percentile Tracking Age BMI
2 yrs 19.3 4 yrs 17.8 9 yrs 21.013 yrs 25.1
For Children, BMI Changes with Age
Boys: 2 to 20 years
BMI BMI
BMI BMI

Genetic and Environmental Risk factors for T2DM
Ethnicity Female gender Family history T2DM Intrauterine factors
Maternal history of gestational diabetes Large for gestational age (>4 kg) Small for gestational age (<2.5 kg)
Obesity Sedentary behaviour

Question
A 13 year old boy with a BMI of 30, acanthosis nigricans, and a family history of Type 2 diabetes presents with a random glucose of 15 mmol/L, negative ketones.
A What is the medication of first choice?
B What is the target A1c?

Treatment of T2DM in Youth Diabetes education for the family Setting glycemic targets
HbA1c < 7.0% Lifestyle modification
<10% achieve glycemic targets Pharmacotherapy
Metformin has been shown to have short term efficacy and safety in adolescents
Insulin rescue is required in those with severe metabolic decompensation at diagnosis
e.g. DKA, A1C ≥9.0%, symptoms of severe hyperglycemia, ketonuria

Thyroid Disorders

Approach to Goitre
+ve
Chronic lymphocytic
thyroiditis
-ve
Goitrogen,
Dyshormonogenesis
Thyroid Antibodies
Elevated
Hypothyroid
+ve
Chronic lymphocytic
thyroiditis
-ve
Colloid goitre
Thyroid Antibodies
Normal
Euthyroid
Grave's disease,Subacute thyroiditis
Toxic nodule
Thyroid Antibodies
Suppressed
Hyperthyroid
TSH
Goitre

Thyroid take home points Thyroid disorders are common in
children and adolescents
Most commonly present with goitre secondary to autoimmune thyroiditis or a simple colloid goitre
TSH and thyroid antibodies is usually all that is required to establish the diagnosis

Thyroid take home points Mild elevations of TSH should be verified
on repeat testing TSH <10mU/L often normal on repeat
Routine monitoring – q6 months while growing, q year once adult height
Natural history studies suggest a high rate of spontaneous resolution with autoimmune thyroid disease and thus, repeat testing should be done before committing to lifelong thyroid hormone replacement
Thyroid take home points
Congenital hypothyroidism detected through newborn screening – they need more intensive monitoring particularly in the 1st 3 years of life
Questions?







