
Results of ACL reconstruction for chronic knee instability, Results of ACL reconstruction for chronic knee instability, using one third of the patellar tendon augmented by extra-using one third of the patellar tendon augmented by extra-
articular plastyarticular plasty
" Mac InJones" operation" Mac InJones" operation
100 cases - follow-up > 10 years100 cases - follow-up > 10 years
JL. LERAT, F. CHOTEL, F. CLADIÈREJL. LERAT, F. CHOTEL, F. CLADIÈRE
Lyon - FranceLyon - France
ISAKOS ISAKOS JUIN 2001JUIN 2001 MONTREUX MONTREUX

Materiel and methodsMateriel and methodsMateriel and methodsMateriel and methods
Prospective study 1OO knees from 134 consecutive operations
(1 surgeon, 1 technique)
• Chronic cases• Accident to surgery interval : 4 ± 4.8 ys• Mean age : 27.8 ± 9 years• Males : 58 %• Sport’s trauma : 83 %• Previous surgery in 32 cases :
15 ACL reconstructions, Meniscal resections : 18 med, 5 lat
• Follow-up : 11.7 ± 2 ys (10 to 16)
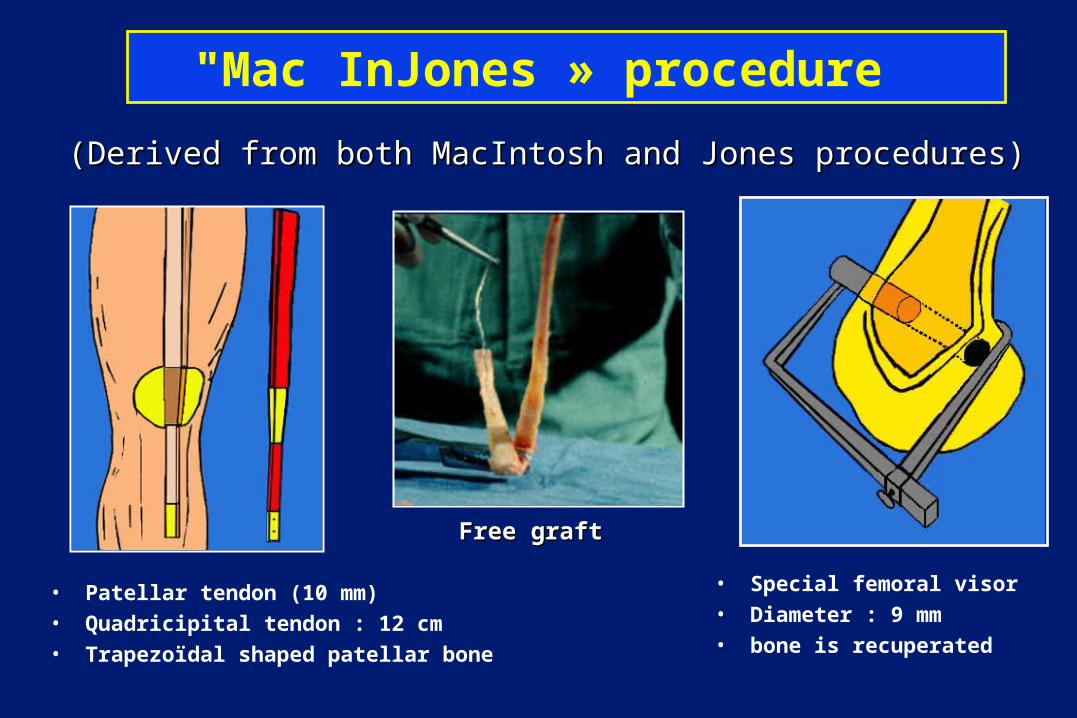
"Mac InJones » procedure
• Patellar tendon (10 mm)• Quadricipital tendon : 12 cm• Trapezoïdal shaped patellar bone
• Special femoral visor• Diameter : 9 mm • bone is recuperated
(Derived from both MacIntosh and Jones procedures)(Derived from both MacIntosh and Jones procedures)
Free graftFree graft

Introduction from outside to inside through the condyle
Stability of the trapezoïdal patellar block into the tunnel by pushing with a hammer
Fixation in the tibia with a metallic wire and a screw
Progressive tension until suppression of the drawer
Bony fragments into the tibial tunnel
Sometimes 1 additional interference screw
"Mac InJones » procedure
1rst step : ACL reconstruction

2d step : Lateral extra-articular plasty2d step : Lateral extra-articular plasty
Quadricipital tendon is stretched from the condyle to Quadricipital tendon is stretched from the condyle to the Gerdy’s tubercule with solid suturesthe Gerdy’s tubercule with solid sutures
"Mac InJones » procedure

"Mac InJones » procedure
With this procedure and the tension adjusted by torsion of
a metallic wire on a screw JL Lerat (1979)
It had become clear than the graft was sufficiently solidly
fixed at both its ends to authorize
immediate mobilisationin full flexion and extensionand agressive rehabilitation
program JL Lerat (1979)
1rst case 19791rst case 1979
Quadricipital tendon is stretched from the condyle to Quadricipital tendon is stretched from the condyle to the Gerdy’s tubercule with solid sutures the Gerdy’s tubercule with solid sutures

Fragments of bone fill Fragments of bone fill the patellar trenchthe patellar trench
Mean skin incision : 13 cm ± 3Mean skin incision : 13 cm ± 3

MaterielMaterielMaterielMateriel
100 knees evaluated
• 88 examinated and radiographied• + 12 questionnaires 17 patients lost for follow-up
+ 3 patients died

Anatomical valueAnatomical value
- KT-1000 arthrometer- KT-1000 arthrometer
- Anterior radiological - Anterior radiological drawerdrawer
FunctionFunction
- IKDC- IKDC (International Knee (International Knee Documentation Commitee)Documentation Commitee)
- A.R.P.E.GE score- A.R.P.E.GE score
MethodsMethodsMethodsMethods

MethodsMethods
KT-1000 Arthrometer(preop - post-op)
• KT 1 : 69 n• KT 2 : 89 n• KT 3 : maxi-manual
Stress radiography (preop - post-op)
• 20° of flexion• Load : 9 kg• Translation of medial and
lateral compartments

Per-operative findings
• Medial meniscus lesions : 30 %+ 25 previous meniscectomies = 55 %
• Lateral meniscus lesions : 19 %
• Cartilages lesions : 19 %– Medial : 12– Lateral : 4– Both : 3

Complications
• 7 ematomas • 2 DVT• 1 temporary peroneal nerve palsy• 2 SND• 3 skin infections • 1 infection

Results Results Results Results
• Flexion : 143° ± 11• Flexion contracture : 4.5° ± 7• Amyotrophy : 1 cm ± 0.8 (28 having none)
• Recurrence of laxity : 9 cases• Pivot-shift test ++ : 3 % + : 22 %

0
10
20
30
40
50
60
Pain effusion apprehension
Activity +++activity ++activity +sedentary
Symptoms according to activity level Symptoms according to activity level

Functional resultsFunctional results
05
101520253035404550
Excellent- A
Good - B Poor - C Bad - D
ARPEGE scoreIKDC
A.R.P.E.GE : 60 % excellent + good
IKDC score : 61 % excellent + good

0 10 20 30 40 50
sports
No sportotherVolleyTennisSkirugbyfightMountainBasketFootballRunningBasket
Competition : 58Competition : 58
Recreative : 35Recreative : 35
Sport before traumaSport before trauma

0
10
20
30
40
50
60
pivot-contact
pivot Withoutpivot
Nosport
Before trauma
preop
follow-up
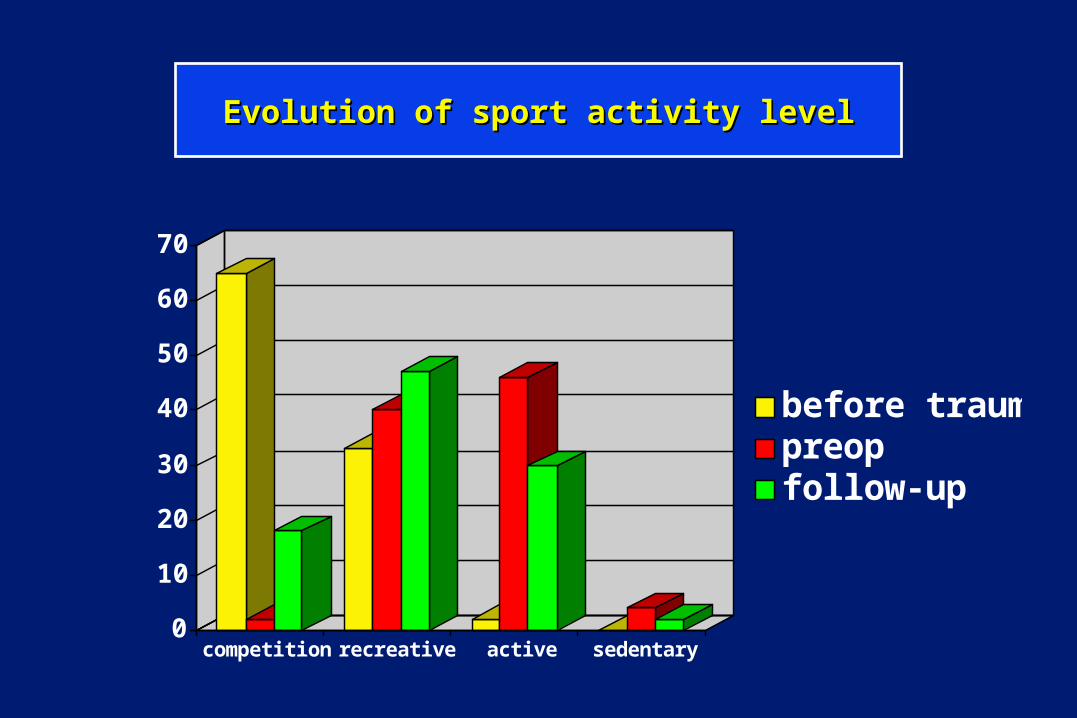
Sport activitySport activity• Satisfaction expressed by the patients : 88 %• 78 % of the patients return to sport activities• Sport with pivot : 30 % (competition : 17 %) • 14 patients stop sport for other reasons
0
10
20
30
40
50
60
70
competition recreative active sedentary
before traumapreopfollow-up
Evolution of sport activity levelEvolution of sport activity level

0
2
4
6
8
10
12
14
16
preop G.A preop G.A post-op
6 m 10 years
KT 1KT 2KT3
Arthrometric evolutionArthrometric evolution
KT-1000 Arthrometer KT 1 : 69 nKT 2 : 89 nKT 3 : maxi-manual
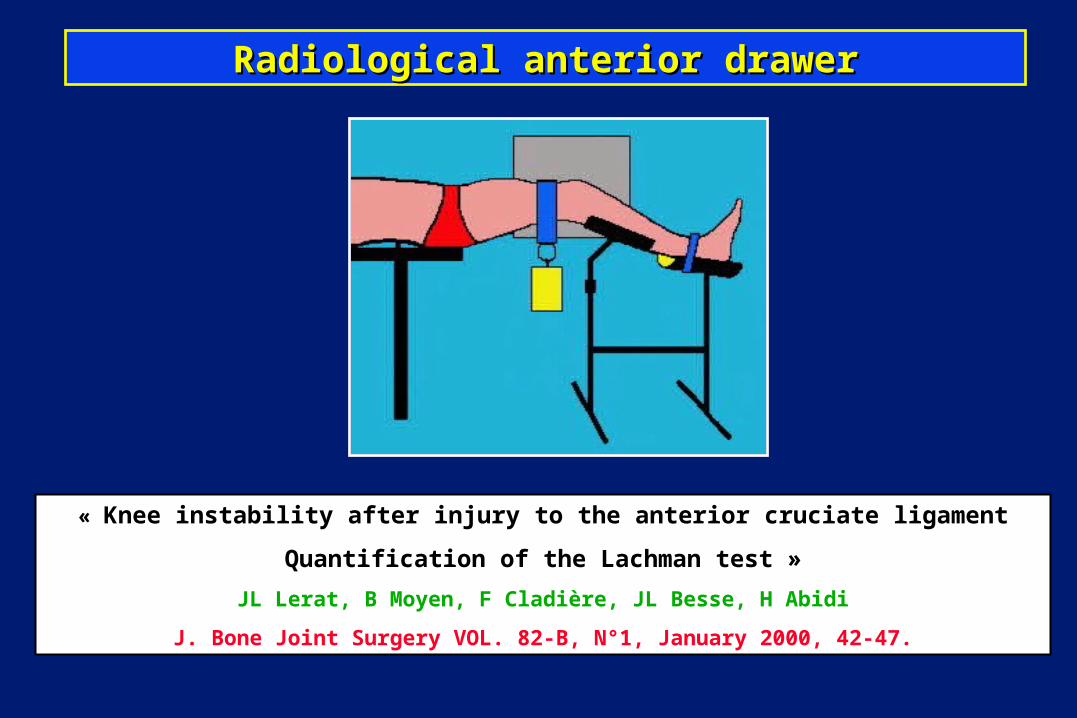
« Knee instability after injury to the anterior cruciate ligament
Quantification of the Lachman test »
JL Lerat, B Moyen, F Cladière, JL Besse, H Abidi
J. Bone Joint Surgery VOL. 82-B, N°1, January 2000, 42-47.
Radiological anterior drawerRadiological anterior drawer

Anterior radiological drawerAnterior radiological drawer
ATMC: ATMC: Anterior Translation of Medial CompartmentAnterior Translation of Medial Compartment
ATLC : ATLC : Anterior Translation of Lateral CompartmentAnterior Translation of Lateral Compartment
• Flexion : 20°Flexion : 20°• Load : 9 kg Load : 9 kg • Free rotationFree rotation• Comfortable for the Comfortable for the
patientpatient• Simple apparatusSimple apparatus

Pathological Pathological ATMCATMC and and ATLCATLC
Anterior radiological drawerAnterior radiological drawer

Differential laxity
Pathological Pathological ATMCATMC and and ATLC ATLC Normal contralateral kneeNormal contralateral knee

Precice and objective measurement of preop and post-op laxity
Pathological Pathological ATMCATMC and and ATLC ATLC Post op 10 yearsPost op 10 years

ACL deficient knees : differential ant. translationACL deficient knees : differential ant. translation
ATLC7.3 ± 4 mm
ATMC
7.8 ± 4.2 mm
0
10
20
30
40
50
60
70
80
-5 0 5 10 15 20 25
Differential ATLC
0
10
20
30
40
50
60
70
80
-5 0 5 10 15 20
Differential ATMC

Evolution of radiological laxityEvolution of radiological laxity
0
1
2
3
4
5
6
7
8
9
preop 6 m 1 year > 10 y
ATMCATLC
Gain for ATMC : 62 % Gain for ATMC : 62 % Gain for ATLC : 77 %Gain for ATLC : 77 %
Differential side to side laxityDifferential side to side laxity

AB/AC x 100AB/AC x 100 AT/AC x 100 AT/AC x 100 IT/IE x 100 IT/IE x 100
68.6 % ± 9.7 68.6 % ± 9.7 32.7 % ± 8 32.7 % ± 8 44 % ± 5.2 44 % ± 5.2
0
5
10
15
20
25
30
<50% 51-55 56-60 61-65 66-70 71-75 76-80 >80 21-25
26-30
31-35
36-40
41-45
46-48
0
5
10
15
20
25
30
35
21-25
26-30
31-35
36-40
41-45
46-48
position du tunnel tibial face
0
5
10
15
20
25
30
35
40
45
28-40 41-45 46-50 51-57

Femoral tunnel : Aglietti index Femoral tunnel : Aglietti index
0
5
10
15
20
25
30
<50% 51-55 56-60 61-65 66-70 71-75 76-80 >80
casescases
index in %index in %
AB / AC x 100 AB / AC x 100 68.6 %± 9.768.6 %± 9.7

28-40 41-45 46-50 51-570
5
10
15
20
25
30
35
40
45
28-40 41-45 46-50 51-57
casescases
index in %index in %
Tibial tunnelTibial tunnel
21-25
26-30
31-35
36-40
41-45
46-48
0
5
10
15
20
25
30
35
21-25
26-30
31-35
36-40
41-45
46-48
position du tunnel tibial face
ProfileProfile A-P A-P
3232 % ± 8 % ± 8 4444 % ± 5.2 % ± 5.2

Correlation position of the tunnels/good resultCorrelation position of the tunnels/good result
Femoral tunnelFemoral tunnelAnterior (< 52%) : IKDC : 0 A , 4 B, 9 CAnterior (< 52%) : IKDC : 0 A , 4 B, 9 C
Posterior (> 80%) : IKDC : 0 A, 6 B, 2 DPosterior (> 80%) : IKDC : 0 A, 6 B, 2 D
Tibial tunnel A-P Tibial tunnel A-P No good resultNo good result if < 30 ou > 50 % if < 30 ou > 50 %
Tibial tunnel (profile) Tibial tunnel (profile) Anterior (< 25 %) : IKDC : 4 A, 8 B, 2 CAnterior (< 25 %) : IKDC : 4 A, 8 B, 2 C
Posterior (> 40 %) : IKDC : 8 C ou DPosterior (> 40 %) : IKDC : 8 C ou D
Difficulty to see the position of the Difficulty to see the position of the ligament into the tunnels on the X-raysligament into the tunnels on the X-rays

Secondary operations
• Flexion under G.A (6 %)• 16 arthroscopies (8 meniscectomies : 5 med, 3 lat)• 3 arthrotomies (osteophytes)• Removal of 4 screws • 1 tibial osteotomy• 2 iterative ACL reconstructions

Degeneratives lesions
• 8 secondary meniscectomies during 10 years(10 times minor than during the 4 preop
years)
• Correlation : Arthrosis / meniscal lesions
• Correlation : Arthrosis / Laxity(Differential laxity : 5.7 vs 8.3 mm)


Les séquelles survenant au niveau du système extenseur, après le prélèvement d'un transplant pour intervention de
type "Mac InJones "
« The sequelae resulting from extensor muscle graft for ACL reconstruction with "Mac InJones" procedure »
JL. Lerat, JL Besse, B. Moyen, E. Brunet-Guedj
Revue de Chirurgie Orthopédique, 1995, 81, 404-410
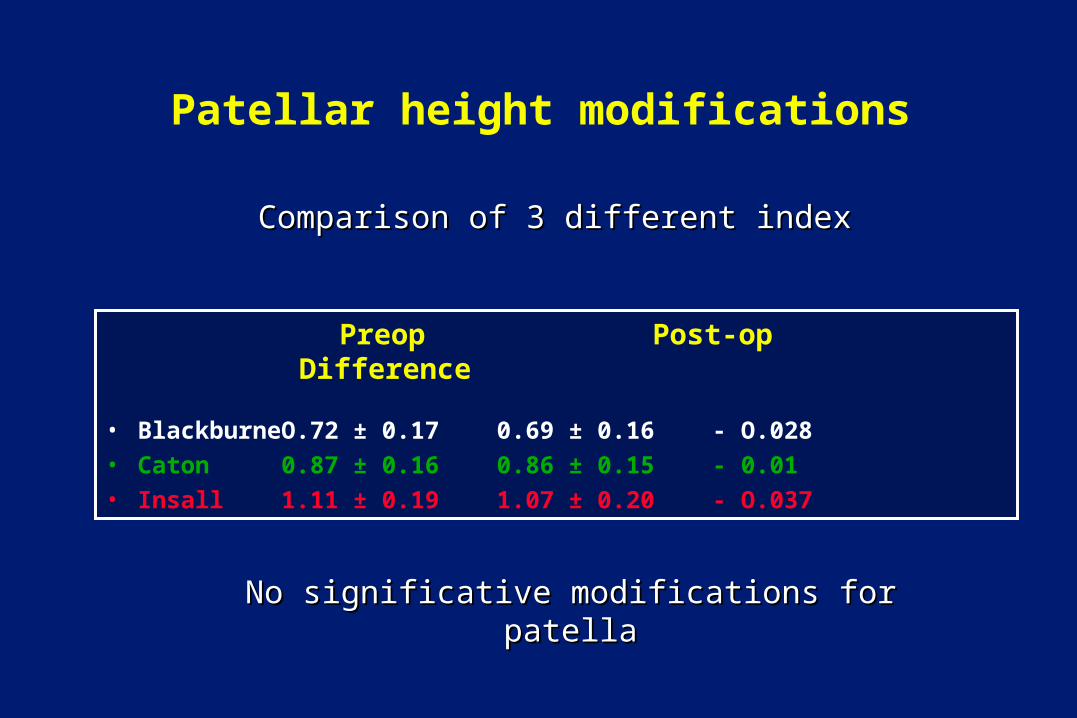
Patellar height modifications
Preop Post-op Difference
• Blackburne O.72 ± 0.17 0.69 ± 0.16 - O.028• Caton 0.87 ± 0.16 0.86 ± 0.15 - 0.01• Insall 1.11 ± 0.19 1.07 ± 0.20 - O.037
Comparison of 3 different indexComparison of 3 different index
No significative modifications for patellaNo significative modifications for patella

• Patellar tendon• Anterior knee pain• Flexion• Flexion contracture• Calcifications (29 %)
– sup pole of the patella : 12– Patellar tendon : 4 – inf pole : 6– None of these calcifications requiered repeat surgery
• Quadriceps value

INFLUENCED BY
• Varus • Residual laxity • Pivot shift• Medial meniscus lesions
(57 %) • Long time before
operation (> 4 y)
ARTHROSISARTHROSISARTHROSISARTHROSIS

Evolution of arthrosisEvolution of arthrosis
JOINTSPACE
F-Tmedial
F-Tlateral
F-P F-Tmedial
F-Tlateral
F-P
Normal 76 97 93.5 30.5 78 66.3Remodeled 15.5 0.7 6.5 44.5 13.5 20.5
Stage I 7 1.5 0 11.5 5.3 9.6Stage II 1.5 0.7 0 13.5 3.1 3.6
pre-op pre-op post-op post-op
%%

Study of the failed cases :Study of the failed cases :Ruptures or elongations of ACL (7 %)
5 ruptures during sport activity2 with poor femoral tunnel positionning
During the same time :During the same time :8 ruptures occured at the opposite ACL (4 years after surgery to the other knee)

Literature with long follow-up
• Johnson & Eriksson (1984) 8 years• Aglietti (1992)• Demsey & Tregonning (1993) 9 years• Dejour & Ait si selmi (1995)
(comparisons are not easy : criteria #, follow-up #)
There are few well documented series after 10 years

Role of the extra-articular reconstruction
Not easy to analyse independently of the ACL
• Nothing to be gained from the adding of lateral plasty– Roth (1987)– Strum (1989)– O Brien (1991)
• Reduction of the pivot shift– Jensen Slocum Larson (1983)– Noyes Barber-Westin (1991)– Lerat (1997)
« Influence of a lateral extra-articular plasty on the results of ACL reconstruction with the patellar tendon. Follow-up 4 years »
JL. Lerat, A. Mandrino, JL. Besse, B. Moyen, E. Brunet-Guedj.
Revue de Chirurgie Orthopédique, 1997, 83, 591-601

ConclusionsConclusionsConclusionsConclusions
• Good results if we compare to the literature
• Confirmation of the good quality of patellar tendon as an ACL substitute.

ConclusionsConclusionsConclusionsConclusions
Quadruple interest of this prospective study :
• Original reconstruction of ACL + Lateral extra-articular reconstruction with a single transplant using the quadriceps tendon and thus preserving the ilio-tibial band and the control of varus stability
• Confirmation of the efficiency of a lateral reconstruction in chronic cases
• Interest of Radiological measurement of the drawer (1979)
• Interest of a early agressive rehabilitation program (1979)

Thank youThank you

pre-op laxitypre-op laxity
Pre-opLAXITY
varusextension
varusflexion
valgusextension
valgusflexion
none 129 116 121 95slight 6 16 14 28
++ 2 2 2 11severe 0 1 0 1









