
18 mars – Académie Nationale de Pharmacie
P. Déchelotte
CHU Rouen, INSERM UMR 1073, Normandie Université
Pharmacologie nutritionnelle
en réanimation
U 1073
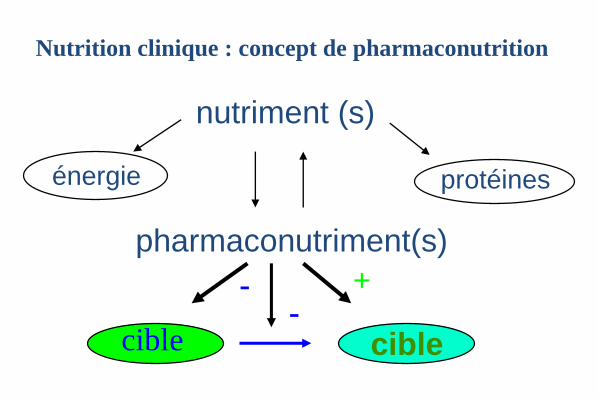
nutriment (s)
pharmaconutriment(s)
énergie protéines
cible cible
+--
Nutrition clinique : concept de pharmaconutrition
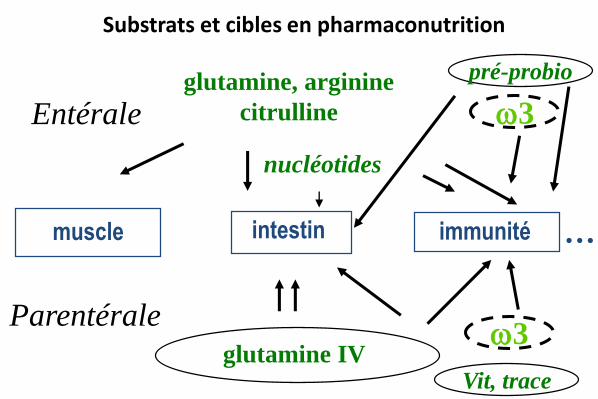
Substrats et cibles en pharmaconutrition
muscle intestin immunité
glutamine IV
3
nucléotides
pré-probio
…
3
Entérale
Parentérale
glutamine, arginine
citrulline
Vit, trace
Domaines d’application de la pharmaconutrition
périopératoire, chirurgie majeure du cancer
traumatologie, brûlé
réanimation médicale, chirurgie compliquée
inflammation intestinale
cachexie, chimiothérapie, escarres, sujet âgé…
Pharmaconutrition entérale
dans la chirurgie pour cancer
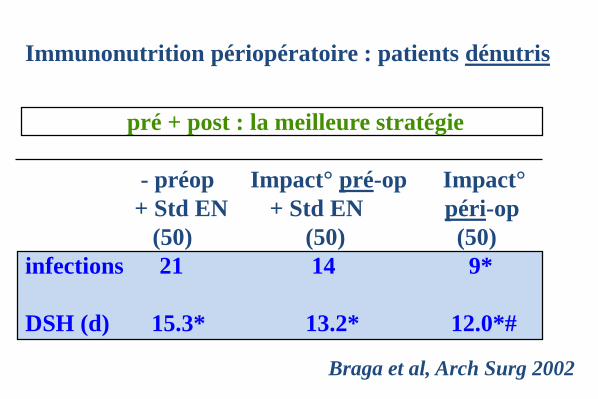
Immunonutrition périopératoire : patients dénutris
Braga et al, Arch Surg 2002
pré + post : la meilleure stratégie
- préop Impact° pré-op Impact°
+ Std EN + Std EN péri-op
(50) (50) (50)
infections 21 14 9*
DSH (d) 15.3* 13.2* 12.0*#
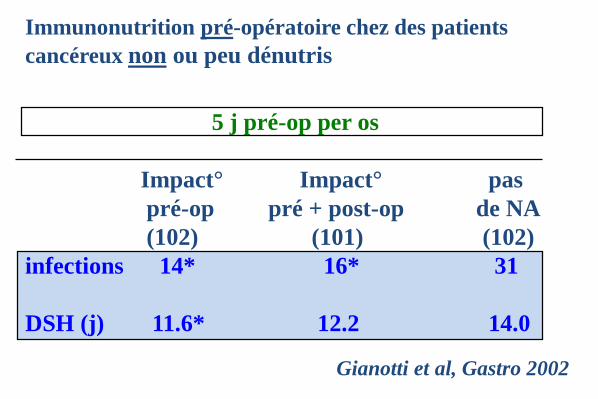
Immunonutrition pré-opératoire chez des patients
cancéreux non ou peu dénutris
Gianotti et al, Gastro 2002
5 j pré-op per os
Impact° Impact° pas
pré-op pré + post-op de NA
(102) (101) (102)
infections 14* 16* 31
DSH (j) 11.6* 12.2 14.0
Immunonutrition : méta-analyses
Beale 1997, Heys 1999, Heyland 2001,
Waitzberg 2006…
chirurgie pour cancer digestif: réduction
significative de la durée de séjour et de
l’incidence des complications infectieuses
recommandations canadiennes, italiennes,
espagnoles, française (SFC), européennes
(ESPEN, grade A); remboursement
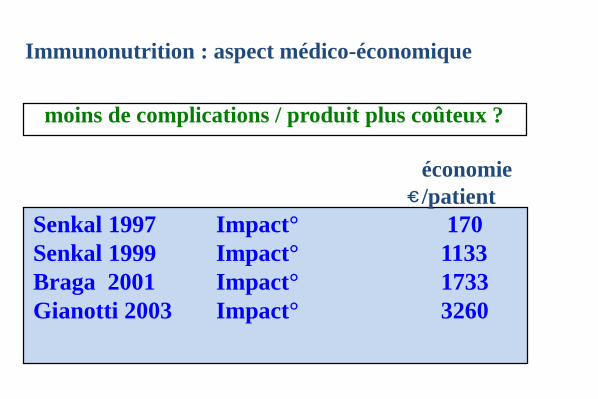
Immunonutrition : aspect médico-économique
moins de complications / produit plus coûteux ?
économie
/patient
Senkal 1997 Impact° 170
Senkal 1999 Impact° 1133
Braga 2001 Impact° 1733
Gianotti 2003 Impact° 3260
c
Pharmaconutrition entérale : en résumé
• périopératoire, chirurgie majeure programmée (cancer) avec arg, n-3, nucléotides : A
• chirurgie cardiaque: évidence faible• polytrauma: glutamine A• brûlé grave: glutamine A, vit & trace A• réanimation médicale : risque ? (arg, omega-3)• chimiothérapie, escarres, sujet âgé, inflammation
intestinale, cachexie : en devenir…
Pharmaconutrition parentérale :
• Glutamine IV (dipeptide)
• Emulsions lipidiques enrichies en omega-3
• Eléments trace : Se, Zn
Pharmaconutrition parentérale :
Bénéfices de la glutamine IV (sous forme d’alanyl-glutamine)
quand le patient nécessite une NP
• Périopératoire - chirurgie majeure programmée pour cancer
• Pancréatites aigüe sévères
• Réanimation médicale et chirurgicale
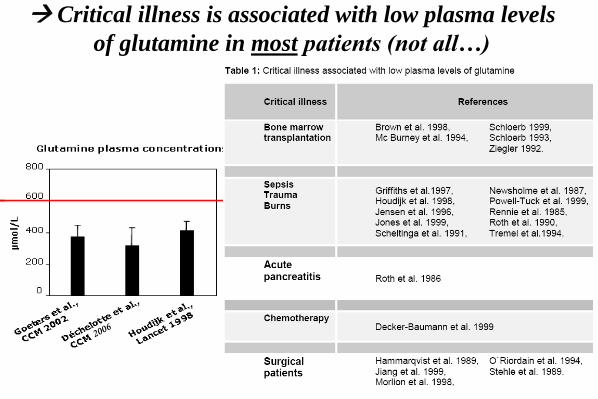
Critical illness is associated with low plasma levels
of glutamine in most patients (not all…)
• Novak 2002, Wang et al, 2010 , Chao Yue 2013 :
meta-analysis of RCTs
significant reduction of length of hospital stay
(p<0.001)
significant reduction of infectious complications
(p=0.02)
Benefits of Gln-dipeptide supplemented PN in
surgical patients
(0.2-0.35 g/kg bw/day dipeptide)
Cancer patients undergoing major
surgery
Severe pancreatitis
Complicated surgery, ICU patients
IV Glutamine-TPN: patients groups
Glutamine-TPN in acute pancreatitis :
(0.2-0.35 g/kg bw/day dipeptide)
Ockenga et al, Clin Nutr 2002
• reduced acute-phase response and better lymphocyte
proliferation
• reduced length of hospital stay (21 vs 25 days)
(11 vs 16 days)
De Beaux, Nutrition 1998
Hadju et al, Mag Seb 2012
• less infections and reinterventions
• less patients with complications
• lower incidence of complications, prevention of
pancreatic infections
metanalysis: reduced infections, LOS, mortality
risk
Glutamine-TPN in acute pancreatitis :
Fuentes-Orozco et al, JPEN 2008
Sahin et al , Eur J Clin Nutr 2007
He et al , Clin Nutr Suppl 2004
Asrani et al, Pancreatology 2013
Jafari et al, Clin Nutr 2014
Cancer patients undergoing major
surgery
Severe pancreatitis
Complicated surgery, ICU patients
IV Glutamine-TPN: patients groups
The french Dipeptiven study
Studies with IV glutamine + TPN in ICU :
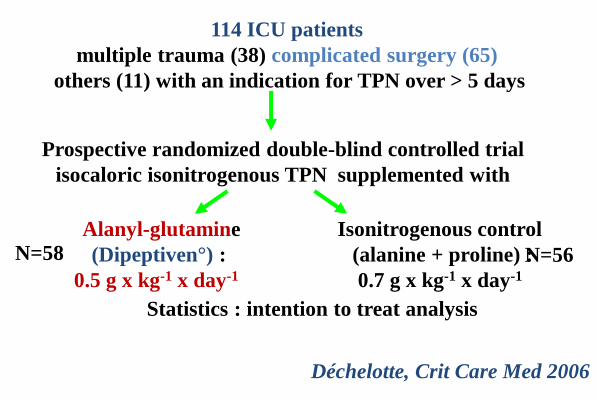
114 ICU patients
multiple trauma (38) complicated surgery (65)
others (11) with an indication for TPN over > 5 days
Prospective randomized double-blind controlled trial
isocaloric isonitrogenous TPN supplemented with
Statistics : intention to treat analysis
Alanyl-glutamine
(Dipeptiven°) :
0.5 g x kg-1 x day-1
N=58 N=56
Isonitrogenous control
(alanine + proline) :
0.7 g x kg-1 x day-1
Déchelotte, Crit Care Med 2006
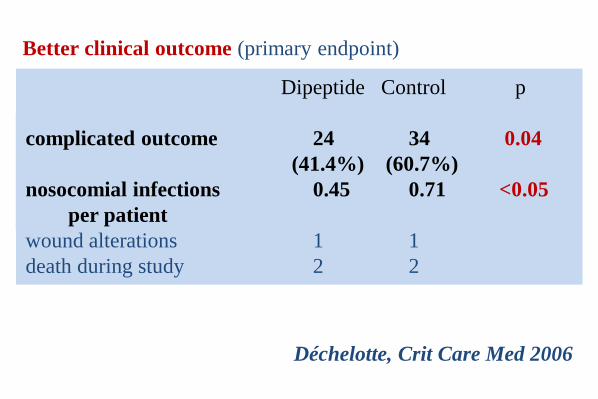
Better clinical outcome (primary endpoint)
Dipeptide Control p
complicated outcome 24 34 0.04
(41.4%) (60.7%)
nosocomial infections 0.45 0.71 <0.05
per patient
wound alterations 1 1
death during study 2 2
Déchelotte, Crit Care Med 2006
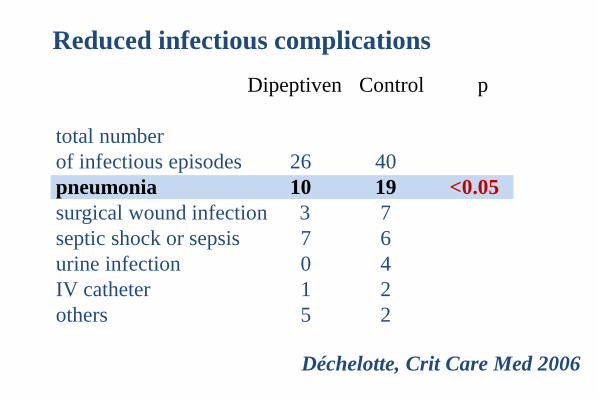
Reduced infectious complications
Dipeptiven Control p
total number
of infectious episodes 26 40
pneumonia 10 19 <0.05
surgical wound infection 3 7
septic shock or sepsis 7 6
urine infection 0 4
IV catheter 1 2
others 5 2
Déchelotte, Crit Care Med 2006
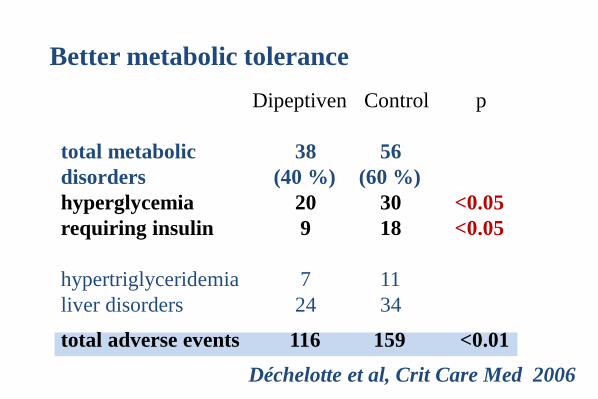
Better metabolic tolerance
Dipeptiven Control p
total metabolic 38 56
disorders (40 %) (60 %)
hyperglycemia 20 30 <0.05
requiring insulin 9 18 <0.05
hypertriglyceridemia 7 11
liver disorders 24 34
total adverse events 116 159 <0.01
Déchelotte et al, Crit Care Med 2006
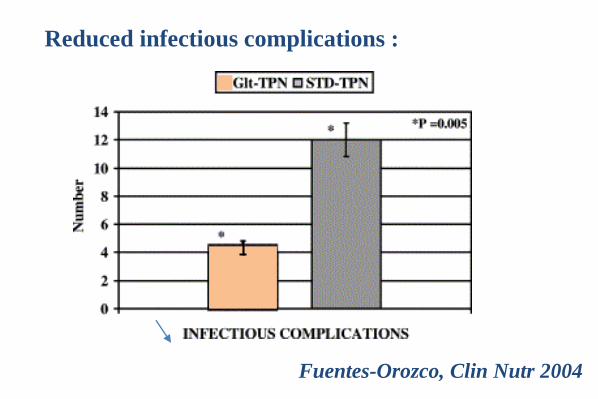
Fuentes-Orozco, Clin Nutr 2004
Reduced infectious complications :
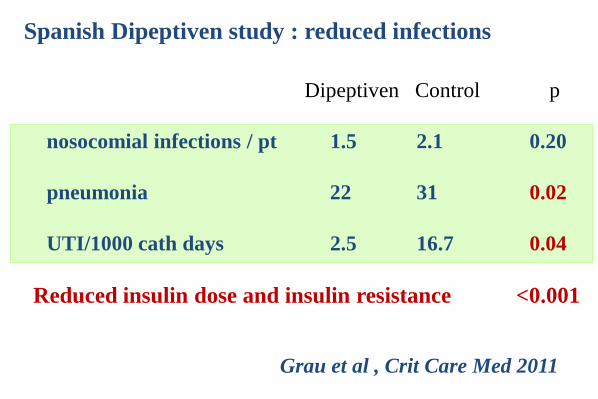
Dipeptiven Control p
nosocomial infections / pt 1.5 2.1 0.20
pneumonia 22 31 0.02
UTI/1000 cath days 2.5 16.7 0.04
Reduced insulin dose and insulin resistance <0.001
Grau et al , Crit Care Med 2011
Spanish Dipeptiven study : reduced infections
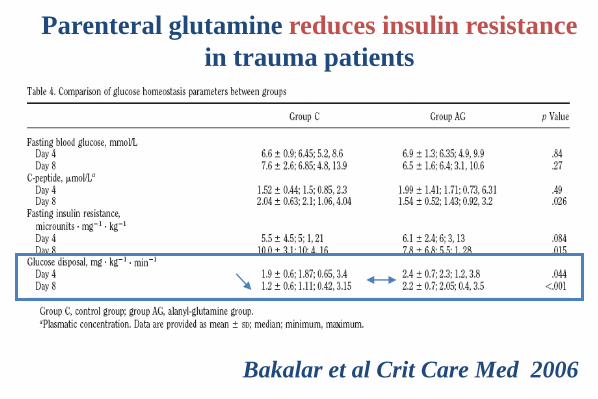
Parenteral glutamine reduces insulin resistance
in trauma patients
Bakalar et al Crit Care Med 2006
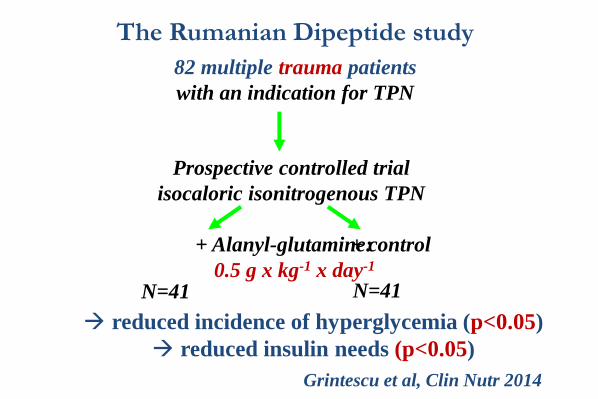
The Rumanian Dipeptide study
82 multiple trauma patients
with an indication for TPN
Prospective controlled trial
isocaloric isonitrogenous TPN
+ Alanyl-glutamine:
0.5 g x kg-1 x day-1
N=41 N=41
+ control
Grintescu et al, Clin Nutr 2014
reduced incidence of hyperglycemia (p<0.05)
reduced insulin needs (p<0.05)
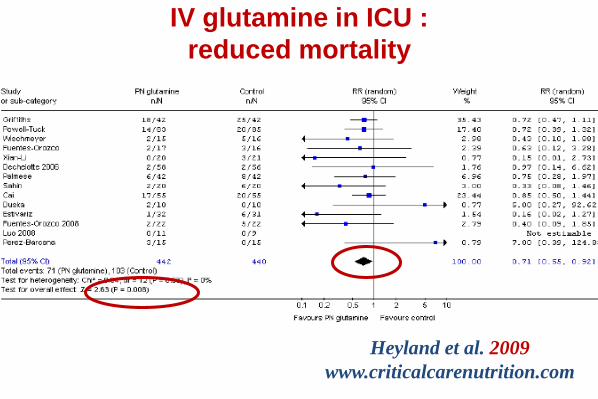
IV glutamine in ICU :
reduced mortality
Heyland et al. 2009
www.criticalcarenutrition.com
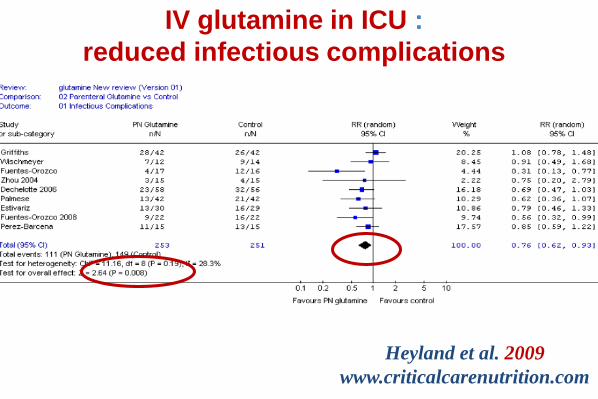
IV glutamine in ICU :
reduced infectious complications
Heyland et al. 2009
www.criticalcarenutrition.com
IV glutamine + PN in ICU : recommendations
« When PN is indicated in ICU patients, the AA solution
should contain 0.2-0.4 g/kg/day of L-glutamine (e.g. 0.3-0.6
g/kg/day of alanyl-glutamine dipeptide) » - grade A
Chambrier et al Ann Fr Anesth Réanim 2011; 30:381-389
French (SFNEP/ASFAR)
European (ESPEN)
Singer et al Clin Nutr 2009, 28:387-400
In case of major post-operative complications, it is
recommended to prescribe glutamine intravenously and
at high dosage (0.2 à 0.4 g/kg/day i.e. 0.3 à 0.6 g/kg/day of
dipeptide).
• 200 italian ICUs data base
• reduced mortality (24.6% ± 1.6% vs. 34.5% ± 2.1%),
infection rate (13.8% ± 2.9% vs. 18.8% ± 3.9%), and
hospital LOS (24.9 ± 0.3 vs. 26.0 ± 0.3 days)
• a lower total cost per patient (23,409 ± 3,345 vs.
24,161 ± 3,523 Euro).
• treatment cost more than offset by savings on ICU
and antibiotic costs cost-efficiency of IV glutamine
Pradelli et al.
Int J Technol Assess Health Care 2012; 28(1):22-8
Effectiveness and cost-effectiveness of supplemental
glutamine dipeptide in TPN for critically ill patients:
IV glutamine + TPN and demonstrated favourable
outcome in ICU patients: which patients?
• mixed populations of ICU patients
• surgical and medical patients, unable to be fed enterally
• some patients in shock, but TPN + IV gln were
introduced after resuscitation,
• severe liver or renal failure : always excluded
IV glutamine + TPN and favourable outcome
in ICU patients: which dose and nutrition?
• dipeptide dose adapted to patient’s weight
• 0.5 g/kg/day of alanyl-glutamine dipeptide
= > recommended dose in ICU
• Gln-dipeptide given along with TPN, continuous infusion
• patients adequately fed with full TPN
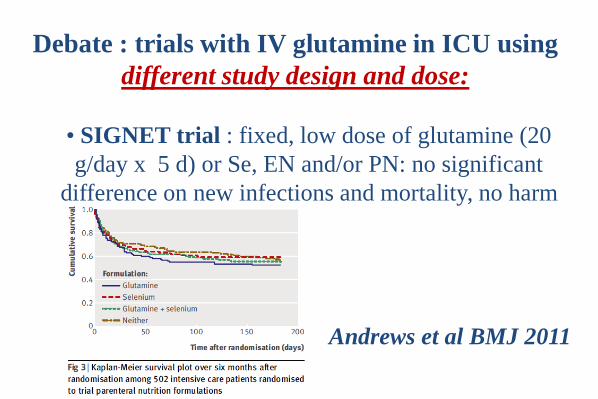
• SIGNET trial : fixed, low dose of glutamine (20
g/day x 5 d) or Se, EN and/or PN: no significant
difference on new infections and mortality, no harm
Andrews et al BMJ 2011
Debate : trials with IV glutamine in ICU using
different study design and dose:
• fixed and low dose of glutamine
• low nitrogen/protein supply
• heterogeneity of nutritional support : underpowered
both for EN and PN-treated patients
• 2x2 design : interactions??
not included in the 2014 meta-analysis
Limitations of the SIGNET trial :
• 40 RCTs, 3107 patients : surgery, critical illness, mixed
• reduction of mortality in critically ill group (p=0.024),
• reduction of infection risk (p=0.009) in global
population
• reduction of hospital length of stay (p=0.001, global)
• in studies with dose 0.3-0.5 g/kg bw/day dipeptide:
significant reduction of short term mortality, infections
and LOS.
• no evidence of harm or toxicity
Bollhalder et al Clin Nutr 2013
Global meta-analysis of RCTs of parenteral Gln
• REDOX Study
• very high Gln load : around 0.7 g/kg bw/d in total
• given both IV and enterally
• alone or combined with AOX,
• 2 x 2 design
• Gln supply separated from nutrition, started D1
• large, multicenter, heterogeneity+++
Heyland, NEJM 2013
Debate : trials with glutamine in ICU using
different study design and dose:
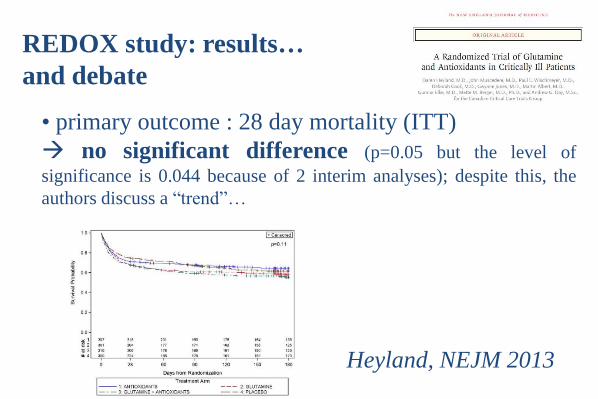
• primary outcome : 28 day mortality (ITT)
no significant difference (p=0.05 but the level of
significance is 0.044 because of 2 interim analyses); despite this, the
authors discuss a “trend”…
REDOX study: results…
and debate
Heyland, NEJM 2013
• post-hoc secondary outcome : “trend” for increased
hospital and 6-month mortality in combined groups with
gln vs no gln…
but :
• this combined “gln” group was not planned in the
statistical design post-hoc analysis
• in-hospital mortality was not a priori defined
• 6-month mortality only exploratory : massive loss in
the follow up, no adjustment for interim analysis
Buys et al, NEJM 2013
REDOX study: controversy on “toxicity”…
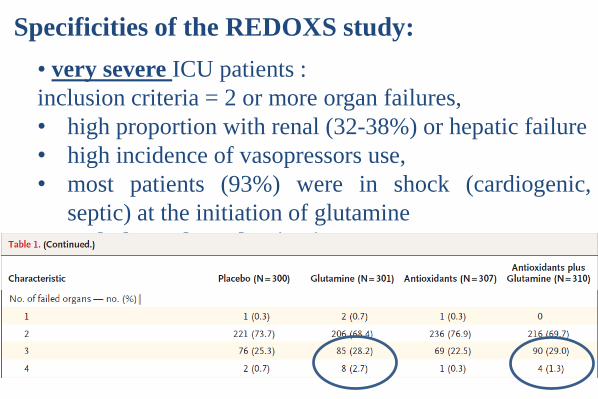
• very severe ICU patients :
inclusion criteria = 2 or more organ failures,
• high proportion with renal (32-38%) or hepatic failure
• high incidence of vasopressors use,
• most patients (93%) were in shock (cardiogenic,
septic) at the initiation of glutamine
• Unbalanced randomisation
Specificities of the REDOXS study:
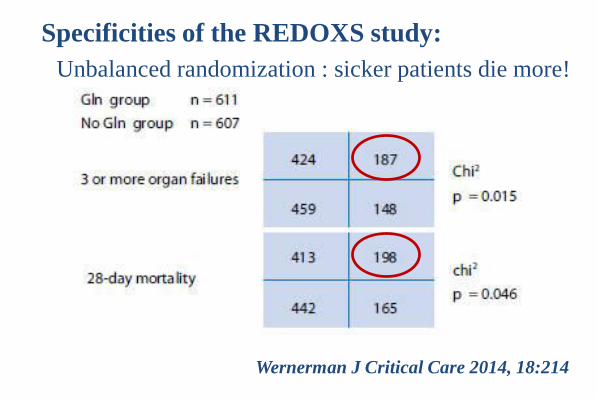
Wernerman J Critical Care 2014, 18:214
Unbalanced randomization : sicker patients die more!
Specificities of the REDOXS study:
• high total dose of Gln, different from guidelines
•full Gln dose at D1 while feeding was minimal
• patients remained severely underfed (mostly enteral
nutrition, < 50% of nutritional goals at 1 week)
• inclusion of patients with renal failure and liver
failure
Specificities of the REDOXS study:
• post-hoc analysis to identify significant
predictors of mortality:
- renal dysfunction,
- fed <30% of caloric needs (p<0.03)
• “trends” for other predictors: GI diagnostic, use of
vasopressors, steroids, early supply of Gln
Heyland, JPEN 2014,
Specificities of the REDOXS study:
• early provision of high Gln dose in ICU patients
with shock, MOF and underfeeding brings no benefit
• gln remains to be avoided in ICU patients with
renal or hepatic failure
• some very sick ICU patients presenting with high
gln plasma levels at admission have a poor prognosis
indicative of Gln impaired metabolism rather
than toxicity
REDOXS study: so what?
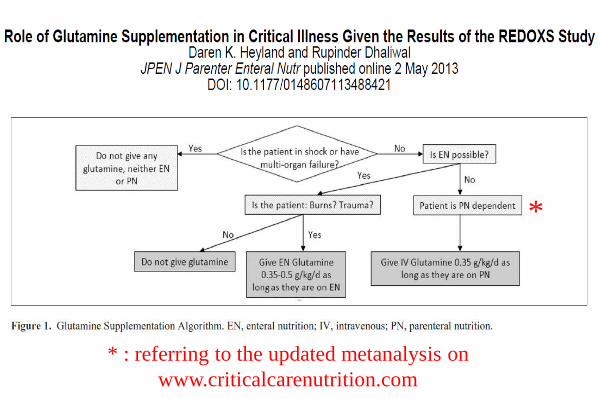
*
* : referring to the updated metanalysis on
www.criticalcarenutrition.com
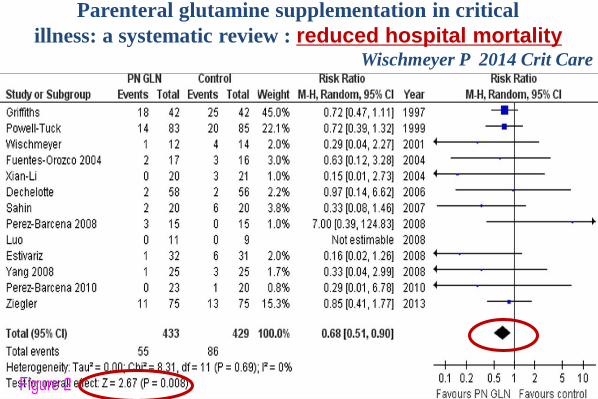
Parenteral glutamine supplementation in critical
illness: a systematic review : reduced hospital mortalityWischmeyer P 2014 Crit Care
Wischmeyer P 2014 Crit Care
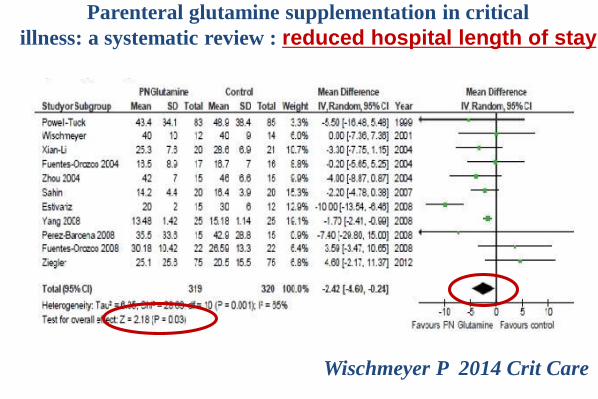
Parenteral glutamine supplementation in critical
illness: a systematic review : reduced hospital length of stay
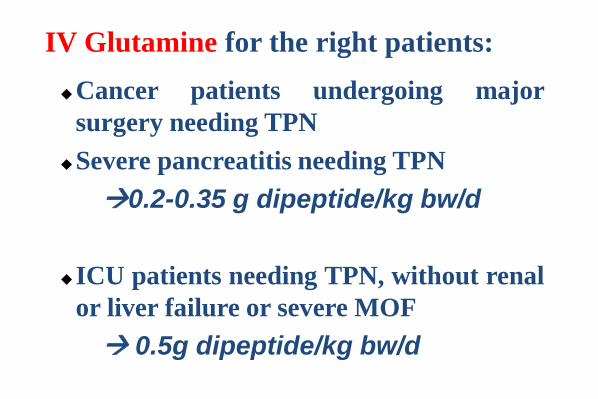
Cancer patients undergoing major
surgery needing TPN
Severe pancreatitis needing TPN
0.2-0.35 g dipeptide/kg bw/d
ICU patients needing TPN, without renal
or liver failure or severe MOF
0.5g dipeptide/kg bw/d
IV Glutamine for the right patients:







