
1/2/2019
1
Evidence-Based Review of Transvaginal
Hysteropexy for Uterovaginal Prolapse
Holly E. Richter, PhD, MD
J Marion Sims Endowed Chair
Professor Obstetrics and Gynecology, Urology and Geriatrics
Division of Urogynecology and Pelvic Reconstructive Surgery
Department of Obstetrics and Gynecology
February 21 , 2019
Disclosures
• Pelvalon-consultant; research funding,
device study, non-surgical treatment FI
• Renovia-consultant; research funding non-
surgical treatment SUI
• Bluewind-consultant, refractory UUI
• UpToDate
• Travel with IUJ and Obstet Gynecol, editor
• NIA-research funding
• NICHD, NIDDK-research funding
• PCORI-research funding
No Conflict of Interest
Objectives
• Discuss hysteropexy indications
-Patient selection
-Contraindications
• To summarize existing evidence regarding
objective and subjective outcomes of native
tissue hysteropexy techniques vs vaginal
hysterectomy for uterovaginal prolapse
• To present results of most recent RCT of mesh
hysteropexy/repairs to TVH/repairs for
uterovaginal prolapse: Study of Uterine Prolapse
Procedures Randomized Trial (SUPeR)
1/2/2019
2
Do We Have to Perform a
Hysterectomy?• Uterus not the cause
• Hysterectomy routinely performed - improve support
• True?
• Standard of care?
• Limited exposure to hysteropexy – residency/
fellowship
• Women request hysteropexy - unique reasons or
preferences/clinical situations
• An increasing number of studies are
investigating uterine sparing procedures with an
emphasis on:
-efficacy
-safety
-improved quality of life
1/2/2019
3
Outcomes of NT Hysteropexy vs Hysterectomy
• Recent systematic review addressing this issue:*
-similar short-term efficacy, 3 years (apical recurrence, RR 2.22, 95% CI, 0.80 to 6.17; anterior, RR 0.86, 95% CI, 0.48 to 1.55; posterior RR 0.79, 95% CI, 0.79 to 2.03
-decreased blood loss (-89.9 mL, 95% CI, -14.9 to -165.0 mL)
-decreased operative time (-17.5 min, 95% CI, -6.0 to -29.2 min)
-satisfaction (RR, 1.07, 95% CI, 0.38 to 2.99)
*Meriwether et al, 2018
Patient Opinions
• 220 referrals prolapse
• 127 (57.5%) response
• 60% choose hysteropexy if equal efficacy
• Hysterectomy: worsen mood, relationship, QOL,
femininity, body image, lubrication, sex drive, weight
gain
• Most important factors:
• Doctor’s opinion
• Risk of surgical complications
• Risk of malignancy
Frick AC et al. Attitudes toward hysterectomy in women undergoing evaluation for uterovaginalprolapse. Female Pelvic Med Reconstr Surg 2013;19:103-9.
So why am I talking about this?
• Do I have something against vaginal
hysterectomy?
• Am I on a crusade to “SAVE THE UTERUS”?
• Do I want to have an evidence-based discussion
with my patients on all surgical options for the
treatment of uterovaginal prolapse?
1/2/2019
4
Why Leave the Uterus?
• Desires future fertility
• Belief that the uterus affects sexual
function or sense of identity
• Concern about risks of hysterectomy
Hysterectomy / Ovarian Function
• Prospective cohort, age 30-47
• Hyst no BSO (406) vs Controls (465)
• Annual blood samples x 5 yrs
• Ovarian failure: FSH ≥ 40
• Hyst: HR = 1.92 (1.29-2.86)
• Hyst only: HR = 1.74 (1.14-2.65)
• Hyst + USO: HR = 2.93 (1.57-5.49)
• 14.8% Hyst vs 8% controls ovarian failure >4 yrs
Moorman PG. Effect of hysterectomy with ovarian preservation on ovarian function. ObstetGynecol 2011;118:1271-9.
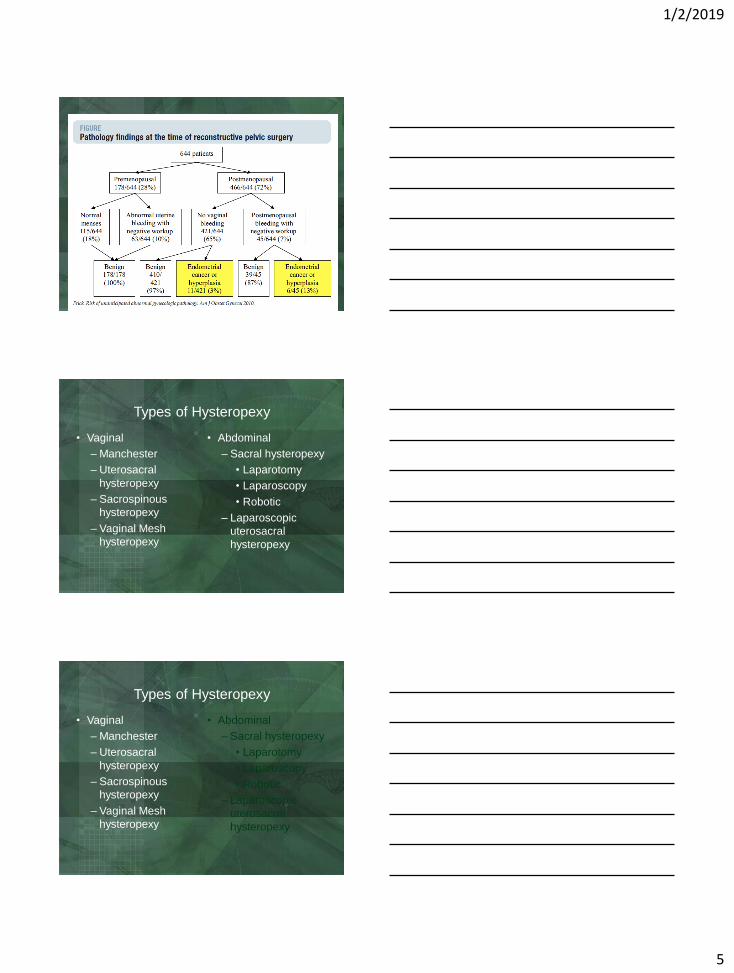
Contraindications Uterine Conservation
• Uterine abnormalities
• Fibroids, adenomyosis, endometrial pathology
• Current/recent cervical dysplasia
• Abnormal menses
• PMB
• Genetic risks
• BRCA 1 & 2, HNPCC
• Tamoxifen therapy
• Unable to comply with routine surveillance
1/2/2019
5
Types of Hysteropexy
• Vaginal
– Manchester
– Uterosacral
hysteropexy
– Sacrospinous
hysteropexy
– Vaginal Mesh
hysteropexy
• Abdominal
– Sacral hysteropexy
• Laparotomy
• Laparoscopy
• Robotic
– Laparoscopic
uterosacral
hysteropexy
Types of Hysteropexy
• Vaginal
– Manchester
– Uterosacral
hysteropexy
– Sacrospinous
hysteropexy
– Vaginal Mesh
hysteropexy
• Abdominal
– Sacral hysteropexy
• Laparotomy
• Laparoscopy
• Robotic
– Laparoscopic
uterosacral
hysteropexy
1/2/2019
6
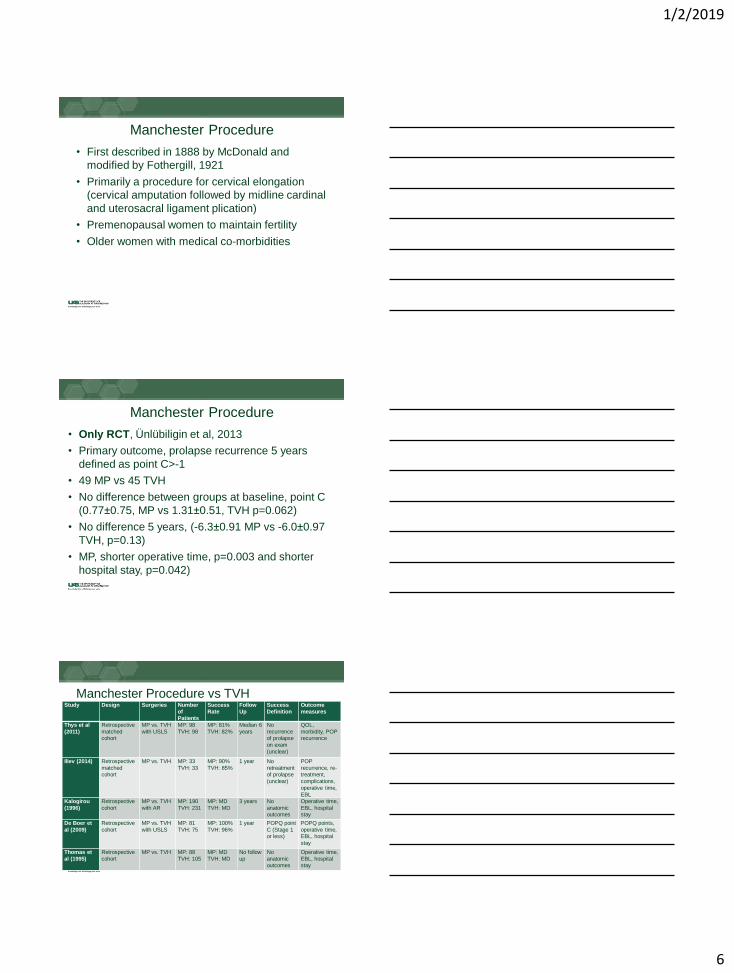
Manchester Procedure
• First described in 1888 by McDonald and
modified by Fothergill, 1921
• Primarily a procedure for cervical elongation
(cervical amputation followed by midline cardinal
and uterosacral ligament plication)
• Premenopausal women to maintain fertility
• Older women with medical co-morbidities
Manchester Procedure
• Only RCT, Ünlübiligin et al, 2013
• Primary outcome, prolapse recurrence 5 years
defined as point C>-1
• 49 MP vs 45 TVH
• No difference between groups at baseline, point C
(0.77±0.75, MP vs 1.31±0.51, TVH p=0.062)
• No difference 5 years, (-6.3±0.91 MP vs -6.0±0.97
TVH, p=0.13)
• MP, shorter operative time, p=0.003 and shorter
hospital stay, p=0.042)
Manchester Procedure vs TVHStudy Design Surgeries Number
of Patients
Success
Rate
Follow
Up
Success
Definition
Outcome
measures
Thys et al
(2011)
Retrospective
matched cohort
MP vs. TVH
with USLS
MP: 98
TVH: 98
MP: 81%
TVH: 82%
Median 6
years
No
recurrence of prolapse
on exam
(unclear)
QOL,
morbidity, POP recurrence
Iliev (2014) Retrospective
matched cohort
MP vs. TVH MP: 33
TVH: 33
MP: 90%
TVH: 85%
1 year No
retreatment of prolapse
(unclear)
POP
recurrence, re-treatment,
complications,
operative time,
EBL
Kalogirou
(1996)
Retrospective
cohort
MP vs. TVH
with AR
MP: 190
TVH: 231
MP: MD
TVH: MD
3 years No
anatomic outcomes
Operative time,
EBL, hospital stay
De Boer et
al (2009)
Retrospective
cohort
MP vs. TVH
with USLS
MP: 81
TVH: 75
MP: 100%
TVH: 96%
1 year POPQ point
C (Stage 1 or less)
POPQ points,
operative time, EBL, hospital
stay
Thomas et
al (1995)
Retrospective
cohort
MP vs. TVH MP: 88
TVH: 105
MP: MD
TVH: MD
No follow
up
No
anatomic outcomes
Operative time,
EBL, hospital stay
1/2/2019
7
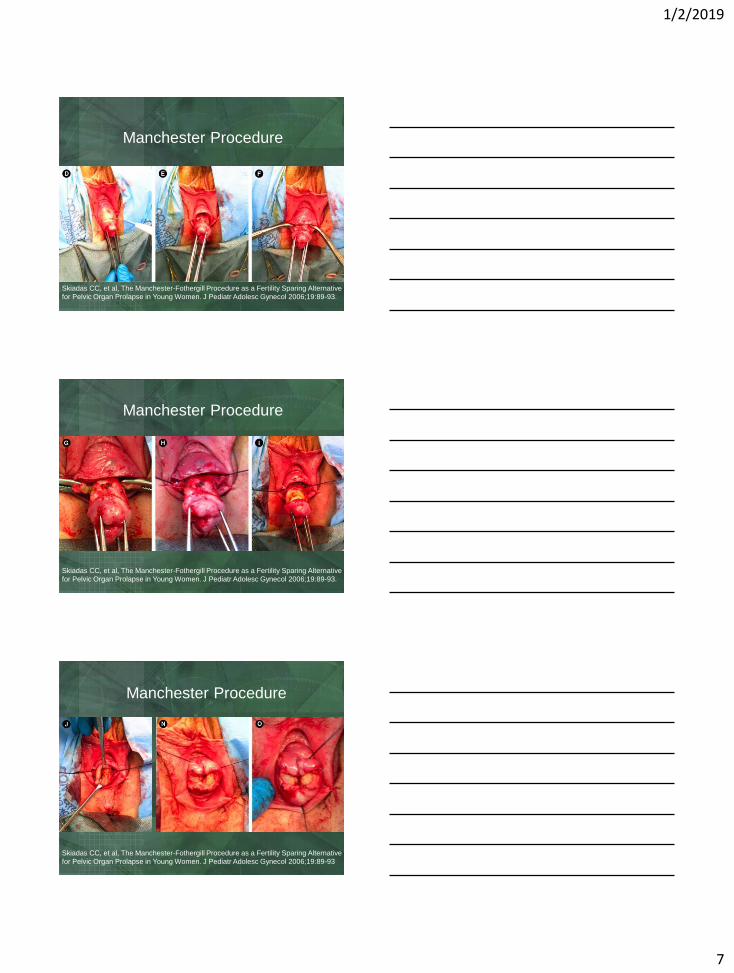
Skiadas CC, et al, The Manchester-Fothergill Procedure as a Fertility Sparing Alternative
for Pelvic Organ Prolapse in Young Women. J Pediatr Adolesc Gynecol 2006;19:89-93.
Manchester Procedure
Skiadas CC, et al, The Manchester-Fothergill Procedure as a Fertility Sparing Alternative
for Pelvic Organ Prolapse in Young Women. J Pediatr Adolesc Gynecol 2006;19:89-93.
Manchester Procedure
Skiadas CC, et al, The Manchester-Fothergill Procedure as a Fertility Sparing Alternative
for Pelvic Organ Prolapse in Young Women. J Pediatr Adolesc Gynecol 2006;19:89-93
Manchester Procedure

1/2/2019
8
Uterosacral Hysteropexy
• No RCTs comparing outcomes of USH and TVH
• Romanzi et al, 2012 retrospective cohort
• Primary outcome ≥Grade 2 prolapse any
compartment; N=100 each group
• No difference in baseline anterior or apical
compartments (point C, 2.91±0.91, USH vs
2.84±1.02, TVH, p=0.82)
• No difference in 2 year recurrence-free durability
apex: (96%, 95% CI, 87.7%, 98.8%), p=0.90
Uterosacral Hysteropexy
Sacrospinous Hysteropexy
• Best studied vaginal uterine-sparing procedure
• SSLF of the vaginal cuff first described in 1950’s
• Richardson et al, reported a case series of 5
patients in 1989
Richardson, Scotti, Ostergard, JRM, 1989
1/2/2019
9
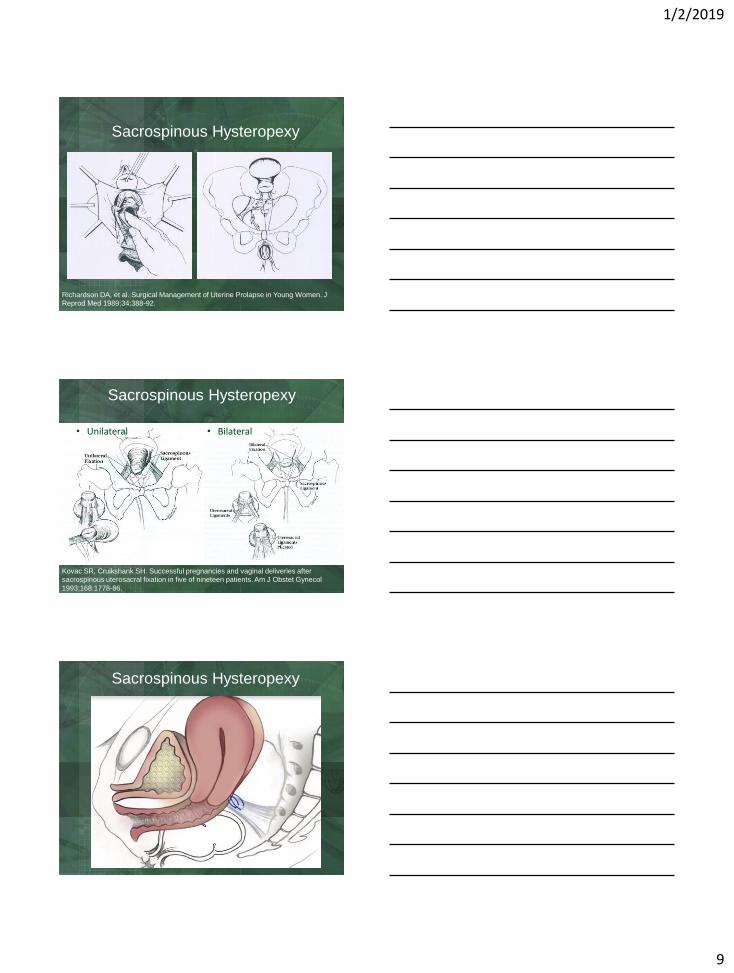
Sacrospinous Hysteropexy
Richardson DA, et al. Surgical Management of Uterine Prolapse in Young Women. J
Reprod Med 1989;34:388-92.
Sacrospinous Hysteropexy
• Unilateral • Bilateral
Kovac SR, Cruikshank SH. Successful pregnancies and vaginal deliveries after
sacrospinous uterosacral fixation in five of nineteen patients. Am J Obstet Gynecol
1993;168:1778-86.
Sacrospinous Hysteropexy

1/2/2019
10
Cohort Studies SSH vs HysterectomyStudy Design Surgery Number of
Patients
Success Rate Follow Up Success Definition
Hefni et al
(2003)24
Prospective
cohort
SSH vs TVH
with SSLF
SSH: 61
TVH: 48
SSH: 94%
TVH: 96%
33 months Apex greater than
6cm from hymen on valsalva
Maher et al
(2001)25
Retrospective
cohort
SSH vs TVH
with SSLF
SSH: 34
TVH: 36
SSH: 74%
TVH: 72%
26 months Apex above ½ TVL,
no repeat surgery
Van
Brummen (2003)26
Retrospective
cohort
SSH vs TVH
with USLS
SSH: 44
TVH: 30
SSH: 89%
TVH: 93%
19 months Baden-Walker grade
1 or less of any compartment
Lo et al
(2015)27
Retrospective
cohort
SSH vs TVH
with SSLF
SSH: 26
TVH: 120
SSH: 50%
TVH: 72%
86 months POPQ Stage 1 or
less
Sacrospinous Hysteropexy
• Dietz 2010
• RCT SSH (n=37) vs. TVH, USLS (n=34)
• Apical recurrences: 21% vs. 3%, p=0.03
• 3 SSHP stage 4 prolapse – all failed
• Subjective: both improved
• Shorter LOS, quicker return work, longer TVL
• Anterior prolapse (51% vs. 64%)
Dietz V, et al. One-year follow-up after sacrospinous hysteropexy and vaginal
hysterectomy for uterine descent: a randomized study. Int Urogynecol J 2010;21: 209-16
Sacrospinous Hysteropexy
• Detollenaere, et al, 2015
• Non-inferiority RCT
• N=103, SSH vs N=105, TVH/USLS
• 1° outcome-composite at 12 months (apical <
Stage 2, no bothersome symptoms and no re-op)
• Success: 100% SSH vs 96% TVH, (-3.9, 95% CI,
-8.6, 0.7)
• Functional and QOL similar
• AEs: Buttock pain, 9% vs 0%
Detollenaere et al, BMJ, 2015
1/2/2019
11
Sacrospinous Hysteropexy
• Jeng 2005
• RCT, SSH vs TVH/SSLF
• No difference sexual function (FSFI-7)
• Low rate dyspareunia (5%)
• No anatomic outcomes
• Transient buttock pain (15%)
Jeng CJ, et al. Sexual functioning after vaginal hysterectomy or transvaginal sacrospinous uterine suspension for uterine prolapse: a comparison. J Reprod Med 2005; 50:669-74
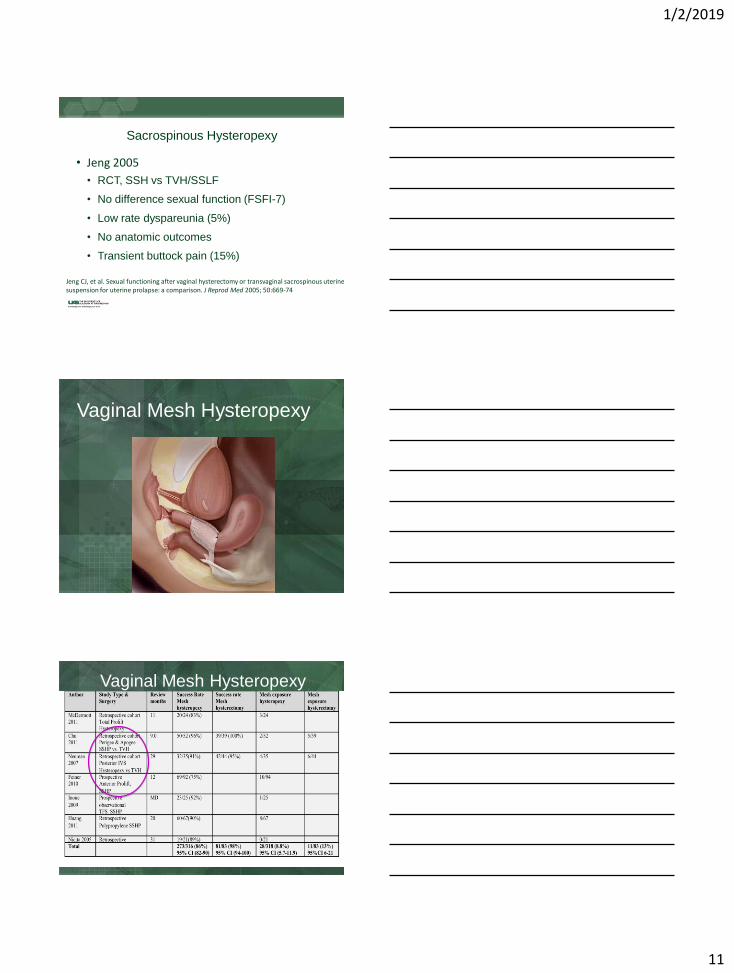
Vaginal Mesh Hysteropexy
Vaginal Mesh Hysteropexy
1/2/2019
12
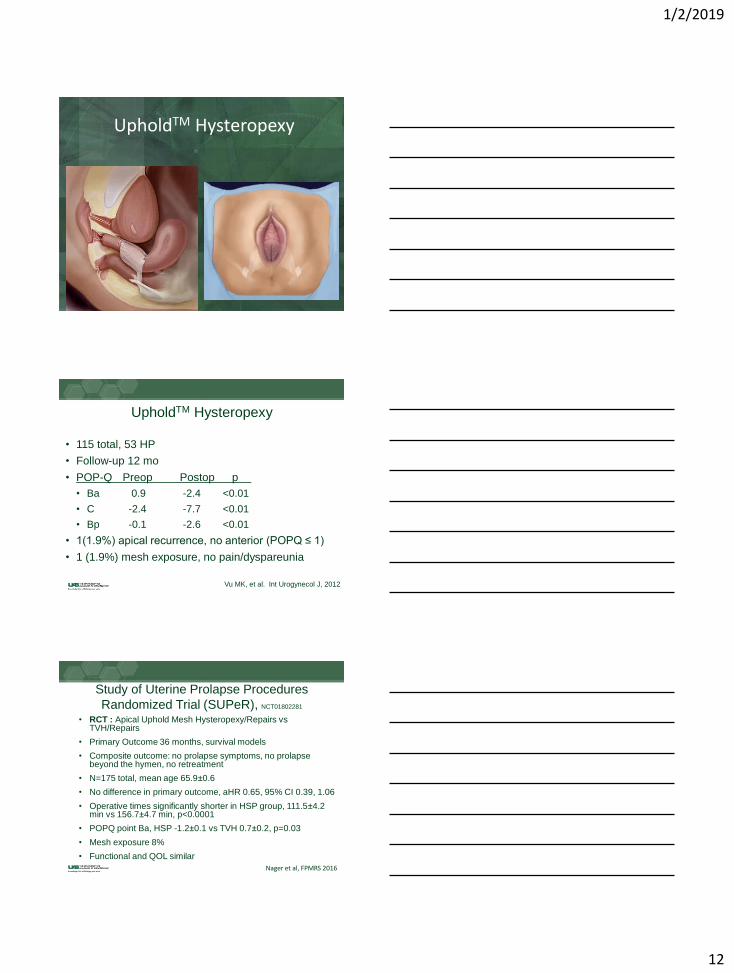
UpholdTM Hysteropexy
UpholdTM Hysteropexy
• 115 total, 53 HP
• Follow-up 12 mo
• POP-Q Preop Postop p
• Ba 0.9 -2.4 <0.01
• C -2.4 -7.7 <0.01
• Bp -0.1 -2.6 <0.01
• 1(1.9%) apical recurrence, no anterior (POPQ ≤ 1)
• 1 (1.9%) mesh exposure, no pain/dyspareunia
Vu MK, et al. Int Urogynecol J, 2012
Study of Uterine Prolapse Procedures
Randomized Trial (SUPeR), NCT01802281
• RCT : Apical Uphold Mesh Hysteropexy/Repairs vs TVH/Repairs
• Primary Outcome 36 months, survival models
• Composite outcome: no prolapse symptoms, no prolapse beyond the hymen, no retreatment
• N=175 total, mean age 65.9±0.6
• No difference in primary outcome, aHR 0.65, 95% CI 0.39, 1.06
• Operative times significantly shorter in HSP group, 111.5±4.2 min vs 156.7±4.7 min, p<0.0001
• POPQ point Ba, HSP -1.2±0.1 vs TVH 0.7±0.2, p=0.03
• Mesh exposure 8%
• Functional and QOL similar
Nager et al, FPMRS 2016

1/2/2019
13
Pregnancy and Hysteropexy
• Pessary first line
• Limited information counselling patients desiring
future pregnancy
• No data regarding which hysteropexy better for:
• Fertility
• Pregnancy & delivery
• Postpartum support & durabilityCavkaytar et al, 2017
How Do I Choose a Vaginal Uterine-Sparing
Approach?• Desires future fertility
• Vaginal SSH
• Completed childbearing and sexually active
• Vaginal SSH, TV mesh hysteropexy
• Done with childbearing and not sexually active
• LeFort Colpocleisis
• Other obliterative approach (SSH/obliterative
closure)
1/2/2019
14
Conclusion• Uterine conservation is a reasonable option and
would discuss all options with patients
• Proper patient selection
• Limited long-term data
• Subsequent hysterectomy may be challenging
• Currently not standard of care-increasingly being
offered and performed
• Better results: data would support mesh anterior
compartment; need longer term outcomes of RCTs
• Risk failure: Stage 4/cervical elongation
For more information on active
studies
Please visit our Urogynecology table:
Kathy Carter, RN, BSN
Jill Hyde, RN, BSN
Robin Willingham, RN, BSN
Call: 205-934-5498
Select References• Korbly NB, Kassis NC, Good MM, et al. Patient preferences for uterine preservation
and hysterectomy in women with pelvic organ prolapse. Am J Obstet Gynecol
2013;209:470.e1-6.
• Madsen AM, Raker C, Sung VW. Trends in hysteropexy and apical support for
uterovaginal prolapse in the United States from 2002 to 2012. Female Pelvic Med
Reconstr Surg 2017;23: 365-371
• Meriwether KV, Antosh DD, Olivera et al. Uterine preservation vs hysterectomy in
pelvic organ prolapse surgery: a systematic review with meta-analysis and clinical
practice guidelines. Am J Obstet Gynecol 2018; 219(2):129-146
• Ünlübilgin E, Sivaslioglu AA, Ilhan TT, Kumtepe Y, Dölen I. Which one is the
appropriate approach for uterine prolapse: Manchester procedure or vaginal
hysterectomy? Turkiye Klinik J Med Sci 2013;33:321-5
• Romanzi, L.J., Tyagi, R. Hysteropexy compared to hysterectomy for uterine prolapse
surgery: does durability differ?. Int Urogynecol J. 2012;23:625–631
• Richardson DA, Scotti RJ, Ostergard DR. Surgical management of uterine prolapse in
young women. J Reproduc Med. 1989 Jun;34(6):388-92
• Dietz, V., van der Vaart, C.H., van der Graaf, Y., Heintz, P., Schraffordt Koops, S.E.
One-year follow-up after sacrospinous hysteropexy and vaginal hysterectomy for
uterine descent: a randomized study. Int Urogynecol J. 2010;21:209–216
1/2/2019
15
Select References• Detollenaere, R.J., den Boon, J., Stekelenburg, J. et al, Sacrospinous hysteropexy vs vaginal
hysterectomy with suspension of the uterosacral ligaments in women with uterine prolapse stage 2 or higher: multicentre randomised non-inferiority trial. BMJ. 2015;351:h3717
• Jeng, C.J., Yang, Y.C., Tzeng, C.R., Shen, J., Wang, L.R. Sexual functioning after vaginal
hysterectomy or transvaginal sacrospinous uterine suspension for uterine prolapse: a comparison.
J Reprod Med. 2005;50:669–674
• Maher, C.F., Cary, M.P., Slack, M.C., Murray, C.J., Milligan, M., Schluter, P. Uterine preservation or
hysterectomy at sacrospinous colpopexy for uterovaginal prolapse?. Int Urogynecol J Pelvic Floor
Dysfunct. 2001;12:381–384 (discussion 384-5)
• Lo, T.S., Pue, L.B., Hung, T.H., Wu, P.Y., Tan, Y.L. Long-term outcome of native tissue
reconstructive vaginal surgery for advanced pelvic organ prolapse at 86 months: Hysterectomy vs
hysteropexy. J Obstet Gynaecol Res. 2015;41:1099–1107
• Maher, C., Baessler, K., Glazener, C.M., Adams, E.J., Hagen, S. Surgical management of pelvic organ prolapse in women: a short version Cochrane review. Neurourol Urodyn. 2008;27:3–12
• Cavkaytar S, Kokanalı MK, Tasdemir U, Doganay M, Aksakal O. Pregnancy outcomes after
transvaginal sacrospinous hysteropexy. Eur J Obstet Gynecol Reprod Biol. 2017 Sep;216:204-207
• Nager CW, Zyczynski H, Rogers RG, Barber MD, Richter HE, Visco AG, Rardin CR, Harvie H,
Wallace D, Meikle SF; Pelvic Floor Disorders Network. The Design of a Randomized Trial of
Vaginal Surgery for Uterovaginal Prolapse: Vaginal Hysterectomy With Native Tissue Vault
Suspension Versus Mesh Hysteropexy Suspension (The Study of Uterine Prolapse Procedures
Randomized Trial). Female Pelvic Med Reconstr Surg. 2016 Jul-Aug;22(4):182-9
•
•







