
Current Status of Pancreas Versus Islet
TransplantationPros and Cons
UCSF Mini-Medical SchoolNovember 2019
Peter Stock MD PhDDepartment of SurgeryUniversity of California
San Francisco

IMPROVEMENTS IN RESULTS:
PANCREAS TRANSPLANTS
ISLET TRANSPLANTS
LONG TERM SUCCESS:
INSULIN INDEPENDENCE
NORMALIZATION OF HGB A1C
ABROGATION OF SECONDARY COMPLICATIONS
Rationale for ß-cell therapyRationale for ß-cell therapy


Relative Risk
15
13
11
9
7
5
3
1HbA1c, %
7 8 9 10 11 12
Neuropathy
Nephropathy
Retinopathy
DCCT Research Group. N Engl J Med. 1993;329:977-986.
Relationship of HbA1c to Risk of Microvascular Complications
Relationship of HbA1c to Risk of Microvascular Complications

John D. Pirsch, Jon S. Odorico & Hans W. Sollinger

Indications for Pancreas TxIndications for Pancreas Tx Diabetes Mellitus (T1 or T2) with:
Renal failure requiring simultaneous kidney transplant (SPK). 75-80%Functioning kidney transplant already on
immunosuppression (PAK). 5-10%Brittle diabetes with hypoglycemic
unawareness (PTA). 10-15%

IPTR/UNOS
International Pancreas Transplant Registry

PTR/UNOSIPTR/UNOSI
5-Year Unadjusted Patient SurvivalUSA Primary DD Pancreas Transplants, 1 /1/1982 – 12/31/2018
PTR/UNOSIPTR/UNOSI
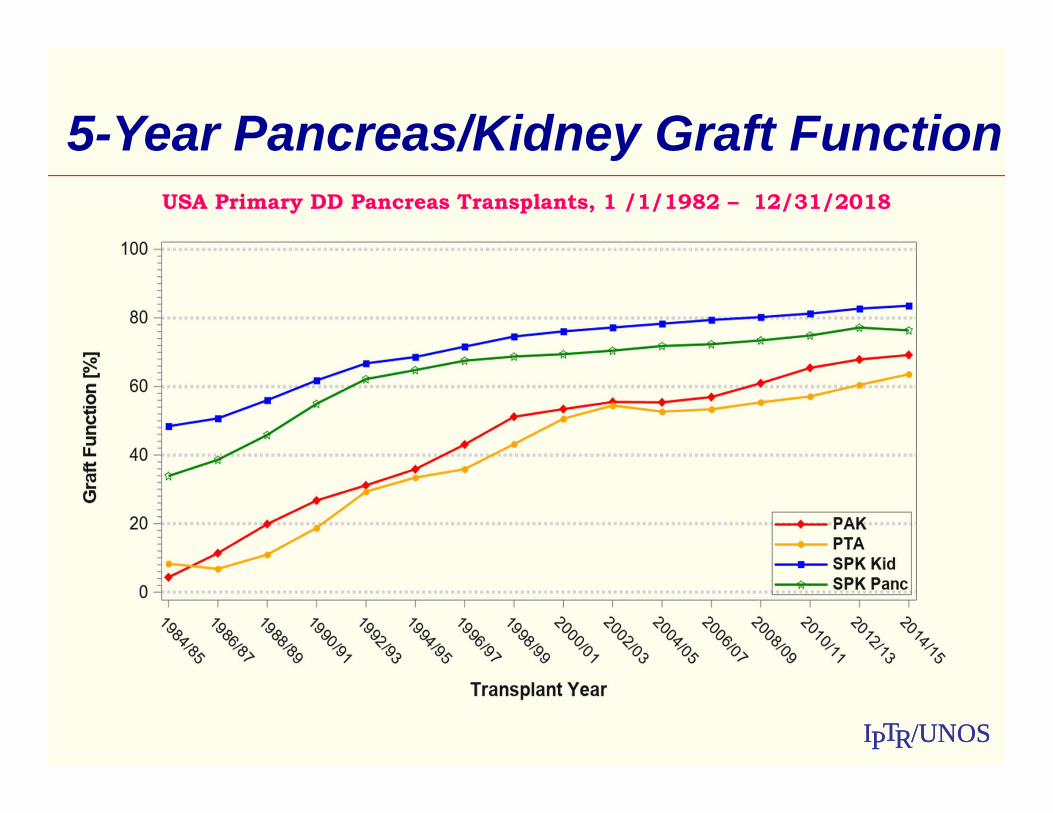
5-Year Pancreas/Kidney Graft FunctionUSA Primary DD Pancreas Transplants, 1 /1/1982 – 12/31/2018

UCSF Evolution in Immunosuppression for Pancreas/Kidney Transplantation
UCSF Evolution in Immunosuppression for Pancreas/Kidney Transplantation
1989-Current (>500 pancreas tx)ERA 1-3 : OKT3 Induction
ERA 4 : Thymoglobulin InductionMaintenance Incidence of rejection of either
kidney or pancreasERA 1: CSA/AZA/PRED 80%ERA 2: CSA/MMF/PRED 50%ERA 3: TACROLIMUS/MMF/PRED 15-20%
ERA 4: STEROID AVOIDANCE 10-15%Thymoglobulin Inductionlow dose tacrolimus/sirolimus/MMF

Typical Demographics for PancreasTransplant Recipients
Typical Demographics for PancreasTransplant Recipients
Recipients:Primary TxNon-highly sensitizedType 1 diabetic recipients <55 years of age BMI <30
Can we push the limits without impacting outcomes?

PTR/UNOSIPTR/UNOSI
1 Yr Pancreas Graft Function by Recip. Age
70
75
80
85
90
95
100
PAK
PTA
SPK
P<0.0001
P<0.0001
P<0.0001
20-29 30-39 40-49 50-59 60-69
USA Primary Pancreas Transplants in Type 1 DM 1/1/2010 – 12/31/2016
Age at Transplant [Yrs]
First World Consensus Conference on Pancreas TransplantationPTR/UNOSI05/17
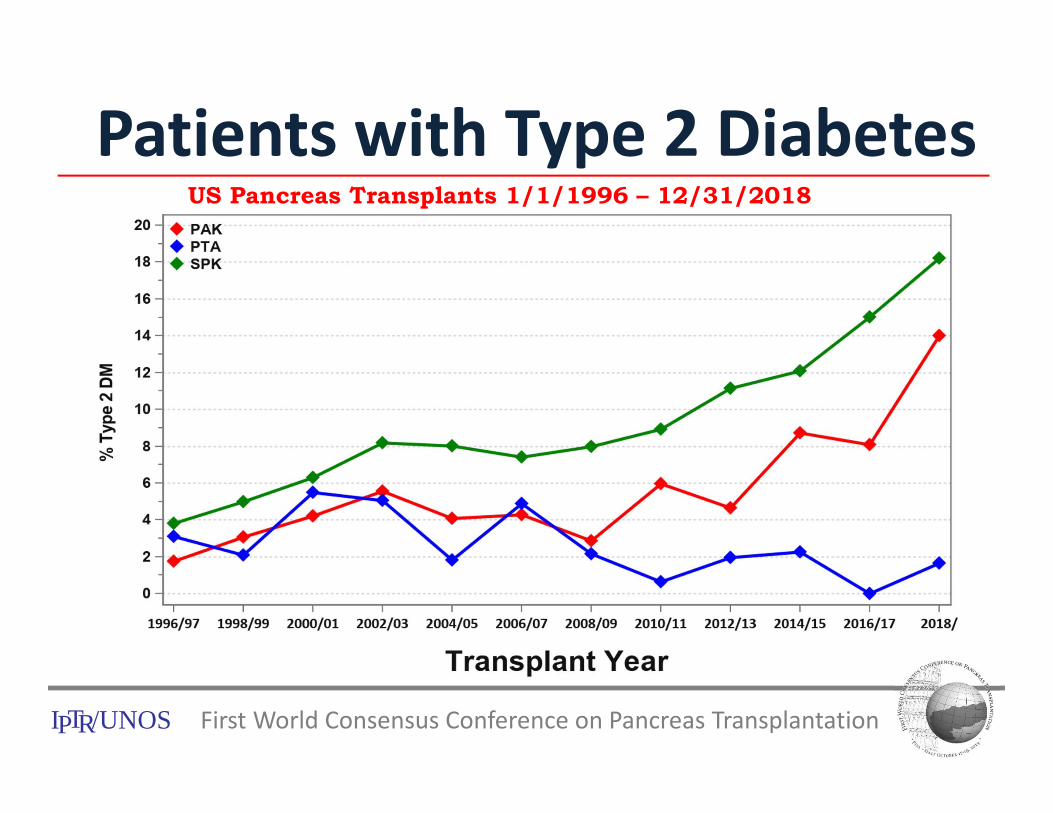
US Pancreas Transplants 1/1/1996 – 12/31/2018
Patients with Type 2 Diabetes
PTR/UNOSI
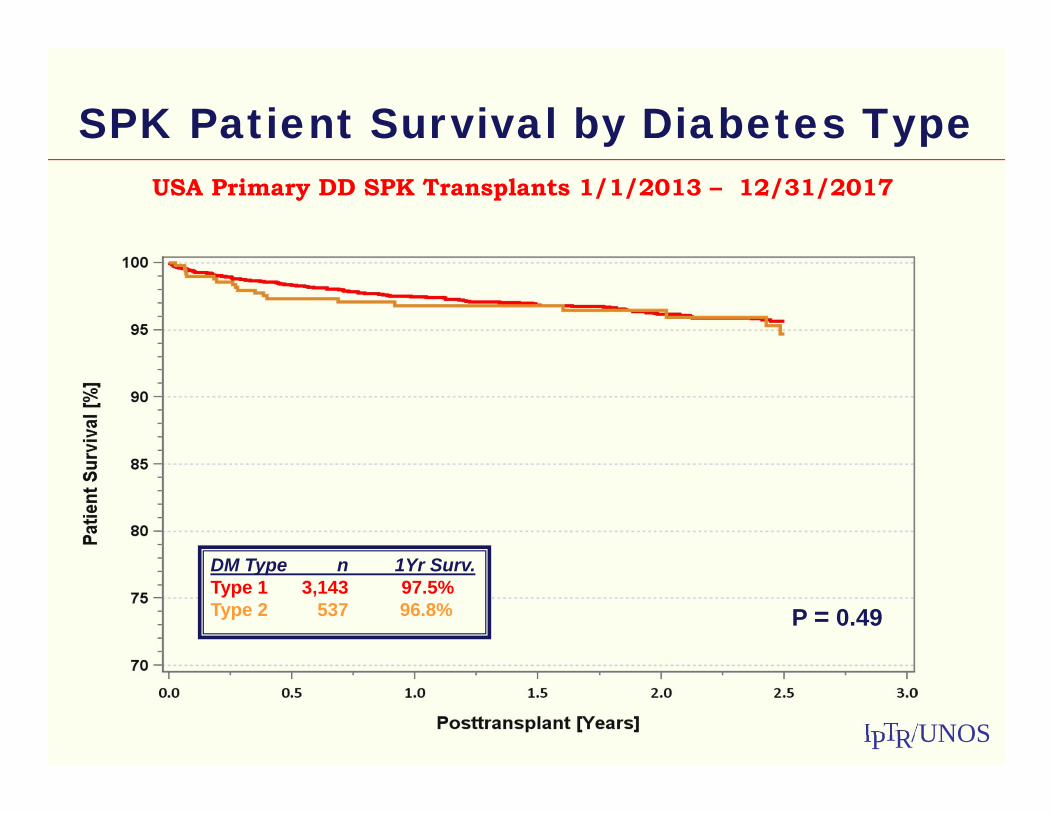
SPK Patient Survival by Diabetes TypeUSA Primary DD SPK Transplants 1/1/2013 – 12/31/2017
P = 0.49
DM Type n 1Yr Surv.Type 1 3,143 97.5% Type 2 537 96.8%
PTR/UNOSI
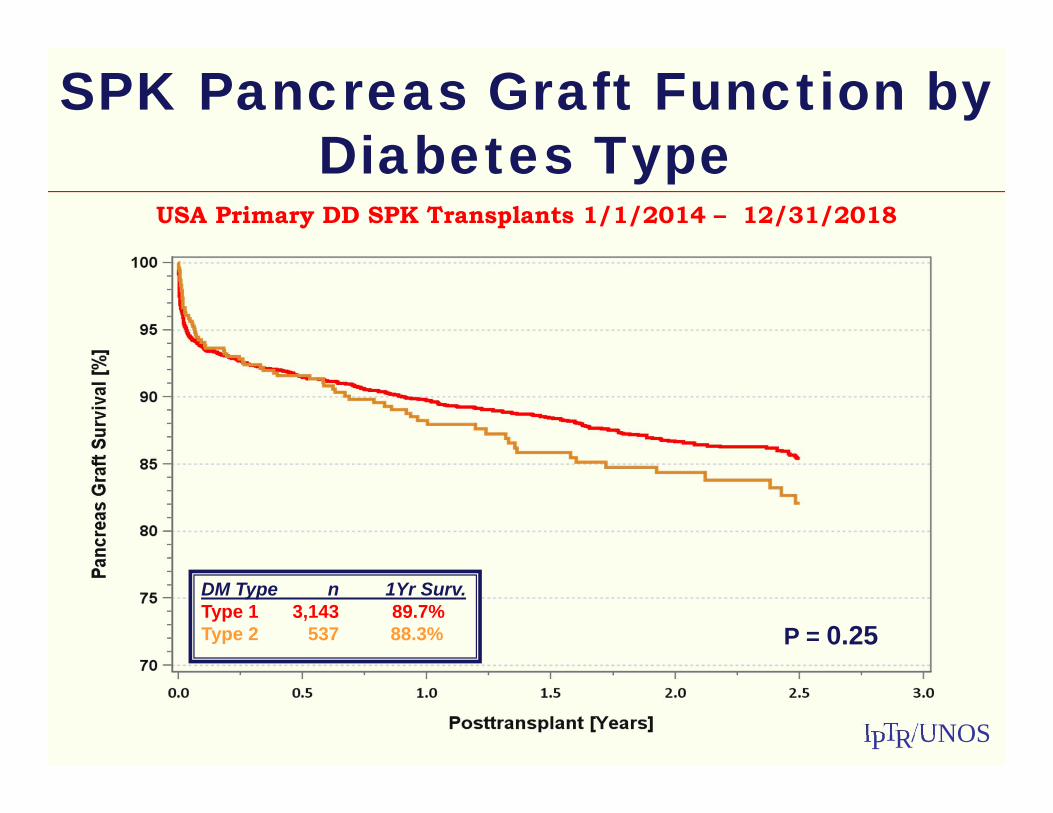
SPK Pancreas Graft Function by Diabetes Type
USA Primary DD SPK Transplants 1/1/2014 – 12/31/2018
DM Type n 1Yr Surv.Type 1 3,143 89.7% Type 2 537 88.3% P = 0.25

PTR/UNOSI
SPK Kidney Graft Function by Diabetes Type
USA Primary DD SPK Transplants 1/1/2014– 12/31/2018
P = 0.71
DM Type n 1Yr Surv.Type 1 3,143 96.1% Type 2 537 95.5%
PTR/UNOSIPTR/UNOSI
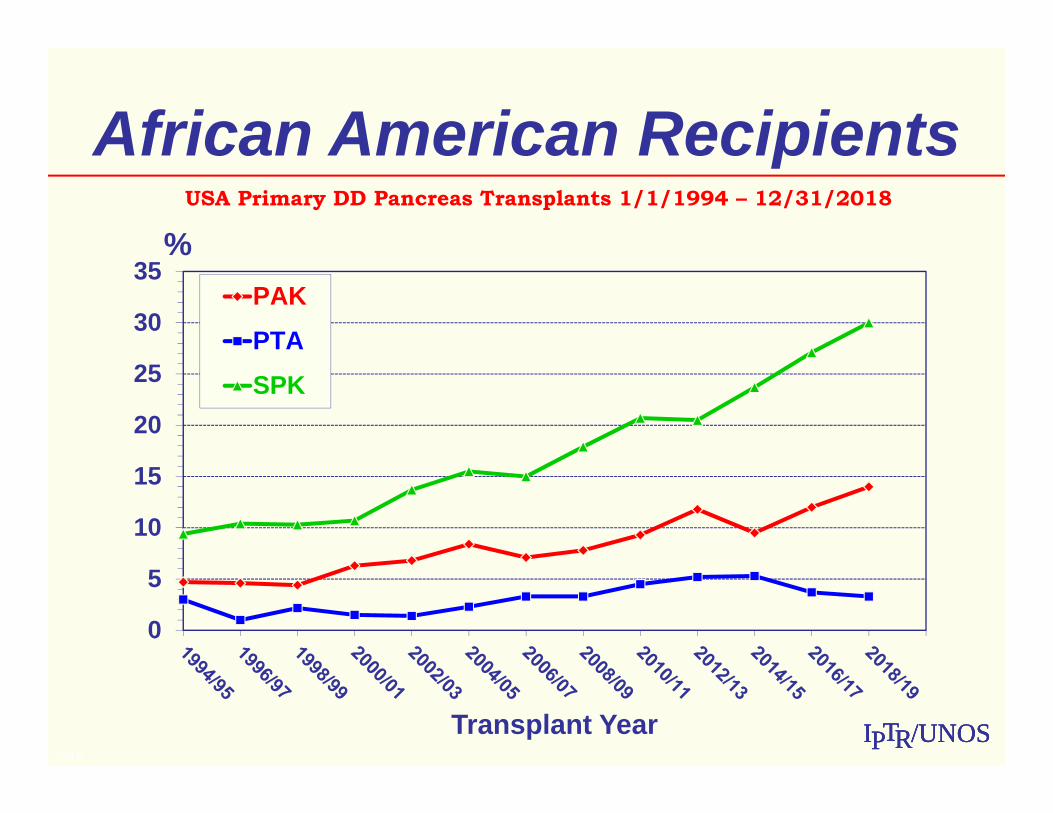
African American RecipientsUSA Primary DD Pancreas Transplants 1/1/1994 – 12/31/2018
2/16
0
5
10
15
20
25
30
35%
Transplant Year
PAK
PTA
SPK
PTR/UNOSI
SPK (n=7) and PAK (n=1)in people with Type 1 diabetes,
ESRD, and HIV infected
SPK (n=7) and PAK (n=1)in people with Type 1 diabetes,
ESRD, and HIV infected Standard immunosuppression for all SPK recipients
Thymo-induction, maintenance with TAC, MMF, Pred
Mean follow-up >4 years
Patient and Graft survival 100% at 1 and 3 years
2 deaths at 4 and 7 years secondary to cardiac events
2 pts with BK viremia – resolved with IS reduction
All recipients maintained insulin independence follow pancreas tx

THE PRO’S OF SUCCESSFUL PANCREAS TRANSPLANT
THE PRO’S OF SUCCESSFUL PANCREAS TRANSPLANT
Single organ tx
Euglycemia without the need for exogenous insulin
Prevents hypoglycemia
Normalizes HgbA1c
Improves patient quality of life
Reverses peripheral neuropathy
Prevents recurrent diabetic nephropathy (kidney damage) in transplanted kidneys
May prolong life
CONS OF PANCREAS TRANSPLANTATION:Cardiovascular risks
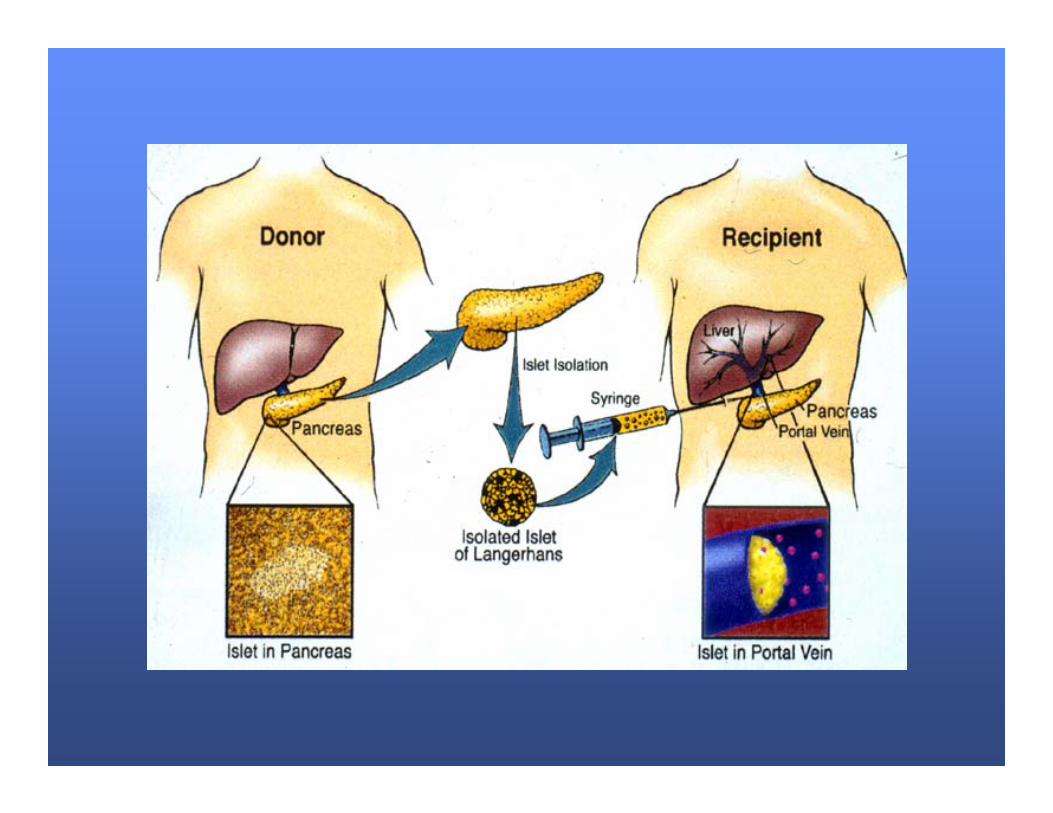
Why Transplant Islets?Are they replacing whole
organ transplants?
CONS OF PANCREAS TRANSPLANTATION:Cardiovascular risks
Why Transplant Islets?Are they replacing whole
organ transplants?
Safer, Simpler Procedure
than Pancreas Transplant


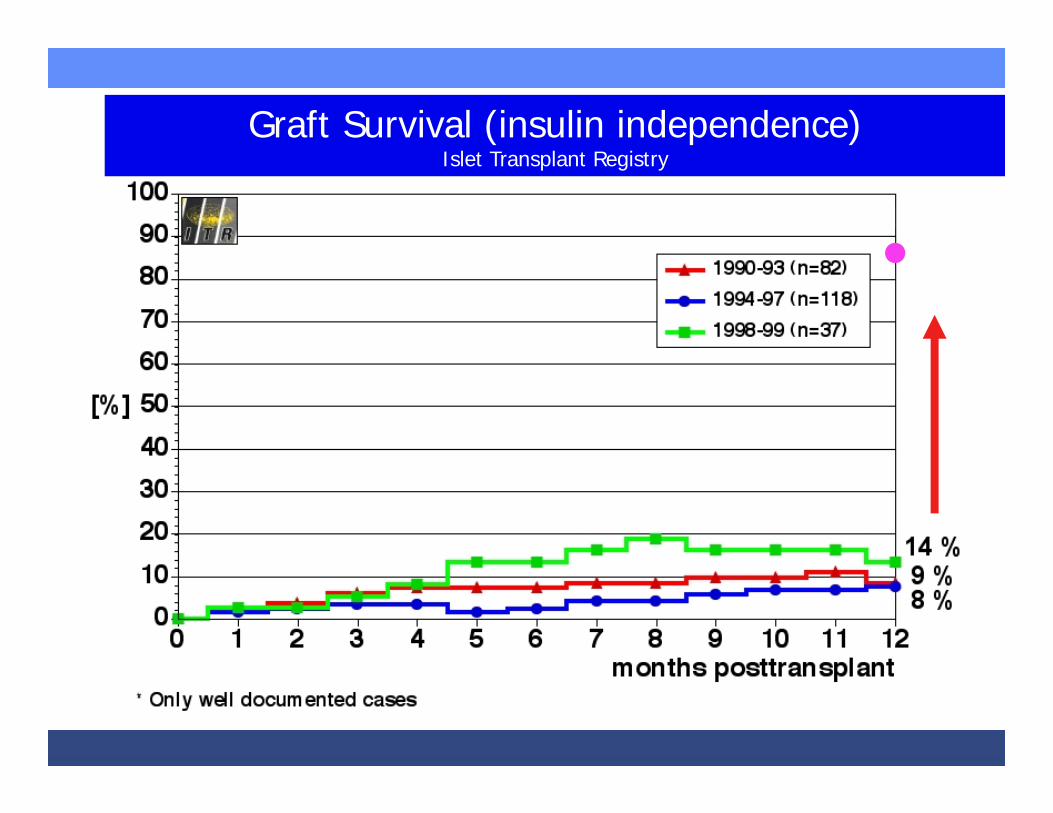
Graft Survival (insulin independence)Islet Transplant Registry
• 87%Edmonton

Ryan EA Diabetes 54:2060-2069, 2005

5-Year Insulin Independence5-Year Insulin IndependenceAuthor Center Immunosu-
ppressionReference Year 5-Year
Hering et al25
Minnesota Anti-CD3, Thymo, Etanercept
AJT 2012 50%
Shapiro et al26
Edmonton Thymo, Tacro, MMF
CJD 2012 79%
Szot et al UCSF Thymo/Efa or Bela, SRL+ MMF
ATC 2012 80 % (4 years)
Berney et al37
GRAGIL Basiliximab, SRL+ Tacro
Diabetes Care
2015 75%
Qi et al38 UIC Daclizumab, SRL + Tacro, +/-
Etancercept/Exenatide
ActaDiabetol
2014 60%
Pattou et al39
Lille Daclizumab, Basiliximab,Tacro + SRL
AJT 2018 58%

Islet recipient 3 years post transplant
modified from Vanthygem JCEM 2012
Glu
cose
(mg/
dL)
Glu
cose
(mg/
dL)T1DM patient on
intensive insulin tx
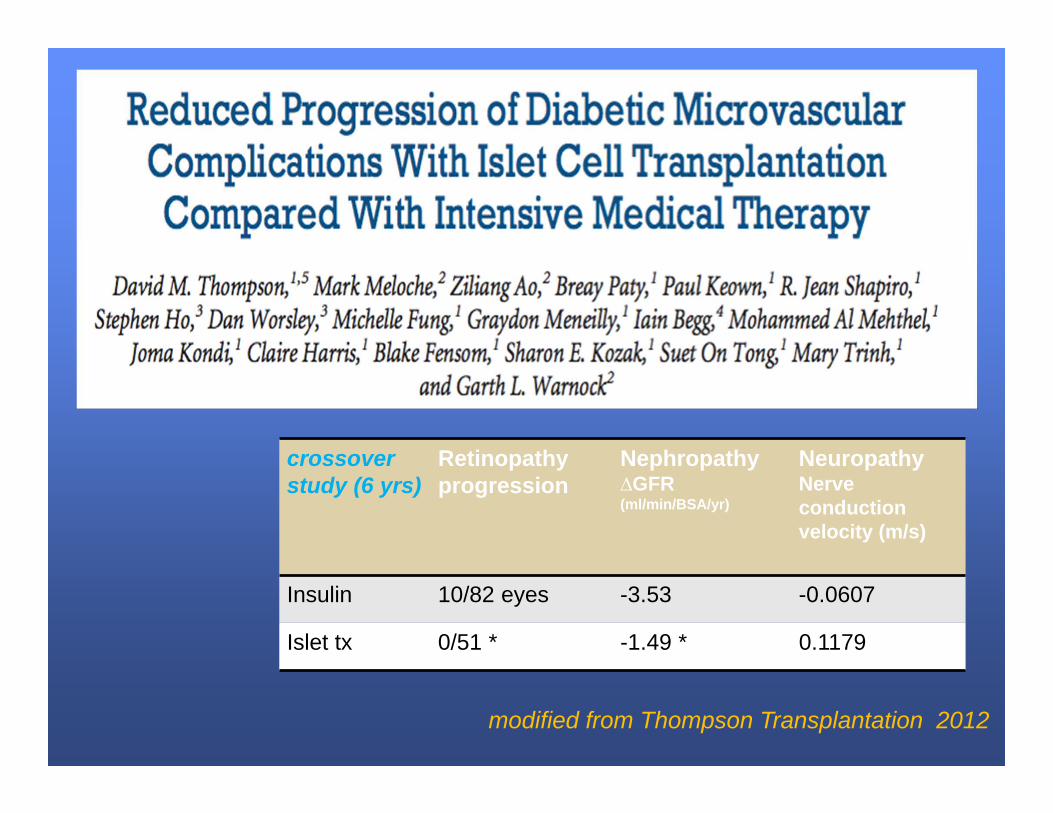
TitleTitle
crossover study (6 yrs)
Retinopathy progression
Nephropathy ∆GFR (ml/min/BSA/yr)
NeuropathyNerve conduction velocity (m/s)
Insulin 10/82 eyes -3.53 -0.0607
Islet tx 0/51 * -1.49 * 0.1179
modified from Thompson Transplantation 2012

Limitations of CNI and Steroid-Based IS in Islet Transplant
Limitations of CNI and Steroid-Based IS in Islet Transplant

Belatacept (Nulojix)Belatacept (Nulojix)
Belatacept (CTLA4‐Ig)IgG1‐Fc/CTLA4 fusion protein
binding CD80/86Competitive antagonist of
CD28 costimulationImproved long‐term outcomes
(43% reduction of death or graft loss at 7yrs) with BELA in renal transplant recipients relative to cyclosporine.
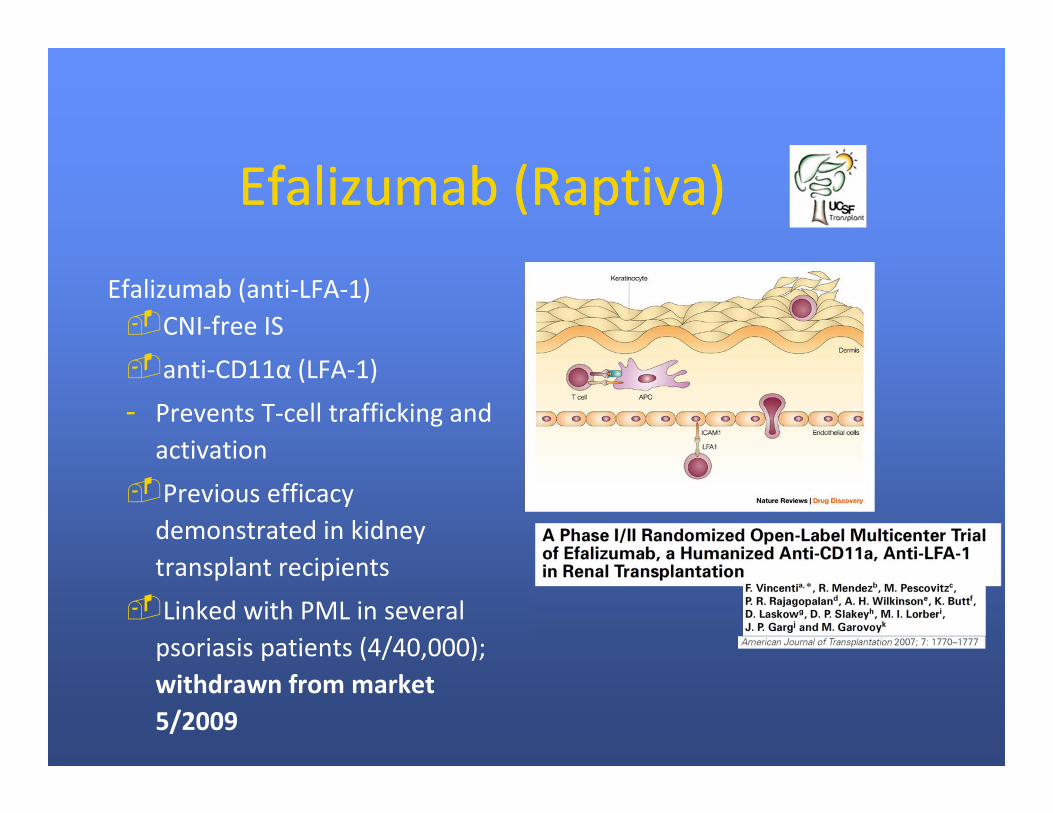
Efalizumab (Raptiva)Efalizumab (Raptiva)
Efalizumab (anti‐LFA‐1)CNI‐free ISanti‐CD11α (LFA‐1)- Prevents T‐cell trafficking and
activationPrevious efficacy
demonstrated in kidney transplant recipients
Linked with PML in several psoriasis patients (4/40,000); withdrawn from market 5/2009
0 365 730 1095 1460 1825 2190 2555 2920 3285 3650
EFA-5EFA-4EFA-3EFA-2EFA-1
BEL…BEL…BEL…BEL…BEL…
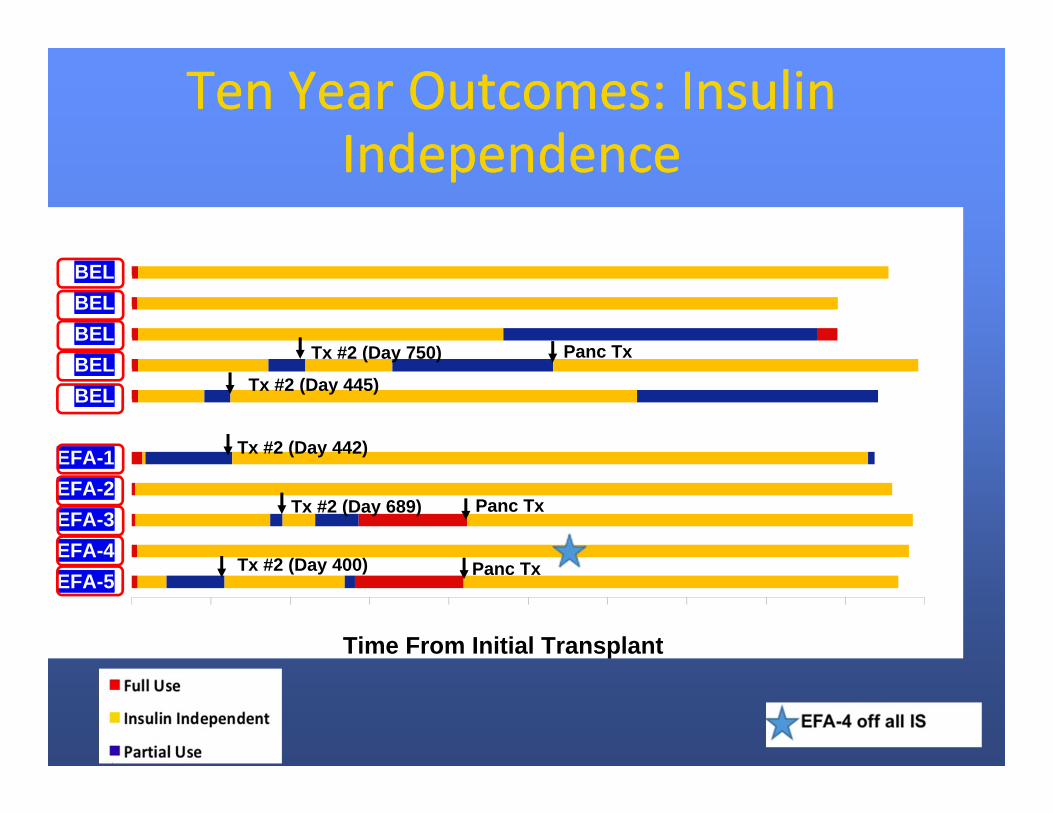
Ten Year Outcomes: Insulin Independence
Ten Year Outcomes: Insulin Independence
Time From Initial Transplant
Tx #2 (Day 442)
Tx #2 (Day 400)
Panc Tx
Panc Tx
Tx #2 (Day 689)
Tx #2 (Day 750)
Tx #2 (Day 445)
Panc Tx

HbA1c Levels after Islet TransplantationHbA1c Levels after Islet Transplantation
4.0
5.0
6.0
7.0
8.0
9.0
10.0
0 30 75 120 180 270 365 455 545 730
Time from Transplant (d)
HbA
1c (%
)
EFA-1
EFA-2
EFA-3
EFA-4
EFA-5
3.0
4.0
5.0
6.0
7.0
8.0
9.0
10.0
0 30 75 120 180 270 365 455 545 730
Time from Transplant (d)
HbA
1c (%
)
BELA-1
BELA-2
BELA-3
BELA-4
BELA-5
EfalizumabBelatacept

C-peptide Responses to a Mixed Meal Tolerance Test
C-peptide Responses to a Mixed Meal Tolerance Test
0
1
2
3
4
5
6
7
8
9
-10.0 -5.0 0.0 15.0 30.0 60.0 90.0 120.0
Time (minutes)
C -
Pept
ide
(ng/
ml) EFA 1
EFA 2
EFA 3
EFA 4
EFA 5
0
1
2
3
4
5
6
7
8
9
10
-10.0 -5.0 0.0 15.0 30.0 60.0 90.0 120.0
Time (minutes)
C -
Pept
ide
(ng/
ml) BELA 1
BELA 2
BELA 3
BELA 4
BELA 5
EfalizumabBelatacept
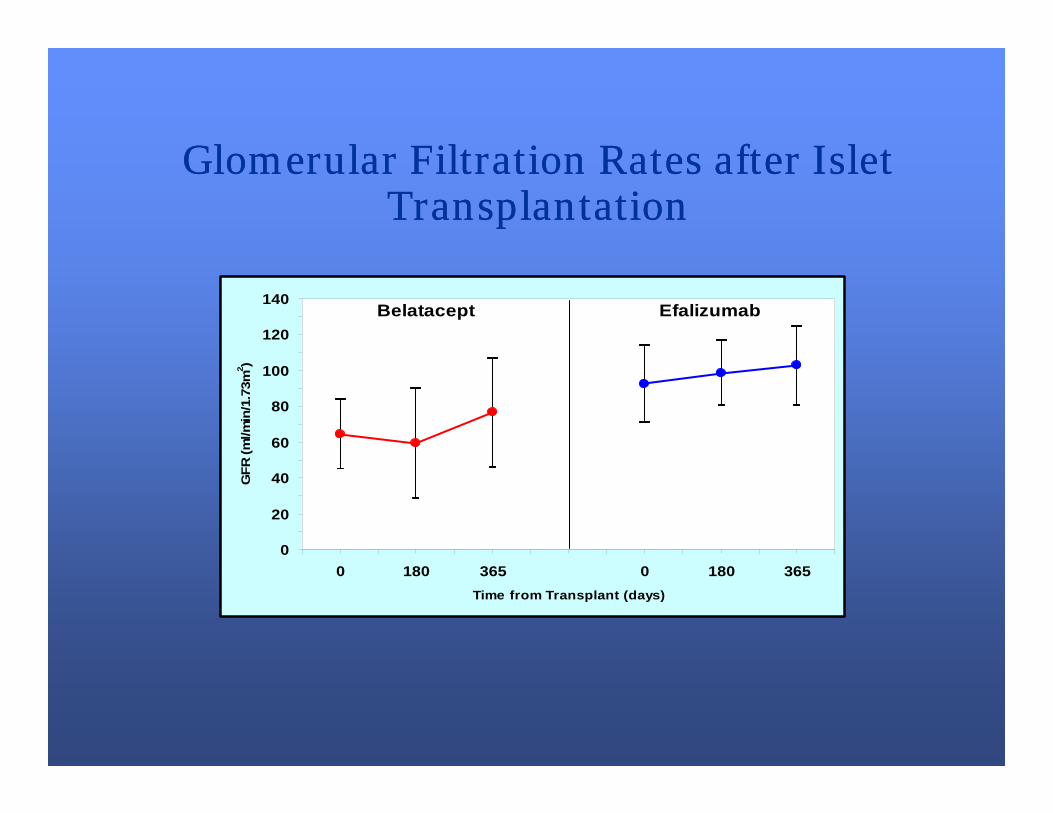
Glomerular Filtration Rates after Islet Transplantation
Glomerular Filtration Rates after Islet Transplantation
0
20
40
60
80
100
120
140
0 180 365 0 180 365Time from Transplant (days)
GFR
(ml/m
in/1
.73m
2 )
Belatacept Efalizumab

T Reg Kinetics in Islet RecipientsT Reg Kinetics in Islet Recipients
0
10
20
30
40
50
60
70
0 30 60 90 120 150 180 210 240 270 300 330 360
Time from Transplant (days)
% F
oxP3
+ of
CD
4+ T
cel
ls
EFA-1EFA-2EFA-3EFA-4EFA-5
0
10
20
30
40
50
60
70
0 30 60 90 120 150 180 210 240 270 300 330 360
Time from Transplant (days)
% F
oxP3
+ of
CD
4+ T
cel
ls
BELA-1BELA-2BELA-3BELA-4BELA-5
BelataceptEfalizumab

EFA-4: A Case of Operational Tolerance?
EFA-4: A Case of Operational Tolerance?
Long‐term insulin independence without immunosuppression Single islet transplant, insulin‐independent for 10 years. ATG induction, on EFA for 15 months, maintained on
sirolimus and MMF after EFA cessation.- Stopped all IS Sept 2012 following an episode of PTLD Tregs increased to 68% one month after transplant No detectable T‐cell response until 24 months, when both
effectors and Tregs re‐expanded. Remains insulin‐independent without immunosuppression,
despite demonstrable alloreactivity in vitro.

Beta Cell Replacement for PreuremicType 1 Diabetic Patients
Moassesfar, Stock, Posselt et al, 2016, AJT
Islet transplantation Whole pancreas transplantation
COST : PANCREAS TX ($ 134,748.08)ISLET TX ($ 138,872.27)
Beta Cell Supply is Severely Limited

Bruin, Rezania, KiefferScience Translational Medicine Dec 2015

From Kushner et al. Cell Stem Cell 2014
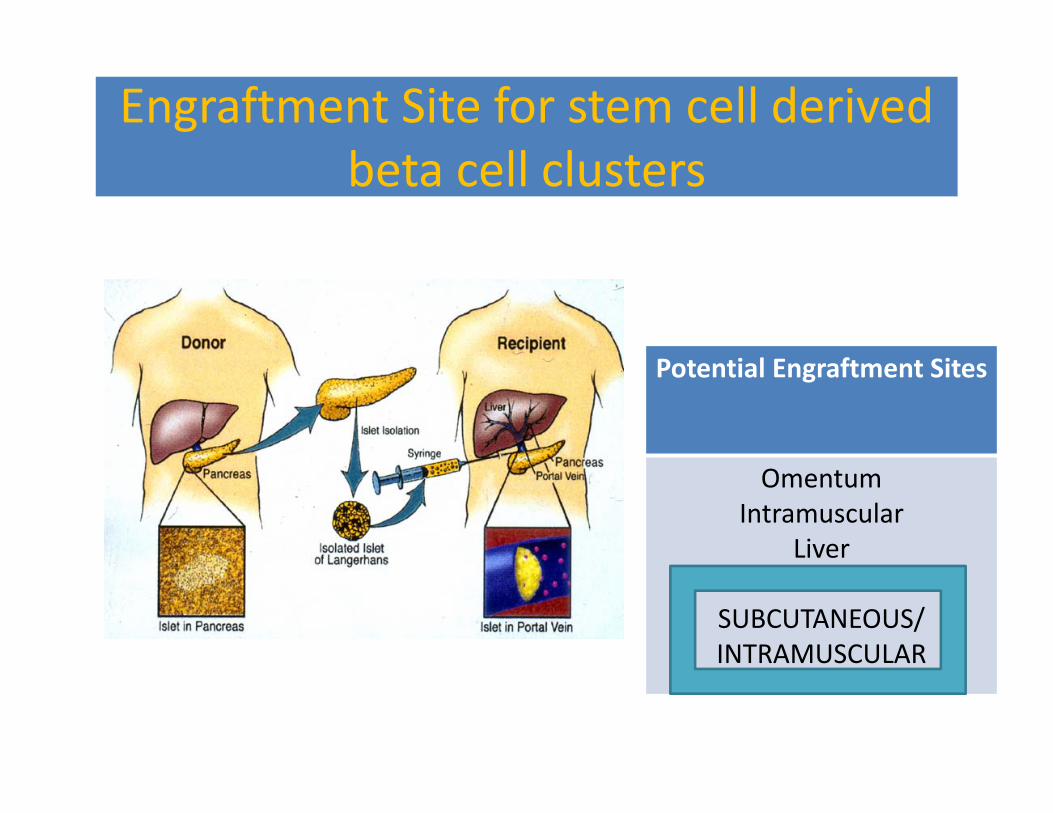
Engraftment Site for stem cell derived beta cell clusters
Potential Engraftment Sites
OmentumIntramuscular
Liver
SUBCUTANEOUS/INTRAMUSCULAR

Massive rejection-independent loss of islets
KC SQ
d0
d7
Luciferase‐expressing mouse isletsin syngeneic recipients
0
20
40
60
80
100
0 5 10 15 20%BLI o
f day 0
days
Kidney capsuleSubcutaneous
Faleo G, Tang Q
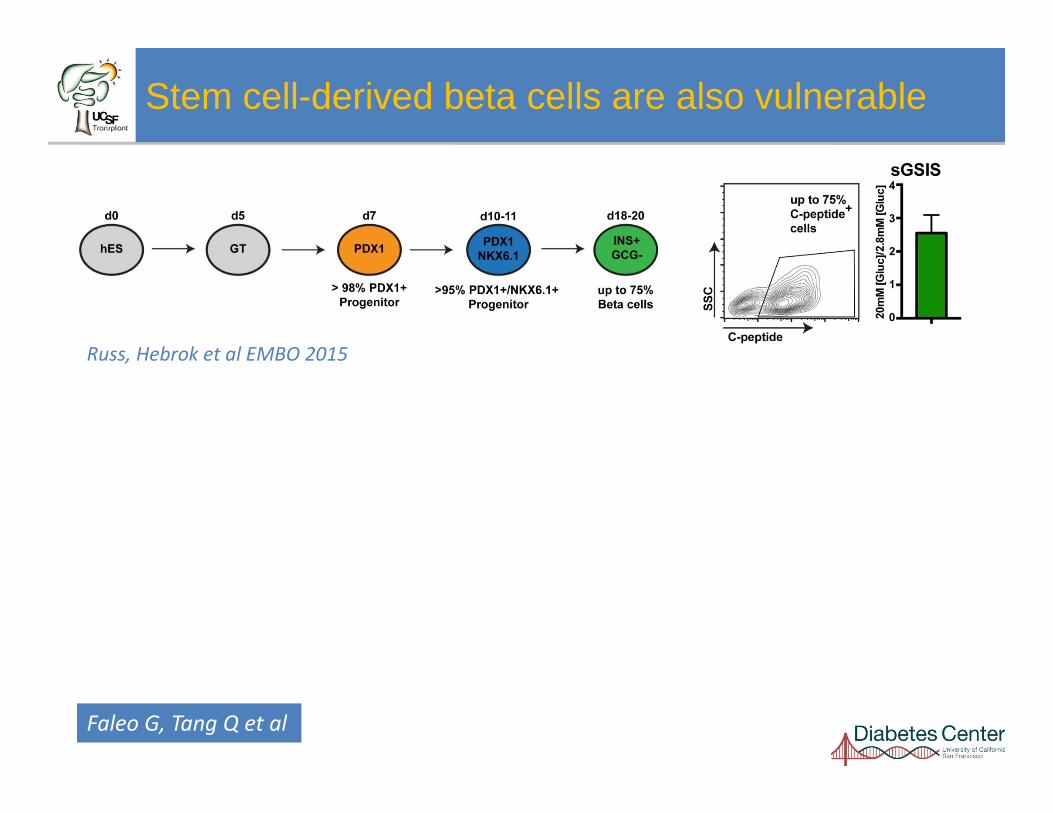
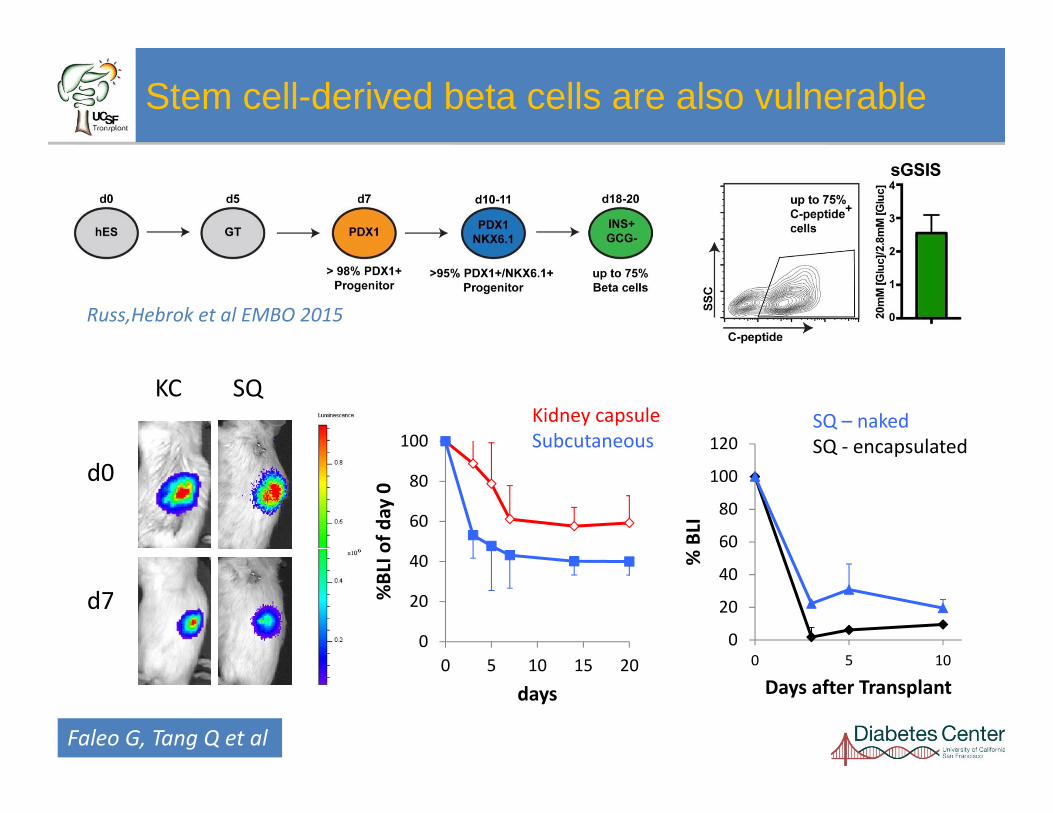
Stem cell-derived beta cells are also vulnerable
Russ, Hebrok et al EMBO 2015
Faleo G, Tang Q
Faleo G, Tang Q et al

Stem cell-derived beta cells are also vulnerable
KC SQ
d0
d7
Russ, Hebrok et al EMBO 2015
0
20
40
60
80
100
0 5 10 15 20
%BLI o
f day 0
days
Kidney capsuleSubcutaneous
Faleo G, Tang Q et al
Stem cell-derived beta cells are also vulnerable
KC SQ
d0
d7
Russ,Hebrok et al EMBO 2015
0
20
40
60
80
100
0 5 10 15 20
%BLI o
f day 0
days
Kidney capsuleSubcutaneous
0
20
40
60
80
100
120
0 5 10
% BLI
Days after Transplant
SQ – nakedSQ ‐ encapsulated
Faleo G, Tang Q et al

Making the Desert
Bloom….• Oxygenation• Nutrients• Pancreas-like niche• 3-dimensional
Scaffold• Parathyroid Tissue

Adult human islet: Minimal mass leads to reversal of diabetes in SQ
1000 human IEQ, 1/4 hPTG

Increased viability of Stem Cell Derived Beta Cell Cluster with
Parathryoid Gland Intra-Muscular (IM)
(5/5) NSG mice, 200 SCIPC’s; hPTG (1/4 gland) per mouse

Co-transplantation of Stem Cell Derived Beta Cell Clusters with PTG leads to diabetes reversal in IM after
6 weeks
0100200300400500600700800
Week4
Week6
Week10
Week12
Hum
an C
-pep
tide
(pg/
ml)
SCIPC SCIPC+PTG
(5/5) NSG mice, 1000 SCIPC clusters, 1/4 hPTG
InsulinDAPI

Translational Opportunities FACILITATED BY SUCCESSFUL
SUBCUTANEOUS/INTRAMUSCULAR SITE
- Allotransplantation
- Auto-islet transplantation
- Stem-cell based transplantation
- Xenotransplantation


PTR/UNOSIPTR/UNOSI
P < 0.0001
Waitlist Survival for Diabetic Patients USA Wait-List for Primary DD Transplants, 1/1/2005 –12/31/2018
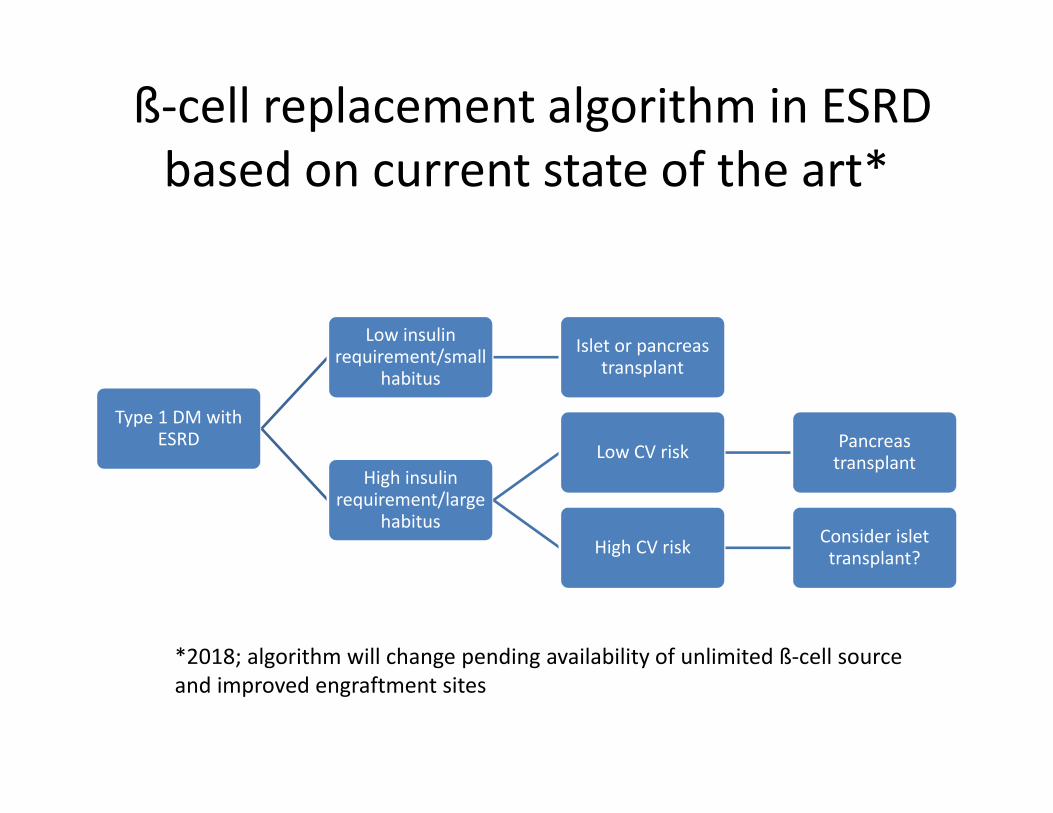
ß‐cell replacement algorithm in ESRD based on current state of the art*
Type 1 DM with ESRD
Low insulin requirement/small
habitus
Islet or pancreas transplant
High insulin requirement/large
habitus
Low CV risk Pancreas transplant
High CV risk Consider islet transplant?
*2018; algorithm will change pending availability of unlimited ß‐cell source and improved engraftment sites

ß‐cell replacement algorithm based on current state of the art in preuremic
patients*
Preuremic type 1 DM
Life‐threatening complications (e.g.
severe hypoglycemia)
High CV risk Islet transplant?
Low CV risk/small habitus
Islet or pancreas transplant
No life‐threatening complications
Continue medical management
*2018; algorithm will change pending availability of unlimited ß‐cell source and improved engraftment sites







