
Severe hypodontia – interdisciplinary planning,
outcome and psychosocial impact
Christina Louise Hvaring
Doctoral thesis for the degree of Philosophiae Doctor (Ph.D.)
Department of Orthodontics
Institute of Clinical Dentistry
Faculty of Dentistry
University of Oslo
Norway
2016
© Christina Louise Hvaring, 2017 Series of dissertations submitted to the Faculty of Dentistry, University of Oslo ISBN 978-82-8327-023-5 All rights reserved. No part of this publication may be reproduced or transmitted, in any form or by any means, without permission. Cover: Hanne Baadsgaard Utigard. Print production: Reprosentralen, University of Oslo.

Table of contents
Acknowledgements 1
List of papers 3
Abbreviations 4
Summary 5
Introduction 7 Hypodontia 7 Persisting primary teeth without successor 13 Oral health-related quality of life 14 Oral Index on Daily Performance 15 Other health-related quality of life instruments in children and adolescents 17 Therapeutic approaches in cases with severe hypodontia 19 Treatment course in hypodontia patients 19 Treatment options and methods for replacing missing teeth in growing individuals 20 Treatment outcome in patients with severe hypodontia 25
Aims of this work 28 Overall aim 28 Specific aims 28
Materials 29 Study groups 29 Data collection 30
Methodological considerations 30 Measurements on panoramic radiographs (paper I) 30 OIDP questionnaire (paper II) 30 Follow-up with clinical examination (paper III) 31 Statistical methods (Papers I-III) 32
Summary of results 33
Discussion 38 Study group and inclusion criteria 38 Evaluation of results 38 Clinical implications 50
Conclusions 51
References 53
1
Acknowledgements
This project was financed by the Faculty of Dentistry at the University of Oslo. The research
is based on a unique collection on clinical data from patients with hypodontia gathered since
the inception of “Eksperttjenesten” in 1998 at the Department of Orthodontics, Faculty of
dentistry, University of Oslo. This systematic collection of quality records to which I was
given free access, formed the basis for my research.
I am deeply grateful to my principal supervisor Associate Professor Kari Birkeland for her
scientific guidance, for sharing her great insight in orthodontics, and for her always-positive
enthusiasm and commitment to this project. Her dedication and effort in always seeking the
best possible solution for patients with very complex dental issues has truly inspired me. I
also wish to express my sincere gratitude to my co-supervisor Professor Bjørn Øgaard who
has kindly shared his extensive knowledge and experience in orthodontics. His accurate and
constructive guidance, as well as his friendly and encouraging nature, have been invaluable in
this process.
I would also like to thank Professor Anne N. Åstrøm at the Faculty of Dentistry, University of
Bergen for her excellent guidance and scientific competence in the field of community
dentistry, and Professor Arild Stenvik who has provided inspiration and great ideas for the
project. Profound thanks to Professor Leiv Sandvik for his statistical support, and the way he
always makes the statistical sessions memorable and interesting.
My appreciation extends to the staff at the Department of Orthodontics, always kind and
helpful. I have spent three years with my seven fellow specialist candidates, and would like to
thank them for exciting and eventful years in a close-knit group of unique and humorous
individuals.
My faithful and patient friends have always been a big support, reminding me of what is
important in life. The quality time we spend hanging out together forms my absolute favourite
moments. My family and in-laws’ support, inspiration and care throughout this journey have
been priceless. Thank you for your kind encouragement and always believing in me. Special
thanks go to my mother and mother-in-law for taking care of my son Albert during long
working sessions. Another special thank you goes to my father for interesting and challenging
discussions in the field of orthodontics.
2
Finally, and most of all, I would like to thank my husband Tore for his eternal and patient
support and care. He has spent hours proofreading my work and helping me with technical
statistical computerish problems. My greatest love goes to him and our beautiful son Albert.
Oslo, November 2016
Christina L. Hvaring

3
List of papers
This thesis is based on original research carried out at the Department of Orthodontics,
Faculty of Dentistry, University of Oslo. The thesis includes three papers listed below, which
will be referred to by their Roman numerals in the text.
Paper I
Hvaring CL, Ogaard B, Stenvik A, Birkeland K. The prognosis of retained primary molars
without successors: infraocclusion, root resorption and restorations in 111 patients. Eur J
Orthod. 2014;36:26-30.
Paper II
Hvaring CL, Birkeland K, Astrom AN. Discriminative ability of the generic and condition
specific Oral Impact on Daily Performance (OIDP) among adolescents with and without
hypodontia. BMC Oral Health. 2014;14:57.
Paper III
Hvaring CL, Ogaard B, Birkeland K. Tooth replacements in young adults with severe
hypodontia: Orthodontic space closure, dental implants, and tooth-supported fixed dental
prostheses. A follow-up study. Am J Orthod Dentofacial Orthop. 2016;150:620-6.

4
Abbreviations COHIP Child Oral Health Impact Profile
CPQ Child Perceptions Questionnaire
CS OIDP Condition specific Oral Index on Daily Performances
CS Condition specific
DHC Dental health component
ED Ectodermal dysplasia
FDP Fixed dental prosthesis
ICC Intraclass correlation coefficient
ICIDH International Classification of Impairments, Disabilities and Handicap
IOTN Index of Orthodontic Treatment Need
MIQ Malocclusion Impact Questionnaire
miRNA Micro-RNA
OHIP Oral Health Impact Profile
OHRQoL Oral health-related quality of life
OIDP Oral Index on Daily Performances
OQLQ Orthognathic Quality of Life Questionnaire
RPD Removable partial denture
SPSS Statistical Package for the Social Sciences
UK United Kingdom of Great Britain and Northern Ireland
USA United States of America
WHO World Health Organization

5
Summary The general purpose of this thesis was to increase the knowledge and understanding of
treatment outcome and psychosocial status in patients with severe hypodontia.
Paper I is a retrospective study aiming at pointing out the limiting prognostic factor for the
persistence of primary mandibular molars whose successors are lacking. Primary mandibular
molars and their degree of infraocclusion, root resorption and restorations were assessed on
panoramic radiographs in 111 subjects missing at least one second mandibular premolar. The
patients had a mean age of 12.6 years and missed 8.4 teeth on average. All persisting primary
mandibular molars were included in the study, as no decision had been made as to whether
they should be kept or extracted. Clinically significant infraocclusion was observed in 43.6
per cent of the patients and classified as severe in 18.8 per cent. The mesial and distal root
exhibited no resorption in 18.9 and 33.3 per cent, respectively (P = 0.01). Most primary
molars had no restorations (78.4 per cent). A significant correlation was found between root
resorption and infraocclusion. Infraocclusion was estimated to be a more critical factor for the
prognosis of retained primary molars than root resorption.
Paper II is a cross-sectional survey assessing the discriminative ability of the generic and
condition specific (CS) forms of the oral impact on daily performance (OIDP) inventory
among adolescents with hypodontia and with a malocclusion of similar treatment need. The
groups consisted of 62 patients with non-syndromic hypodontia and 101 patients with a
malocclusion. The mean number of missing teeth in the hypodontia group was 6.2. Both
groups reported a considerable burden of oral impacts. The prevalence of generic and CS oral
impacts in the hypodontia group were 64% and 30%, respectively, and the corresponding
rates in the non-hypodontia group were 62% and 10%. The CS OIDP measure discriminated
most effectively between patients with and without hypodontia and was related to severity
and upper anterior location of hypodontia.
Paper III is a longitudinal follow-up study of 50 patients with severe hypodontia aged 18
years or more (mean age, 25.6 years). The purpose of the study was to describe types and
locations of substitutes for missing teeth in patients with severe hypodontia, and to compare
the crown and soft tissue morphologies of orthodontic space closure, dental implants, and
tooth-supported fixed dental prostheses replacing teeth in the anterior region. The patients
were examined clinically, with panoramic radiographs and clinical photographs being taken.
Dental implants, orthodontic space closure, and retaining deciduous teeth were the most
commonly prescribed treatments. Persisting deciduous teeth showed a good survival rate at
the follow-up examination. Dental implants in the anterior region proved to be an inadequate
6
treatment modality in patients with severe hypodontia because of mucosal discoloration seen
for almost all fixtures in the anterior mandible and two thirds of those in the anterior maxilla.

7
Introduction
Hypodontia
Definitions
Hypodontia is a congenital condition of having fewer teeth than the normal number of teeth.
The word originates from Greek where hypo means under and odous means tooth. The
condition is the most common dental anomaly in man (2, 3), and the term hypodontia is used
to describe congenitally missing teeth in general. Various synonyms have been used in the
literature to describe the phenomenon: oligodontia, anodontia, aplasia of teeth, agenesis of
teeth, congenitally missing teeth and lack of teeth. Agenesis of teeth is perhaps the most
precise definition, referring to the failure of an organ to develop during embryonic growth.
Schalk-van der Weide et al. (4) defined oligodontia as a condition in which six or more teeth,
excluding third molars, are congenitally missing. The author defined two forms of
oligodontia: oligodontia/I (isolated) and oligodontia/S (syndrome), as the condition can occur
alone or as part of a syndrome (4). Severe hypodontia was considered by Hobkirk et al. (5) to
be the same as oligodontia, and the definition is commonly used in the dental literature.
Anodontia is a rare developmental dental anomaly characterized by absence of all teeth.
These definitions of hypodontia, oligodontia/severe hypodontia and anodontia will be used in
this thesis.
Prevalence
The reported prevalence of hypodontia varies depending on population and gender. Because
of its high frequency and limited functional importance, lack of third molars is usually
excluded from the definition of hypodontia, as is the case in the present thesis. Absence of at
least one third molar has been reported in as much as 20-30% of the European population (6,
7). A meta-analysis by Polder et al. (8) in 2004 reviewed 31 studies of the prevalence of
hypodontia published from 1936 to 2001. The same year, Mattheeuws et al. (9) performed a
meta-analysis including 19 articles from 1936 to 1993 concerning a possible increase in
hypodontia during the 20th century. The authors concluded that the considered period of time
was too short and the available data too limited to describe a trend in the human dentition.
However, hypodontia seems to have been diagnosed more often in recent studies. In 2014,
Khalaf et al. (1) published an updated meta-analysis extending the two already mentioned
with additional data from articles published after 2002. The authors included 93 studies, of
which 39 studies were taken from the previous two systematic reviews. The overall

8
prevalence of hypodontia was found to be 6.4% (95% CI: 5.7-7.2). Table 1 shows the
prevalence of hypodontia in schoolchildren. Fifteen of these 27 studies were from the Nordic
countries. The variation in reported prevalence may be due to differences in methods of
sampling, age distribution, gender and racial origin. The assessment of congenitally missing
teeth in younger individuals might also be inaccurate due to the occasionally insufficient
mineralisation of the mandibular second premolar (10). A study by Wisth et al. (10) found
that the prevalence of hypodontia was higher when the same patient sample was examined at
the age of 7 years, as compared to when it was examined at 9 years of age. The meta-analysis
by Khalaf et al. (1) revealed a statistically significant difference in prevalence by continent,
with the highest prevalence in Africa (13.4%) followed by Europe (7%), Asia (6.3%),
Australia (6.3%), North America (5%) and Latin America and the Caribbean (4.4%).
Furthermore, the prevalence among females was 1.22 times that among males.
In general, hypodontia is mild (1 or 2 teeth missing) in most subjects (82%) (1), whereas
oligodontia is much more rare. A Norwegian study examined 9532 subjects in two counties
aged 18 years, and found 0.084% with oligodontia (11). Furthermore, two studies from
Denmark and Netherlands reported a prevalence of oligodontia of 0.16% and 0.08%
respectively (12, 13).

9
Table 1. Prevalence of hypodontia in schoolchildren from various countries according to
Khalaf et al. (1)
Author Year Country Age Sample size
Prevalence (%)
Dolder 1936 Switzerland 6-15 10000 3.4 Grahnen 1956 Sweden 11-14 1006 6.1 Gimnes 1963 Norway 6-15 36000 4.5 Volk 1963 Austria 9-15 9533 9.6 Blayney_1 1967 USA 12-14 11713 3.8 Blayney_2 1967 USA 12-14 1320 4.1 Davies 1968 Australia 12-14 2170 6.3 Helm 1968 Denmark 6-18 1700 6.1 Egemark-Erikson 1971 Sweden 10-16 3327 6.3 Haaviko 1971 Finland 5-13 1041 8.0 Hunstadbraten 1973 Norway 7-14 1295 10.1 Thilander 1973 Sweden 7-13 5459 6.1 Bachmann 1974 Switzerland 9-10 8694 7.7 Brook 1974 UK 11-14 1115 4.4 Thompson 1974 Canada 6-12 1191 7.4 Wisth 1974 Norway 9 813 6.8 Bergstrom 1977 Sweden 8-9 2589 7.4 Magnusson 1977 Iceland 8-16 1116 7.9 Rolling 1980 Denmark 9-10 3325 7.8 Davis 1987 Hong Kong 12 1093 6.9 Al Emran 1990 Saudi Arabia 13-14 500 4.0 Aasheim 1993 Norway 7-10 1953 6.5 Johannsdottir 1997 Iceland 6-7 396 4.3 Backmann 2001 Sweden 7 739 7.4 Abu Alhaija 2005 Jordan 13-15 1003 6.0 Maatouk 2008 Tunisia 12-18 262 13.4 Rolling 2009 Denmark 9-12 8138 7.4

10
Characteristics
The distribution of congenitally missing teeth by tooth type is shown in Figure 1. The most
commonly missing tooth, in most studies, is the mandibular second premolar, followed by the
maxillary lateral incisor and the maxillary second premolar (1). However, this distribution
varies between populations. In a Norwegian study, 50% of the missing teeth were mandibular
premolars, 20% maxillary second premolars, 16% maxillary lateral incisors and 4%
mandibular central incisors (14). In a study of Chinese schoolchildren, the most commonly
affected teeth were the mandibular incisors, followed by the upper second premolars and the
upper lateral incisors (15). Absence of maxillary central incisors, maxillary and mandibular
first molars, and mandibular canines seems to be very rare. No clear difference in
congenitally missing teeth has been found between the maxilla and mandible and between the
right and the left side (16). Unilateral hypodontia is most common, with the exception of
maxillary lateral incisors, where bilateral lack of teeth is most often seen (8).
Associated skeletal effects
The craniofacial structure and growth pattern of patients with hypodontia have been assessed
in a number of cephalometric studies. Some studies have reported a Class I skeletal
Figure 1. Distribution of missing teeth by tooth type in % of all missing teeth according to Khalaf et al. (1)

11
relationship and a normal growth pattern (17-19), while others have reported a smaller and
more retrognathic maxilla with a tendency towards a Class III skeletal pattern (20-23). The
hypodontia patients also have a tendency towards a reduced anterior lower face height and a
decrease in the mandibular plane angle (22, 24). These tendencies become more evident as
the severity of the hypodontia increases (23, 24). A study by Ogaard et al. (24) compared the
craniofacial morphology of hypodontia patients with a varying number of missing teeth.
When more than 10 teeth were missing, the maxillary protrusion was significantly reduced
and the mandible rotated anteriorly, probably as a consequence of less posterior support.
Associated dental anomalies
Hypodontia is frequently accompanied by reduction in tooth size (microdontia), short root
anomaly, malformation of other teeth, impaction, maxillary canine and first premolar
transposition, delayed formation or eruption of teeth, taurodontism, enamel hypoplasia and
altered craniofacial growth (7). A phenotype of congenital absence of a maxillary lateral
incisor on one side and a peg-shaped lateral incisor on the other side is common; these two
anomalies are considered different manifestations of the same genotype (7).
Etiology
Several theories on the etiology of hypodontia have been proposed in the literature (2). Brook
(25), (26) suggested a unifying aetiological explanation for anomalies of tooth number and
size, and argued that hypodontia is caused by a number of complex interactions between
genetic, epigenetic and environmental factors during the process of dental development. Kjaer
(27) refers to embryological investigations showing the existence of neural development
fields in the jaws and dentition, namely the incisor field, the canine/premolar field and the
molar field. The hypothesis is that agenesis of teeth might be the result of deviations in nerve
tissue proliferation in a field during embryogenesis, resulting in lack of formation of hard
tissue, such as teeth. The region within a single field where innervation occurs last is more
likely to manifest tooth agenesis.
Environmental factors
Hypodontia may be associated with environmental factors such as infections, trauma in the
dental region, surgical procedures on the jaws or extraction of the preceding primary tooth
(7). Somatic diseases such as syphilis, scarlet fever, rickets, or nutritional disturbances during
pregnancy or infancy may also affect tooth development (2). Developing teeth are irreversibly

12
affected by multi-agent chemotherapy and radiation therapy, with the latter having the
strongest adverse impact (28).
Genetics
The genetic basis is the most important factor in the etiology of hypodontia, and the
occurrence of hypodontia among individuals related to hypodontia patients is higher than in
the general population (2, 7, 16, 29). Non-syndromic hypodontia is more common than the
syndromic variant, and the condition can follow autosomal dominant, autosomal recessive or
X-linked patterns of inheritance, with variations in penetrance and expressivity (30). Since the
condition segregates in families, strategies for gene identification can be performed.
The genes PAX9, MSX1, AXIN2, EDA, EDAR, EDARADD, and WNT10A have been described
as being involved in tooth development (2, 16, 30), and mutations of these may disrupt the
epithelial-mesenchymal interactions necessary for tooth formation. In 2009, Shimizu et al.
(30) published a review of genetic studies addressing hypodontia in humans and mouse
models. The authors concluded that although recent genetic studies provide information
regarding genes related to hypodontia, the causes of the most common form of hypodontia are
still unknown. It is therefore likely that other hypodontia-related genes still exist and will be
identified in the future (30). A high discordance rate of hypodontia sub-phenotypes has been
established in a study of monozygotic twins; epigenetic influences on spatiotemporal gene
regulation might be involved (31). Regulation of gene expression by miRNAs may also affect
tooth development (32). Recently, a robust investigation mapping out tooth agenesis patterns
and phenotype variation in a Belgian cohort of 67 families with oligodontia and 12 families
with hypodontia was published (33). The authors found an extreme variation in the
expressivity of the hypodontia/oligodontia between affected family members, and concluded
that tooth agenesis is not a simple monogenic condition, but that a complex interaction of
genetic and environmental factors comes into play.
Syndromic hypodontia Congenitally missing teeth can occur as an isolated feature or as part of a syndrome. The
London dysmorphology database reports 150 syndromes as being associated with hypodontia
(34), indicating that the development of teeth and certain organs are under the control of the
same molecular mechanisms. Commonly associated syndromes are ectodermal dysplasia,
Rieger syndrome, Down syndrome (trisomy 21), Witkop syndrome, van der Woude
syndrome, Brook syndrome, hemifacial microsomia and many others (16). Ectodermal
dysplasia refers to a heterogeneous inherited disorder characterized by variable defects in the
morphogenesis of ectodermal structures including hair, skin, nails, sweat glands, and teeth

13
(30). Oral and facial clefts are one of the most common birth anomalies: 1 in every 730
children is born with a cleft lip and/or palate (35). The anomaly is highly associated with
hypodontia, with a reported frequency (outside the cleft region) between 17.5% and 31.5%
(36).
Persisting primary teeth without successor When a permanent successor tooth is absent, the corresponding primary tooth often remains
in place beyond the time it would otherwise be shed. Once a congenitally absent successor
has been diagnosed, the choice of treatment must be based on the skeletal relationship,
occlusion and space requirements. Persisting primary teeth serve as space maintainers,
prevent resorption of the alveolar bone, may function as a semi-permanent solution long into
adulthood, and postpone the need for prosthetic replacement. Primary teeth left in situ carry a
risk of developing idiopathic root resorption and infraocclusion.
Infraocclusion refers to a tooth that has failed to maintain its occlusal relationship relative to
the adjacent teeth. Kurol (37) defined infraocclusion as the occlusal surface of the primary
molar being more than 1 mm below the occlusal plane of fully erupted neighbouring teeth.
Ankylosis is believed to be the primary pathological process in infraocclusion (38, 39).
Dental ankylosis occurs when partial root resorption is followed by either cementum or bone
formation, fusing the root and the alveolar bone (40). The mechanism may be due to an
imbalance in the normal pattern of resorption and repair, with repair processes prevailing over
resorptive ones, leading to excessive deposition of simple lamellar bone and cellular
cementum (41). The epithelial cell rests of Malassez are also believed to maintain the
function and regeneration of the periodontal membrane (42), and changes in the distribution
of these cells have been observed in the periodontium of ankylosed deciduous molars (40).
This might indicate a protective role of the epithelial rest of Malassez against root resorption.
Genetic factors may also be of importance, as the incidence of ankylosis is much higher
amongst siblings (37, 43). In addition, children with one infraoccluded primary molar often
develop infraocclusion of additional teeth (37). There is also an association, and most likely a
common genetic origin, between infraoccluded teeth and ectopic eruption of first molars, peg-
shaped laterals, enamel hypoplasia, palatal displacement of maxillary canines and
congenitally absent second premolars (44).
Infraocclusion occurs most commonly in the primary dentition, and the primary mandibular
molars are most frequently affected (37). The prevalence of infraoccluded primary molars has
been reported to vary between 8% and 14% among Swedish children (45), with an increasing
prevalence when the permanent successor tooth is missing. In a retrospective study, 66% of

14
patients with hypodontia showed infraocclusion of primary molars (46). In a longitudinal
study, infraocclusion of the primary mandibular second molar when lacking a successor was
found in 52% cases when the patients were 28-29 years (47). The extent of infraocclusion is
directly correlated with the rate of facial growth. If the infraocclusion is manifested before the
pubertal growth spurt, it may increase to a considerable amount when the velocity of growth
is at its peak (48). The ankylosed tooth will not be able to keep up with the vertical growth
and simultaneous eruption of the adjacent teeth, which may lead to occlusal disturbances such
as tilting of adjacent teeth and supra-eruption of antagonists. Progression of infraocclusion in
adults, however, has been reported to be negligible (49). The mandibular second premolar,
which is the successor of the primary mandibular second molar, is the most commonly
missing tooth with a prevalence of 2.4-4.3% (47). Despite the risk of infraocclusion, the
primary canines and mandibular second molars have the longest reported life span among
persisting primary teeth without successors (50). As a result, these particular teeth have been
the focus of the modest number of publications on the long-term survival of persisting
primary teeth left in situ. In general, these studies show a favourable prognosis (47-49, 51,
52), which will be discussed further in the section “Treatment options and methods for
replacing missing teeth in growing individuals”.
Other detrimental factors for the prognosis of persisting primary teeth are root resorption and
the amount of restorations. Root resorption occurs regardless of whether the permanent
successor is present or not, indicating that these processes are, to a great extent, governed by
intrinsic factors (40). The resorptive process has been reported not to follow any particular
pattern; both individual roots and teeth in the same patient can show completely different
degrees of resorption (40). It has also been observed that the rate of resorption of the roots of
primary teeth diminishes with age (45, 48, 51).
Oral health-related quality of life
Development
Several measures of oral health-related quality of life (OHRQoL) have been developed in the
recent years in order to improve the understanding of the psychosocial consequences of oral
diseases. OHRQoL was defined by Locker et al. (53) as “The impact of oral diseases and
disorders on aspects of everyday life that a patient or person values, that are of sufficient
magnitude, in terms of frequency, severity or duration to affect their experience and
perception of their life overall”. Adding a subjective dimension to the objective clinical
assessment of oral conditions gives a broader insight into oral health (54). There is now a

15
substantial body of research documenting self-perceived oral health, and the number of
indices continues to evolve (55). In general, these measures assess the frequency and/or
severity of functional, psychosocial and social impacts associated with oral disorders. They
have been referred to as sociodental indicators, subjective oral health status measures, patient-
based outcome measures, participant-based outcome measures or OHRQoL measures (55).
The use of patient-based outcome measures, such as OHRQoL, in dentistry emerged in the
early 1980s in line with the shift from a biomedical perspective to a broader biopsychosocial
model of health (56, 57). OHRQoL is a multi-dimensional approach to the impact of oral
disorders on an individual’s life measured from their own viewpoint, and includes subjects’
expectations and values (58). The assessment of the patient perspective offers new
opportunities for the improvement of dental care may serve as a basis for the allocation of
health care resources (59). OHRQoL questionnaires are used in epidemiological surveys to
identify the impact of oral conditions on the quality of life, and in clinical trials to measure
the effectiveness of interventions (55). The fundamental aim in all studies using these
measures is to detect differences between groups, either at one point in time (e.g. patients
with malocclusion or hypodontia) or over time (e.g. pre- and post-treatment) (55). Clearly
defined cut-off values for classifying an individual as mildly, moderately or severely
compromised on the basis of an OHRQoL measure have not been established.
Oral Index on Daily Performance
Background
One of the most commonly used OHRQoL instruments is the Oral Index on Daily
Performance (OIDP). The scale was developed to measure oral impacts that seriously affect
individuals’ daily activities (60), and has proven to be reliable and valid in cross-sectional
population-based studies as well as in studies of patients with specific oral disorders (61, 62).
The theoretical framework of OIDP is modified from the World Health Organization’s
(WHO) International Classification of Impairments, Disabilities and Handicap (ICIDH),
which was amended for dentistry by Locker (54). The modification is shown in Figure 2, and
is constructed with different consequence variables: impairment, intermediate impacts (pain,
discomfort, functional limitation and dissatisfaction with appearance) and ultimate impacts.
The first level refers to the oral status or the immediate biophysical outcome of disease, which
most clinical indices attempt to measure. The second level addresses the possible earliest
negative impacts caused by the oral health status. The dimensions may lead to one another;
functional limitation may cause pain, discomfort or dissatisfaction with appearance and vice
versa. The third level represents the physical, psychological and social impacts affecting the

16
ability to perform daily activities, i.e., “ultimate impacts,” which correspond to WHO’s and
Locker’s concept of disability and handicap (54, 63). Any of the dimensions in the first and
second level can lead to the third level. The advantages of measuring only level three
consequences are precise measurement while covering all dimensions, avoiding overscoring
of the same impact at each of the levels, the recording of significant impacts only, and the
ease of measuring behavioural impacts rather than feeling-state dimensions. Another
advantage of the OIDP instrument is that it consists of only eight items: eating, speaking,
cleaning teeth, smiling, sleeping, emotional balance, studying, and social contact. The OIDP
inventory has been translated into Norwegian, and validated in a representative sample of the
Norwegian adult population (64).
Generic and condition specific
The OIDP inventory is designed as a generic or condition specific (CS) measure. While the
generic inventory assesses the overall impact of oral problems simultaneously, the CS form
focuses on impacts attributed to a particular disease or condition. This makes the CS
instrument more sensitive to small, but clinically relevant, changes in specific oral diseases
(65, 66). This unique characteristic may provide insight into the consequences of an untreated
oral condition, and is particularly important when assessing treatment need as well as
prioritising dental health care services (67). A couple of studies have compared the generic
and CS forms of the OIDP, finding the CS OIDP to discriminate better among groups with or
without normative dental treatment requirements for caries, malocclusion, periodontal
disease, and traumatic dental injuries (68).
Figure 2. Theoretical framework of consequences of oral impacts, inspired by a figure by Adulyanon et al. (61)

17
Other health-related quality of life instruments in children and adolescents
Child Perceptions Questionnaire (CPQ)
The questionnaire was developed in Canada, and originally validated in children with caries,
malocclusion and craniofacial anomalies. The questionnaire is one of the most widely used
(69). It consists of questions divided into four domains, which encompass oral symptoms,
functional limitations, emotional and social well-being. The questions assess the child’s
opinions, the perceived views of peers about his/her dental appearance and behavioural
problems. The CPQ originally consisted of 37 questions; however, in order to facilitate its use
in clinical studies and population-based health surveys, the CPQ was shortened to 16 and 8
item versions (70). The CPQ has been translated into Norwegian, but not validated in a
Norwegian population (69).
The Oral Health Impact Profile (OHIP)
The OHIP index was originally developed based on Locker’s model of oral health (54). The
questionnaire was developed by asking Australians about their experience with oral diseases,
and the kinds of consequences that arose from the diseases. The most commonly used
experiences were reduced to 49 indicators/questions, which was the basis for the OHIP-49
(71). A shortened version of the OHIP with 14 items was developed later, and is organised
into seven dimensions (functional limitation, physical pain, psychological discomfort,
physical disability, psychological disability, social disability and handicap). The OHIP-14 and
its Norwegian translation have been shown to have acceptable reliability, validity and
precision (72-74).
Condition-specific measures in orthodontics
A condition-specific measure to assess quality of life in patients with hypodontia was
developed in 2011 by Akram et al. (75). A series of focus groups were used to identify four
issues (treatment, effect on daily activities, appearance and other peoples' reactions) of
importance for patients with hypodontia. The themes were incorporated into a questionnaire,
which was later tested, and proved to be a valid and reliable tool (76). The measure was
designed to illustrate how hypodontia affects a person’s quality of life, and how orthodontic
treatment might improve it, and also to influence issues such as funding for patients with
hypodontia.
18
Very recently, Patel et al. (77) developed the Malocclusion Impact Questionnaire (MIQ) to
measure oral-health related quality of life of young people with malocclusion. Three themes
(appearance of teeth, effect on social interactions and oral health/function) related to the
impact of malocclusion emerged after semi-structured interviews of patients referred for
orthodontic treatment. The themes were used to generate individual items for inclusion in the
questionnaire. The items were tested, and reduced to 17 questions. Cross-sectional testing
showed that the new MIQ was both valid and reliable (78); however, further evaluation is
required to confirm whether the measure is generalizable and has the ability to detect change
over time.
A condition-specific measure for patients with severe dentofacial deformities requesting
orthognathic treatment, called the Orthognathic Quality of Life Questionnaire (OQLQ) was
developed in 2000 by Cunningham et al. (79). The instrument’s content was derived through
a literature review and interviews with clinicians and patients. Four clinically meaningful
domains were established (social aspects of deformity, facial aesthetics, oral function and
awareness of facial deformity), with 22 contributing items/statements. The OQLQ shows
good evidence of reliability, validity and responsiveness, suggesting that the instrument may
be useful both in clinical trials (e.g. comparing the effects of single jaw and bimaxillary
surgery) and in quality assurance.
Quality of life in patients with hypodontia
The quality of life in patients with hypodontia has been examined to some extent. Anweigi et
al. (80) investigated the impact of mild, moderate and severe hypodontia on OHRQoL in 82
patients using the OHIP-49. All patients experienced one or more impact, with impacts
related to appearance being the most prevalent. The number and location of missing
permanent teeth was not a good predictor of quality of life. Females reported a higher level of
impacts than males. Using the CPQ, Wong et al. (81) assessed the OHRQoL in 25 patients
with severe hypodontia and its association to the number of missing teeth. All participants
reported OHRQoL impacts. When accounting for retained primary teeth, the number of
missing teeth correlated positively with OHRQoL impacts. The drawback to these two studies
is that they do not have any comparable control group.
Laing et al. (82) and Kotecha et al. (83) compared children with hypodontia to a malocclusion
control group using the CPQ. Laing et al. (82) compared 62 hypodontia patients to a
malocclusion group of similar normative treatment need and found no difference in quality of
life. Kotecha et al. (83) compared 86 hypodontia patients to a malocclusion group of lesser
normative treatment need and observed significantly higher oral impacts in the hypodontia
group. Locker et al. (84) assessed the functional and psychosocial impact of oligodontia in 36

19
children, and compared the results to published data of other clinical groups. Slightly above
three-quarters of the subjects reported one or more functional and/or psychosocial impacts.
Children with oligodontia appeared to have worse OHRQoL than children with dental decay
and malocclusion, but better OHRQoL than children with oro-facial conditions.
A few studies have demonstrated a clear improvement in OHRQoL among patients with
hypodontia after missing teeth have been replaced by either resin-bonded bridges (85) or
dental implants (86).
Therapeutic approaches in cases with severe hypodontia
Interdisciplinary approach
Children and adolescents with congenitally missing teeth need thorough planning and serious
consideration of different therapies, in order to optimise the outcome of treatment in a
lifelong perspective (87). The treatment approach will depend on the overall dentofacial
morphology, the location and the number of missing teeth, the availability of different
treatment methods, and the age of the patient. Severe hypodontia is often complicated and
requires an interdisciplinary approach at specialist level, both during the initial evaluation
phase and when treatment is provided. The interdisciplinary team may include participation
from the disciplines of orthodontics, paediatric dentistry, oral surgery, prosthodontics and oral
radiology (88).
The co-operation of specialists has the advantage that each discipline contributes with their
expertise to assure a satisfactory outcome. Experience from Aplasicenteret in Northern
Jutland documents that treatment of severe hypodontia is complex, with numerous treatment
alternatives, and that that the interventions carried out by different specialist disciplines must
be coordinated (89). Furthermore, centralising the management of patients with rare
diagnoses allows the team of participating specialists to accumulate knowledge and gain
relevant experience with such a patient group. It also provides a unique opportunity for
aggregation of research data.
Treatment course in hypodontia patients Treatment usually takes place in stages. In an early stage, often at the end of the mixed
dentition phase, vertical dimensions are increased if necessary; teeth are orthodontically
moved to the anterior region; and primary teeth and/or small permanent teeth (peg-shaped)
are reshaped in order to improve aesthetics. Eruption disturbances are treated, and primary
teeth sometimes extracted to guide the eruption of the permanent teeth. The option of
20
autotransplantation is always kept in mind, especially in cases of asymmetric hypodontia, and
primary teeth with a reasonably good prognosis are maintained. When appropriate, the
patients may receive semi-permanent solutions such as resin-bonded bridges, laminates or
crowns. Partial dentures may be applied as an interim phase, or, in some cases, as a definitive
treatment. A further stage usually takes place when the need arises, after the cessation of
growth. At this point in time, more permanent solutions are considered, such as dental
implants and bridges. Orthodontic therapy is often required prior to prosthetics in order to
parallel the roots, optimise the location of the teeth and, in some cases, increase the bone
volume.
Treatment options and methods for replacing missing teeth in growing
individuals An overarching goal in growing individuals is to minimise the number of teeth to be replaced.
Biological methods, such as growth-adapted measures, orthodontic treatment and
autotransplantation are preferable to prosthetic replacement (88). The loss of teeth, primary or
permanent, leads to a risk of reduction in the volume of the alveolar ridge by resorption. A
25% reduction of the ridge width within 3 years after extraction of a primary mandibular
molar with a missing permanent successor has been reported (90). A reduction in alveolar
ridge width or height is likely to influence future treatment options, and the preservation of
the alveolar processes should be strived for whenever possible. Therapies that both substitute
missing teeth and preserve the alveolar ridge are orthodontic or spontaneous space closure,
autotransplantation and preservation of primary teeth.
Preservation of primary teeth
In children with a reduced number of permanent teeth, the primary teeth are of great value,
and should be preserved as long as they remain functional and other treatment does not
require extraction. Extraction of primary teeth with a missing successor may be
contraindicated in some types of malocclusions such as low-angled cases with deep bite,
patients with general spacing or patients with broad jaws and narrow teeth. The decision to
preserve a primary tooth as a substitute for a missing permanent tooth depends on the
prognosis of the primary tooth in terms of infraocclusion, root resorptions and the extent of
restorations. Nordquist et al. (52) collected x-rays of patients with retained primary teeth. The
authors concluded that the primary mandibular molars and maxillary canines had the best
prognosis.

21
Bjerklin et al. (47) found that only 7 of 99 primary molars were lost from the age of 12-13 to
adulthood. Ith-Hansen et al. (51) carried out a follow-up study spanning 15 years. Out of 26
persisting primary molars, only three had been extracted and three showed extensive root
resorption. Rune et al. (48) observed 77 children with 123 retained primary molars to a mean
age of 17 years. Only 5% of the teeth had been extracted, and root resorption remained
unchanged in 50%. Sletten et al. (49) evaluated 20 adults with 28 persisting mandibular
molars. Four teeth were lost due to caries or periodontal disease, and 86% were still in
function. In 2008, Bergendal (91) reviewed the topic of when to extract deciduous teeth in
young individuals and replace them with implants. There was only limited, low-level
evidence concerning this question in the literature. Recommendations were mainly based on
clinical experience. The review stated that there are a limited number of reports, which
support that a majority of the deciduous teeth that are healthy at 20 years of age can serve for
many more years, and that retaining them can be a viable and biologic treatment alternative.
Space closure
Spontaneous space closure
Spontaneous space closure involves extracting a primary tooth with the intention of guiding
the eruption of a permanent tooth to a more favourable position. Thereby, the need for
orthodontic therapy is reduced.
Lindqvist (92) reported that in subjects congenitally missing the mandibular second premolar,
extraction of the second primary molar at the age of 8 to 9 – before the root development of
the mandibular first premolar and the emergence of the second permanent molar – was
followed by spontaneous space closure. Mamopoulou et al. (93) investigated the amount of
space closure and occlusal changes in 11 patients (mean age 11.8 years) with agenesis of the
mandibular second premolar after extraction of the primary molar and the maxillary second
premolar on the side of the agenesis. After four years, only 1 mm and 2 mm residual space
were recorded in the maxilla and in the mandible, respectively. Most of the extraction space
closed during the first year. In the maxilla, the mesial and rotational movements of the first
molars contributed to 70% of the closure of the extraction space, while in the mandible, the
space closure occurred by mesial/rotational movements and tipping of the first molars, as well
as distal movement and tipping of the first premolars. The teeth were extracted when the
occlusion of the first premolars was secured, close to the peak of the pubertal growth spurt.
Unilateral extraction had no influence on the maxillary midline, whereas it caused a
statistically significant mandibular dental shift to the extraction side. Extraction therapy had
no impact on the overjet, overbite or incisor inclination. A favourable factor for space closure
according to Bjork et al. (94) is the growth in facial height, which stimulates tooth eruption

22
and mesial dental drifting of the molars. Additionally, a growth pattern involving anterior
rotation of the mandible influences the direction of eruption of the posterior teeth, with
correlations between mandibular growth and mesial migration of the lower molars (95). In
patients with severe hypodontia, extraction of primary teeth might be suitable, in order to
guide the eruption of permanent teeth such as permanent molars or canines in a more mesial
direction.
Orthodontic space closure
The obvious advantages of orthodontic space closure are the longevity of the therapeutic
result, and the completion of the treatment in early adolescence (96). The movement of a
tooth into an edentulous space ensures that the alveolar bone height is maintained, and that
adaptive changes taking place after treatment will be in line with natural development (97). In
patients with a high smile line, a normal gingival and alveolar architecture is important in
order to meet the aesthetic demands (97, 98). In cases of congenitally missing lateral incisors,
orthodontic space closure with canine substitution has been reported to be a viable alternative
with predictable results (99-101). Interventions to improve aesthetics such as tooth reshaping,
positioning and bleaching, and in some cases thin porcelain veneers or composite build-ups,
might be necessary (97). According to Kokich et al. (102), there are two malocclusions that
permit canine substitution. These are an Angle class II malocclusion, with no crowding in the
mandibular arch, or an Angle class I malocclusion, with severe crowding in the lower arch
where it is necessary to carry out extractions. Other factors to be considered are the facial
profile, and the size and colour of the canine.
In patients with severe hypodontia, reaching the therapeutic goal solely by orthodontic space
closure is unrealistic, and might also compromise facial aesthetics. In these severe cases,
orthodontic space closure seeks to mesialise teeth into the anterior region, preparing spaces
posteriorly for prosthetics. A disadvantage of orthodontic space closure is that long-term
retention with directly bonded lingual retainers is often required in order to assure stability. In
addition, orthodontic treatment may involve substantial tooth movements over a prolonged
period of time, which increases the risk of apical root resorption (103). A long-lasting
treatment is also burdensome for the patient and orthodontist.
Autotransplantation Dental autotransplantation is a procedure in which a tooth is surgically moved from one site
in the mouth to another in the same individual (104). An autotransplanted tooth can substitute
either a congenitally missing tooth or early loss of teeth due to trauma or caries. The
treatment has the potential to preserve the alveolar bone during growth, and re-establish a

23
normal alveolar process after traumatic bone loss (105). The missing tooth is replaced by the
patient’s own tooth, which is the most biocompatible material (104).
Autotransplantation can be suitable in patients with asymmetrical agenesis, where the
transplanted teeth can provide a more even distribution of teeth in the arch. The procedure has
shown highly predictable results and good long-term outcomes, with reported survival rates
ranging from 75.3% to 91% (104, 106). The teeth most frequently used as grafts are
premolars, whose root development is favourable for transplantation in the age range 10 to 12
years on average. Autotransplantation carries a significant risk in hypodontia patients, as
failure of the procedure will result in the loss of one of the patient’s already few teeth. One
must therefore be confident of a good prognosis for this intervention to be recommended. In
addition, the success rate depends to a great extent upon surgeon skill (106). Complications
after autotransplantation include the risk of root resorption, arrested root formation and
replacement resorption (ankylosis) (107). Clinical signs of ankylosis include arrested eruption
within 6 to 12 months (107).
Removable dentures
Removable dentures may be indicated to restore long spans and multiple missing teeth where
dental implants are not possible. In young patients where a definitive treatment is postponed,
they may also function as a semi-permanent solution. The dentures can provide a predictable
solution and are able to replace soft and hard tissue deficiencies without invasive surgery
(108). However, they do have the potential to increase caries incidence and periodontal
problems, increasing the importance of preventative measures and appropriate case selection
(108).
Conventional and adhesive fixed bridgework
Conventional bridgework is generally contraindicated in young patients with relatively
immature pulps, and where abutment teeth are sound (108). In cases with a narrow alveolar
ridge not suitable for dental implants and where the edentulous span is relatively short, this
treatment option may be indicated. This may be the case where teeth are conical, diminutive
or worn, requiring only limited preparation, and there is a plan to increase the occlusal
vertical dimension (108). Another indication for a conventional bridge is the presence of
adjacent teeth that require rehabilitation due to caries, fractures or discolorations (96). A
systematic review conducted by Sailer et al. (109) reported a 5-year survival rate of 94.4% for
metal-ceramic restorations and of 88.6% for all-ceramic restorations.

24
The adhesive technique has the great advantage that it requires only a limited amount of tooth
substance to be removed during preparation. Other advantages include the avoidance of
pulpal trauma, the supragingival preparation, the simplicity of the clinical procedures and the
reduced cost and chair time, in comparison with conventional fixed prostheses (96). The
vertical position of the abutment teeth is a prognostic factor, as a shallow overbite reduces the
excessive lateral forces on the abutments and permits sufficient tooth surface for bonding.
Other concerns influencing the prognosis are the inclination, mobility and labiolingual
thickness of the abutment teeth (96). Various studies have been published regarding the
longevity of resin-bonded prostheses. The change in design from two retainers to a single-
retainer cantilever, as well as from metal-ceramic to all-ceramic restorations with more recent
cementation systems, have led to increased survival rates (96). Recent studies have shown
survival rates of single-retained resin bonded fixed dental prostheses from 94.4% to 100%
after 4 to 10 years of follow-up (110-113).
Dental implants
Modern dental implantology began more than 40 years ago with the work of Professor
Brånemark from Sweden and Professor Schroeder from Switzerland. Brånemark was the first
to observe that titanium had the unique property of developing a direct attachment to bone,
which he termed “osseointegration” (114). The concept of osseointegration was designed and
evaluated for the mature skeleton (114). Dental implants in the growing maxilla or mandible
have been demonstrated, both clinically and experimentally, to behave like ankylosed teeth,
becoming submerged adjacent to natural teeth, because of the continued eruption of teeth and
associated growth of the alveolus (115-118). The insertion of osseointegrated dental implants
should therefore, in general, be delayed until the permanent dentition is fully erupted and
growth is completed. However, large variations in skeletal maturation exist among
individuals.
In extreme forms of hypodontia, such as hypohidrotic ectodermal dysplasia, severe
oligodontia or anodontia, early placement of dental implants may take place as early as at the
age of 3 years in order to provide support for overdentures or bridge restorations (89). A
consensus conference recommended that the earliest age for placement of implants in the
anterior region of the growing mandible (with the absence of alveolar bone) should be 7 or 8
years of age (119). In the growing edentulous maxilla, there was insufficient clinical or
experimental data to support a recommendation for the placement of implants (119).
Several studies have reported the successful osseointegration of single implants replacing
missing teeth, provided that there is sufficient bone volume and appropriate space between
adjacent teeth (96, 120-124). The main advantage of placing a dental implant is that healthy

25
adjacent teeth remain untouched. The most frequently reported aesthetic complications with
implants have been resorption of the facial bone wall, recession of the facial soft tissue,
incomplete papilla filling, thread exposure and infraocclusion (96, 125-129). Additional
biological and technical complications include fistulas, peri-implantitis, screw loosening and
porcelain chipping (96, 120, 123, 125).
Treatment outcome in patients with severe hypodontia Clinical studies of hypodontia patients are challenging due to the dynamic nature of the
condition, where the clinical picture and treatment need are in constant change. Recently, a
systematic review was published comparing the outcome of dental treatment in patients with
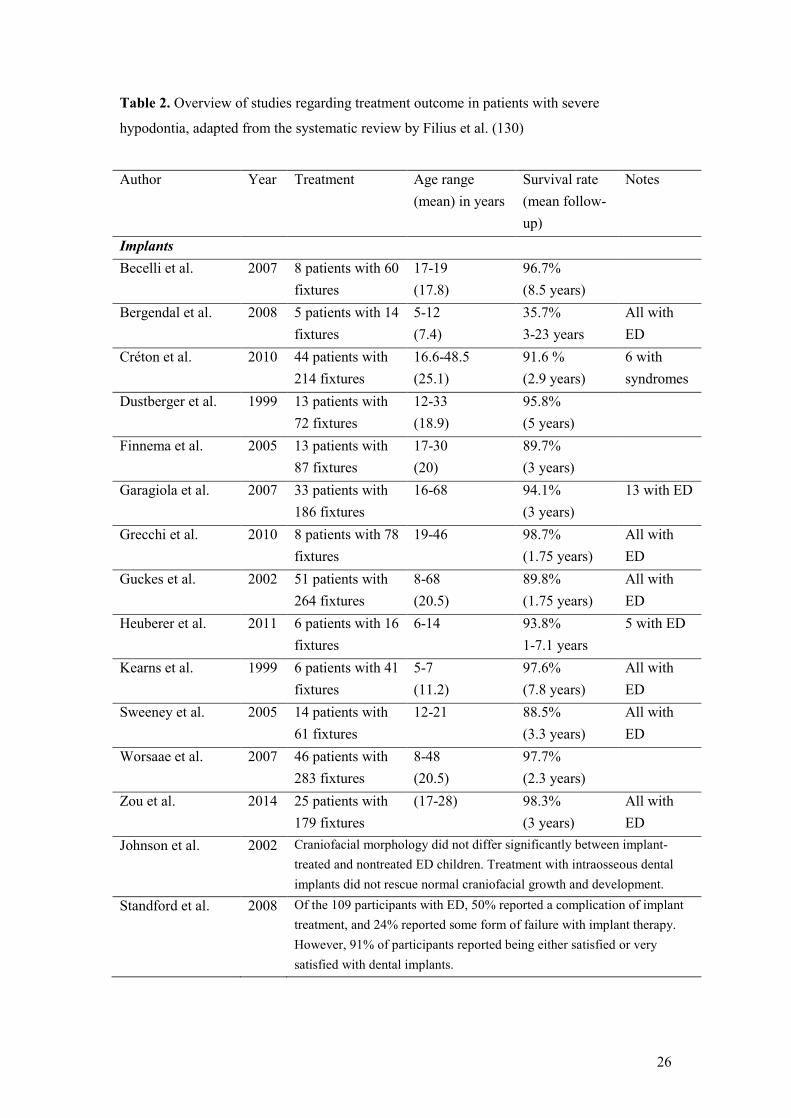
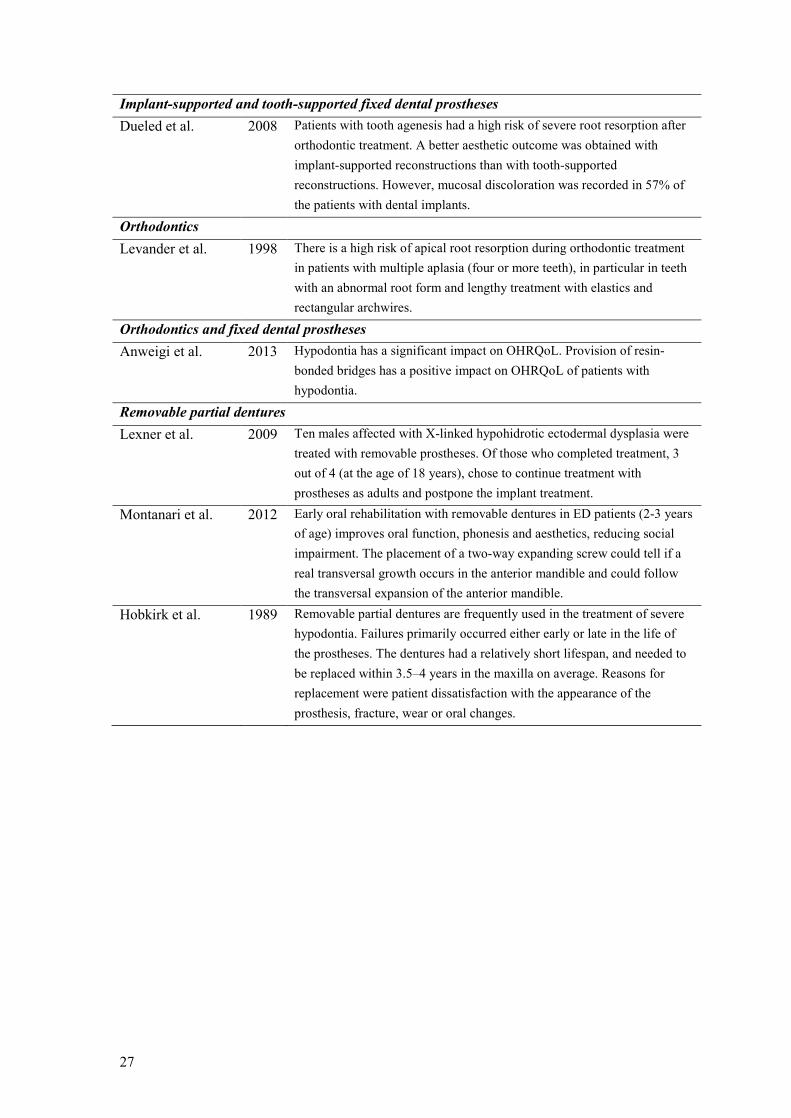
severe hypodontia (Table 2) (130). The authors emphasised that there is currently no standard
approach or favourable dental treatment option to treat this group of patients. Twenty-one
studies were included; seventeen studies had a retrospective design; sixteen studies described
the results of implant treatment. The results of treatment with dentures, orthodontics, fixed
crowns or bridges were sparsely presented. Implant survival ranged from 35.7% to 98.7%
(mean 93.7%), and was influenced by bone quantity and implant location. Most implants
were lost during the first year after placement, and more implants were lost in the maxilla
than in the mandible. Patients with severe hypodontia have a higher implant loss compared to
healthy subjects. Deepened peri-implant sulci and radiographic crestal bone resorption were
seen in severe hypodontia patients, with most bone resorption occurring the first year after
placement and continuing at a relatively constant level afterwards. The review concluded that
it is currently not possible to make evidence-based decisions for the treatment of patients with
severe hypodontia due to the condition’s heterogenic presentation, its low prevalence and the
poor quality of studies.
26
Table 2. Overview of studies regarding treatment outcome in patients with severe
hypodontia, adapted from the systematic review by Filius et al. (130)
Author Year Treatment Age range (mean) in years
Survival rate (mean follow-up)
Notes
Implants Becelli et al. 2007 8 patients with 60
fixtures 17-19 (17.8)
96.7% (8.5 years)
Bergendal et al. 2008 5 patients with 14 fixtures
5-12 (7.4)
35.7% 3-23 years
All with ED
Créton et al. 2010 44 patients with 214 fixtures
16.6-48.5 (25.1)
91.6 % (2.9 years)
6 with syndromes
Dustberger et al. 1999 13 patients with 72 fixtures
12-33 (18.9)
95.8% (5 years)
Finnema et al. 2005 13 patients with 87 fixtures
17-30 (20)
89.7% (3 years)
Garagiola et al. 2007 33 patients with 186 fixtures
16-68 94.1% (3 years)
13 with ED
Grecchi et al. 2010 8 patients with 78 fixtures
19-46 98.7% (1.75 years)
All with ED
Guckes et al. 2002 51 patients with 264 fixtures
8-68 (20.5)
89.8% (1.75 years)
All with ED
Heuberer et al. 2011 6 patients with 16 fixtures
6-14 93.8% 1-7.1 years
5 with ED
Kearns et al. 1999 6 patients with 41 fixtures
5-7 (11.2)
97.6% (7.8 years)
All with ED
Sweeney et al. 2005 14 patients with 61 fixtures
12-21 88.5% (3.3 years)
All with ED
Worsaae et al. 2007 46 patients with 283 fixtures
8-48 (20.5)
97.7% (2.3 years)
Zou et al. 2014 25 patients with 179 fixtures
(17-28) 98.3% (3 years)
All with ED
Johnson et al. 2002 Craniofacial morphology did not differ significantly between implant-treated and nontreated ED children. Treatment with intraosseous dental implants did not rescue normal craniofacial growth and development.
Standford et al. 2008 Of the 109 participants with ED, 50% reported a complication of implant treatment, and 24% reported some form of failure with implant therapy. However, 91% of participants reported being either satisfied or very satisfied with dental implants.
27
Implant-supported and tooth-supported fixed dental prostheses Dueled et al. 2008 Patients with tooth agenesis had a high risk of severe root resorption after
orthodontic treatment. A better aesthetic outcome was obtained with implant-supported reconstructions than with tooth-supported reconstructions. However, mucosal discoloration was recorded in 57% of the patients with dental implants.
Orthodontics Levander et al. 1998 There is a high risk of apical root resorption during orthodontic treatment
in patients with multiple aplasia (four or more teeth), in particular in teeth with an abnormal root form and lengthy treatment with elastics and rectangular archwires.
Orthodontics and fixed dental prostheses Anweigi et al. 2013 Hypodontia has a significant impact on OHRQoL. Provision of resin-
bonded bridges has a positive impact on OHRQoL of patients with hypodontia.
Removable partial dentures Lexner et al. 2009 Ten males affected with X-linked hypohidrotic ectodermal dysplasia were
treated with removable prostheses. Of those who completed treatment, 3 out of 4 (at the age of 18 years), chose to continue treatment with prostheses as adults and postpone the implant treatment.
Montanari et al. 2012 Early oral rehabilitation with removable dentures in ED patients (2-3 years of age) improves oral function, phonesis and aesthetics, reducing social impairment. The placement of a two-way expanding screw could tell if a real transversal growth occurs in the anterior mandible and could follow the transversal expansion of the anterior mandible.
Hobkirk et al. 1989 Removable partial dentures are frequently used in the treatment of severe hypodontia. Failures primarily occurred either early or late in the life of the prostheses. The dentures had a relatively short lifespan, and needed to be replaced within 3.5–4 years in the maxilla on average. Reasons for replacement were patient dissatisfaction with the appearance of the prosthesis, fracture, wear or oral changes.

28
Aims of this work
Overall aim The overall objective of this work was to gain knowledge about the clinical course of
hypodontia, treatment alternatives and their suitability in different circumstances, and how the
condition affects the patients’ psychosocial wellbeing.
Specific aims
• To assess the prognosis of persisting primary mandibular molars without a successor,
in terms of root resorption, infraocclusion and restorations (Paper I).
• To survey the psychosocial status of patients with hypodontia and a malocclusion of
similar normative treatment need. The two groups were compared using a generic
form and a condition specific form of the Oral Impact on Daily Performance (OIDP)
inventory (Paper II).
• To follow up patients with severe hypodontia, comparing the resulting crown and
soft-tissue morphology for orthodontic space closure, dental implants and tooth-
supported fixed dental prostheses (FDPs) replacing teeth in the anterior region. Also,
the treatment performed and the types and locations of substitutes for all congenitally
missing teeth are assessed (Paper III).
29
Materials
Study groups The basis of this thesis is a patient sample collected through the activities of an
interdisciplinary team (Eksperttjenesten) at the Department of Orthodontics, University of
Oslo from 1998 to 2010. During this period, 573 patients were referred by their primary
dentist or dental hygienist. Of these, 212 had hypodontia and 134 suffered from severe
hypodontia.
The interdisciplinary team was established in 1998, and includes specialists in orthodontics,
paediatric dentistry, oral surgery and prosthodontics. The purpose of the unit is to provide
advisory and therapeutic dental services for children and adolescents in need of advanced oral
health care. The patients are referred to the team for a clinical examination, and a tentative
treatment plan in both a short- and a long-term perspective is established. Patients residing
within a practical distance to the university clinic are often offered to complete the entire
treatment course there, and the remaining patients usually carry out treatment at their local
dentist or specialist clinic. Seventy-seven patients received treatment at the university clinic,
and 135 patients were treated at their place of residence.
In paper I, 111 of the 212 patients with hypodontia are included, as the inclusion criteria are
the congenital absence of at least one mandibular second premolar.
In paper III, 71 of the 134 patients with severe hypodontia are included, as they were aged 18
or more, and could be expected to have completed the majority of the treatment course. The
patients were invited by mail or telephone to participate in a follow-up study, and 50 patients
(70%) accepted. Of those not attending, 5 could not be reached, 7 did not wish to participate
in the study, and 9 declined for practical reasons. In 9 of the 50 cases, the patients were
unable to travel to the University of Oslo, and examination was performed in cooperation
with an orthodontist at the patient’s place of residence.
In paper II, patients referred to the interdisciplinary team or to the post-graduate clinic at the
Department of Orthodontics between January 2012 and September 2013 were consecutively
recruited. Sixty-two patients with non-syndromic hypodontia and 101 non-hypodontia
patients with a malocclusion of similar normative treatment need were included.
30
Data collection All records for the 212 hypodontia patients were retrieved, and the following data denoted:
gender, date of birth, year of referral, referring dentist or specialist, original place of
residence, diagnosis, involved teeth (number and location), persisting primary teeth (number
and location), and recommended treatment plan. Treatment was categorised as orthodontic
treatment, implant-supported prostheses, retaining primary teeth, composite restoration, tooth-
supported fixed dental prostheses, veneer restoration, orthognathic surgery,
autotransplantation, or combinations of the above.
Methodological considerations
Measurements on panoramic radiographs (paper I) Decisions on whether or not to preserve a persisting primary molar without a successor
should be based on a prediction of the tooth’s longevity. In this regard, the three parameters
infraocclusion, root resorption and restorations will guide the clinical decision about the fate
of the primary tooth.
For the purpose of measuring infraocclusion, linear measurements on intraoral radiographs or
dental casts have been the most common method (45, 47-49, 51). With only panoramic
radiographs available in the records of patients included in paper I, relative measurements
were chosen, knowing that magnification is not reproducible between panoramic radiographs
and even between regions in the same image. These relative measurements are not directly
comparable with absolute measurements from other studies. Therefore, a threshold of
clinically significant infraocclusion roughly equivalent to other authors’ definitions (37, 131)
was established. Root resorption was scored subjectively on a six-point scale of severity,
adapted from Bjerklin et al. (132), and restorations were recorded as no restoration,
approximal restoration or occlusal restoration.
OIDP questionnaire (paper II) The hypodontia patients and the malocclusion patients were administered a structured
questionnaire, including the OIDP inventory and questions regarding their perceived oral
health status. Both generic and condition specific OIDP indicators were calculated. The
questionnaire was self-administered at the university clinic. All included patients were

31
assigned to either the hypodontia group or the malocclusion group based on available dental
casts, intraoral photographs and radiographs.
Other measures of OHRQoL, such as the Child Perception Questionnaire (CPQ) (133) or the
Child Oral Health Impact Profile (COHIP) (134), which, in addition to the OIDP, are the most
frequently used measures for self-completion by children (69), could also have been
appropriate for the study. The OIDP has already been translated into Norwegian and validated
in a representative population sample; thus, a set of normative data exists (64). The OIDP is
also simple in that it measures behavioural impacts only rather than feeling-state dimensions,
and consists of only eight questions.
In addition to the generic OIDP measure, the inventory is also designed with a condition
specific measure, assessing impacts caused by a particular disease or condition. Paper II
compared the ability of the generic and condition specific OIDP measures to discriminate
between patients with hypodontia and patients with a malocclusion of similar normative
treatment need. A malocclusion group was chosen as controls, rather than patients with an
ideal Class I occlusion that would not be comparable due to expected large differences in
daily impacts. By including the condition specific measure, it is also possible to assess
whether impacts experienced by hypodontia patients are directly associated to the condition,
and not to a co-existing malocclusion. Impacts attributed to small teeth, gaps between teeth
and missing teeth were considered to be condition specific impacts attributed to hypodontia,
and only these items were scored in the condition specific analysis.
Follow-up with clinical examination (paper III) After several years of operation, the interdisciplinary team at the University of Oslo had
evaluated a relatively large group of hypodontia patients. The time was appropriate to gather
knowledge on the patients’ outcome. Patients with severe hypodontia aged 18 or more, who
would most likely have completed the majority of the planned treatment course, were invited
for a follow-up examination. Mucosal discoloration, crown morphology, colour of the
replacement tooth, and papilla level was compared for three different treatment modalities:
orthodontic space closures, dental implant fixtures (either single or part of an implant-retained
prosthesis) and FDPs (tooth-supported conventional or resin-retained prostheses) replacing
one or more missing teeth in the anterior region. Neither biological (e.g. pocket depths,
bleeding on probing, bacteriological sampling) nor radiographic (marginal bone level, buccal
bone level, 3D imaging) measures were performed, as no prior data for comparison existed in
the patients’ records. In addition, treatment had already been performed at a number of
different clinics, and such parameters had not been systematically recorded.

32
The patients who accepted to take part in the study were invited to the university clinic. For
those who accepted, but could not attend due to a long travel distance, a local orthodontist
carried out the examination after being briefed by one of the investigators. The morphological
variables were assessed by the author using standardised photographs and radiographs taken
during the examination. This gives rise to potential errors, as a perfect standardisation of
photographs is not possible due to different equipment and operators.
The treatment performed was noted and compared to the original plan. The number of
persisting primary teeth without successors, and their survival, was recorded. In addition, the
patients were given a questionnaire regarding their satisfaction with their dental status, the
treatment process and the outcome.
Statistical methods (Papers I-III) All data were processed with the Statistical Package for the Social Sciences (versions 19.0—
22.0; SPSS Inc., Chicago, IL, USA).
Papers I and III raised a common methodological issue, namely the unit of analysis for
statistical tests. Both papers involved several measurements being performed on individual
teeth. If the individual tooth is chosen as unit of analysis, measurements made on different
teeth belonging to the same patient will represent a problem, as the data are not independent.
A requirement for tests of statistical significance is that the data to be tested are independent.
Therefore, the data in question had to be aggregated with the patient as unit of analysis. This
was achieved by selecting only one data point from each patient to be included in significance
testing. A consequence of this is that some information will be lost; however, we found this to
be the most correct method of performing rigorous statistics on such unstructured clinical
data.
Table 3 summarizes the statistical methods used in the papers; the specific statistical tests
performed are described in detail in the separate papers.

33
Table 3. Statistical methods and tests used in Papers I-III.
Statistical method Paper I Paper II Paper III
Intraclass correlation coefficient (ICC) +
Paired t-test +
Spearman correlation coefficient + +
Effect size statistics +
Chi-square statistics + + +
Mann-Whitney U test +
Cronbach’s alpha coefficient +
Logistic regression +
Summary of results
Paper I: The prognosis of retained primary molars without successors: infraocclusion,
root resorption and restorations in 111 patients
The prognosis of the persisting primary molars without successors was estimated in terms of
infraocclusion, root resorption and restoration. An infraocclusion ratio was calculated in 92
patients (49 left molars and 43 right molars); infraocclusion of clinical significance (ratio > 2,
i.e. more than 20% of the neighbouring first molar’s crown height) was found in 44% of the
patients. The analyses of root resorption and restorations were carried out on 111 patients (58
left molars and 53 right molars). The mesial and distal root exhibited no root resorption in
19% and 34%, respectively. Most of the patients had no restorations (78%). Infraocclusion
and age were found to be weakly, but significantly correlated with root resorption.
Paper II: Discriminative ability of the generic and condition specific Oral Impact on
Daily Performance (OIDP) among adolescents with and without hypodontia
Questionnaires and clinical data were obtained for 62 patients (mean age 13.6, SD 2.1) with
hypodontia and 101 patients (mean age 12.5, SD 1.5) without hypodontia, but with a
malocclusion of similar normative treatment need (IOTN, DHC 4 or 5). The mean number of
missing teeth (absolute hypodontia) in the hypodontia group was 6.2 (1–21), and the mean
number of missing teeth minus number of persisting primary teeth (relative hypodontia) was
3.1 (0–14). The prevalence of generic and CS oral impacts in the hypodontia group were 64%
and 30%, respectively, and the corresponding rates in the non-hypodontia group were 62%

34
and 10%. The generic OIDP did not discriminate between the two groups with respect to
overall scores. The CS OIDP discriminated strongly between patients with and without
hypodontia regarding problems with emotional status, showing teeth, social contact, speaking
and carrying out work. Compared to the non-hypodontia group, patients with hypodontia,
with severe hypodontia (≥ 6 missing teeth) and upper anterior hypodontia were respectively
3.4, 2.5 and 7.0 times more likely to report any oral impact attributed to small teeth, gaps
between teeth and missing teeth.
Paper III: Tooth replacements in young adults with severe hypodontia: orthodontic
space closure, dental implants and tooth-supported fixed dental prostheses. A follow-up
study
Fifty patients (mean age 25.6 years) with severe hypodontia were invited to participate in a
follow-up study of treatment outcome. The most commonly prescribed treatments were dental
implants, orthodontic space closure and retaining primary teeth. The persisting primary teeth
showed a good survival rate at the follow-up examination. Crown and soft-tissue variables
(mucosal discoloration, crown morphology, colour and papilla index) were compared for
orthodontic space closure, dental implant fixtures and tooth-supported fixed dental prostheses
(FDPs) replacing teeth in the anterior region. All implant fixtures in the anterior mandible and
almost two thirds in the anterior maxilla had either mucosal discoloration or visible metal.
The crown morphology in the anterior mandible was significantly better for FDPs than
implant fixtures, but the colour score was better with an implant fixture than an FDP in the
anterior maxilla. For both dental fixtures and FDPs, poor papilla indexes were observed.
Orthodontic space closure resulted in superior papilla aesthetics, but had the drawback of a
less optimal crown morphology in the anterior mandible.
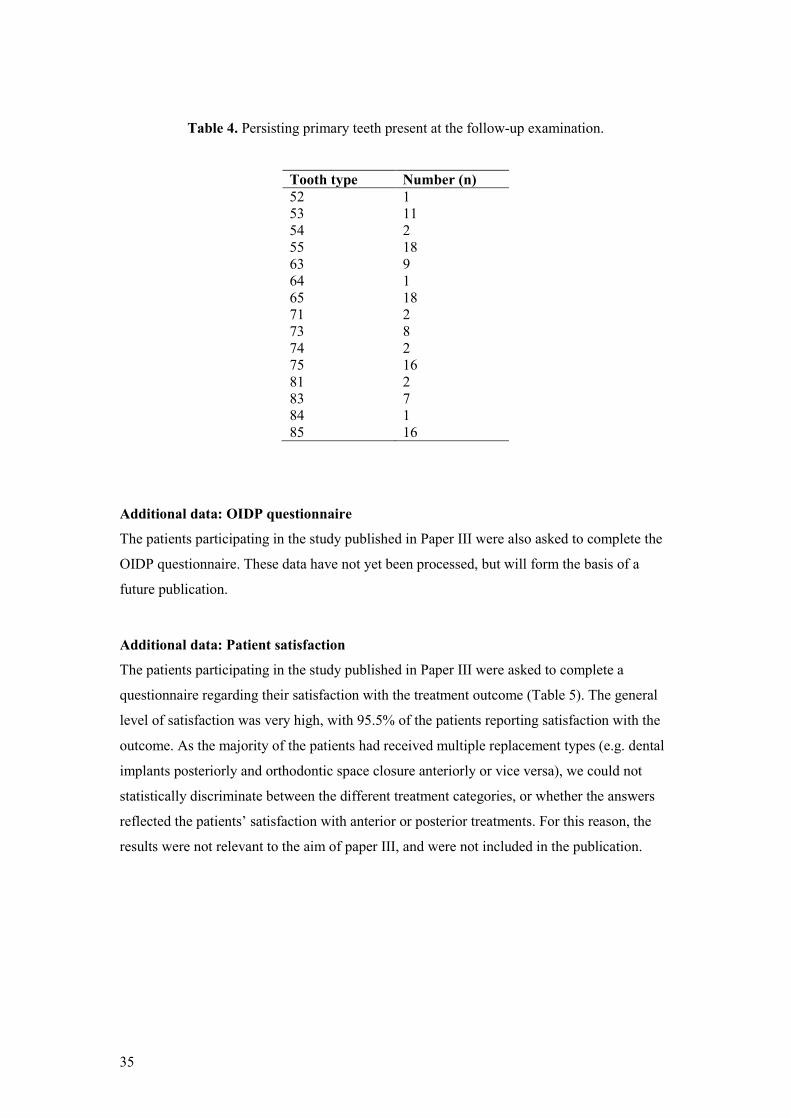
Additional data: Persisting primary teeth
The persisting primary teeth that were present at the follow-up examination are presented in
Table 4. Thirty patients were recommended to keep one or more primary teeth. At the follow-
up examination after a mean of 12 years 28 patients still possessed primary teeth.
35
Table 4. Persisting primary teeth present at the follow-up examination.
Tooth type Number (n) 52 1 53 11 54 2 55 18 63 9 64 1 65 18 71 2 73 8 74 2 75 16 81 2 83 7 84 1 85 16
Additional data: OIDP questionnaire
The patients participating in the study published in Paper III were also asked to complete the
OIDP questionnaire. These data have not yet been processed, but will form the basis of a
future publication.
Additional data: Patient satisfaction
The patients participating in the study published in Paper III were asked to complete a
questionnaire regarding their satisfaction with the treatment outcome (Table 5). The general
level of satisfaction was very high, with 95.5% of the patients reporting satisfaction with the
outcome. As the majority of the patients had received multiple replacement types (e.g. dental
implants posteriorly and orthodontic space closure anteriorly or vice versa), we could not
statistically discriminate between the different treatment categories, or whether the answers
reflected the patients’ satisfaction with anterior or posterior treatments. For this reason, the
results were not relevant to the aim of paper III, and were not included in the publication.

36
Table 5. Questions related to tooth replacements with patients’ responses.
1. How was your experience with pain and
discomfort in conjunction with the
treatment?
No such problems
Acceptable
Uncomfortable
6 (13.6%)
20 (45.5%)
18 (40.9%)
2. Did you or your parents receive
sufficient information about the treatment
procedures?
Yes
Don’t remember
No
31 (70.5%)
7 (15.9%)
6 (13.6%)
3. Did you or your parents receive
sufficient information about other
treatment options?
Yes
Don’t remember
No
12 (27.3%)
25 (56.8%)
7 (15.9%)
4. Did you/your parents find it easy or
difficult to choose a tooth replacement as a
solution to your problem with missing
teeth?
Easy
Unsure
Difficult
36 (81.8%)
6 (13.6%)
2 (4.5%)
5. Were you concerned about whether the
replacements would look similar to your
natural teeth?
Yes
Don’t remember
No
16 (36.4%)
2 (4.5%)
26 (59.1%)
6. In general, how do the replacements feel
compared to your natural teeth?
The same or almost the same
Different, but good enough
Completely different
34 (77.3%)
4 (9.1%)
6 (13.6%)
7. What is your opinion of the
replacements’ appearance?
Satisfied
Dissatisfied
42 (95.5%)
2 (4.5%)
8. Does the gum surrounding the
replacements bleed?
Yes
Unsure
No
9 (20.9%)
5 (11.6%)
29 (67.4%)
9. When brushing teeth, do you need to be
more meticulous around the replacements
compared to your natural teeth?
The same
It is more demanding
It is a lot of work
17 (38.6%)
25 (56.8%)
2 (4.5%)
10. When eating, do you chew in a similar
way with the replacements as with your
natural teeth?
Yes
Unsure
No
39 (88.6%)
3 (6.8%)
2 (4.5%)
11. Do the replacements feel similar to
your natural teeth?
Yes
Unsure
No
34 (77.3%)
4 (9.1%)
6 (13.6%)
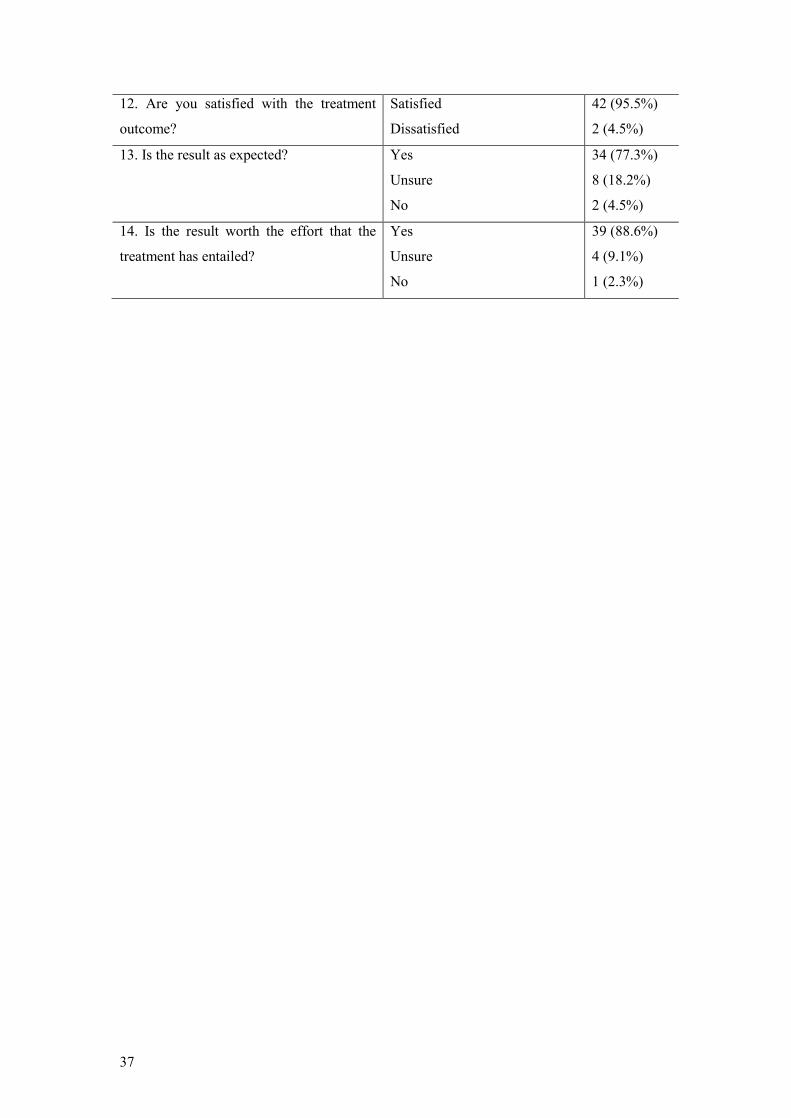
37
12. Are you satisfied with the treatment
outcome?
Satisfied
Dissatisfied
42 (95.5%)
2 (4.5%)
13. Is the result as expected? Yes
Unsure
No
34 (77.3%)
8 (18.2%)
2 (4.5%)
14. Is the result worth the effort that the
treatment has entailed?
Yes
Unsure
No
39 (88.6%)
4 (9.1%)
1 (2.3%)

38
Discussion This thesis deals with different issues related to the condition of congenitally missing teeth.
The studies (papers I-III) address the prognosis of persisting primary teeth, the psychosocial
impact caused by missing teeth, and the treatment outcome in patients with hypodontia. The
unpredictable and complex nature of the condition, the long treatment duration and the
relatively small sample of patients do not allow a randomised clinical trial design for
comparison of treatment alternatives. Paper I has a retrospective design, paper II is a cross-
sectional survey and paper III is a longitudinal follow-up study.
Study group and inclusion criteria The study group in paper I and III is based on 212 hypodontia patients referred to an
interdisciplinary team at the University of Oslo between 1998 and 2010. For paper I, 111
patients missing one or both mandibular second premolars with a corresponding persisting
primary molar and a panoramic radiograph of acceptable quality were included. Paper III was
based on the same study group, and only patients missing six or more teeth and aged 18 years
or more, 71 patients in total, were invited for a follow-up study. For paper II, patients referred
to the Department of Orthodontics, either to the specialist clinic or to the interdisciplinary
team, from January 2012 to September 2013 were consecutively recruited. Only patients with
a hypodontia diagnosis or a malocclusion with a similar normative treatment need (measured
by the index of orthodontic treatment need (IOTN), dental health component (DHC) of 4 or 5)
were included.
Evaluation of results
Persisting primary teeth without successors
The option of retaining primary teeth when successors are lacking might be viewed as a
temporary and uncertain alternative by professionals, as well as by patients and their
caregivers. Paper I showed that infraocclusion was the limiting prognostic factor for the
preservation of primary mandibular molars. This is particularly the case if it occurs before the
pubertal growth spurt. In cases where the number of missing teeth is limited to only a few,
other alternatives such as orthodontic space closure or insertion of a single implant after
cessation of growth is often more suitable. However, in growing individuals with a large
number of missing teeth, the primary teeth are an invaluable resource that artificial substitutes
cannot match in a biological perspective. Persisting primary teeth preserve the alveolar bone
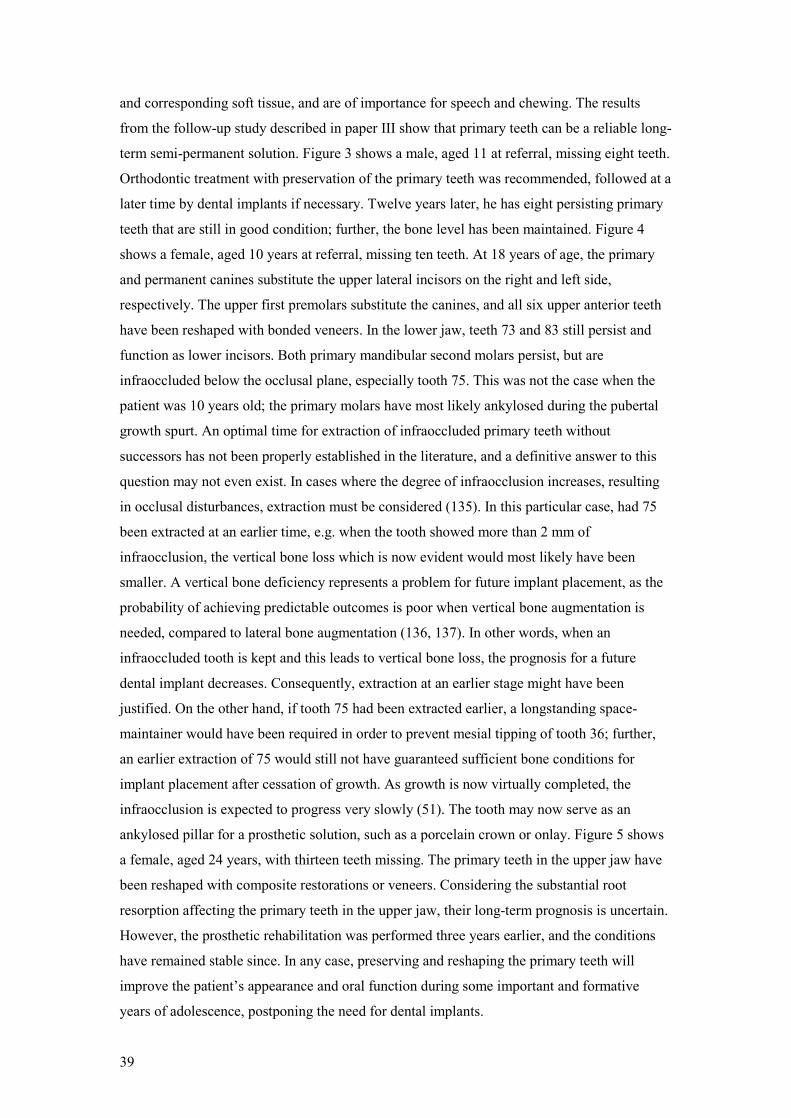
39
and corresponding soft tissue, and are of importance for speech and chewing. The results
from the follow-up study described in paper III show that primary teeth can be a reliable long-
term semi-permanent solution. Figure 3 shows a male, aged 11 at referral, missing eight teeth.
Orthodontic treatment with preservation of the primary teeth was recommended, followed at a
later time by dental implants if necessary. Twelve years later, he has eight persisting primary
teeth that are still in good condition; further, the bone level has been maintained. Figure 4
shows a female, aged 10 years at referral, missing ten teeth. At 18 years of age, the primary
and permanent canines substitute the upper lateral incisors on the right and left side,
respectively. The upper first premolars substitute the canines, and all six upper anterior teeth
have been reshaped with bonded veneers. In the lower jaw, teeth 73 and 83 still persist and
function as lower incisors. Both primary mandibular second molars persist, but are
infraoccluded below the occlusal plane, especially tooth 75. This was not the case when the
patient was 10 years old; the primary molars have most likely ankylosed during the pubertal
growth spurt. An optimal time for extraction of infraoccluded primary teeth without
successors has not been properly established in the literature, and a definitive answer to this
question may not even exist. In cases where the degree of infraocclusion increases, resulting
in occlusal disturbances, extraction must be considered (135). In this particular case, had 75
been extracted at an earlier time, e.g. when the tooth showed more than 2 mm of
infraocclusion, the vertical bone loss which is now evident would most likely have been
smaller. A vertical bone deficiency represents a problem for future implant placement, as the
probability of achieving predictable outcomes is poor when vertical bone augmentation is
needed, compared to lateral bone augmentation (136, 137). In other words, when an
infraoccluded tooth is kept and this leads to vertical bone loss, the prognosis for a future
dental implant decreases. Consequently, extraction at an earlier stage might have been
justified. On the other hand, if tooth 75 had been extracted earlier, a longstanding space-
maintainer would have been required in order to prevent mesial tipping of tooth 36; further,
an earlier extraction of 75 would still not have guaranteed sufficient bone conditions for
implant placement after cessation of growth. As growth is now virtually completed, the
infraocclusion is expected to progress very slowly (51). The tooth may now serve as an
ankylosed pillar for a prosthetic solution, such as a porcelain crown or onlay. Figure 5 shows
a female, aged 24 years, with thirteen teeth missing. The primary teeth in the upper jaw have
been reshaped with composite restorations or veneers. Considering the substantial root
resorption affecting the primary teeth in the upper jaw, their long-term prognosis is uncertain.
However, the prosthetic rehabilitation was performed three years earlier, and the conditions
have remained stable since. In any case, preserving and reshaping the primary teeth will
improve the patient’s appearance and oral function during some important and formative
years of adolescence, postponing the need for dental implants.
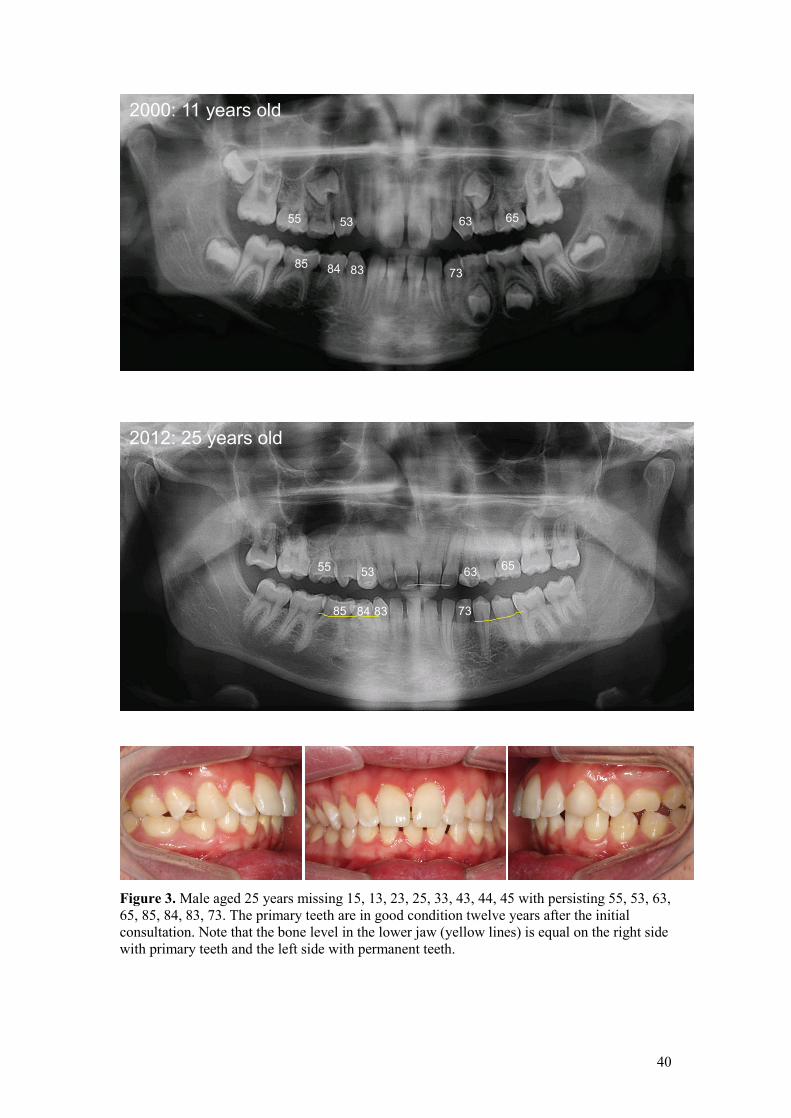
40
Figure 3. Male aged 25 years missing 15, 13, 23, 25, 33, 43, 44, 45 with persisting 55, 53, 63, 65, 85, 84, 83, 73. The primary teeth are in good condition twelve years after the initial consultation. Note that the bone level in the lower jaw (yellow lines) is equal on the right side with primary teeth and the left side with permanent teeth.
55 53 63 65
73 83 84 85
2000: 11 years old
2012: 25 years old
55 53 63 65
73 83 84 85

41
Figure 4. Female aged 18 years missing 15, 13, 12, 22, 35, 34, 31, 41, 44, 45 with persisting 55, 53, 75, 73, 83, 85. The roots of the primary teeth have shortened since first consultation ten years ago, but the teeth are in occlusion and in function, except for the ankylosed primary molars 75 and 85.
2006: 10 years old
55 53
75 85 73 83
2014: 18 years old
55 53
75 73 83 85
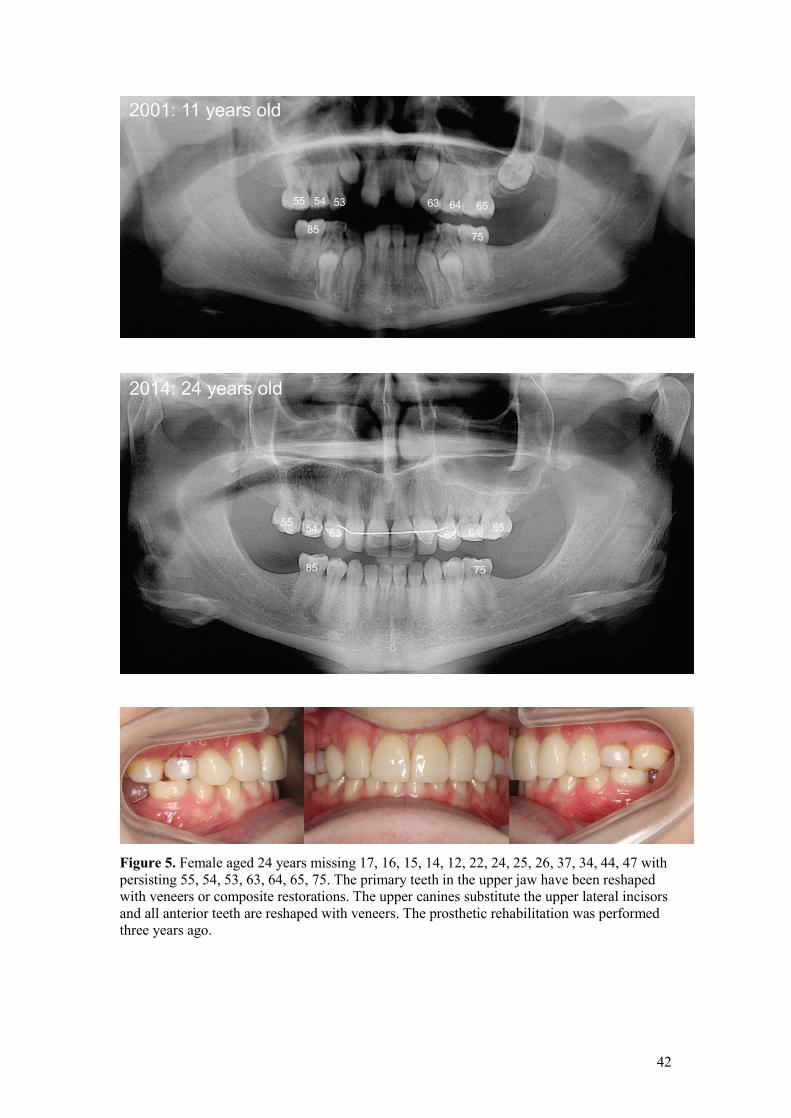
42
Figure 5. Female aged 24 years missing 17, 16, 15, 14, 12, 22, 24, 25, 26, 37, 34, 44, 47 with persisting 55, 54, 53, 63, 64, 65, 75. The primary teeth in the upper jaw have been reshaped with veneers or composite restorations. The upper canines substitute the upper lateral incisors and all anterior teeth are reshaped with veneers. The prosthetic rehabilitation was performed three years ago.
2001: 11 years old
55 54 53 63 64 65
75 85
2014: 24 years old
55 54 53 63 64 65
75 85

43
Mental health and social aspects related to hypodontia
Patients missing a large number of teeth not only struggle with functional problems, but
might also receive negative comments about their appearance from peers, and in some cases
experience bullying. Bullying has been described as a situation in which a person is exposed
repeatedly and over time to negative actions by at least one other person (138). The
prevalence of bullying among children and adolescents was examined in 11 European
countries, with 20.6% reporting being bullied, ranging from 10.5% in Hungary to 29.6% in
the United Kingdom (139). A study examining the prevalence of bullying, its effect on school
attendance and the contribution of general physical and dentofacial features was performed
among Jordanian schoolchildren (140). The prevalence of bullying among 11- to 12-year old
schoolchildren was 47%, and more boys reported being bullied than girls. Teeth were the
feature most frequently targeted, and the three most commonly reported dentofacial features
targeted by bullies were spacing between teeth or missing teeth, shape or colour of the teeth,
and prominent maxillary anterior teeth. A British study (141) examined 531 schoolchildren
between 9 and 13 years, and found that 66% were teased about one or more characteristics.
Height and weight were the commonest targets for teasing, dental features the fourth
commonest, and 7% of the children reported to be teased about their teeth once per week or
more. In comparison, the prevalence of peer victimization was found to be 12.8% in a group
of 10-14-year-olds awaiting orthodontic treatment (142). Adolescents who are bullied
because of a malocclusion or their dentofacial features experience a general impact on their
OHRQoL, including more pronounced oral symptoms and functional limitations, as well as
emotional and social effects (142, 143). Dentofacial appearance can affect interpersonal
relationships and perceived qualities such as friendliness, social class, intelligence, and
popularity, from infancy to adulthood (82). For young people with hypodontia, it is especially
distressing that their malocclusion is not just a phase in the mixed dentition or early
permanent dentition, which can be solved in the teenage years. Instead, the condition entails a
lifelong treatment need, and can never be considered fully treated.
The findings from paper II show that a malocclusion and congenitally missing teeth have an
almost equal negative impact on quality of life. The hypodontia patients reported more
problems with emotional status, and patients with upper anterior hypodontia were more
affected than those with a malocclusion of similar treatment need. Both groups scored
significantly worse than the general Norwegian population: 64% in the hypodontia group and
62% in the malocclusion group reported oral impacts, as compared to 18% of the general
population (64). Paper II also showed that the impacts reported by the hypodontia patients
were directly related to the missing teeth, and not to a co-existing malocclusion, since the
condition specific measure discriminated much better between the groups than the generic

44
measure. Gaps between teeth and small teeth might be regarded as unattractive, leading to
reluctance to interact socially. In some cases, the condition may exacerbate self-
consciousness and prevent young people from expressing themselves the way they would
otherwise have done, e.g. by smiling, talking and laughing. As an ultimate consequence, the
condition might lead to isolation and academic underachievement. This underlines the
importance of remedying the issues caused by missing teeth at least in the early teens, with
emphasis on making the anterior segment as attractive as possible.
The hypodontia patients examined in paper II were relatively young at the time of
investigation with a mean age of 13.6 years, had little treatment experience and may not yet
have understood the extent of treatment needed. The treatment of hypodontia patients is often
undertaken in phases, and some procedures, such as dental implants, are usually conducted
when the patients are over 20 years of age. The Norwegian public dental health service
provides all services except orthodontics free of charge until the age of 18; from 19 to 20
years, the patients pay 25% of the treatment cost. Persons above the age of 20 years are no
longer eligible for public dental health care, but treatment costs for certain defined conditions
are partly covered by the national insurance scheme. As treatment plans for patients with
severe hypodontia usually extend into adulthood, the financing situation may lead to
uncertainty at the planning stage as to whether the part of the treatment plan extending after
the age of 20 will actually come to execution. Experience from this work suggests that
patients with severe hypodontia should be offered dental treatment free of charge conducted
and coordinated by interdisciplinary teams, which continue to accumulate experience with
this patient group.
Treatment alternatives in individuals with multiple missing teeth
Methods to replace teeth in individuals with multiple missing teeth involve dental implants,
tooth-supported fixed dental prostheses, partial dentures and orthodontic space closure.
Dental implants
The literature on treatment outcome for patients with severe hypodontia has focused mostly
on dental implant treatment (130). The systematic review by Filius et al. (130) regarding
treatment outcome in patients with severe hypodontia revealed an implant survival rate from
35.7% to 98.7% (mean 94%). A systematic review by Pjetursson et al. (144) investigated
survival rates for implant-supported prostheses in the general population, and compared the
rates in studies published before the year 2000 to rates in studies published after year the
2000. The 5-year overall survival rate increased from 93.5% to 97.1%, and lower
complication rates were reported in the more recent clinical studies. The incidence of

45
aesthetic, biologic, and technical complications were, however, still high. The lower implant
survival rate in hypodontia patients compared to the general population may be associated
with the bone quality. The jawbone density in patients with ectodermal dysplasia is higher
than in healthy individuals, possibly impairing the prognosis for dental implants in this patient
group (145, 146). Such an association has not been demonstrated in patients with severe
hypodontia, as no radiographic difference in the structure of mandibular trabecular bone
could be found between hypodontia patients without ectodermal dysplasia and healthy
subjects in a study by Creton et al. (147). Other factors, such as location and amount of
available bone, might explain the higher loss of implants in patients with severe hypodontia
(130).
Paper III did not assess the survival of dental implants, biological variables such as pocket
depth, bleeding on probing, plaque index etc., or the marginal bone level on radiographs. Part
of the reason for this was that records from the time of treatment were often incomplete, and
many patients were not treated at the University clinic, but by local dentists with different
practices with regard to clinical documentation. Instead, the paper attempted to describe what
the patients actually looked like several years after treatment. The patients were a
heterogeneous group, and had undergone numerous interventions over many years; the
majority expressed tiredness from treatment. Dental implants in the anterior mandible showed
gingival discoloration in almost all subjects, with four different cases exemplified in Figure 6.
Dueled et al. (148) had similar observations, finding discoloration surrounding dental
implants in almost 60% of a group of hypodontia patients. The patients in paper III had a
mean age of 25.6 years at the follow-up examination, and the prosthetic rehabilitation was
performed on average 4.6 years earlier. The extent of the gingival discoloration and/or visible
metal after such a short observation period indicates that the anterior mandible provides
anatomical and biological limitations for implant insertion. Treatment alternatives that
preserve the alveolar process, such as retaining primary teeth, orthodontic space closure or
autotransplantation, are certainly preferable if the alveolar process is narrow; this is usually
the case when teeth are not present. Alternatively, based on the findings from paper III, a
tooth-supported fixed dental prosthesis (FDP) in the anterior mandible will probably serve as
a better solution than an implant-based solution.
Fixed dental prostheses
The replacement of congenitally missing teeth by an FDP has not been thoroughly discussed
in the literature. Dueled et al. (148) compared the aesthetic outcome of FDPs and dental
implants in patients with tooth agenesis, and found acceptable aesthetics in 92% of the
implant reconstructions and 83% of the FDPs. Replacing teeth with a conventional full-

46
coverage FDP is the least conservative approach, as extensive tooth reduction is usually
required, leading to a risk of pulpal trauma in young patients. If the conditions are favourable,
or rendered favourable by pre-prosthetic orthodontics, minimally invasive techniques using
resin-bonded FDPs are preferable. The findings from paper III showed that the crown
morphology was better for FDPs than for implant fixtures. A possible explanation for this
might be that there are fewer biological limitations to take into account when designing an
FDP, namely the bone level and corresponding soft tissue. An FDP has two pillar teeth
defining its design, whereas if an implant is placed in an area of deficient or little bone, the
crown morphology must be designed so that it compensates for this to some extent.
A viable alternative for the replacement of single missing teeth is a single-retained resin-
bonded prosthesis. In recent literature, the reported survival rates (94.4% to 100% after 4 to
10 years of follow-up (110-113)) for these have been promising, and this option should
therefore be regarded as a long-term semi-permanent or permanent alternative. Experience
from patients in this work supports this view, as the aesthetics are satisfactory, the durability
is good and minimal grinding of neighbouring teeth is required. Figure 7 shows a female,
aged 22 years with nine teeth missing. Two single-retained resin bonded prosthesis have
replaced 12 and 41 respectively, with a pleasing aesthetical and functional result.
Removable partial dentures
None of the 50 investigated patients in paper III had been recommended a removable partial
denture (RPD) or received one as a permanent option. Some of the patients reported to have
used one during an intermediate phase before receiving permanent replacements. A few
studies have described the use of RPDs in patients with severe hypodontia or ectodermal
dysplasia. In 1989, RPDs were frequently used in the treatment of severe hypodontia, as
reported by Hobkirk et al. (149). The dentures had a relatively short lifespan, and needed to
be replaced within 3.5–4 years in the maxilla on average. Reasons for replacement were
dissatisfaction with the appearance of the prosthesis, fracture, wear or oral changes. Lexner et
al. (150) investigated ten males affected with X-linked hypohidrotic ectodermal dysplasia
who were treated with removable prostheses. In 7 out of 10, the treatment was a success
according to the patient, their parents and the dentist. The prostheses had to be re-made
regularly due to eruption of teeth or growth of the mandible.
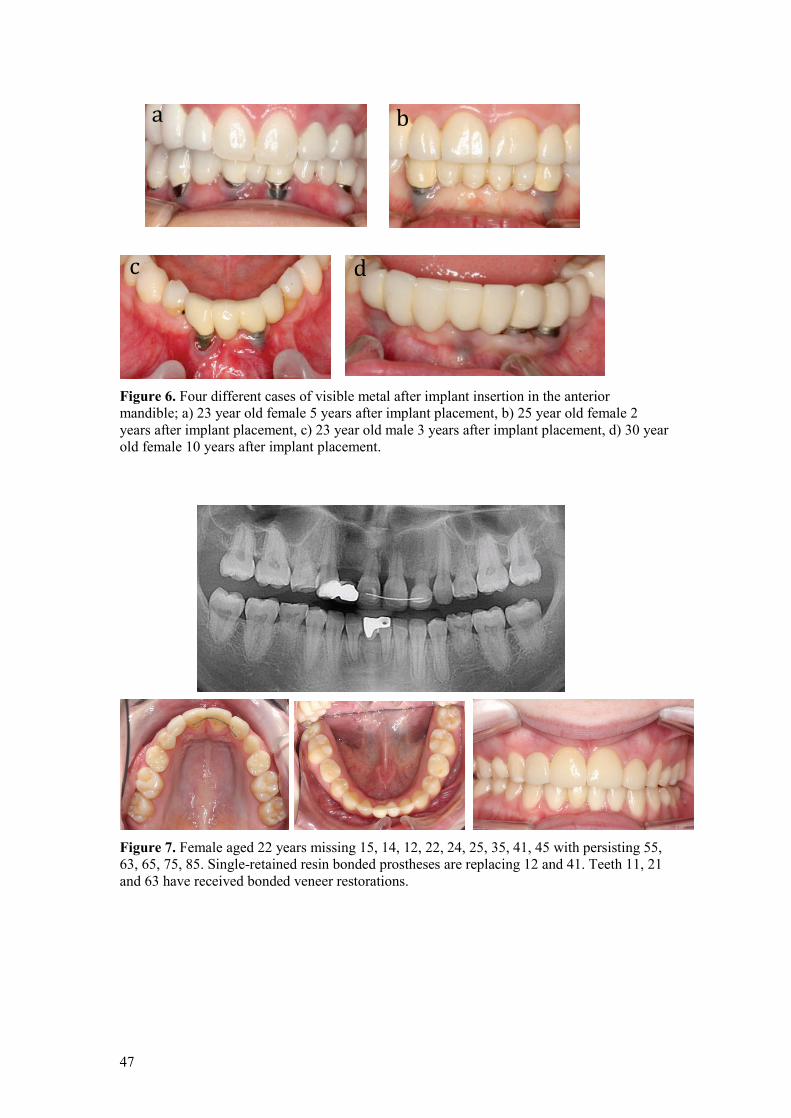
47
Figure 6. Four different cases of visible metal after implant insertion in the anterior mandible; a) 23 year old female 5 years after implant placement, b) 25 year old female 2 years after implant placement, c) 23 year old male 3 years after implant placement, d) 30 year old female 10 years after implant placement.
Figure 7. Female aged 22 years missing 15, 14, 12, 22, 24, 25, 35, 41, 45 with persisting 55, 63, 65, 75, 85. Single-retained resin bonded prostheses are replacing 12 and 41. Teeth 11, 21 and 63 have received bonded veneer restorations.
a b
c d

48
Orthodontic treatment
Orthodontic treatment is usually unavoidable for the majority of hypodontia patients. Most
patients require an increase in the vertical dimensions of the jaw, a more favourable
distribution of developed teeth and, if possible, to close gaps after missing teeth. Paper III
showed that out of the 571 teeth that were missing among the 50 investigated subjects, 111
were substituted by orthodontic space closure. The literature regarding orthodontic space
closure in hypodontia patients has mainly focused on closing spaces due to congenitally
missing maxillary lateral incisors or premolars; the success of space closure has often been
compared to dental implant treatment. Space closure with canine substitution in cases of
missing lateral incisors is associated with aesthetic challenges such as the large canine
dimensions, the darker and more yellow colour of the canine and the gingival height (151).
Other disadvantages are the tendency for relapse, usually requiring long-term retention, and
the lack of a canine-protected occlusion. However, no significant difference in the prevalence
of temporomandibular disorders was found between patients treated with space closure or
prosthetic replacement (152). Insertion of dental implants usually involves an initial phase of
orthodontic treatment to upright and parallel the adjacent teeth, and to gain sufficient space in
the mesio-distal dimension (151). A few studies have shown that orthodontic space opening
prior to implant insertion leads to reduction of the alveolar ridge dimension (153-155), and
one author argued that space opening before the age of 13 led to the least amount of alveolar
ridge reduction (155). Some negative observations have been reported for the implant
technique, such as infra-position of the implant-supported crown, even when growth and
dental development is complete, due to continuous eruption of the adjacent teeth (126),
resulting in apical displacement of the soft-tissue margin. Mucosal recession, reduction of the
buccal bone wall, thread exposure and reduction of the marginal bone level of the adjacent
teeth have also been reported (96, 151). A review by Kiliaridis et al. (96) of treatment options
for missing lateral incisors showed that both space closure and implants have their advantages
as well as disadvantages, but that in cases where both therapeutic options are indicated,
orthodontic space closure is more preferable than space opening, due to superior periodontal
health and aesthetic outcome. In addition, early completion of the definitive treatment and
absence of long-term biological and technical complications are aspects in favour of
orthodontic space closure (96). A study by De-Marchi et al. (156) assessed smile
attractiveness in patients with missing lateral incisors treated with either space opening
followed by implant placement, or space closure followed by teeth recontouring, in addition
to a control group with a complete dentition. Smile attractiveness was rated by laypersons,
dentists and the patients themselves. The smiles of patients with maxillary lateral incisor
agenesis were judged to be as attractive as those of the controls. All participants had high
levels of satisfaction with their own smile; patients treated with space closure were the most

49
satisfied. These results indicate that both treatments are capable of achieving aesthetic results
similar to an intact dentition. A very recent and similar study by Schneider et al. (157)
concluded that orthodontists and dentists rank implant treatment and space closure as equally
aesthetically pleasing, whereas laypersons prefer space closure.
Treatment outcome from the patients’ perspective
Previously unpublished data on patients’ own evaluation of treatment outcome are listed in
the result section. The patients are the same as those included in paper III. The preceding
discussion has mainly dealt with objective evaluations of different treatment options.
However, in line with a patient-centred philosophy, self-reported satisfaction must be
considered an equally important indicator as objective measures of treatment outcome. The
patient is, after all, the supreme judge of whether the treatment is to be considered a success.
The patients from paper III were in surprising agreement, with 95.5% reporting satisfaction
with the treatment outcome. We were unable to distinguish whether there was any difference
in satisfaction between the groups that had received different treatment alternatives. The
reason for this was twofold: almost all patients were satisfied, and each patient had gone
through many different procedures. Only a very few had undergone a single means of
treatment (e.g. solely implant treatment or orthodontic space closure) to replace missing teeth.
The majority of the patients, 77.3% and 88.6% respectively, reported that the replacement
teeth felt similar to the natural teeth, and that chewing with the replacement teeth was similar
to the natural teeth. As all patients had received several replacements, these results indicate a
reasonable good acceptance of the artificial teeth as substitutes for their natural teeth.
However, 61.3% found it more demanding or a lot of work to maintain hygiene around the
replacement teeth.
High patient satisfaction has also been found in other studies where teeth have been replaced.
In a study of treatment outcome in hypodontia patients, Dueled et al. (148) reported that 98 %
of the patients treated with dental implants and 84% of the patients treated with FDP were
satisfied. Czochrowska et al. reported high patient satisfaction after tooth transplantation
(106) and space closure of a missing maxillary central incisor (158).

50
Clinical implications
Standardisation, specialisation and the participation of high-volume operators have been
shown to result in favourable outcomes for patients with other conditions such as cleft lip and
palate (159). The development of such standards for patients with severe hypodontia would
be most welcome, but still remains a challenge. These patients form a heterogeneous group,
with large individual differences, and a clinical picture in constant change. There is also a
lack of evidence evaluating treatment outcome. In order to optimise treatment planning in this
group, early diagnosis and referral to an interdisciplinary team is crucial. Owing to the low
prevalence of severe hypodontia, a single clinician will encounter patients with this condition
only rarely. Interdisciplinary teams will serve to increase knowledge and experience with rare
conditions. They also contribute to information and support to the patient and family, offer a
thoroughly planned and co-ordinated treatment with high continuity, and the involved
specialists share responsibility for treatment decisions (88). The findings from this thesis
suggest that children who were referred early and recommended to preserve and take care of
their primary teeth were better off than those who were referred late. Early referral leaves all
treatment options available, whereas some options (e.g. autotransplantation or growth-
adaptive approaches) may have become unavailable if patients are referred late.
Results from this work show that tooth replacements can be made minimally invasive in
growing children, for example by using resin bonded prostheses attached to either permanent
or primary teeth, especially in the anterior region. This has proven to result in an aesthetically
pleasing result with good durability as a semi-permanent solution. In addition, such solutions
will ease the psychosocial burden for young patients. More invasive prosthetic interventions
such as conventional FDPs and implants may thereby be postponed for as long as possible.
The placement of dental implants in the anterior mandible, in these individuals with reduced
amounts of alveolar bone, should be considered inadvisable based on the results of the
follow-up study described in paper III, and all other means should be considered prior to
undertaking such therapy.
51
Conclusions
In accordance with the proposed aims, the following conclusions can be drawn:
Prognostic factors for retaining persisting primary mandibular molars
• Critical factors for the survival of a persisting primary molar without successor are
infraocclusion, root resorption and restorations. Clinically significant infraocclusion
was found in 43.6% of the patients, and was the most critical factor for the prognosis
of primary mandibular molars. This is particularly important for individuals who have
not yet completed the pubertal growth spurt.
Generic and condition-specific impacts in patients with hypodontia or a malocclusion
with similar treatment need
• Hypodontia and malocclusion patients reported a considerable burden of oral
impacts. The generic inventory did not discriminate between patients with and
without hypodontia, whereas the condition specific measure attributed to hypodontia
discriminated with statistical significance between the groups, and was related to
severity and upper anterior location of hypodontia. This indicates that the hypodontia
patients have psychosocial impacts directly related to their condition, and
consequently an objective need for treatment.
Tooth replacements in young adults with severe hypodontia
• Dental implants in the anterior region proved to be an inadequate treatment modality
in patients with severe hypodontia, with visible metal the most notable issue. Mucosal
discoloration was evident in the anterior mandible in almost all patients and, in the
anterior maxilla, in two thirds of the patients. Orthodontic space closure resulted in
superior papilla aesthetics, but had the drawback of a less optimal crown morphology
in the anterior mandible. Dental implants, orthodontic space closure, and retaining
primary teeth were the most commonly prescribed treatments. Persisting primary
teeth showed a good survival rate.
In conclusion, results from this thesis show that patients with severe hypodontia require a
comprehensive, interdisciplinary planning, as well as life-long treatment and follow-up. In
addition to understanding of the patients’ dental issues, a more profound comprehension of
their social and emotional struggles is also essential for the clinicians involved. Patient
satisfaction is very high after treatment regardless of replacement type; however,
professionals should be aware of biological limitations in different circumstances, and always

52
pursue the most appropriate and longest-lasting solutions possible for these young
individuals.

53
References 1. Khalaf K, Miskelly J, Voge E, Macfarlane TV. Prevalence of hypodontia and associated factors: a systematic review and meta-analysis. J Orthod. 2014;41:299-316.
2. Vastardis H. The genetics of human tooth agenesis: new discoveries for understanding dental anomalies. Am J Orthod Dentofacial Orthop. 2000;117:650-6.
3. Nunn JH, Carter NE, Gillgrass TJ, Hobson RS, Jepson NJ, Meechan JG, et al. The interdisciplinary management of hypodontia: background and role of paediatric dentistry. Br Dent J. 2003;194:245-51.
4. Schalk-van der Weide Y, Steen WH, Bosman F. Distribution of missing teeth and tooth morphology in patients with oligodontia. ASDC J Dent Child. 1992;59:133-40.
5. Hobkirk JA, Brook AH. The management of patients with severe hypodontia. J Oral Rehabil. 1980;7:289-98.
6. Haavikko K. Hypodontia of permanent teeth. An orthopantomographic study. Suom Hammaslaak Toim. 1971;67:219-25.
7. Grahnen H. Hypodontia in the permanent dentition. A clinical and genetical investigation. Odontol Revy. 1956;7:1-100.
8. Polder BJ, Van't Hof MA, Van der Linden FP, Kuijpers-Jagtman AM. A meta-analysis of the prevalence of dental agenesis of permanent teeth. Community Dent Oral Epidemiol. 2004;32:217-26.
9. Mattheeuws N, Dermaut L, Martens G. Has hypodontia increased in Caucasians during the 20th century? A meta-analysis. Eur J Orthod. 2004;26:99-103.
10. Wisth PJ, Thunold K, Boe OE. Frequency of hypodontia in relation to tooth size and dental arch width. Acta Odontol Scand. 1974;32:201-6.
11. Nordgarden H, Jensen JL, Storhaug K. Reported prevalence of congenitally missing teeth in two Norwegian counties. Community Dent Health. 2002;19:258-61.
12. Rolling S, Poulsen S. Oligodontia in Danish schoolchildren. Acta Odontol Scand. 2001;59:111-2.
13. Schalk-van der Weide Y. Oligodontia. A clinical, radiographic and genetic evaluation [Ph.D. thesis]. Utrecht: University of Utrecht; 1992.
14. Aasheim B, Ogaard B. Hypodontia in 9-year-old Norwegians related to need of orthodontic treatment. Scand J Dent Res. 1993;101:257-60.
15. Davis PJ. Hypodontia and hyperdontia of permanent teeth in Hong Kong schoolchildren. Community Dent Oral Epidemiol. 1987;15:218-20.
16. Arte S. Phenotypic and genotypic features of familial hypodontia [Ph.D. thesis]. Helsinki: University of Helsinki; 2001.
17. Yuksel S, Ucem T. The effect of tooth agenesis on dentofacial structures. Eur J Orthod. 1997;19:71-8.
54
18. Dermaut LR, Goeffers KR, De Smit AA. Prevalence of tooth agenesis correlated with jaw relationship and dental crowding. Am J Orthod Dentofacial Orthop. 1986;90:204-10.
19. Roald KL, Wisth PJ, Boe OE. Changes in cranio-facial morphology of individuals with hypodontia between the ages of 9 and 16. Acta Odontol Scand. 1982;40:65-74.
20. Wisth PJ, Thunold K, Boe OE. The craniofacial morphology of individuals with hypodontia. Acta Odontol Scand. 1974;32:281-90.
21. Sarnas KV, Rune B. The facial profile in advanced hypodontia: a mixed longitudinal study of 141 children. Eur J Orthod. 1983;5:133-43.
22. Woodworth DA, Sinclair PM, Alexander RG. Bilateral congenital absence of maxillary lateral incisors: a craniofacial and dental cast analysis. Am J Orthod. 1985;87:280-93.
23. Chung LK, Hobson RS, Nunn JH, Gordon PH, Carter NE. An analysis of the skeletal relationships in a group of young people with hypodontia. J Orthod. 2000;27:315-8.
24. Ogaard B, Krogstad O. Craniofacial structure and soft tissue profile in patients with severe hypodontia. Am J Orthod Dentofacial Orthop. 1995;108:472-7.
25. Brook AH. A unifying aetiological explanation for anomalies of human tooth number and size. Arch Oral Biol. 1984;29:373-8.
26. Brook AH, Griffin RC, Smith RN, Townsend GC, Kaur G, Davis GR, et al. Tooth size patterns in patients with hypodontia and supernumerary teeth. Arch Oral Biol. 2009;54 Suppl 1:S63-70.
27. Kjaer I. Can the location of tooth agenesis and the location of initial bone loss seen in juvenile periodontitis be explained by neural developmental fields in the jaws? Acta Odontol Scand. 1997;55:70-2.
28. Nasman M, Forsberg CM, Dahllof G. Long-term dental development in children after treatment for malignant disease. Eur J Orthod. 1997;19:151-9.
29. Tan SP, van Wijk AJ, Prahl-Andersen B. Severe hypodontia: identifying patterns of human tooth agenesis. Eur J Orthod. 2011;33:150-4.
30. Shimizu T, Maeda T. Prevalence and genetic basis for tooth agenesis. Japanese Dental Science Review. 2009;45:52-8.
31. Townsend GC, Richards L, Hughes T, Pinkerton S, Schwerdt W. Epigenetic influences may explain dental differences in monozygotic twin pairs. Aust Dent J. 2005;50:95-100.
32. Michon F. Tooth evolution and dental defects: from genetic regulation network to micro-RNA fine-tuning. Birth Defects Res A Clin Mol Teratol. 2011;91:763-9.
33. Dreesen K, Swinnen S, Devriendt K, Carels C. Tooth agenesis patterns and phenotype variation in a cohort of Belgian patients with hypodontia and oligodontia clustered in 79 families with their pedigrees. Eur J Orthod. 2014;36:99-106.
34. Baraitser M, Winter RM. The London dysmorphology database (LDDB). Oxford medical databases. Oxford: Oxford University Press; 1999.
55
35. Kadir A, Mossey PA, Blencowe H, Moorthie S, Lawn JE, Mastroiacovo P, et al. Systematic Review and Meta-analysis of the Birth Prevalence of Orofacial Clefts in Low- and Middle-Income Countries. Cleft Palate Craniofac J. 2016; doi: 10.1597/15-221 [Epub ahead of print].
36. Andersson EM, Sandvik L, Abyholm F, Semb G. Clefts of the secondary palate referred to the Oslo Cleft Team: epidemiology and cleft severity in 994 individuals. Cleft Palate Craniofac J. 2010;47:335-42.
37. Kurol J. Infraocclusion of primary molars: an epidemiologic and familial study. Community Dent Oral Epidemiol. 1981;9:94-102.
38. Kurol J, Thilander B. Infraocclusion of primary molars and the effect on occlusal development, a longitudinal study. Eur J Orthod. 1984;6:277-93.
39. Kurol J, Magnusson BC. Infraocclusion of primary molars: a histologic study. Scand J Dent Res. 1984;92:564-76.
40. Rygh P, Retain K. Changes in the supporting tissues of submerged deciduous molars with and without permanent successors. Eur Orthod Soc Tr. 1963;39:171-84.
41. Mancini G, Francini E, Vichi M, Tollaro I, Romagnoli P. Primary tooth ankylosis: report of case with histological analysis. ASDC J Dent Child. 1995;62:215-9.
42. Rincon JC, Young WG, Bartold PM. The epithelial cell rests of Malassez – a role in periodontal regeneration? J Periodontal Res. 2006;41:245-52.
43. Proffit WR, Vig KW. Primary failure of eruption: a possible cause of posterior open-bite. Am J Orthod. 1981;80:173-90.
44. Baccetti T. A controlled study of associated dental anomalies. Angle Orthod. 1998;68:267-74.
45. Kurol J, Thilander B. Infraocclusion of primary molars with aplasia of the permanent successor. A longitudinal study. Angle Orthod. 1984;54:283-94.
46. Lai PY, Seow WK. A controlled study of the association of various dental anomalies with hypodontia of permanent teeth. Pediatr Dent. 1989;11:291-6.
47. Bjerklin K, Al-Najjar M, Karestedt H, Andren A. Agenesis of mandibular second premolars with retained primary molars: a longitudinal radiographic study of 99 subjects from 12 years of age to adulthood. Eur J Orthod. 2008;30:254-61.
48. Rune B, Sarnas KV. Root resorption and submergence in retained deciduous second molars. A mixed-longitudinal study of 77 children with developmental absence of second premolars. Eur J Orthod. 1984;6:123-31.
49. Sletten DW, Smith BM, Southard KA, Casko JS, Southard TE. Retained deciduous mandibular molars in adults: a radiographic study of long-term changes. Am J Orthod Dentofacial Orthop. 2003;124:625-30.
50. Haselden K, Hobkirk JA, Goodman JR, Jones SP, Hemmings KW. Root resorption in retained deciduous canine and molar teeth without permanent successors in patients with severe hypodontia. Int J Paediatr Dent. 2001;11:171-8.
56
51. Ith-Hansen K, Kjaer I. Persistence of deciduous molars in subjects with agenesis of the second premolars. Eur J Orthod. 2000;22:239-43.
52. Nordquist I, Lennartsson B, Paulander J. Primary teeth in adults – a pilot study. Swed Dent J. 2005;29:27-34.
53. Locker D, Allen F. What do measures of 'oral health-related quality of life' measure? Community Dent Oral Epidemiol. 2007;35:401-11.
54. Locker D. Measuring oral health: a conceptual framework. Community Dent Health. 1988;5:3-18.
55. Tsakos G, Allen PF, Steele JG, Locker D. Interpreting oral health-related quality of life data. Community Dent Oral Epidemiol. 2012;40:193-200.
56. Buck D, Newton JT. Non-clinical outcome measures in dentistry: publishing trends 1988-98. Community Dent Oral Epidemiol. 2001;29:2-8.
57. Engel GL. The need for a new medical model: a challenge for biomedicine. Science. 1977;196:129-36.
58. Carr AJ, Gibson B, Robinson PG. Measuring quality of life: Is quality of life determined by expectations or experience? BMJ. 2001;322:1240-3.
59. Strassburger C, Heydecke G, Kerschbaum T. Influence of prosthetic and implant therapy on satisfaction and quality of life: a systematic literature review. Part 1– Characteristics of the studies. Int J Prosthodont. 2004;17:83-93.
60. Adulyanon S, Sheiham A. Oral impacts on daily performances. In: Slade GD, editor. Measuring Oral Health and Quality of Life. Chapel Hill University of North Carolina, Dental Ecology; 1997. p. 152-60.
61. Cortes MI, Marcenes W, Sheiham A. Impact of traumatic injuries to the permanent teeth on the oral health-related quality of life in 12-14-year-old children. Community Dent Oral Epidemiol. 2002;30:193-8.
62. de Oliveira CM, Sheiham A. The relationship between normative orthodontic treatment need and oral health-related quality of life. Community Dent Oral Epidemiol. 2003;31:426-36.
63. World Health Organization. International classification of impairments, disabilities and handicaps: a manual of classification. Geneva: 1980.
64. Astrom AN, Haugejorden O, Skaret E, Trovik TA, Klock KS. Oral Impacts on Daily Performance in Norwegian adults: validity, reliability and prevalence estimates. Eur J Oral Sci. 2005;113:289-96.
65. Cunningham SJ, Hunt NP. Quality of life and its importance in orthodontics. J Orthod. 2001;28:152-8.
66. Guyatt GH, Feeny DH, Patrick DL. Measuring health-related quality of life. Ann Intern Med. 1993;118:622-9.
57
67. Bernabe E, Tsakos G, Messias de Oliveira C, Sheiham A. Impacts on daily performances attributed to malocclusions using the condition-specific feature of the Oral Impacts on Daily Performances Index. Angle Orthod. 2008;78:241-7.
68. Gherunpong S, Tsakos G, Sheiham A. A sociodental approach to assessing dental needs of children: concept and models. Int J Paediatr Dent. 2006;16:81-8.
69. Gilchrist F, Rodd H, Deery C, Marshman Z. Assessment of the quality of measures of child oral health-related quality of life. BMC Oral Health. 2014;14:40.
70. Jokovic A, Locker D, Guyatt G. Short forms of the Child Perceptions Questionnaire for 11-14-year-old children (CPQ11-14): development and initial evaluation. Health Qual Life Outcomes. 2006;4:4.
71. Slade GD, Spencer AJ. Development and evaluation of the Oral Health Impact Profile. Community Dent Health. 1994;11:3-11.
72. Slade GD. Derivation and validation of a short-form oral health impact profile. Community Dent Oral Epidemiol. 1997;25:284-90.
73. Robinson PG, Gibson B, Khan FA, Birnbaum W. Validity of two oral health-related quality of life measures. Community Dent Oral Epidemiol. 2003;31:90-9.
74. Holst D, Dahl KE. Oral health related quality of life. A national, descriptive survey. Nor Tannlegeforen Tid. 2008;118:212-18.
75. Akram AJ, Jerreat AS, Woodford J, Sandy JR, Ireland AJ. Development of a condition-specific measure to assess quality of life in patients with hypodontia. Orthod Craniofac Res. 2011;14:160-7.
76. Akram AJ, Ireland AJ, Postlethwaite KC, Sandy JR, Jerreat AS. Assessment of a condition-specific quality-of-life measure for patients with developmentally absent teeth: validity and reliability testing. Orthod Craniofac Res. 2013;16:193-201.
77. Patel N, Hodges SJ, Hall M, Benson PE, Marshman Z, Cunningham SJ. Development of the Malocclusion Impact Questionnaire (MIQ) to measure the oral health-related quality of life of young people with malocclusion: part 1 – qualitative inquiry. J Orthod. 2016;43:7-13.
78. Benson PE, Cunningham SJ, Shah N, Gilchrist F, Baker SR, Hodges SJ, et al. Development of the Malocclusion Impact Questionnaire (MIQ) to measure the oral health-related quality of life of young people with malocclusion: part 2 – cross-sectional validation. J Orthod. 2016;43:14-23.
79. Cunningham SJ, Garratt AM, Hunt NP. Development of a condition-specific quality of life measure for patients with dentofacial deformity: I. Reliability of the instrument. Community Dent Oral Epidemiol. 2000;28:195-201.
80. Anweigi L, Allen PF, Ziada H. The use of the Oral Health Impact Profile to measure the impact of mild, moderate and severe hypodontia on oral health-related quality of life in young adults. J Oral Rehabil. 2013;40:603-8.
81. Wong AT, McMillan AS, McGrath C. Oral health-related quality of life and severe hypodontia. J Oral Rehabil. 2006;33:869-73.

58
82. Laing E, Cunningham SJ, Jones S, Moles D, Gill D. Psychosocial impact of hypodontia in children. Am J Orthod Dentofacial Orthop. 2010;137:35-41.
83. Kotecha S, Turner PJ, Dietrich T, Dhopatkar A. The impact of tooth agenesis on oral health-related quality of life in children. J Orthod. 2013;40:122-9.
84. Locker D, Jokovic A, Prakash P, Tompson B. Oral health-related quality of life of children with oligodontia. Int J Paediatr Dent. 2010;20:8-14.
85. Anweigi L, Finbarr Allen P, Ziada H. Impact of resin bonded bridgework on quality of life of patients with hypodontia. J Dent. 2013;41:683-8.
86. Allen PF, Lee S, Brady P. Clinical and subjective evaluation of implants in patients with hypodontia: a two-year observation study. Clin Oral Implants Res. 2016; doi: 10.1111/clr.12951 [Epub ahead of print].
87. Koch G, Poulsen S. Pediatric dentistry – a clinical approach. Copenhagen: Munksgaard; 2001.
88. Bergendal B, Bergendal T, Hallonsten AL, Koch G, Kurol J, Kvint S. A multidisciplinary approach to oral rehabilitation with osseointegrated implants in children and adolescents with multiple aplasia. Eur J Orthod. 1996;18:119-29.
89. Worsaae N, Jensen BN, Holm B, Holsko J. Treatment of severe hypodontia-oligodontia – an interdisciplinary concept. Int J Oral Maxillofac Surg. 2007;36:473-80.
90. Ostler MS, Kokich VG. Alveolar ridge changes in patients congenitally missing mandibular second premolars. J Prosthet Dent. 1994;71:144-9.
91. Bergendal B. When should we extract deciduous teeth and place implants in young individuals with tooth agenesis? J Oral Rehabil. 2008;35 Suppl 1:55-63.
92. Lindqvist B. Extraction of the deciduous second molar in hypodontia. Eur J Orthod. 1980;2:173-81.
93. Mamopoulou A, Hagg U, Schroder U, Hansen K. Agenesis of mandibular second premolars. Spontaneous space closure after extraction therapy: a 4-year follow-up. Eur J Orthod. 1996;18:589-600.
94. Bjork A, Skieller V. Facial development and tooth eruption. An implant study at the age of puberty. Am J Orthod. 1972;62:339-83.
95. Bjork A, Skieller V. Normal and abnormal growth of the mandible. A synthesis of longitudinal cephalometric implant studies over a period of 25 years. Eur J Orthod. 1983;5:1-46.
96. Kiliaridis S, Sidira M, Kirmanidou Y, Michalakis K. Treatment options for congenitally missing lateral incisors. Eur J Oral Implantol. 2016;9:5-24.
97. Zachrisson BU, Rosa M, Toreskog S. Congenitally missing maxillary lateral incisors: canine substitution. Point. Am J Orthod Dentofacial Orthop. 2011;139:434, 6, 8 passim.
98. Rosa M, Zachrisson BU. Integrating esthetic dentistry and space closure in patients with missing maxillary lateral incisors. J Clin Orthod. 2001;35:221-34.

59
99. Tuverson DL. Orthodontic treatment using canines in place of missing maxillary lateral incisors. Am J Orthod. 1970;58:109-27.
100. Thordarson A, Zachrisson BU, Mjor IA. Remodeling of canines to the shape of lateral incisors by grinding: a long-term clinical and radiographic evaluation. Am J Orthod Dentofacial Orthop. 1991;100:123-32.
101. Nordquist GG, McNeill RW. Orthodontic vs. restorative treatment of the congenitally absent lateral incisor – long term periodontal and occlusal evaluation. J Periodontol. 1975;46:139-43.
102. Kokich VO, Jr., Kinzer GA. Managing congenitally missing lateral incisors. Part I: Canine substitution. J Esthet Restor Dent. 2005;17:5-10.
103. Levander E, Malmgren O, Stenback K. Apical root resorption during orthodontic treatment of patients with multiple aplasia: a study of maxillary incisors. Eur J Orthod. 1998;20:427-34.
104. Machado LA, do Nascimento RR, Ferreira DM, Mattos CT, Vilella OV. Long-term prognosis of tooth autotransplantation: a systematic review and meta-analysis. Int J Oral Maxillofac Surg. 2016;45:610-7.
105. Czochrowska EM, Stenvik A, Album B, Zachrisson BU. Autotransplantation of premolars to replace maxillary incisors: a comparison with natural incisors. Am J Orthod Dentofacial Orthop. 2000;118:592-600.
106. Czochrowska EM, Stenvik A, Bjercke B, Zachrisson BU. Outcome of tooth transplantation: survival and success rates 17-41 years posttreatment. Am J Orthod Dentofacial Orthop. 2002;121:110-9.
107. Czochrowska EM. Management of missing teeth in growing indivuduals: Tooth transplantation and orthodontic space closure. A synopsis [Ph.D. thesis]. Oslo: University of Oslo; 2003.
108. Durey K, Cook P, Chan M. The management of severe hypodontia. Part 1: Considerations and conventional restorative options. Br Dent J. 2014;216:25-9.
109. Sailer I, Pjetursson BE, Zwahlen M, Hammerle CH. A systematic review of the survival and complication rates of all-ceramic and metal-ceramic reconstructions after an observation period of at least 3 years. Part II: Fixed dental prostheses. Clin Oral Implants Res. 2007;18 Suppl 3:86-96.
110. Sailer I, Bonani T, Brodbeck U, Hammerle CH. Retrospective clinical study of single-retainer cantilever anterior and posterior glass-ceramic resin-bonded fixed dental prostheses at a mean follow-up of 6 years. Int J Prosthodont. 2013;26:443-50.
111. Sailer I, Hammerle CH. Zirconia ceramic single-retainer resin-bonded fixed dental prostheses (RBFDPs) after 4 years of clinical service: a retrospective clinical and volumetric study. Int J Periodontics Restorative Dent. 2014;34:333-43.
112. Kern M, Sasse M. Ten-year survival of anterior all-ceramic resin-bonded fixed dental prostheses. J Adhes Dent. 2011;13:407-10.
113. Sasse M, Kern M. Survival of anterior cantilevered all-ceramic resin-bonded fixed dental prostheses made from zirconia ceramic. J Dent. 2014;42:660-3.
60
114. Brånemark PI, Zarb GA, Albrecktsson T. Tissue-integrated prostheses. Osseointegration in clinical dentistry. Chicago: Quintessence Publishing; 1985.
115. Thilander B, Odman J, Grondahl K, Friberg B. Osseointegrated implants in adolescents. An alternative in replacing missing teeth? Eur J Orthod. 1994;16:84-95.
116. Thilander B, Odman J, Jemt T. Single implants in the upper incisor region and their relationship to the adjacent teeth. An 8-year follow-up study. Clin Oral Implants Res. 1999;10:346-55.
117. Odman J, Grondahl K, Lekholm U, Thilander B. The effect of osseointegrated implants on the dento-alveolar development. A clinical and radiographic study in growing pigs. Eur J Orthod. 1991;13:279-86.
118. Thilander B, Odman J, Grondahl K, Lekholm U. Aspects on osseointegrated implants inserted in growing jaws. A biometric and radiographic study in the young pig. Eur J Orthod. 1992;14:99-109.
119. Klineberg I, Cameron A, Hobkirk J, Bergendal B, Maniere MC, King N, et al. Rehabilitation of children with ectodermal dysplasia. Part 2: an international consensus meeting. Int J Oral Maxillofac Implants. 2013;28:1101-9.
120. Jemt T. Single implants in the anterior maxilla after 15 years of follow-up: comparison with central implants in the edentulous maxilla. Int J Prosthodont. 2008;21:400-8.
121. Scheller H, Urgell JP, Kultje C, Klineberg I, Goldberg PV, Stevenson-Moore P, et al. A 5-year multicenter study on implant-supported single crown restorations. Int J Oral Maxillofac Implants. 1998;13:212-8.
122. Polizzi G, Fabbro S, Furri M, Herrmann I, Squarzoni S. Clinical application of narrow Branemark System implants for single-tooth restorations. Int J Oral Maxillofac Implants. 1999;14:496-503.
123. Andersen E, Saxegaard E, Knutsen BM, Haanaes HR. A prospective clinical study evaluating the safety and effectiveness of narrow-diameter threaded implants in the anterior region of the maxilla. Int J Oral Maxillofac Implants. 2001;16:217-24.
124. Santing HJ, Raghoebar GM, Vissink A, den Hartog L, Meijer HJ. Performance of the Straumann Bone Level Implant system for anterior single-tooth replacements in augmented and nonaugmented sites: a prospective cohort study with 60 consecutive patients. Clin Oral Implants Res. 2013;24:941-8.
125. Zhao X, Qiao SC, Shi JY, Uemura N, Arai K, Lai HC. Evaluation of the clinical and aesthetic outcomes of Straumann (®) Standard Plus implants supported single crowns placed in non-augmented healed sites in the anterior maxilla: a 5-8 years retrospective study. Clin Oral Implants Res. 2016;27:106-12.
126. Thilander B, Odman J, Lekholm U. Orthodontic aspects of the use of oral implants in adolescents: a 10-year follow-up study. Eur J Orthod. 2001;23:715-31.
127. Bernard JP, Schatz JP, Christou P, Belser U, Kiliaridis S. Long-term vertical changes of the anterior maxillary teeth adjacent to single implants in young and mature adults. A retrospective study. J Clin Periodontol. 2004;31:1024-8.

61
128. Gallucci GO, Grutter L, Chuang SK, Belser UC. Dimensional changes of peri-implant soft tissue over 2 years with single-implant crowns in the anterior maxilla. J Clin Periodontol. 2011;38:293-9.
129. Cosyn J, Eghbali A, De Bruyn H, Dierens M, De Rouck T. Single implant treatment in healing versus healed sites of the anterior maxilla: an aesthetic evaluation. Clin Implant Dent Relat Res. 2012;14:517-26.
130. Filius MA, Cune MS, Raghoebar GM, Vissink A, Visser A. Prosthetic treatment outcome in patients with severe hypodontia: a systematic review. J Oral Rehabil. 2016;43:373-87.
131. Ekim SL, Hatibovic-Kofman S. A treatment decision-making model for infraoccluded primary molars. Int J Paediatr Dent. 2001;11:340-6.
132. Bjerklin K, Bennett J. The long-term survival of lower second primary molars in subjects with agenesis of the premolars. Eur J Orthod. 2000;22:245-55.
133. Jokovic A, Locker D, Stephens M, Kenny D, Tompson B, Guyatt G. Validity and reliability of a questionnaire for measuring child oral-health-related quality of life. J Dent Res. 2002;81:459-63.
134. Broder HL, McGrath C, Cisneros GJ. Questionnaire development: face validity and item impact testing of the Child Oral Health Impact Profile. Community Dent Oral Epidemiol. 2007;35 Suppl 1:8-19.
135. Kurol J. Infraocclusion of primary molars. An epidemiological, familial, longitudinal clinical and histological study. Swed Dent J Suppl. 1984;21:1-67.
136. Sanz-Sanchez I, Ortiz-Vigon A, Sanz-Martin I, Figuero E, Sanz M. Effectiveness of Lateral Bone Augmentation on the Alveolar Crest Dimension: A Systematic Review and Meta-analysis. J Dent Res. 2015;94:128-42s.
137. Rocchietta I, Fontana F, Simion M. Clinical outcomes of vertical bone augmentation to enable dental implant placement: a systematic review. J Clin Periodontol. 2008;35:203-15.
138. Olweus D. Bullying at school: basic facts and effects of a school based intervention program. J Child Psychol Psychiatry. 1994;35:1171-90.
139. Analitis F, Velderman MK, Ravens-Sieberer U, Detmar S, Erhart M, Herdman M, et al. Being bullied: associated factors in children and adolescents 8 to 18 years old in 11 European countries. Pediatrics. 2009;123:569-77.
140. Al-Bitar ZB, Al-Omari IK, Sonbol HN, Al-Ahmad HT, Cunningham SJ. Bullying among Jordanian schoolchildren, its effects on school performance, and the contribution of general physical and dentofacial features. Am J Orthod Dentofacial Orthop. 2013;144:872-8.
141. Shaw WC, Meek SC, Jones DS. Nicknames, teasing, harassment and the salience of dental features among school children. Br J Orthod. 1980;7:75-80.
142. Seehra J, Fleming PS, Newton T, DiBiase AT. Bullying in orthodontic patients and its relationship to malocclusion, self-esteem and oral health-related quality of life. J Orthod. 2011;38:247-56.
62
143. Al-Omari IK, Al-Bitar ZB, Sonbol HN, Al-Ahmad HT, Cunningham SJ, Al-Omiri M. Impact of bullying due to dentofacial features on oral health-related quality of life. Am J Orthod Dentofacial Orthop. 2014;146:734-9.
144. Pjetursson BE, Asgeirsson AG, Zwahlen M, Sailer I. Improvements in implant dentistry over the last decade: comparison of survival and complication rates in older and newer publications. Int J Oral Maxillofac Implants. 2014;29 Suppl:308-24.
145. Silthampitag P, Klineberg I, Jones AS, Austin B, Zee KY, Wallace C, et al. Ultramicroscopy of bone at oral implant sites: a comparison of ED and control patients. Part 1 – defining the protocol. Int J Prosthodont. 2011;24:147-54.
146. Lesot H, Clauss F, Maniere MC, Schmittbuhl M. Consequences of X-linked hypohidrotic ectodermal dysplasia for the human jaw bone. Front Oral Biol. 2009;13:93-9.
147. Creton M, Geraets W, Verhoeven JW, van der Stelt PF, Verhey H, Cune M. Radiographic features of mandibular trabecular bone structure in hypodontia. Clin Implant Dent Relat Res. 2012;14:241-9.
148. Dueled E, Gotfredsen K, Trab Damsgaard M, Hede B. Professional and patient-based evaluation of oral rehabilitation in patients with tooth agenesis. Clin Oral Implants Res. 2009;20:729-36.
149. Hobkirk JA, Goodman JR, Reynolds IR. Component failure in removable partial dentures for patients with severe hypodontia. Int J Prosthodont. 1989;2:327-30.
150. Lexner MO, Almer L. Case series: Treatment considerations in x-linked hypohidrotic ectodermal dysplasia. Eur Arch Paediatr Dent. 2009;10 Suppl 1:26-30.
151. Thilander B. Orthodontic space closure versus implant placement in subjects with missing teeth. J Oral Rehabil. 2008;35 Suppl 1:64-71.
152. Robertsson S, Mohlin B. The congenitally missing upper lateral incisor. A retrospective study of orthodontic space closure versus restorative treatment. Eur J Orthod. 2000;22:697-710.
153. Uribe F, Chau V, Padala S, Neace WP, Cutrera A, Nanda R. Alveolar ridge width and height changes after orthodontic space opening in patients congenitally missing maxillary lateral incisors. Eur J Orthod. 2013;35:87-92.
154. Uribe F, Padala S, Allareddy V, Nanda R. Cone-beam computed tomography evaluation of alveolar ridge width and height changes after orthodontic space opening in patients with congenitally missing maxillary lateral incisors. Am J Orthod Dentofacial Orthop. 2013;144:848-59.
155. Beyer A, Tausche E, Boening K, Harzer W. Orthodontic space opening in patients with congenitally missing lateral incisors. Angle Orthod. 2007;77:404-9.
156. De-Marchi LM, Pini NI, Ramos AL, Pascotto RC. Smile attractiveness of patients treated for congenitally missing maxillary lateral incisors as rated by dentists, laypersons, and the patients themselves. J Prosthet Dent. 2014;112:540-6.
157. Schneider U, Moser L, Fornasetti M, Piattella M, Siciliani G. Esthetic evaluation of implants vs canine substitution in patients with congenitally missing maxillary lateral incisors: Are there any new insights? Am J Orthod Dentofacial Orthop. 2016;150:416-24.

63
158. Czochrowska EM, Skaare AB, Stenvik A, Zachrisson BU. Outcome of orthodontic space closure with a missing maxillary central incisor. Am J Orthod Dentofacial Orthop. 2003;123:597-603.
159. Shaw WC, Dahl E, Asher-McDade C, Brattstrom V, Mars M, McWilliam J, et al. A six-center international study of treatment outcome in patients with clefts of the lip and palate: Part 5. General discussion and conclusions. Cleft Palate Craniofac J. 1992;29:413-8.







