Download - Respiratory Tract Conditions
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams and Wilkins
Respiratory Tract ConditionsRespiratory Tract Conditions
Chapter 22
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams and Wilkins
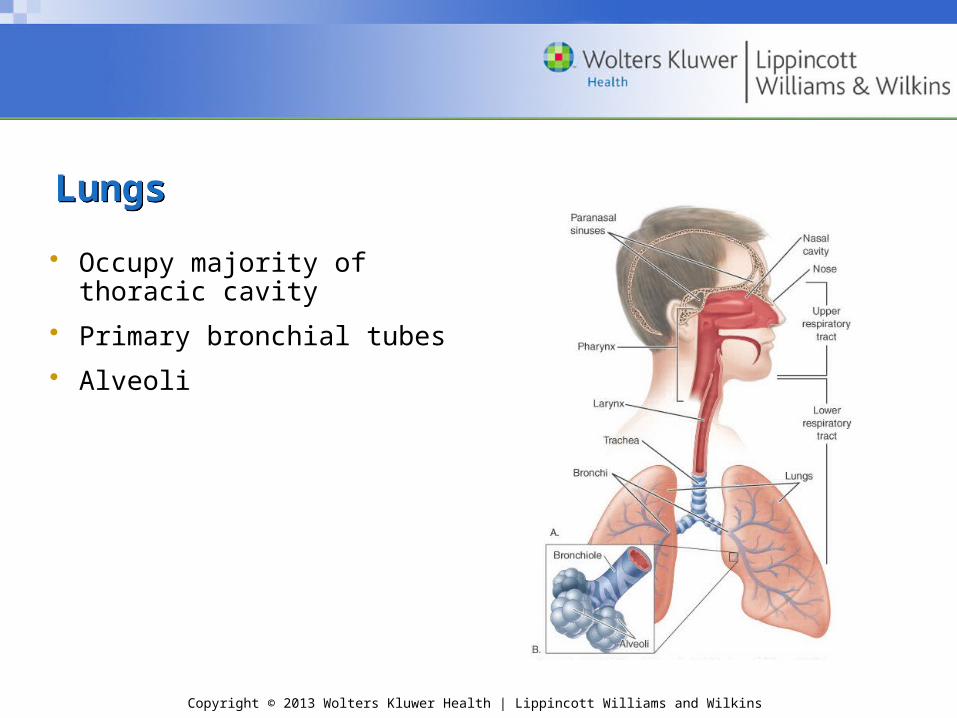
LungsLungs
• Occupy majority of thoracic cavity
• Primary bronchial tubes
• Alveoli
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams and Wilkins
Upper Respiratory Tract InfectionsUpper Respiratory Tract Infections
• Often caused by viruses
• No participation in physical activity
– Fever (≥100.5°F)
– Severe malaise
– Myalgias
– Weakness
– Shortness of breath
– Dehydrated
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams and Wilkins
Common ColdCommon Cold
• Contagious – Person–person contact– Airborne droplets
• Key—prevention!!!!
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams and Wilkins
Common Cold (cont.)Common Cold (cont.)• S&S (begin 1–2 days after exposure and last 1–2 weeks)
– Rhinorrhea– Sneezing– Nonproductive cough– Eye irritation– Malaise– Sore throat– Low-grade fever/chills
• Management– No cure—viral; OTCs can alleviate symptoms– Rest; fluids– Vitamin C; zinc gluconate
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams and Wilkins
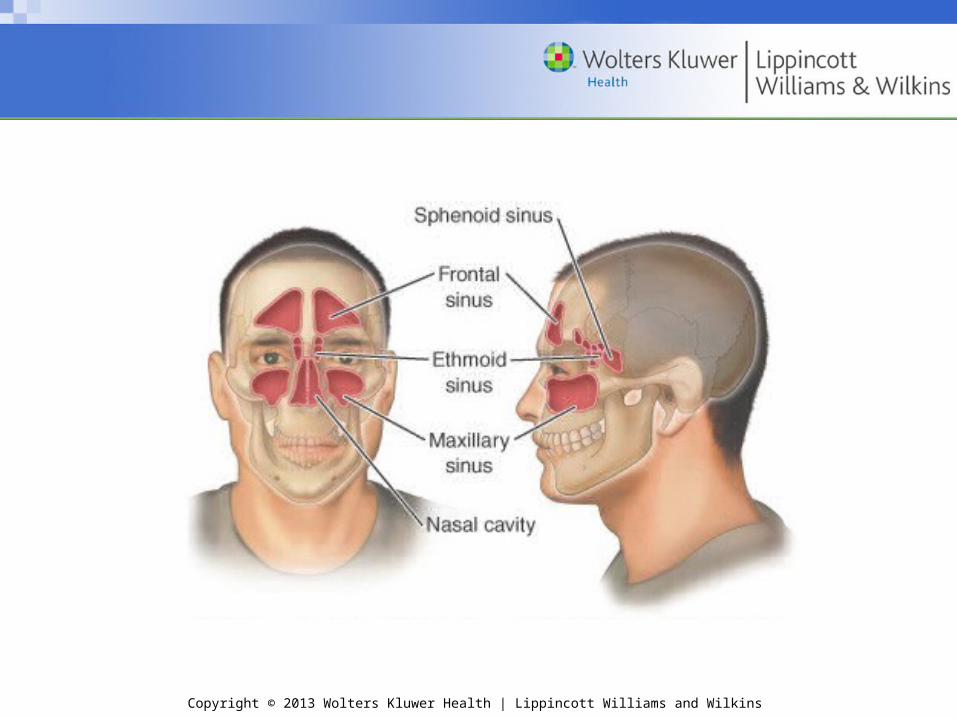
SinusitisSinusitis• Inflammation of the paranasal sinus
• Bacterial, viral, allergy, or environmental factors
• Often triggered by obstruction of passageway between the sinuses
• S&S
– Congestion
– Facial pain (behind cheeks and eyes, above teeth)
– Purulent discharge possible
– Coughing
– Swelling of eyes
– Fever and chills
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams and Wilkins
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams and Wilkins
Sinusitis (cont.)Sinusitis (cont.)
• Bacterial infection—drainage will be dark; other causes—clear
• Management
– Physician referral
– Control infection, reduce mucosal edema, and allow for nasal discharge
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams and Wilkins
PharyngitisPharyngitis• Viral, bacterial, or fungal infection of the pharynx, leading to a
“sore throat”• S&S
– Throat—dark red– Tonsils swollen and red (possible pus present)– Swallowing—painful– Ear pain (due to swallowing)– Rhinorrhea– Lymphangitis– Headache– Cough – Low-grade fever
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams and Wilkins
Pharyngitis (cont.)Pharyngitis (cont.)
• Management– Physician referral—must rule out “strep”; requires
antibiotic– Otherwise, treat symptoms—rest, fluids, warm saline
gargles, lozenges, and analgesics
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams and Wilkins
LaryngitisLaryngitis• Tissues below level of epiglottis are swollen and inflamed • S&S
– Weak, hoarse, gravely voice – Sore throat– Fever– Cough (usually dry and nonproductive)– Difficulty swallowing
• Management– Self-limiting– Decrease talking! – Treat symptoms
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams and Wilkins
TonsillitisTonsillitis• Lymph glands located at back of throat • Help protect the pharynx by filtering disease-producing
bacteria• S&S
– Inflamed and enlarged tonsils– Fever– Painful swallowing– Sore throat– Slight voice change
• Acute cases: treated with antibiotics• Chronic: surgical removal
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams and Wilkins
Allergic Rhinitis (Hay Fever)Allergic Rhinitis (Hay Fever)
• Seasonal allergic rhinitis– Involves a specific period of symptoms in
successive years – Caused by airborne pollens or fungus spores
associated with that season • Perennial allergic rhinitis
– Occurs year-round if continually exposed to allergens
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams and Wilkins
Allergic Rhinitis (Hay Fever) (cont.)Allergic Rhinitis (Hay Fever) (cont.)
• S&S– Postnasal drainage leads to chronic sore throat and
bronchial infection• Take a complete history • Management
– Limiting exposure to allergen– Suppressive medication to alleviate symptoms
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams and Wilkins
BronchitisBronchitis
• Inflammation of mucosal lining of tracheobronchial tree• Acute
– Commonly seen in physically active individuals– Involves bronchial swelling, mucus secretion, and
increased resistance to expiration– S&S
• Coughing• Wheezing• Large amounts of purulent mucus
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams and Wilkins
Bronchitis (cont.)Bronchitis (cont.)
• Chronic bronchitis – Can progress to serious illness– S&S
• Marked cyanosis• Edema• Large production of sputum• Abnormally high levels of CO2 and low levels of O2
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams and Wilkins
Bronchitis (cont.)Bronchitis (cont.)
• Management– Viral—no specific therapy available – Bacterial—treated more effectively with macrolides – Chronic—medical supervision to control symptoms
and prevent systemic failure
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams and Wilkins
Bronchial AsthmaBronchial Asthma
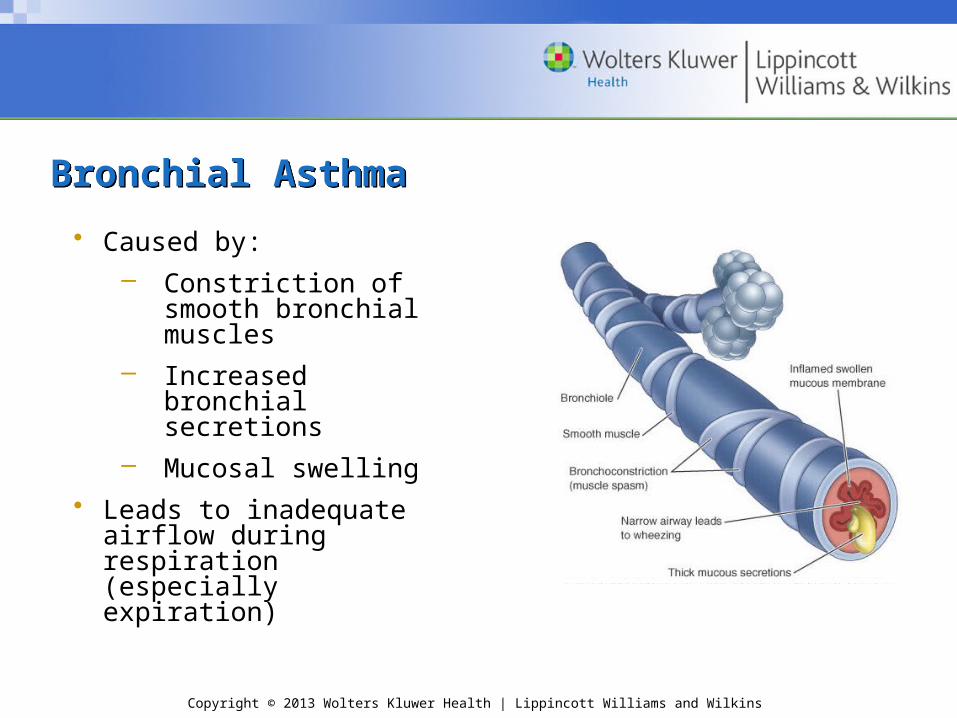
• Caused by: – Constriction of
smooth bronchial muscles
– Increased bronchial secretions
– Mucosal swelling• Leads to inadequate
airflow during respiration (especially expiration)
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams and Wilkins
Bronchial Asthma (cont.)Bronchial Asthma (cont.)• S&S
– Wheezing– Rapid fatigue– Acute attack– Thick yellow/green sputum– Anxiety– Sweating– Rapid heart rate– Cyanosis, ↓ LOC in severe cases
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams and Wilkins
Bronchial Asthma (cont.)Bronchial Asthma (cont.)
• Management– Seek medical help if no medications have been
prescribed– Administer prescribed medications
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams and Wilkins
Exercise-Induced BronchospasmExercise-Induced Bronchospasm• Various factors can contribute to severity; ↑ risk with
allergies, sinus disease, hyperventilation• Key—amount of ventilation and temperature of inspired
air– ↑ ventilations in cold, dry, air → ↑ EIB risk – ↑ strenuous exercise → ↑ ventilations
• Use of peak flowmeter– Normal: up to a 10% ↓ in FEV1 after exercise – Mild EIB: ↓ 10%–20%– Moderate to severe EIB: ↓ 20%–40%– Severe EIB: >40%
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams and Wilkins
Exercise-Induced Bronchospasm (cont.)Exercise-Induced Bronchospasm (cont.)
• S&S
– Chest pain and tightness
– Regular dry cough
– SOB after or during exercise
– Symptoms appear after 8–10 minutes of activity and may worsen after activity stops
– Refractory period
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams and Wilkins
Exercise-Induced Bronchospasm (cont.)Exercise-Induced Bronchospasm (cont.)
• Management
– Prescribed medications
– Use of inhaler
– Proper warm-up and cool-down
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams and Wilkins
InfluenzaInfluenza• Viral bronchitis caused by Haemophilus influenzae type A, B,
or C• Often epidemics—immunization available• S&S
– ↑ temperature– Chills– Malaise– Headache– General muscle aches– Hacking cough– Inflamed mucous membranes– Rapid onset within 24–48 hours of exposure
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams and Wilkins
Influenza (cont.)Influenza (cont.)
• Management– Rest and fluids– Cough medications and analgesics for pain and fever– Referral—fever does not reduce within 24 hours or
fever >103°F
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams and Wilkins
PneumoniaPneumonia• Inflammation and infection of lungs • Caused by bacteria, viruses, mycoplasmas, and other
infectious agents • S&S (can vary with type of organism causing infection)
– Bacterial pneumonia • Often follows URI • Symptoms appear suddenly• Shaking, chills, a high fever, sweating• Chest pain (pleurisy)• Cough that produces thick, rust-colored, greenish or
yellow phlegm
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams and Wilkins
Pneumonia (cont.)Pneumonia (cont.)
– Viral pneumonia• Starts with a dry (nonproductive) cough, headache,
fever, muscle, and fatigue • Progression—may become breathless and develop
cough that produces phlegm• Risk of developing a secondary bacterial pneumonia
as well• Management
– Bacterial pneumonia—antibiotics– Viral—rest and fluids; antibiotics are not effective







