Preoperative Assessment forPreoperative Assessment forNonNon--Cardiac SurgeryCardiac Surgery
Kim A. Eagle, MDAlbion Walter Hewlett Professor
Director
Kim A. Eagle, MDKim A. Eagle, MDAlbion Walter Hewlett ProfessorAlbion Walter Hewlett Professor
DirectorDirector
University of MichiganUniversity of MichiganCardiovascular CenterCardiovascular Center

Kim A. Eagle, MD, FACCKim A. Eagle, MD, FACCDirectorDirector
University of MichiganUniversity of MichiganCardiovascular CenterCardiovascular Center
Grants: NIH, Hewlett Foundation, Grants: NIH, Hewlett Foundation, Mardigian Foundation, Varbedian Fund, Mardigian Foundation, Varbedian Fund,
GOREGORE
Consultant: NIH NHLBIConsultant: NIH NHLBI

Lecture OutlineLecture Outline
• Estimating Patient Risk
• Causes of Perioperative Cardiac Events
• Role of Non Invasive Testing
• Medical Therapy
• Role of Revascularization
• Approach to Preoperative Screening
• Perioperative Management
• Final Comments

Estimation of the PatientEstimation of the Patient’’s Risks Risk
Functional Status
Surgery - Specific Risk
Proceed with Surgery
Clinical Markers
Eagle KA, et al. JACC Guidelines 2002;39:542-53.
Further Evaluation/Mgmt.
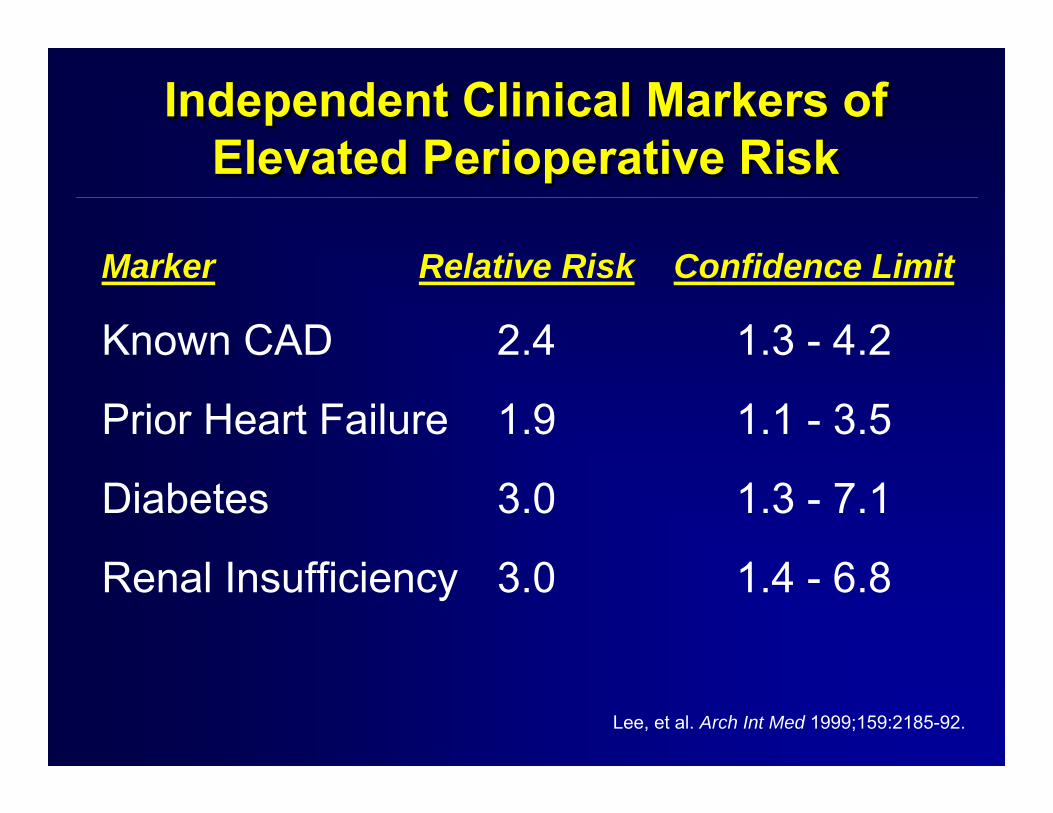
Independent Clinical Markers of Elevated Perioperative Risk
Independent Clinical Markers of Independent Clinical Markers of Elevated Perioperative RiskElevated Perioperative Risk
Marker Relative Risk Confidence Limit
Known CAD 2.4 1.3 - 4.2
Prior Heart Failure 1.9 1.1 - 3.5
Diabetes 3.0 1.3 - 7.1
Renal Insufficiency 3.0 1.4 - 6.8
Lee, et al. Arch Int Med 1999;159:2185-92.

Clinical Risk Status andVascular Surgery
Clinical Risk Status andClinical Risk Status andVascular SurgeryVascular Surgery
Clinical Risk Status
0%
5%
10%
Low Risk(0 markers)
Per
iop.
MI o
r Dea
th(n=1476)
0.3%Intermediate Risk
(1-2 markers)High Risk
(≥ 3 markers)
2.2%
8.5%
Poldermans et al. JACC 2006;48:964-969.

Higher
Functional StatusFunctional StatusFunctional Status
Lower
Risk
• Difficulty with ADL• Can’t walk four blocks or
up two flight of stairs• Inactive but no limitation• Active: Easily does
vigorous tasks• Performs regular
vigorous exercise
Eagle KA, et al. JACC Guidelines 2002;39:542-53.

Surgery - Specific RiskSurgery Surgery -- Specific RiskSpecific Risk
• Aortic• Non-Carotid Peripheral
Vascular• Major Thoracic• Major Abdominal• Carotid• Head/Neck• Orthopedic• Eye, Skin
Eagle KA, et al. JACC Guidelines 2002;39:542-53.
Higher
Lower
Risk

Operative MortalityOperative Mortality
Birkmeyer et al. N Engl J Med 2002;346:1128-37.
0
4
8
12
Carotid Endarterectomy
Lower-extremity bypass
Elective repair of abdominalaortic aneurysm
<40
40-69
70-10
911
0-164
>164 <22
22-39
40-60
61-94 >9
4
<17
17-30
31-49
50-79 >7
9
Adj
uste
d M
orta
lity
(%)
1.7 1.51.51.61.6
5.1
4.14.84.64.8
6.5
5.24.6 4.7
3.9

Independent Predictors of RiskIndependent Predictors of RiskIndependent Predictors of Risk
Surgery - High Risk
Poor Functional Status
Clinical Markers
(RR 2.8)
(RR 1.8)
Renal Insuf. (RR 3.0)
DM (RR 3.0)
HF (RR 1.9)
CAD (RR 2.4)

Who Needs FurtherNonInvasive Testing?Who Needs FurtherWho Needs Further
NonInvasive Testing?NonInvasive Testing?
Questions:
1. Will test results lead to change in care?
2. Has the patient been tested recently?
3. Is the concern related to CAD or is LV
Dysfunction a concern?
4. Can the patient do an exercise test?

Radionuclideventriculography 8 532 54 50 (32-69) 91 (87-96)Ambulatoryelectrocardiography 8 893 52 52 (21-84) 70 (57-83)Exerciseelectrocardiography 7 685 25 74 (60-88) 69 (60-78)Myocardial perfusionscintigraphy 23 3119 207 83 (77-89) 49 (41-57)Dobutamine stressechocardiography 8 1877 82 85 (74-97) 70 (62-79)Dipyridamole stressechocardiography 4 850 33 74 (53-94) 86 (80-93)
NonCardiac Testing Prior to Vascular NonCardiac Testing Prior to Vascular Surgery Meta Analysis Surgery Meta Analysis
Devereaux, P.J. et al. CMAJ 2005;173:627-634.
No. of No. of No. of Sensitivity, Specificity,Test studies patients events % (95% CI) % (95% CI)
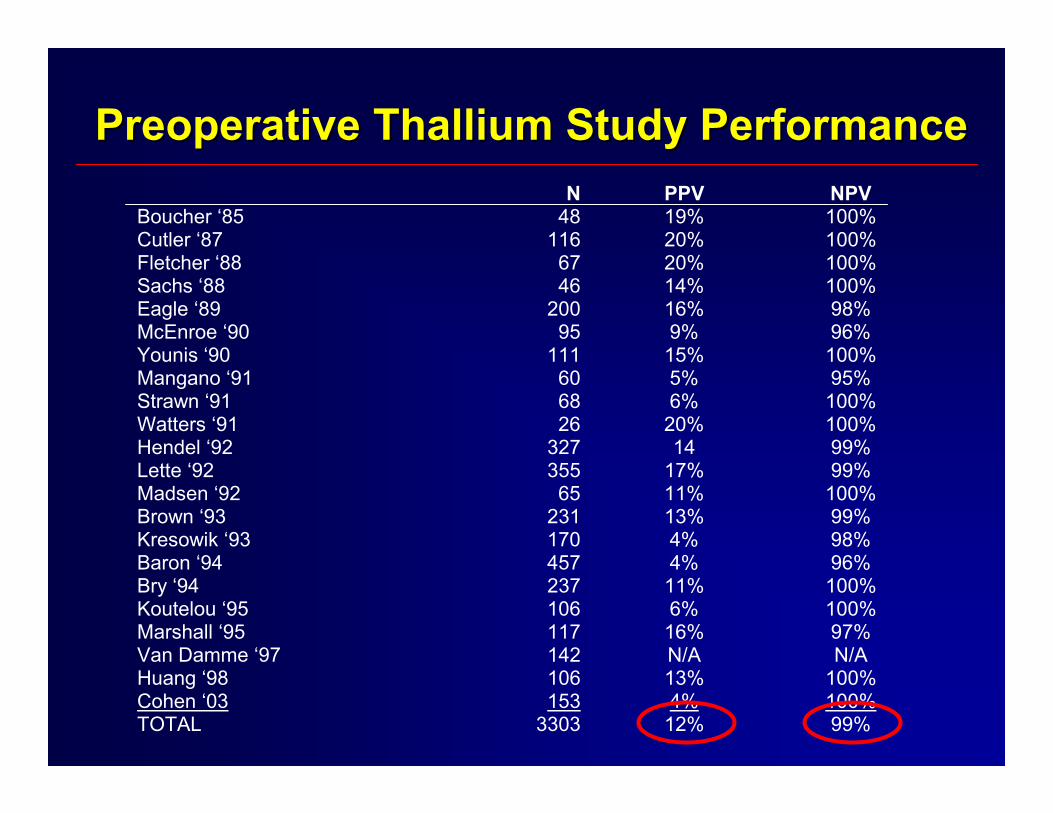
Preoperative Thallium Study PerformancePreoperative Thallium Study Performance N PPV NPV
Boucher ‘85 48 19% 100% Cutler ‘87 116 20% 100% Fletcher ‘88 67 20% 100% Sachs ‘88 46 14% 100% Eagle ‘89 200 16% 98% McEnroe ‘90 95 9% 96% Younis ‘90 111 15% 100% Mangano ‘91 60 5% 95% Strawn ‘91 68 6% 100% Watters ‘91 26 20% 100% Hendel ‘92 327 14 99% Lette ‘92 355 17% 99% Madsen ‘92 65 11% 100% Brown ‘93 231 13% 99% Kresowik ‘93 170 4% 98% Baron ‘94 457 4% 96% Bry ‘94 237 11% 100% Koutelou ‘95 106 6% 100% Marshall ‘95 117 16% 97% Van Damme ‘97 142 N/A N/A Huang ‘98 106 13% 100% Cohen ‘03 153 4% 100% TOTAL 3303 12% 99%

Preoperative Dobutamine Preoperative Dobutamine Echocardiogram PerformanceEchocardiogram Performance
N PPV NPV Lane ‘91 38 16% 100% Lalka ‘92 60 23% 93% Eichelberger ‘93 75 7% 100% Langan ‘93 74 17% 100% Poldermans ‘93 131 14% 100% Davila-Roman ‘93 Poldermans ‘95 Shafritz ‘97 Plotkin ‘98 Ballal ‘99 Bossone ‘99 Das ’00
88 302 42 80 233 46 530
10% 24% NA
33% 0% 25% 15%
100% 100% 97% 100% 96% 100% 100%
Boersma ’01 1097 14% 98% Morgan ’02 78 0% 100% Torres ’02 105 18% 98% Labib ’04 429 9% 98% TOTAL 466 20% 99%

No Yes Test
Can the patient exercise? ETT
Am I concerned about valve disease? Echo
Am I quantifying muscle at risk? Nuclear
Am I concerned about false positive? Echo
Am I concerned about LV? Echo/Nuke
Which Stress Test?Which Stress Test?Which Stress Test?
x
x
x
x
x
Role of CT and MR not yet clear

Clinical Assessment Only
1081 patients
Moderate8%(42/550)
(6-10%) (p<0.0001)
DypridomoleThallium
550 patients
Moderate9%(7/76)(4-18%)
(p<0.0001)
Low3%(11/345)
(2-6%)
High19%(24/129)
(13-26%)
Low3%(10/344)
(1-7%)
High18%(33/187)
(12-24%)Dypridomole
Thallium344 patients
DypridomoleThallium
187 patients
Moderate3%(1/33)(0-16%) (p=.610)
Low3%(9/281)
(2-6%)
High0%(0/30)(0-12%)
Moderate7%(2/31)(0-21%) (p=.107)
Low12%(3/25)(3-31%)
High24%(28/131)
(15-30%)
L’Italien G, et al. JACC 1996;27:779-786.
BayesTheorem

What Causes Perioperative Cardiovascular Events?
What Causes Perioperative What Causes Perioperative Cardiovascular Events?Cardiovascular Events?
• Catecholamine surges
• Prothrombotic milieau
• Blood Loss
• Volume Shifts
• Coronary Plaque destabilization
• Fixed Coronary Disease+
+Stress testing predicts only one of the six!


Coronary Stenosis Pathology(<50% X-section narrowing) Fatal Periop (MI)Left main 8 (19%)3-vessel disease 25 (59%)2-vessel disease w/LAD 11 (26%)2-vessel disease w/o LAD 1 (2.3%)1-vessel disease 1 (24%)No severe CAD 2 (4.7%)Plaque disturbed – 55%; more than half the time not the most severe stenosis
Fatal Perioperative MICoronary Pathology (n=42)
Fatal Perioperative MIFatal Perioperative MICoronary Pathology (n=42)Coronary Pathology (n=42)
Dawood MM et al. Intl J Cardiol 1996;57:37-44.

Medical Therapy to Reduce Perioperative Events
Medical Therapy to Reduce Medical Therapy to Reduce Perioperative EventsPerioperative Events
• Beta Adrenergic Blockers
• Statins
• Aspirin

Decrease Study DesignDecrease Study DesignDecrease Study Design
Elective Aortic SurgeryElective Aortic Surgery
Clinical Markers of RiskClinical Markers of Risk
Demonstrable IschemiaDemonstrable Ischemiaonon
Dobutamine EchoDobutamine Echo
BB--BlockerBlocker++ PlaceboPlacebo
NEJM 1994; 341:1749.
+Titrated over days/weeks

High risk vasc surgeryHigh risk vasc surgeryBisoprolol 7Bisoprolol 7--89 days pre89 days pre--op (mean 37)op (mean 37)
BetaBeta--blocker Rx (Bisoprolol)blocker Rx (Bisoprolol)11
PeriPeri--operative Managementoperative Management
1Poldermans D et al. NEJM 1999;341:1789
D(%) MI(%) p
CONT 17 17 0.02BIS 3.4 0 <0.001P<0.001
0 7 14 21 28Days after Surgery
Perc
enta
ge o
f Pat
ient
s
0
10
20
30
40Standard care
Bisoprolol
“I always like to use a
new drug before its
effectiveness wears off”- William Osler

Effect of Perioperative BEffect of Perioperative B--BlockadeBlockadein Nonin Non--cardiac surgery among Medicare beneficiariescardiac surgery among Medicare beneficiaries
Lindenaeur PK, Pekow P, Wang K, et al., Perioperative Beta Blocker Therapy and Mortality following major Non-cardiac Surgery. NEJM 2005;353:349-61.
AmongIdeal
MedicarePatients
Treatedwith
Beta Blockers(n=75,190)
Not treatedwith
Beta Blockers(n=260,238)
Mortality 2.73% 2.91%

Revised Cardiac Risk Death Rate Odds Ratio #Needed: Treat #Needed: HarmClinical SubgroupScore - 0 1.4% 1.36 - 208Score - 1
All 2.2% 1.09 - 504Diabetes 1.7% 1.28 - 209Isch. Hrt. Disease 2.0% 1.12 - 408Cerebro. Vasc. Dis. 9.0% 1.03 - 410Renal Insuff. 7.2% 1.01 - 1505High Risk Surgery 2.0% 0.94 864
Score - 2 3.9% 0.88 227Score - 3 5.8% 0.71 62Score - 4 7.4% 0.58 33
Targeting PerioperativeB-Blockers to the “Right” Patients
Targeting PerioperativeTargeting PerioperativeBB--Blockers to the Blockers to the ““RightRight”” PatientsPatients
Lindenaur PK, et al. NEJM 2005; 353:349-61.

Perioperative Ischemic EvaluationPOISE Trial
PPerieriooperative perative IsIschemic chemic EEvaluationvaluationPOISE TrialPOISE Trial
8351 Patients8351 Patients++
Toprol XLToprol XL100mg 2100mg 2--44
Hrs PreopHrs Preop→→30 Days30 Days
Randomized
PlaceboPlacebo
+ >45yrs of age+ >45yrs of ageHad or at risk forHad or at risk for
AtherosclerosisAtherosclerosis--82%82%Had CAD or PVDHad CAD or PVD
Toprol3.6%5.8%1.0%6.6%
Placebo5.1%6.9%0.5%2.4%
P-value<0.001
0.040.005
<0.001
30 Day EventNon Fatal MICV Death, MI, ♥ ArrestStrokeBradycardia
Devereaux PJ, et al. Lancet 2008: 371:1839-47.

POISE Trial: Metoprolol vs. Placebo in Patients Undergoing Noncardiac Surgery
POISE Trial: Metoprolol vs. Placebo in POISE Trial: Metoprolol vs. Placebo in Patients Undergoing Noncardiac SurgeryPatients Undergoing Noncardiac Surgery
5.8
6.9
3.12.3
0
2
4
6
8
CV Death, MI, or CardiacArrest HR 0.83
Total Mortality HR 1.33
MetoprololPlacebo
Devereaux PJ, et al. Lancet 2008;371:1839-47.
Perc
ent
P=0.04 P=0.03

Independent Postoperative Independent Postoperative Predictors of DeathPredictors of Death
Predictor HR 95% CI
Stroke 12.74 7.77-20.88
Hypotension 4.32 3.22-5.80
Symptomatic MI 3.51 2.02-6.11
Asymptomatic MI 2.80 1.87-4.19
Bradycardia 1.99 1.35-2.92
Bleeding 1.54 1.09-2.16

Negative Consequences ofSudden Discontinuation of Beta-
Blockers after Hip Surgery
Negative Consequences ofSudden Discontinuation of Beta-
Blockers after Hip Surgery
Van Klei et al. Anesthesiology 2009;111:717-24.

Fleisher L, et al. J Am Coll Cardiol 2007:50:1707-1732.
Recommendations for Beta-Blocker Medical Therapy
Class I1. Beta blockers should be continued in patients
undergoing surgery who are receiving beta blockers to treat angina, symptomatic arrhythmias, hypertension, or other ACC/AHA Class I guideline indications. (Level of Evidence: C)
2. Beta blockers should be given to patients undergoing vascular surgery who are at high cardiac risk owing to the finding of ischemia on preoperative testing. (Level of Evidence: B)

Durazzo et al. J Vasc Surg 2004;39:967.
Days after Surgery
RCT of StatinsRCT of Statins• 100 vascular
surgery patients
• 20mg atorvastatin or placebo for 45 days
• Vascular surgery an average of 30 days after randomization
0 30 60 90 120 150 180
50 44 43 41 40 40 40
50 38 36 35 34 33 33
0
20
40
60
80
100
Even
t-fre
e Su
rviv
al (%
)
Atorvastatin
Placebo
AtorvastatinPlacebo
P = 0.018

0%
2%
4%
In-hospital Mortality after Non-Cardiac Surgery: Lipid lowering therapy
In-hospital Mortality after Non-Cardiac Surgery: Lipid lowering therapy
2.13%
3.05%
Lipid Rx No Lipid Rx
(OR 0.71; 95% CI0.67-0.75)
Lindenauer PK, et al. JAMA 2004;291:2092-99.

Assessed for Eligibility(n=1669)
Assessed for EligibilityAssessed for Eligibility(n=1669)(n=1669)
N = 250N = 250 N = 247N = 247
AllocationAllocation
AnalysisAnalysis
FollowFollow--upup
Excluded (n=1172)Excluded (n=1172)Not meeting inclusion criteria Not meeting inclusion criteria (n=356)(n=356)Statin users (n=798)Statin users (n=798)Other reasons (n=18)Other reasons (n=18)
Dutch Echographic Cardiac Risk Evaluation Applying Stress Echo III
EnrollmentEnrollment
Lost to followLost to follow--up at 30 days (n= 0)up at 30 days (n= 0)Temporarily discontinued (n=54)Temporarily discontinued (n=54)Permanently discontinued (n=18)Permanently discontinued (n=18)
Lost to followLost to follow--up at 30 days (n=0)up at 30 days (n=0)Temporarily discontinued (n=61)Temporarily discontinued (n=61)Permanently discontinued (n=16)Permanently discontinued (n=16)
RandomizationRandomization
Allocated to Fluvastatin (n= 250)Allocated to Fluvastatin (n= 250)Received allocated interventionReceived allocated intervention
(n= 247)(n= 247)
Allocated to Placebo (n= 247)Allocated to Placebo (n= 247)Received allocated interventionReceived allocated intervention
(n= 246)(n= 246)

DECREASE IIIDECREASE III
Days after surgery
Placebo
Fluvastatin
0
3
6
9
12
15
0 5 10 15 20 25 30
Car
diac
dea
th o
r non
fata
l MI
(%)
P = 0.039
N Engl J Med. 2009;361:984.

45,00045,000
6,4606,460
1,4211,421
1,066(2.4%)
Eligible Eligible Excluded
38,540(86%)
5,039(78%)
355(25%)
Low or High Risk
Beta-Blocker and/or Statin Therapy
Informed Consent, Previous Participation
IncludedIncludedIncluded
DECREASE IVDECREASE IV
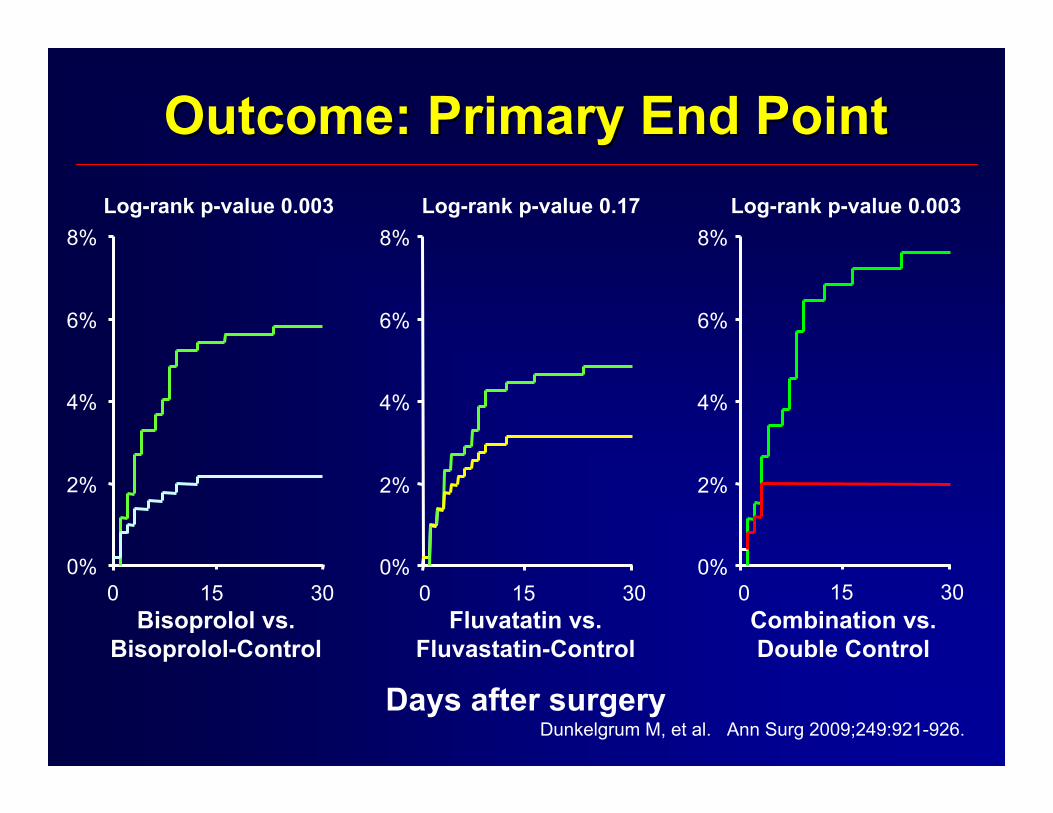
Outcome: Primary End PointOutcome: Primary End Point
Bisoprolol vs. Bisoprolol-Control
Days after surgery
Combination vs. Double Control
Fluvatatin vs. Fluvastatin-Control
Log-rank p-value 0.003 Log-rank p-value 0.17 Log-rank p-value 0.003
0%
2%
4%
6%
8%
0%
2%
4%
6%
8%
0 15 300%
2%
4%
6%
8%
15 300 15 30 0
Dunkelgrum M, et al. Ann Surg 2009;249:921-926.

Fleisher L, et al. J Am Coll Cardiol 2007:50:1707-1732.
Recommendations for Statin Therapy
Class I
1. For patients currently taking statins and scheduled for noncardiac surgery, statins should be continued. (Level of Evidence: B)
Class IIa
1. For patients undergoing vascular surgery with or without clinical risk factors, statin use is reasonable. (Level of Evidence: B)
What About Immediate
Coronary Revascularization
To Lower Risk?
What About Immediate
Coronary Revascularization
To Lower Risk?

Surgery After (bare metal) Stent Implantation –Methodist Hospital Houston
Kaluza et al, JACC 2000
0.0 0.0
28.0
32.0
0
20
40
1-14 days >14 days
MIMIDeath
P=0.015Surgery 1-14d
(n=25)Surgery 15-39d
(n=15)
Stent
• 8 deaths•6 due to MI•2 due to bleeding
• 11 bleeds• 3/5 pts operated on
ticlid died (1 bleed – 2 MI+ bleed)
Results Pt(%)
6 of 7 pts died (86%)

Death/MI after Non Cardiac SurgeryDeath/MI after Non Cardiac Surgeryin Patients with Recent Bare Metal Stentin Patients with Recent Bare Metal Stent
0%
1%
2%
3%
4%
5%
J Am Coll Cardiol 2003;42:234-40.
PCI ≤ 6 weeksBefore Surgery
PCI ≥ 7 weeksBefore Surgery
0%0%(0/39)(0/39)
4.8%4.8%(8/168)(8/168)

Stent Thrombosis AfterNonCardiac Surgery
Stent Thrombosis AfterNonCardiac Surgery
Anwaruddin S, et al. JACC Intv 2009;2:542-9.
Time from PCI with DES (yrs)
10
8
6
4
2
0
30 D
ay S
tent
Thr
ombo
sis
(%)
p = 0.014
0.00 0.25 0.50 0.75 1.00 1.25 1.50 1.75 2.00 2.25 2.50 2.75

CARP: Coronary Revascularization Prophylaxis before Major Vascular Surgery
CARP: Coronary Revascularization CARP: Coronary Revascularization Prophylaxis before Major Vascular SurgeryProphylaxis before Major Vascular Surgery
McFalls EO, et al. N Engl J Med 2004;351:2785-804.
Study PatientsStudy Patients(n=510; 8.7%)(n=510; 8.7%)
CoronaryCoronaryAngiographyAngiography
ScreeningScreeningProcessProcess
VascularVascularPatientsPatients
Anatomical Exclusions from the TrialAnatomical Exclusions from the Trial• Non-obstructive coronary arteries (n=363)• Not amenable to revascularization (n=215)• Left Main Stenosis > 50% (n=54)• LV Ejection Fraction < 20% (n=11)• Refusal (n=29)
Clinical Exclusions from the TrialClinical Exclusions from the Trial• Insufficient cardiac risk (n=1654)• Urgent/Emergent surgery (n=1025)• Prior CABG/PCI and no ischemia (n=626)• Co-morbid condition (n=731)• Refusal or non-eligible (n=633)
Surgical Indications for the TrialSurgical Indications for the Trial• Abdominal Aortic Aneurysm (n=1935)• Claudication (n=1528)• Rest Pain (n=981)• Tissue Loss (n=1415)
(n=5859)
(n=4669; 79.7%)
(n=380; 11.6%)

Baseline Clinical Variables: CARPBaseline Clinical Variables: CARPBaseline Clinical Variables: CARPClinical Variables Revascularization No Revascularization P-value
(N=258) (N=252)
HistoryAge (years) 65±11.1 67.2±10.4 0.099Angina (%) 39.9 37.7 0.606Prior MI (%) 43.0 40.9 0.623Prior CHF (%) 12.0 7.5 0.089Diabetes (%) 37.6 40.0 0.840
LaboratoryLDL (mg/dL) 105±37 107±42 0.596
Cardiac StatusLV Ejection Fraction 54±12 55±12 0.3633-vessel CAD (%) 35.4 31.4 0.685
Indications for SurgeryAbdominal aneurysm (%) 34.4 32.1 0.613Claudication (%) 38.8 35.3 0.613Rest pain (%) 11.6 13.9 0.613

CARP: Main ResultsCARP: Main ResultsCARP: Main ResultsRevasc. Revasc. No Revasc.No Revasc. PP--valuevalue(N=225)(N=225) (N=237)(N=237)
Surgical ManagementSurgical ManagementAbdominal Surgery (%)Abdominal Surgery (%) 39.939.9 42.142.1 0.8900.890Urgent or Emergent (%)Urgent or Emergent (%) 5.85.8 5.95.9 0.9000.900General anesthesia (%)General anesthesia (%) 81.181.1 84.384.3 0.4990.499
Perioperative MedicationsPerioperative MedicationsBetaBeta--adrenergic blockers (%)adrenergic blockers (%) 83.983.9 86.486.4 0.4480.448Aspirin (%)Aspirin (%) 76.176.1 70.070.0 0.1630.163Statins (%)Statins (%) 53.553.5 54.054.0 0.9250.925
Postoperative EventsPostoperative EventsDeath (%)Death (%) 3.13.1 3.43.4 0.8730.873MI (enzymes and ECG) (%)MI (enzymes and ECG) (%) 7.67.6 6.86.8 0.7370.737Loss of LimbLoss of Limb 0.50.5 0.90.9 0.1140.114
McFalls EO, et al. N Eng J Med 2004;351:2785-804.
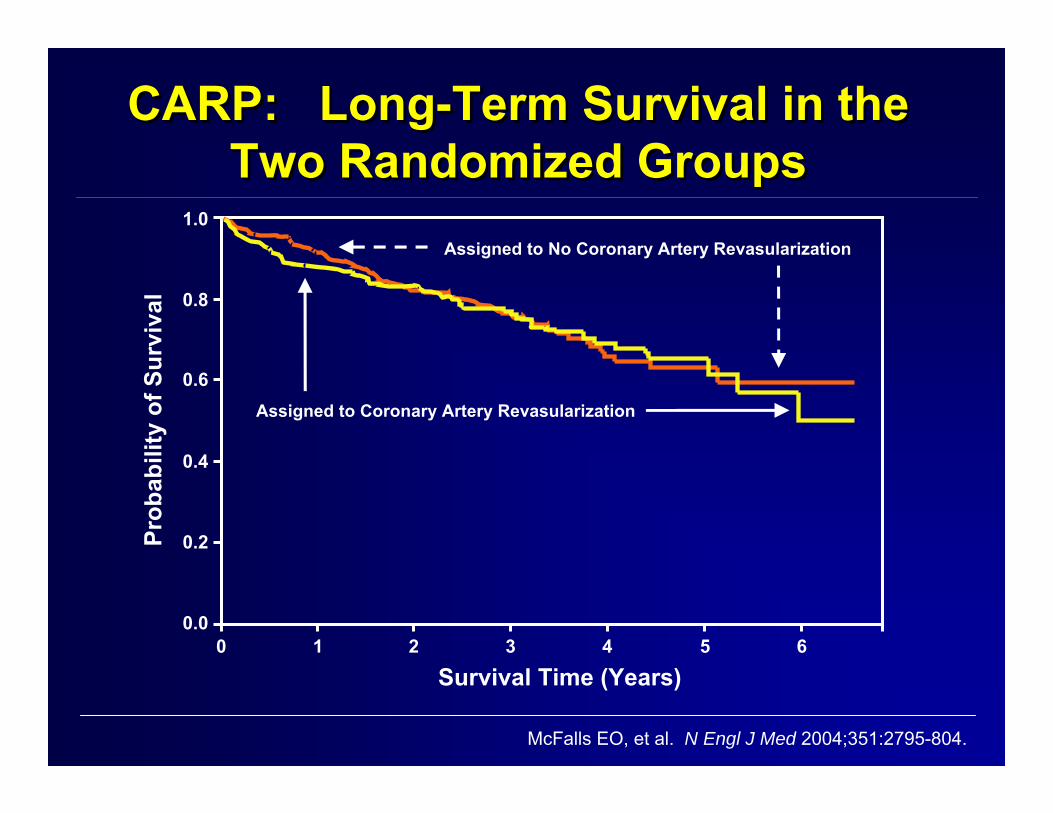
CARP: Long-Term Survival in theTwo Randomized Groups
CARP:CARP: LongLong--Term Survival in theTerm Survival in theTwo Randomized GroupsTwo Randomized Groups
McFalls EO, et al. N Engl J Med 2004;351:2795-804.
Assigned to No Coronary Artery Revasularization
Assigned to Coronary Artery Revasularization
Survival Time (Years)0 1 2 3 4 5 6
0.0
0.2
0.4
0.6
0.8
1.0
Prob
abili
ty o
f Sur
viva
l

Long Term Survival in CARP (2-5 Yrs)Long Term Survival in CARP (2Long Term Survival in CARP (2--5 Yrs)5 Yrs)
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
2-Vessel (N=204)
3-Vessel (N=130)
Left Main (N=48)
Prior CABG(N=225)
MedicalTreatment
PreoperativeRevascularization
Garcia S, et al. Am J Cardiol 2008;102:809-15.
Surv
ival
Pos
t-Vas
cula
r Sur
gery

Perioperative GuidelinesPerioperative GuidelinesPerioperative Guidelines
Treatment for patients requiring percutaneous coronary intervention who need subsequent surgery. ACS indicates acute coronary syndrome; COR, class of recommendation; LOE, level of evidence; and MI, myocardial infarction.
Fleisher L, et al. JACC 2007;50:1707-32.
Acute MI, highAcute MI, high--risk ACS, or highrisk ACS, or high--risk cardiac anatomyrisk cardiac anatomy
Bleeding riskBleeding riskof surgeryof surgery
Stent and continuedStent and continueddualdual--antiplateletantiplatelet
therapytherapy
14 to 29 days 30 to 365 days
Low
Greater than 365 days
BareBare--metalmetalstentstent
TimingofSurgery
DrugDrug--elutingelutingstentstent
BalloonBalloonangioplastyangioplasty
(COR IIb/LOE C) (COR IIa/LOE C) (COR IIb/LOE C)
(COR IIb/LOE C)Not Low
Fleisher L, et al. J Am Coll Cardiol 2007:50:1707-1732.
Coronary Revascularization before Non-Cardiac Surgery
Class III
It is not recommended that routine
prophylactic coronary revascularization
Be performed in stable CAD before non-
cardiac surgery.

Who Needs Coronary Angiography?Who Needs Coronary Angiography?
• Indicators are the same as for patients not being seen for preop evaluation
• Unstable or poorly controlled symptoms on medical Rx
• Stable patients with likelihood of advanced multivessel CAD +/- LV Dysfunction facing high stress surgery
Eagle KA, et al. JACC Guidelines 2002;30:542-63.

Who Should I ScreenWho Should I Screen
BeforeBefore
Non Cardiac Surgery?Non Cardiac Surgery?

Potential ApproachPotential ApproachPotential Approach1. Stable Clinical
Markers and/or Not Revascularization candidate
• Angina, q-waves, prior MI
– Beta Blocker + Statin + ASA
• Systolic heart failure– Beta Blocker,
ACE inhibitor, Aldo inhibitor
• Stress Echo• Rarely Cath if severe
ischemia in large regions• Best medical Rx based
on history & stress echo
2. Multiple Markers, established CAD or HF, and high risk surgery

Potential ApproachPotential ApproachPotential Approach
3.Unstable CAD and/or HF
• Cath
• Revascularize those eligible
• B-Blocker if HTN
• Statin if ↑ lipids
4.Non-cardiac markers only…DM, Age, ↑creatinine
Recommendations forPost-operative Surveillance
Recommendations forRecommendations forPostPost--operative Surveillanceoperative Surveillance
• Patients without evidence of CAD– Surveillance restricted to those who develop
perioperative signs of cardiovascular dysfunction
• Patients with known or suspected CAD, and undergoing high or intermediate risk procedure:
– ECG’s at baseline, immediately after procedure, and daily x 2 days
– Cardiac troponin measurements 24 hours postoperatively and on day 4 or hospital discharge (whichever comes first)
2002 ACC/AHA Guidelines for Perioperative Cardiovascular Evaluation for Noncardiac Surgery

Resource Use and Outcomes After Implementation of ACC/AHA Preoperative
Risk Assessment Guidelines
Resource Use and Outcomes After Resource Use and Outcomes After Implementation of ACC/AHA PreoperativeImplementation of ACC/AHA Preoperative
Risk Assessment GuidelinesRisk Assessment Guidelines
J Vasc Surg 2002;36:758-63.
Resource I II III P-value P-valueUtilization “Post “Late Post
“Controls” Guideline” Guideline” I vs. II I vs. III(n=102) (n=94) (104)
Stress Test 90 (88%) 44 (47%) 43 (41%) <0.001 <0.001
Coronary Angio. 24 (24%) 10 (11%) 11 (11%) <0.05 0.01
PTCA or CABG 24 (24%) 2 (2%) 6 (6%) <0.001 <0.001
Length of Stay 20.7 13.2 <0.001
PREOP Cost $1087 $171 <0.001
Cost per Case $21,947 $15,188 0.02

Resource Use and Outcomes After Implementation of ACC/AHA Preoperative
Risk Assessment Guidelines
Resource Use and Outcomes After Resource Use and Outcomes After Implementation of ACC/AHA PreoperativeImplementation of ACC/AHA Preoperative
Risk Assessment GuidelinesRisk Assessment Guidelines
J Vasc Surg 2002;36:758-63.
Resource I II III P-value P-valueUtilization “Post “Late Post
“Controls” Guideline” Guideline” I vs. II I vs. III
(n=102) (n=94) (104)
Outcomes
Death 4 (4%) 3 (3%) 0 (0%) 0.77
MI 7 (7%) 3 (3%) 5 (5%) 0.24
Death or MI 11 (11%) 4 (4%) 5 (5%) 0.08
““Prediction Is Very Difficult, Prediction Is Very Difficult,
Especially About The FutureEspecially About The Future””
-- Niels Bohr, Danish PhysicistNiels Bohr, Danish Physicist

Former President Bush VisitFormer President Bush VisitFormer President Bush Visit

““Medicine is an Art Medicine is an Art
of Uncertainty, and a of Uncertainty, and a
Science of ProbabilityScience of Probability””-- Sir William OslerSir William Osler







