Download - Pharmacological management Insulin

Slides current until 2008
Pharmacological managementInsulin

Insulin managementCurriculum Module III-3
Slide 2 of 41
Slides current until 2008
Insulin
• A hormone secreted by the beta cells
• Secreted in response to glucose or other stimuli, such as amino acids
• Normal response characterized by low basal levels of insulin, with surges of insulin triggered by a rise in blood glucose
Insu
lin
60
0
20
40
Breakfast Lunch Supper
Insulin managementCurriculum Module III-3
Slide 3 of 41
Slides current until 2008
Insulin action
1. Increases glucose uptake, particularly in muscle, liver and adipose tissue
2. Suppresses glucose output from the liver
3. Increases formation of fat
4. Inhibits breakdown of fats
5. Promotes amino-acid uptake and prevents protein breakdown

Insulin managementCurriculum Module III-3
Slide 4 of 41
Slides current until 2008
Indications for insulin therapy
• Type 1 diabetes
• Women with diabetes who become pregnant or are breastfeeding
• Transiently in type 2 diabetes in special situations
• In type 2 diabetes, inadequately controlled on glucose-lowering medicines (secondary failure)

Insulin managementCurriculum Module III-3
Slide 5 of 41
Slides current until 2008
Insulin therapy
• Insulin therapy aims to replicate the normal physiological insulin response
• Insulin regimens should be individualized
– type of diabetes
– willingness to inject
– lifestyle
– blood glucose monitoring
– age
– dexterity
– glycaemic targets

Insulin managementCurriculum Module III-3
Slide 6 of 41
Slides current until 2008
Insulin types and actionOnset (hrs) Peak (hrs) Duration (hrs)
Rapidlispro aspart
<¼ ¾-2½ 3½-4½
Shortsolubleregular
½-1 2-4 6-8
IntermediateNPHlente
1-21-3
6-12 6-12
18-24 18-24
Long actingultralente glarginedetemir
4-63-41-2
8-20 3-243-8
24 or more≥24 or more 12-24 (dose-dependent)

Insulin managementCurriculum Module III-3
Slide 7 of 41
Slides current until 2008
International labeling
www.idf.org

Insulin managementCurriculum Module III-3
Slide 8 of 41
Slides current until 2008
Variability in insulin absorption

Insulin managementCurriculum Module III-3
Slide 9 of 41
Slides current until 2008
Factors affecting absorption
• Lipohypertrophy
• Dose of injection
• Site and depth of injection
• Exercise
• Ambient and body temperature
• Insulin type
• Incomplete re-suspension

Insulin managementCurriculum Module III-3
Slide 10 of 41
Slides current until 2008
• What is the most common insulin regimen used in your country?
• How well do you think it works?
• How do people accept insulin?
ACTIVITY
Insulin managementCurriculum Module III-3
Slide 11 of 41
Slides current until 2008
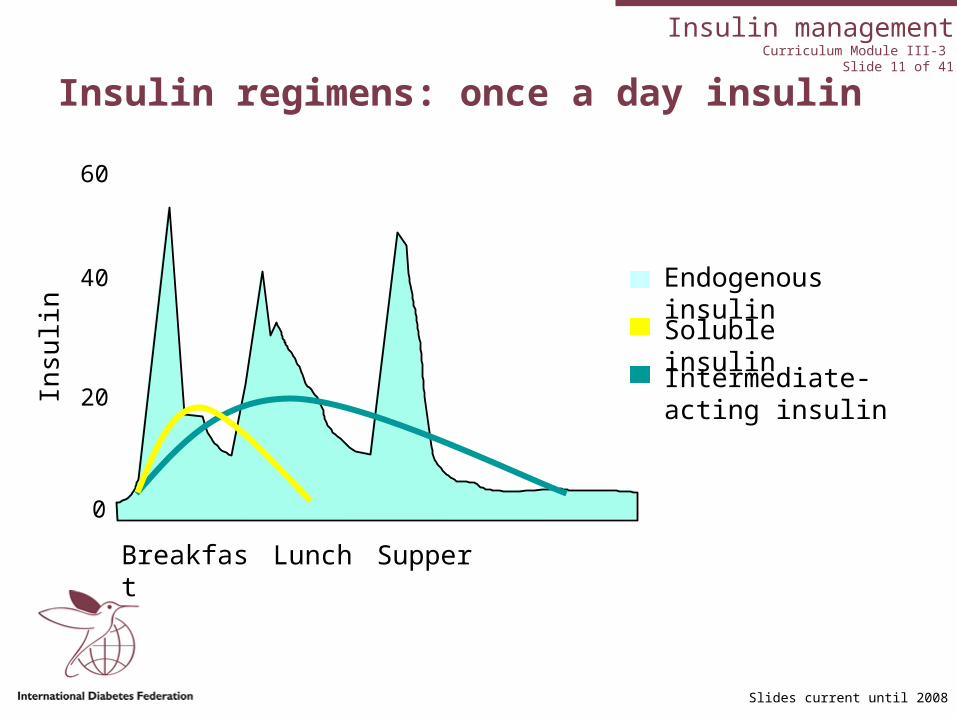
Insulin regimens: once a day insulin
Soluble insulin
Intermediate-acting insulin
Insu
lin
60
0
20
40
Breakfast Lunch Supper
Endogenous insulin
Insulin managementCurriculum Module III-3
Slide 12 of 41
Slides current until 2008
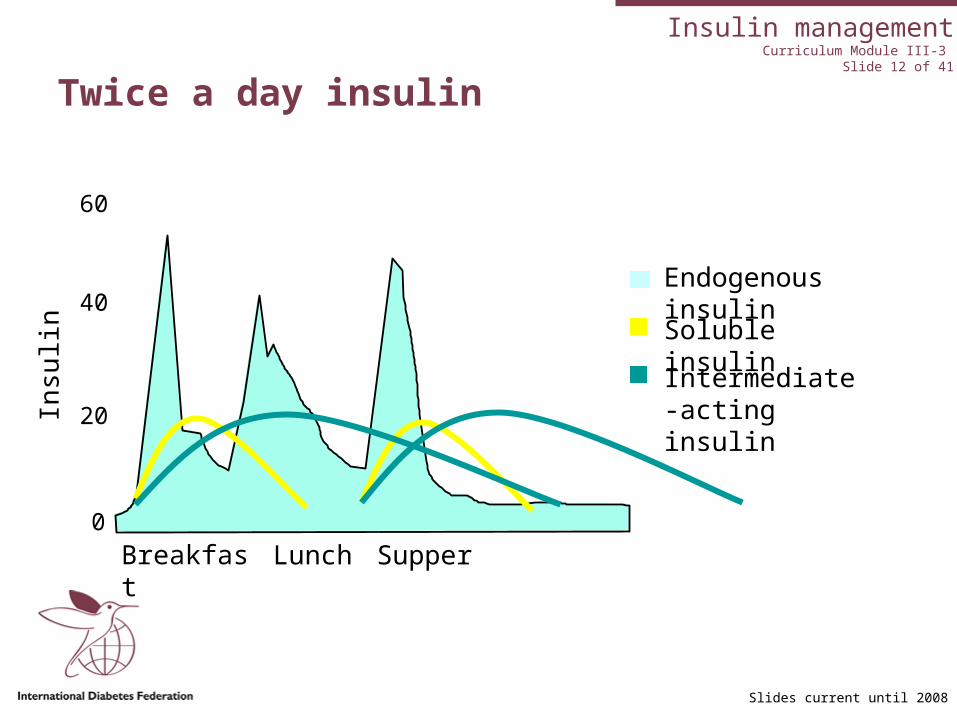
Twice a day insulin
Soluble insulin
Intermediate-acting insulinIn
sulin
60
0
20
40Endogenous insulin
Breakfast Lunch Supper

Insulin managementCurriculum Module III-3
Slide 13 of 41
Slides current until 2008
Three times a day insulin
Soluble insulin
Intermediate-acting insulin
Insu
lin
60
0
20
40 Endogenous insulin
Breakfast Lunch Supper
Insulin managementCurriculum Module III-3
Slide 14 of 41
Slides current until 2008
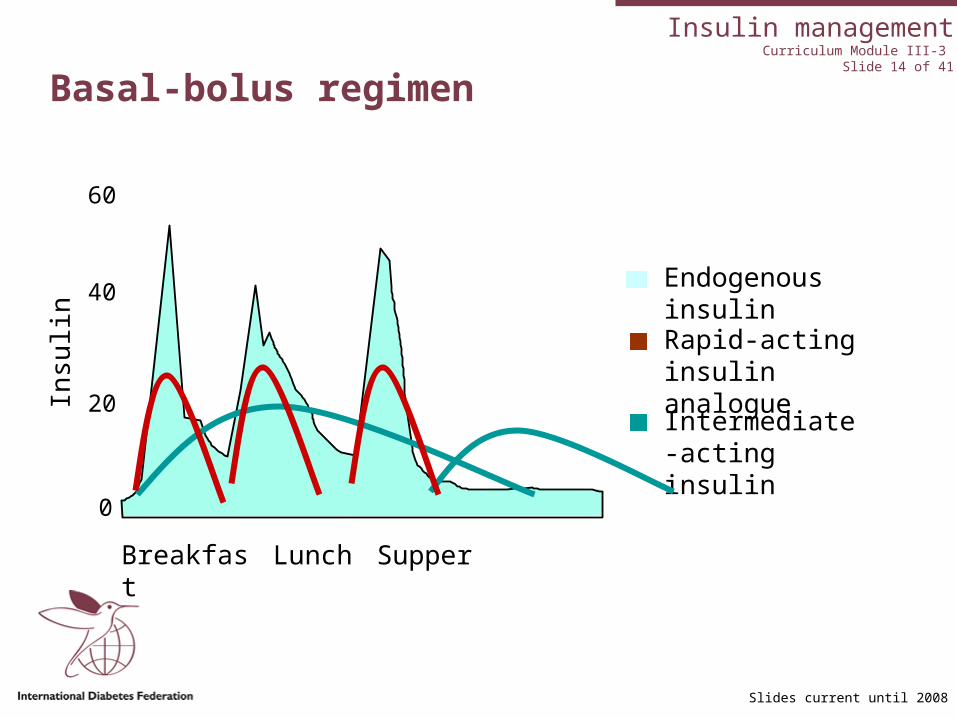
Rapid-acting insulin analogue
Intermediate-acting insulin
Basal-bolus regimenIn
sulin
60
0
20
40 Endogenous insulin
Breakfast Lunch Supper

Insulin managementCurriculum Module III-3
Slide 15 of 41
Slides current until 2008
Long-acting insulin analogue
Long-acting insulin analogues
Rapid-acting insulin analogue
Insu
lin
60
0
20
40 Endogenous insulin
Breakfast Lunch Supper

Insulin managementCurriculum Module III-3
Slide 16 of 41
Slides current until 2008
Commencing insulin therapy
• Insulin should never be used as a threat
• Fear of injecting is common; needle phobia is rare
• Healthcare professional’s attitude is key to acceptance
• People should be praised and encouraged to promote a positive attitude
• Blood test is more painful than insulin injection
• Forget the oranges; just do it!
Insulin managementCurriculum Module III-3
Slide 17 of 41
Slides current until 2008
Commencing insulin therapy
• Starting dose will depend on many factors– age– weight– type and duration of diabetes– glycaemic targets
• In type 2 diabetes, consider continuing maximum tolerated oral glucose-lowering medicines– 10 units of intermediate-acting
insulin once a day

Insulin managementCurriculum Module III-3
Slide 18 of 41
Slides current until 2008
Injecting insulin
• Should be given into subcutaneous tissue
• Skin of a very thin person may have to be gently pinched
• Insulin at room temperature less painful
• Needle can be inserted at 45-90º
– 45º for very thin people
– 90º for overweight people or when using short needle
• Swabbing with alcohol is not necessary

Insulin managementCurriculum Module III-3
Slide 19 of 41
Slides current until 2008
Insulin devices
Syringe and needle • Usually disposable, intended for
one injection only• May need to use doses divisible
by 5 or 10 if visually impaired
Pens • Easy to use• Loading pen may be difficult for
elderly• Disposable pens

Insulin managementCurriculum Module III-3
Slide 20 of 41
Slides current until 2008
Insulin devices
Pumps• Insulin delivered every few
minutes over 24 hours• Require large commitment
Inhaled insulin• For bolus doses only• Large device• Unknown long-term effects on
lungs

Insulin managementCurriculum Module III-3
Slide 21 of 41
Slides current until 2008
HbA1c Pre-meal 2 hours post-meal
Target for most people with diabetes
<7% 4-7mmol/L*
90-130 mg/dl*1
5-10mmol/L*
<180mg/dl*1
IDF Global guideline for Type 2 diabetes*2
<6.5% <6.0mmol/L
<110mg/dl
<8.0mmol/L
<145mg/dl
Adjusting insulin – what are the targets?
*CDA 2003, *1ADA 2004, *2 IDF 2005
• Treatment targets should be individualized, especially for very young and very old
• Absence of hypoglycaemia

Insulin managementCurriculum Module III-3
Slide 22 of 41
Slides current until 2008
Starting insulin in type 2 diabetes
FINFAT: start small dose intermediate- acting insulin at night
• Aim for target fasting levels first
• Adjust by 2-4 units or 10%
• Second injection only added once fasting targets reached

Insulin managementCurriculum Module III-3
Slide 23 of 41
Slides current until 2008
Adjusting insulin
Pattern management
• Watch levels for 2-3 days
• Address hypoglycaemia first
• Aim for target fasting levels next
• Adjust by 2-4 units or 10%
• Wait 2-3 days

Insulin managementCurriculum Module III-3
Slide 24 of 41
Slides current until 2008
Adjusting insulin
• Flexible dose guideline
• Eating more
• Exercising more
• Insulin to carbohydrate ratio
• Evaluate with next blood glucose
• Tailored to individual needs

Insulin managementCurriculum Module III-3
Slide 25 of 41
Slides current until 2008
Which insulin to adjust when?
Blood glucose Insulin to be changed
Fasting Bedtime or supper intermediate- or long-acting
Post-breakfast Morning short- or rapid-acting insulin
Pre-lunch Morning intermediate-acting insulin
Post-lunch Morning intermediate-acting insulin or lunchtime short- or rapid-acting insulin
Pre-supper (dinner) Morning intermediate-acting insulin
Post-supper (dinner) Supper-time short- or rapid-acting insulin
During the night Supper-time or bedtime intermediate-acting

Insulin managementCurriculum Module III-3
Slide 26 of 41
Slides current until 2008
Insulin practicalities
Timing• Soluble insulin: 30-45 minutes pre-
meal• Short-acting insulin analogues: no
more than 15 minutes pre-meal and can be given post-meal
• Intermediate- or long-acting insulins do not have to be given in relation to a meal

Insulin managementCurriculum Module III-3
Slide 27 of 41
Slides current until 2008
Storage• One month in fridge or at room
temperature once the vial has been opened
• Must never be frozen• Store away from source of heat• If refrigeration not available store
in clay pot or hole in ground• May be damaged by direct
sunlight or vigorous shaking
Insulin practicalities

Insulin managementCurriculum Module III-3
Slide 28 of 41
Slides current until 2008
• Insulin strength may differ (U40, U100, U500)
• Ensure that the syringe matches the strength!
• Long-acting insulin analogues are clear in appearance
• Identify and differentiate insulin type
Precautions

Insulin managementCurriculum Module III-3
Slide 29 of 41
Slides current until 2008
Mixing insulins
• NPH and soluble insulins can be mixed without changing properties
• Check with the manufacturer before mixing any other insulins
• Pre-drawn syringes can be kept in fridge (2-80 C or 36-460 F) for one month

Insulin managementCurriculum Module III-3
Slide 30 of 41
Slides current until 2008
Side effects
• Hypoglycaemia
• Weight gain
• Lipohypertrophy
• Lipoatrophy
• Insulin oedema
• Allergic reaction

Insulin managementCurriculum Module IV-1
Slide 31 of 41ACTIVITY
Slides current until 2008
Insulin: NPH 25 units, Reg. 10 units before breakfast
NPH 15 units, Reg. 10 units before supper
Pre-breakfastmmol/L (mg/dl)
Pre-lunch Pre-supper
2 hours post-supper
Day 1 10.4 (187) 6.5 (117) 7.0 (126) 9.2 (165)
Day 2 9.6 (172) 5.4 (97) 6.8 (122) 10.2 (183)
Day 3 11.0 (198) 6.2 (112) 6.5 (117) 8.8 (158)
Example 1
Insulin managementCurriculum Module IV-1
Slide 32 of 41ACTIVITY
Slides current until 2008
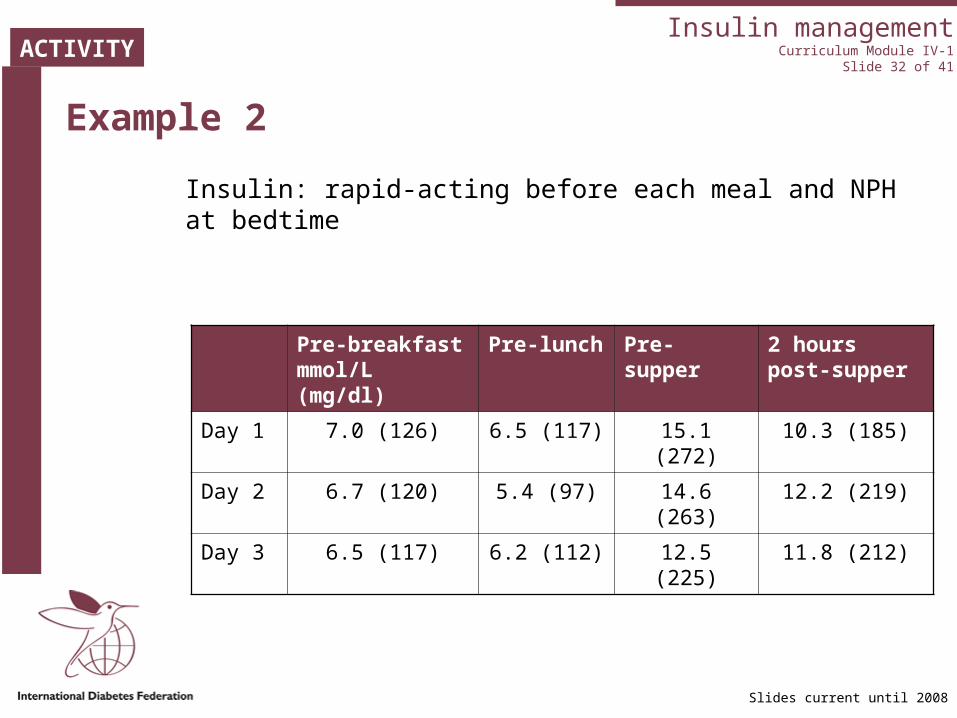
Example 2
Insulin: rapid-acting before each meal and NPH at bedtime
Pre-breakfast mmol/L (mg/dl)
Pre-lunch Pre-supper
2 hours post-supper
Day 1 7.0 (126) 6.5 (117) 15.1 (272) 10.3 (185)
Day 2 6.7 (120) 5.4 (97) 14.6 (263) 12.2 (219)
Day 3 6.5 (117) 6.2 (112) 12.5 (225) 11.8 (212)

Insulin managementCurriculum Module III-3
Slide 33 of 41
Slides current until 2008
What would you advise if….
1. The insulin had been taken and the restaurant meal was late
2. Regular insulin should be taken before a meal but the pre-meal blood glucose is 3.5 mmol/L (63 mg/dl)
3. A tennis match is scheduled an hour after lunch
4. A person wakes up nauseated and does not want to eat
5. Blood glucose levels do not coincide with how a person feels
ACTIVITY

Insulin managementCurriculum Module III-3
Slide 34 of 41
Slides current until 2008
Summary
• All people with type 1 diabetes must be treated with insulin
• The majority of people with type 2 diabetes will need insulin within 5 to 10 years of diagnosis
• Insulin therapy should not be used as a threat
• Insulin regimens should be individualized • Insulin should be adjusted to achieve
blood glucose as close to target range as possible
Insulin managementCurriculum Module III-3
Slide 35 of 41
Slides current until 2008
Review question
1. One advantage that rapid-acting insulin has over regular insulin is that it:
a. Must be given immediately after the meal
b. Does not have to be kept in the fridge
c. Does not need a basal insulin to be given as well
d. Has a short and predictable action time

Insulin managementCurriculum Module III-3
Slide 36 of 41
Slides current until 2008
Review question
2. Which of the following does not affect the absorption of insulin?
a. The temperature of the insulinb. The temperature of the area to be
injectedc. The amount of insulin to be
injectedd. The type of injection device, i.e.
pen or syringe

Insulin managementCurriculum Module III-3
Slide 37 of 41
Slides current until 2008
Review question
3. Jonathan says his doctor has suggested he take insulin four times a day. He asks if this is not going to be too much insulin. What is your best response?
a. It is not possible to take too much insulin, you just have to eat more
b. The action of insulin taken four times a day is closest to the action of endogenous insulin
c. Taking insulin four times a day will be very difficult, and the results will not be much better
d. Your doctor feels that taking insulin four times a day will make you pay more attention to your diabetes
Insulin managementCurriculum Module III-3
Slide 38 of 41
Slides current until 2008
Review question
4. Suleen has been on insulin twice a day – a mixture of intermediate and soluble in the morning, and again before dinner. Her records show that her fasting levels are 10-12mmol/L (180-216mg/dl), but the rest of the day, her levels are less than 8.5mmol/L (153mg/dl). What change(s) would you suggest to her insulin regimen to improve her levels?
a. Suggest she eats less at dinner and more at lunch
b. Suggest she increases her soluble before dinnerc. Suggest she increases her intermediate before
dinnerd. Suggest she moves her intermediate to bedtime
and decrease her soluble in the morning

Insulin managementCurriculum Module III-3
Slide 39 of 41
Slides current until 2008
Review question
5. The goal of bedtime insulin in the person with type 2 diabetes who is on oral blood glucose-lowering medicines is to:
a. Provide insulin to cover the bedtime snack
b. Reduce the fasting glucose level
c. Reduce the number of oral blood glucose-lowering medicines
d. Prevent hypoglycaemia during the night

Insulin managementCurriculum Module III-3
Slide 40 of 41
Slides current until 2008
Answers
1. d
2. d
3. b
4. d
5. b
Insulin managementCurriculum Module III-3
Slide 41 of 41
Slides current until 2008
References
1. Klingensmith GJ, Ed. Intensive Diabetes Management, 3rd ed. Virginia: American Diabetes Association, 2003.
2. Colwell JA. Hot Topics Diabetes. Philadelphia: Hanley & Belfus, 2003.
3. American Diabetes Association. Insulin Administration. Diabetes Care 2004; 27(Suppl 1): S106-109.
4. Davidson MB. Diabetes Mellitus Diagnosis and Treatment. 4th ed. Philadelphia: W.B. Saunders Company, 1998.
5. Ilkova H, Glaser B, Tunckale A, Bagriacik N, Cerasi E. Induction of long-term glycemic control in newly diagnosed type 2 diabetic patients by transient intensive insulin treatment. Diabetes Care 1997; 20: 1353-6.
6. Nathan DM. Initial management of glycemia in Type 2 diabetes mellitus. N Engl J Med 2002; 347: 1342-9.
7. Canadian Diabetes Association Clinical Practice Guidelines Expert Committee. Canadian Diabetes Association 2003 Clinical Practice Guidelines for the Prevention and Management of Diabetes in Canada. Canadian Journal of Diabetes 2003; 27(suppl 2).
8. Olsson P-O, Hans A, Henning VS. Miscibility of human semisynthetic regular and lente insulin and human biosynthetic, regular and NPH insulin. Diabetes Care 1987; 10: 473-7.
9. IDF Clinical Guidelines Task Force. Global Guidelines for Type 2 diabetes. Brussels: International Diabetes Federation, 2005.







