
Population ReportsExpanding Services for Injectable Contraceptives
Based on Population Reports, Series K, Number 6 Dec. 2006 Prepared by Robert Lande and Catherine Richey, MPH
Population Reports
More Women Are Choosing Injectables
• Worldwide use of injectables more than doubled over 10 years among married women ages 15-49, increasing from 12 million in 1995 to over 32 million in 2005.
• Injectables are currently the fourth most popular contraceptive method worldwide.– In sub-Saharan Africa,
injectables are the most popular method: among women using modern methods, 38% use injectables.

Population Reports
Levels of Use Vary Widely Within Regions
• In sub-Saharan Africa, Asia, and Latin America and the Caribbean over 40% of married contraceptive users rely on injectables in some countries, while 5% to 7% use them in other countries.
• Variations can be attributed to a variety of factors.– Access to injectables– Customs related to
contraceptive use– Government policies– Tolerance for side effects– Communication about
injectables

Population Reports
Numbers Expected to Grow as Injectables Become More Available
• By 2015, worldwide use is projected to reach 40 million—more than triple the 1995 level.
Source: Mauldin, 1994; Ross, 2005; United Nations, 2005

Population Reports
Two Types of Injectables Are Used Currently
Progestin-Only Injectables Combined Injectables
•DMPA: Injected every three months•NET-EN: Injected every two months
•Estrogen + Progestin (e.g., Cyclofem, Mesigyna)•Injected every month (also called “monthly injectables”)

Population Reports
• Highly effective– Used correctly, injectables are more effective than female
sterilization.
• Long acting– No action required every day or at time of intercourse.
• Reversible– Fertility returns after a woman stops using an injectable.
• Private– Women can use injectables without anyone else knowing.– No supplies must be kept around the house.
Injectables Are a Popular Choice

Population Reports
Injectables Are Not For Everyone
• Side effects may deter use or lead to discontinuation.– Common side effects include irregular bleeding,
no monthly bleeding, and weight gain. – In a large WHO trial, half of women stopped using
DMPA and NET-EN within 12 months (WHO, 1983).
• Some women have trouble returning to the clinic for repeat injections.
• Counseling helps women continue using injectables (Canto de Cetina, 2001; Lei, 1996).

Population Reports
A Strategy to Meet Rising Demand for Injectables Includes:
• Maintaining adequate supplies; • Increasing efficiency;• Providing training and supervision;• Ensuring safe injections;• Disposing of waste safely;• Considering community provision of
injectables;• Helping women who need more information
about side effects or safety.

Population Reports
Supply Meets Demand With Forecasting and Ingenuity

Population Reports
Programs Can Maintain Adequate Stock Levels by…
• Keeping necessary supplies on hand:– Needles and syringes– Vials of injectable contraceptives– Sharps disposal containers
• Properly storing supplies to maintain potency.– Store vials upright between 20°
and 25°C (68° and 77°F) away from direct sunlight.
• Avoiding loss of expired stock.– Use supplies with the earliest
expiration date first.

Population Reports
Forecasting Is Important When Demand Is Rising
• Good forecasting takes into account:– Expected increases in use of injectables;– Past trends in use of injectables;– Numbers of new and returning injectables clients;– Changes in population.
• Software tools help monitor injectables stock and plan procurement.– E.g. Pipeline Software Tool (John Snow, Inc.)

Population Reports
If Stockouts Do Occur…• Order an emergency shipment.
– USAID* and UNFPA can facilitate a fast shipment.
• Borrow supplies from nearby facilities.• Mobilize suppliers, volunteers, and shippers.
– During a national stockout in Nepal, supplies were procured, packaged, and delivered to every MOH health facility within 60 days.
• Share clients.– Facilities with low stocks of injectables can
encourage clients to go to other sources.
*for USAID-funded programs

Population Reports
Staffing and Training to Meet Demand

Population Reports
Tailor Training to Fit Program Needs
• Comprehensive training may be needed if a program is adding injectables as a new method or training new workers.
• Focused training may be used to strengthen a specific component of service delivery.
• Training may include:– Characteristics of
injectables;– Giving safe injections; – Counseling;– Screening clients using
medical eligibility criteria;– Correcting misperceptions;– Conducting return visits;– Managing side effects.
Population Reports
A Range of Providers Can Give Contraceptive Injections
• With training, any health care provider can give contraceptive injections. – Such providers may include pharmacists, auxiliary
nurses, midwives, medical assistants, and community providers.
• Training a wider range of providers can expand access to injectables.– In Honduras, allowing auxiliary nurses to provide
injectables increased use by 19-35% in the rural clinics where the nurses were posted (Mendoza,
2001).

Population Reports
Safe Injections Protect Clients, Clinic Staff, and the Community

Population Reports
Auto-Disable (AD) Syringes Now Preferred
• WHO recommends disposable syringes—ideally AD syringes—for contraceptive injections.
• AD syringes inactivate after a single use, eliminating the risk of infection due to reuse.
Population Reports
Safe Injection Practices Prevent Infection Transmission
• Rules for safe injections:– Prepare each injection in a clean,
designated area;– Use a sterile syringe and needle
for each injection;– Discard disposable needles and
syringes in a sharps container immediately after use;
– Safely dispose of waste according to local or environmental regulations.

Population Reports
Choose an Appropriate Method of Waste Disposal
• Programs should choose the disposal method that is most appropriate for their local conditions, taking into account cost, safety risks, and environmental regulations. – Burying waste in a protected pit at least two meters
deep.
– Incineration, at temperatures above 800°C.
– Burning waste at low temperatures and burying remaining ash and noncombustible material in a protected pit.

Community Distribution Expands Access to Injectables

Population Reports
Community Distribution Expands Access to Injectables
• Programs in several countries offer injectables in community outlets:– Mobile clinics, village clinics, periodic
temporary outreach clinics, or at the homes of clients or community health workers
• Community provision has dramatically increased use of injectables in some areas– In the Navrongo Initiative in Ghana, 92% of
contraceptive users chose injectables from a community provider (Debpuur, 2002; Phillips, 2005).

Population Reports
Community and Clinic Provision Are Comparable
• A 2005 study in Uganda compared the quality of injectables services in the community and in the clinic.
– Screening for medical eligibility: No reported screening mistakes in either group.
– Counseling: Levels of client knowledge were the same in both groups, but both needed improvement.
– Injection safety: No reported infections or needlestick injuries.
– Disposal of waste: Disposal practices in both groups needed improvement.
– Continuation rates: 88% of community clients and 85% among clinic clients had a second injection.
– On-time repeat injections: 94% of clients in both groups received their second injections on time (Stanback 2005) .

Population Reports
Challenges of Scaling-Up Community Programs
• Retaining community providers– To improve morale, the Ghana Health Service increased
incentives for community nurses to stay on the job and allowed them to work in their home areas.
• Ensuring quality of care– Training and supervision must cover screening for medical
eligibility, counseling, and waste disposal.
• Cost of offering household visits – Encouraging women to visit community clinics can reduce
costs but may decrease access for some poor or uneducated women who depend on household visits.

Population Reports
Meeting Rising Demand Efficiently

Population Reports
Programs Can Avoid Large Increases in Costs By…
• Organizing work better– Improve the flow of clients through clinics by
reducing waiting time or setting up an “express” line for routine repeat injections.
• Reducing the costs of supplies and facilities– Buy injectables supplies and equipment in bulk at
the lowest available price.• Increasing productivity
– In some clinics providers can be encouraged to spend less time on administrative duties and more time seeing clients.

Population Reports
Programs Can Recover Some Costs by Encouraging Clients
to Pay if They Can• Charging clients for services does not always
decrease demand substantially.– Doubling the price of contraceptives has reduced
demand by no more than 15%, according to studies in Bangladesh, Indonesia, and Nigeria.
• A willingness-to-pay survey can help gauge what people are willing to pay for injectables and other contraceptives.

Population Reports
Communication Helps Women Try and Use Injectables

Population Reports
Tailor Messages For Specific Audiences
• Potential users – May know about injectables but hesitate to try them.
– Seeing satisfied users and receiving correct information can help women make informed choices about injectables.
• Current users – May have questions or concerns about side effects.
– Interacting with a trusted source of information helps women cope with changes if they occur.
• Partners and husbands – Can help women use injectables effectively. – A 1995 study in the Philippines found that women whose husbands
approved of injectables were more than twice as likely to continue using the method (Population Council, 1996).

Population Reports
Interactive Sources Help Inform About Injectables
• Telephone Hotlines– Offer a private connection with a trained family planning
counselor. – In Turkey injectables users called with questions about side
effects (Berg, 1998).
• Discussions with providers– Gives women a chance to interact directly with a trusted
source.
• Community meetings– An interactive and public way to improve knowledge and
answer questions about injectables.
Population Reports
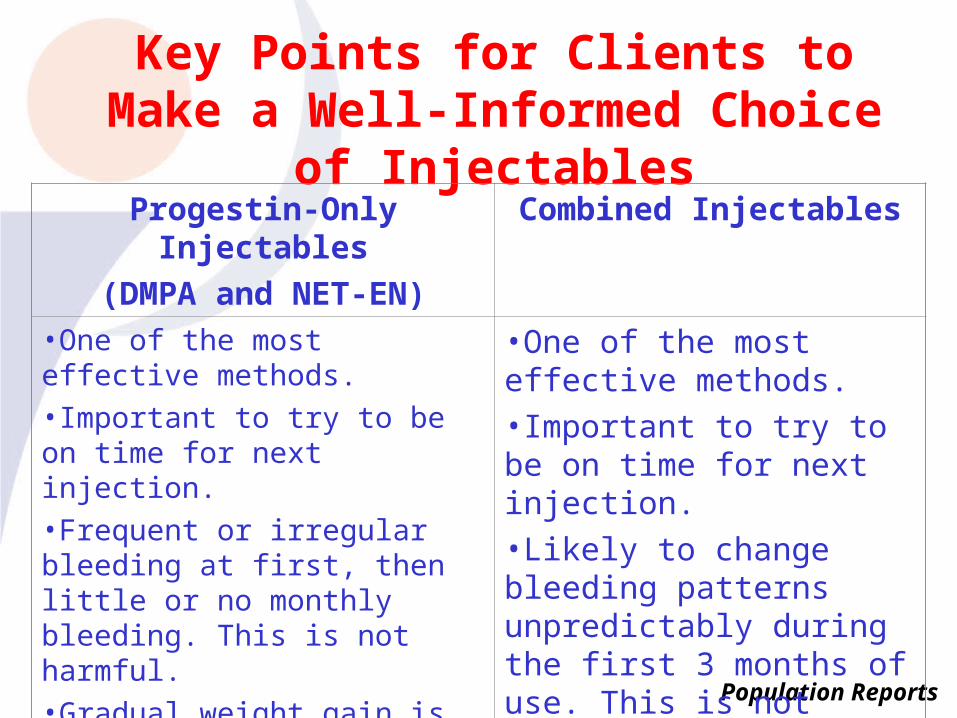
Key Points for Clients to Make a Well-Informed Choice of Injectables
Progestin-Only Injectables
(DMPA and NET-EN)
Combined Injectables
•One of the most effective methods.
•Important to try to be on time for next injection.
•Frequent or irregular bleeding at first, then little or no monthly bleeding. This is not harmful.
•Gradual weight gain is common and not harmful.
•Delay in return to fertility (DMPA)
•One of the most effective methods.•Important to try to be on time for next injection.•Likely to change bleeding patterns unpredictably during the first 3 months of use. This is not harmful.

Population Reports
Providers Can Help Clients be Informed Users of Injectables
• To support a client using injectables, tell her:– When to return for her next injection and what to
do if she is late.– That side effects are not harmful; providers can
help women manage some bothersome side effects.
• If a client is dissatisfied with injectables, help her choose a different method.

Population Reports
Women with HIV/AIDS Can Use Injectables
• Injectables are safe and effective for women with HIV/AIDS, and for those taking ARV medications.– The few studies available find that DMPA has little effect on
ARV medications and ARV medications do not reduce effectiveness of DMPA (Chu, 2005; Cohn, 2005; WHO, 2004).
– Women on ARV medications can use the same injection schedule as other women. They do not need to come back earlier.
• Injectables offer no protection against transmission of STIs; male or female condoms can be used with injectables to protect against STIs.

Population Reports
New Options Offer Women Additional Choices
• Subcutaneous Injection– The low-dose depo-subQ provera
104 (DMPA-SC) is injected under the skin every 3 months.
– Currently approved in the U.S. and U.K.; may be available in developing countries by 2008.
• Self-Injection– In trials many women preferred
giving themselves injections– May avoid repeated visits and
increase continuation rates

Population Reports
Photo and Illustration Credits
• Slide 1 Bangladesh/CCP• Slide 5: JSI/DELIVER and Schering AG• Slide 9: JSI/DELIVER• Slide 10: JSI/DELIVER• Slide 13: John Stanback/FHI• Slide 16: John Stanback/FHI• Slide 17: Dr. Sanjeev Badiger, Courtesy of Photoshare • Slide 18: Rafael Avila/CCP• Slide 20: Kingson Namun/Mark Munguas, Courtesy of Photoshare• Slide 24: Population Services International• Slide 27: Sarah A. Holtz, Courtesy of Photoshare• Slide 33: Rafael Avila/CCP

Population Reports
References• Berg, R., Kanesathasan, N., and Bollinger, L. Getting from awareness to use:
Lessons learned from SOMARC III about marketing hormonal contraceptives. Washington, D.C., Futures Group International, Social Marketing for Change (SOMARC), Sep. 1998. (SOMARC III Special Study No. 6) 21 p.
• Canto De Cetina, T.E., Canto, P., and Ordonez Luna, M. Effect of counseling to improve compliance in Mexican women receiving depot-medroxyprogesterone acetate. Contraception 63(3): 143–146. Mar. 2001
• Chu, J.H., Gange, S.J., Anastos, K., Minkoff, H., Cejtin, H., Bacon, M., Levine, A., and Greenblatt, R.M. Hormonal contraceptive use and the effectiveness of highly active antiretroviral therapy. American Journal of Epidemiology 161(9): 881–890. May 1, 2005.
• Cohn, S., Watts, D., Lertora, J., Park, J.G., and Yu, S. An open–label, non–randomised study of the effect of depo–medroxyprogesterone acetate on the pharmacokinetics of selected protease inhibitors and non–nucleoside reverse transcriptase inhibitors therapies among HIV–infected women. Presented at the 12th Conference on Retroviruses and Opportunistic Infections, Boston, Feb. 22-25, 2005.
• Debpuur, C., Phillips, J.F., Jackson, E.F., Nazzar, A., Ngom, P., and Binka, F.N. The impact of the Navrongo Project on contraceptive knowledge and use, reproductive preferences, and fertility. Studies in Family Planning 33(2): 141–164. Jun. 2002.

Population Reports
References (continued)…• Lei, Z.W., Wu, S.C., Garceau, R.J., Jiang, S., Yang, Q.Z., Wang, W.L., and
Vander Meulen, T.C. Effect of pretreatment counseling on discontinuation rates in Chinese women given depomedroxyprogesterone acetate for contraception. Contraception 53(6): 357–361. Jun. 1996.
• Mauldin, W.P. and Miller, V.C. Contraceptive use and commodity costs in developing countries, 1994–2005. New York, United Nations Population Fund (UNFPA), 1994. 64 p.
• Mendoza, I. and Vernon, R. Promoting reproductive health services in rural communities in Honduras. Population Council, Frontiers in Reproductive Health, Jun. 15, 2001. 11 p. (http://www.popcouncil.org/pdfs/frontiers/FR_FinalReports/Honduras_Nurse_roles.pdf)
• Phillips, J.F., Bawah, A.A., and Binka, F.N. Accelerating reproductive and child health program development: The Navrongo Initiative in Ghana. New York Population Council, 2005. 27 p. (http://www.popcouncil.org/pdfs/wp/208.pdf)
• Population Council. Focus on the Philippine DMPA reintroduction program: Continuing users vs. drop–outs. Manila, Population Council, Apr. 1996. (Research News No. 7) 2 p.

Population Reports
References (continued)…• Ross, J., Stover, J., and Adelaja, D. Profiles for family planning and reproductive
health programs: 116 countries. Futures Group, 2005. 182 p. (Available: http://www.constellafutures.com/Documents/Profiles116FP2ed.pdf)
• Stanback, J., Mbonye, A., Lemelle, J., Bekiita, M., Ssekito, G., and Kajura, N.J. Safety and feasibility of community–based distribution of Depo–Provera in Nakasongola, Uganda. Final Report. Research Triangle Park, North Carolina, Family Health International, Uganda Ministry of Health, Save the Children, Nakasongola Local Government, Jun. 2005. 20 p.
• United Nations (UN). World contraceptive use 2005. [Wall Chart]. New York, UN, Jan. 2006.
• World Health Organization (WHO). Multinational comparative clinical trial of long–acting injectable contraceptives: Norethisterone enanthate given in two dosage regimens and depot–medroxyprogesterone acetate. Final report. Contraception 28(1): 1–20. Jul. 1983.
• World Health Organization (WHO). Scaling up antiretroviral therapy in resource–limited settings: Treatment guidelines for a public health approach. Geneva, WHO, 2004. 68 p. (Available: http://www.who.int/hiv/pub/prev_care/en/arvrevision2003en.pdf)

Population Reports
Ordering Information
You may order this report in one of four ways:
Online at http://www.jhuccp.org/cgi-bin/orders/orderform.cgi;
by sending an e-mail message to [email protected];
by sending a fax to 1-410-659-6266;
or by writing to
INFO Project
Distribution
111 Market Place
Suite 310
Baltimore, MD 21202 USA







