Download - Rohan R. Walvekar

1
UCSF Salivary Endoscopy Course 2014
Basic Set Up and Instruments
Rohan R. Walvekar, MD
Department of Otolaryngology & Head Neck Surgery
Louisiana State University Health Sciences Center
New Orleans, LA
DisclosureI have the following relationship(s) with commercial interests.
Hood Laboratories *Walvekar Salivary Stent
Cook Industries
Medtronic Xome
A commercial interest is any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients.
� Instruments for Exposure of the Oral Cavity� Anesthesia – Nasal Intubation is preferred
� Epistaxis• Pre-op nasal endoscopy to document spurs,
deviated septum or other abnormality• Afrin and lubricated nasal trumpet while
patient is in preoperative holding area � Disposable Plastic cheek retractor� Dental splints � Jennings's mouth gag � Minnesota and Sweetheart
retractors
Basic Sialendoscopy Set
� Dilator System � Marchal Dilator System
� Probes No.0000 to No.8� Schaitkin’s Fluted Dilators \
� No.0 – 5� Conical Dilator � Helps to transition between dilators� Useful usually once papilla is dilated up to Marchal
No.1 or 2 dilator� Bougies (increasing diameter)
� Compatible with 0.4 mm guide wire� COOK Dilator System with Operating Sheath
� Guide Wire � Cook Dilators 1-8
Basic Sialendoscopy Set

2
Schaitkin Salivary Dilator Set
3
Sialendoscopy
Kolenda Introducer Set (COOK)
Sialendoscopy
Sialendoscopy
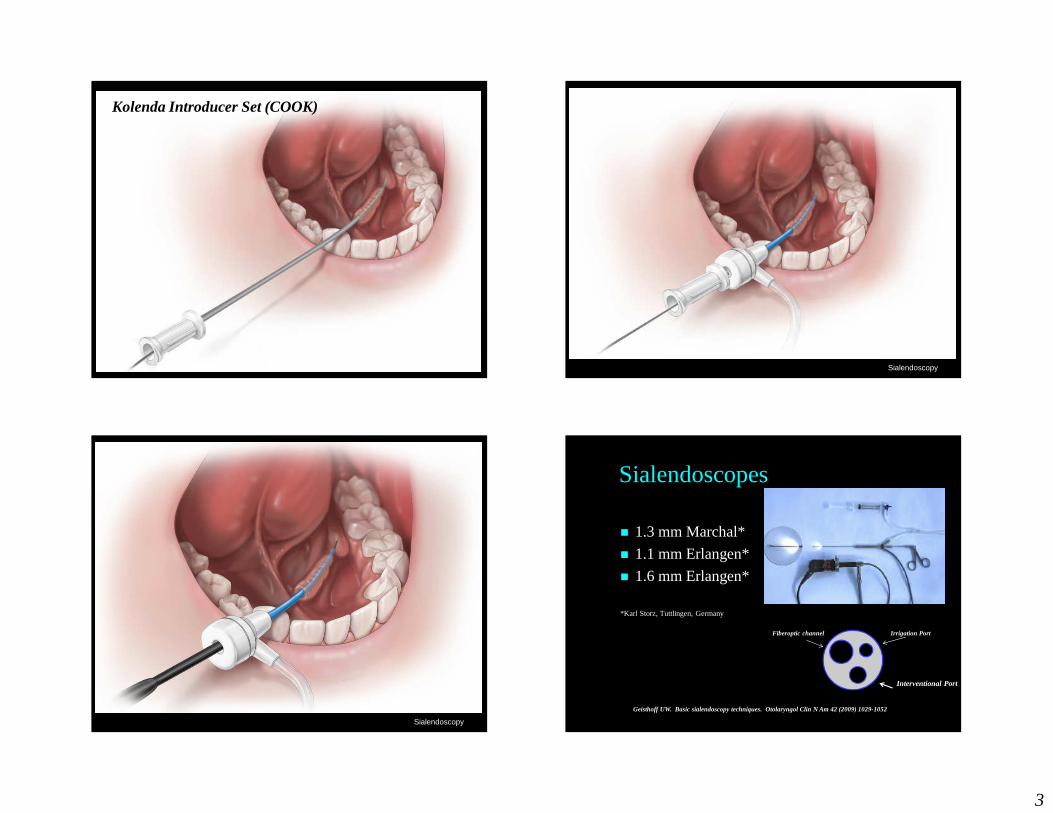
Sialendoscopes
Geisthoff UW. Basic sialendoscopy techniques. Otolaryngol Clin N Am 42 (2009) 1029-1052
� 1.3 mm Marchal*
� 1.1 mm Erlangen*
� 1.6 mm Erlangen*
*Karl Storz, Tuttlingen, Germany
Fiberoptic channel Irrigation Port
Interventional Port

4
� Fifth generation endoscopes
� Original was flexible
� 1.3 mm semi rigid scope with 6000 pixels, 0.25mm rinsing channel and 0.65mm working channel
Marchal Sialendoscope� Sialendoscopes� 0.8 mm
� Pediatric diagnostic sialendoscopy� No interventional channel
� 1.1 mm “all in one” Erlangen Sialendoscope� Can be autoclaved� Interventional Tools that can be used with the scope
� 0.4 mm guide wire basket� 0.4 mm stone basket � Laser fiber (Holmium laser)� Hand held microburr
� Does not have a protective sheath� Dilate up to No.3 or 4 prior to endoscopy
Basic Sialendoscopy Set
� Sialendoscopes� 1.3 mm Marchal “all in one” scope
� Autoclavable. � Interventional Tools that similar to 1.1 Erlangen
scope� Does have a protective sheath� Optics are excellent� Dilate up to No.4 / 5 prior to endoscopy� Gentle bend at the tip of the scope
Basic Sialendoscopy Set
� 1.6 mm “all in one” Erlangen Sialendoscope� Can be autoclaved� Interventional Tools that can be used with the scope
� 0.4/6 mm guide wire basket� 0.4/6 mm stone basket � Cup forceps**
� Does not have a protective sheath� Dilate up to No.5 or 6 prior to endoscopy
� Balloon Dilator (Storz) – compatible with all in one scopes
Basic Sialendoscopy Set

5
Sialendoscopy
� IV Extension Tubing� 20 cc syringe � Vessel loops� Angled Forces with and without teeth� Standard Endoscopy Tower and Monitor with recording
capabilities**Accessories� Disposables
� Stone baskets� Guide wires� Cleaning brushes� Stents (Hood Laboratories)*� Balloon Dilator
� Not Disposable� Hand-held micro burr� Stone forceps
Basic Sialendoscopy Set
Three way stopcock/valve
STORZ WIRE BASKETS COOK WIRE BASKETS - - N Gage

6
LSU Sialendoscopy Course
Diagnostic Sialendoscopy
Rohan R. Walvekar, MD
Department of Otolaryngology & Head Neck Surgery
Louisiana State University Health Sciences Center
New Orleans, LA
� 100% Successful endoscopy
� Ductal or papillary stenosis in 7/15 (47%)
� Essentially normal endoscopy in 8/15 (53%)
� Symptoms improved in 13/15 (87%) cases
Diagnostic Sialendoscopy Data
Bowen M et al. Diagnostic and Interventional Sialendoscopy: A preliminary experience. 2010 Laryngoscope (accepted for publication)
� Progressive dilation� Marchal Dilator System
(No.0000 to No.6)
� Conical dilator
� Seldinger technique� Guide wire and bougies
� Papillotomy� 25% (7/28)
� Successful endoscopy� 96% (27/28)
Sialendoscope CannulationSERIAL DILATION USING THE DILATOR SYSTEM
SELDINGER TECHNIQUE USING GUIDE WIRE AND BOUGIES (adopted from Chossegros et al2)
Success of Diagnostic Endoscopy ~ 95-98%
Rate Limiting Step : Dilation of Papilla
� Approaches to the papilla
� Dilation technique
� Seldinger technique
� With bougies
� With sialendoscope
� Papillotomy
� Proximal papillotomy and sialodochoplasty
7
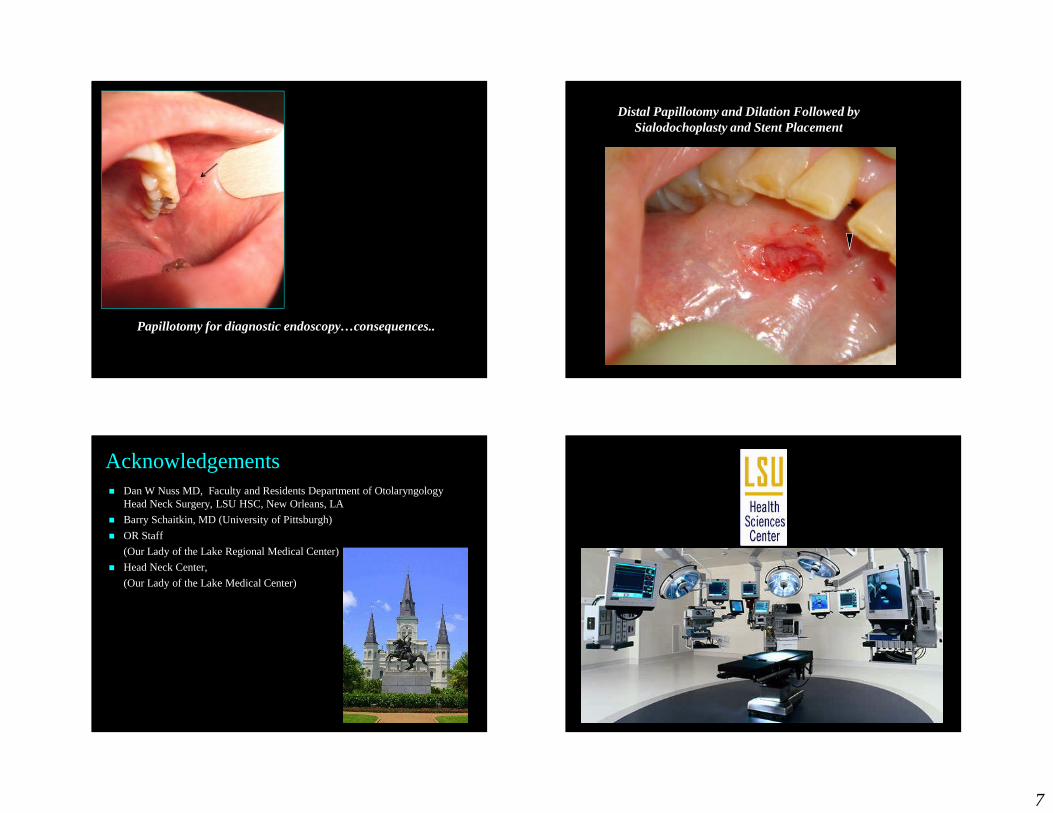
Papillotomy for diagnostic endoscopy…consequences..
Distal Papillotomy and Dilation Followed by Sialodochoplasty and Stent Placement
Acknowledgements� Dan W Nuss MD, Faculty and Residents Department of Otolaryngology
Head Neck Surgery, LSU HSC, New Orleans, LA
� Barry Schaitkin, MD (University of Pittsburgh)
� OR Staff
(Our Lady of the Lake Regional Medical Center)
� Head Neck Center,
(Our Lady of the Lake Medical Center)
8
Avoid Complications
�Local Anesthesia:�-Lidocaine 4.5mg/kg (<300mg)�-Lidocaine/epineprine 7mg/kg (<500 mg)
�MAC (sedation):�-Over�-Under
�Local Anesthesia:�-Beware of ETT position�-NO atropine or like medication
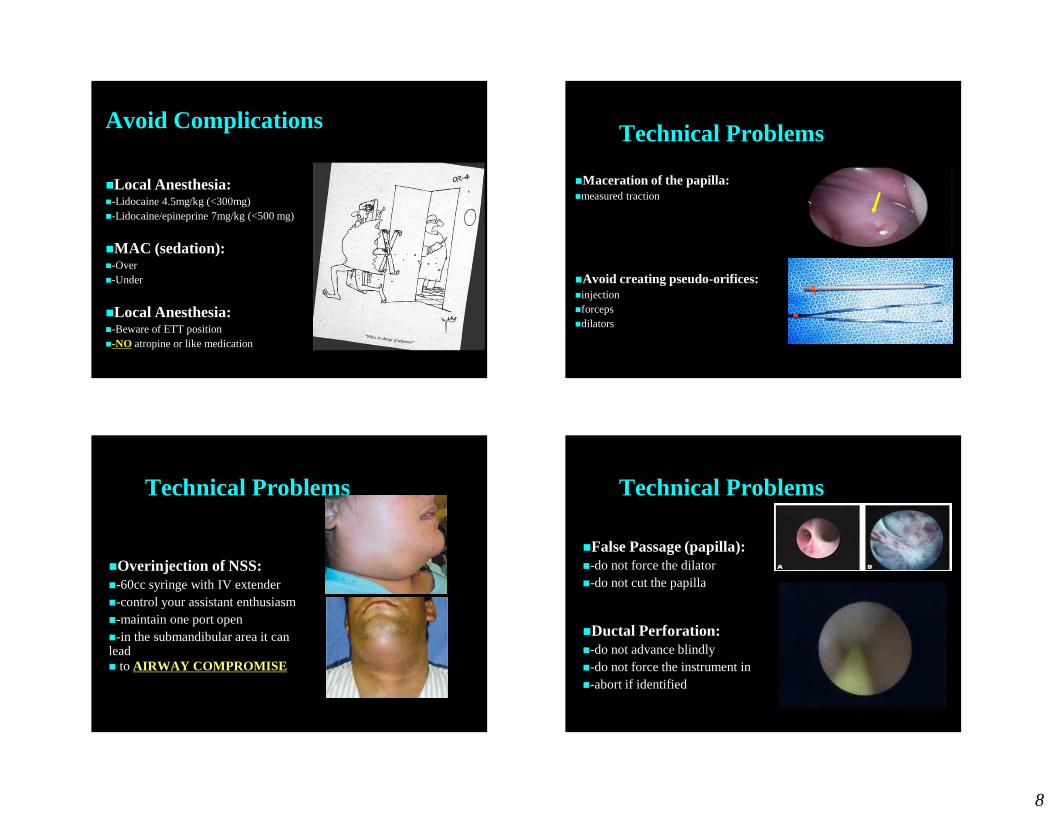
Technical Problems
�Maceration of the papilla:�measured traction
�Avoid creating pseudo-orifices:�injection�forceps�dilators
Technical Problems
�Overinjection of NSS:�-60cc syringe with IV extender�-control your assistant enthusiasm�-maintain one port open�-in the submandibular area it can lead � to AIRWAY COMPROMISE
Technical Problems
�False Passage (papilla):�-do not force the dilator�-do not cut the papilla
�Ductal Perforation:�-do not advance blindly�-do not force the instrument in�-abort if identified

9
Equipment Failure
�Be cognizant of the turns:�-scope is semi-rigid (it is fragile) �-straighten the duct using manual traction
and pressure
�Be cognizant of the teeth
�Have back up gear
The Learning Curve







