Sue Hanson National Director Clinical Services
Little Company of Mary Health Care
Co-Chair NSW ACI Palliative Care Network
What does „ACP‟ actually mean?
Why do we need to change our thinking about ACP?
How can we improve peoples experience in the last year of life?
Advance Care Planning in the Community

Depends - confusing terminology:
Advance Care Planning
Advance Care Directives
Medical Orders for Life Sustaining Treatment
Advanced Resuscitation Plans - NFR
Goals of Care
What is Advance Care Planning anyway?
144,000 people will die in Australia each year
expected to increase to 320,000 by 2056
75% of deaths can be „expected‟
51% of all deaths in those aged 80+1
400% increase in those aged 85+
88% of those aged 65+ have 3 or more chronic illnesses 3
88% of residents leave RACF due to death4 17% had stayed less than 3 months
Further 19% between 3-12 months before death
What we know about dying
5
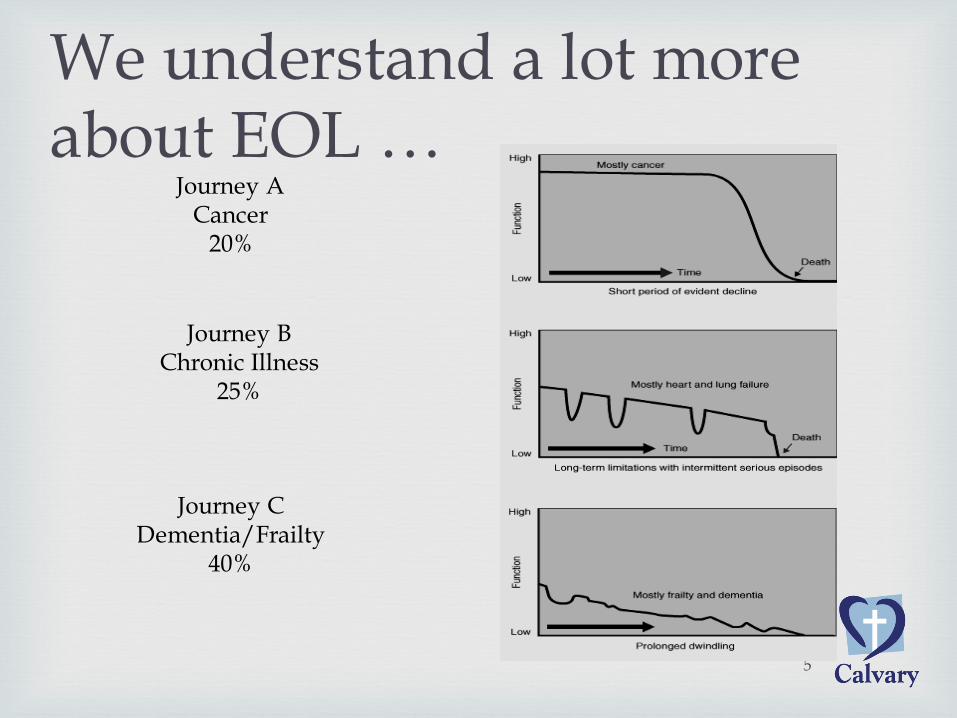
We understand a lot more about EOL …
Journey A Cancer
20%
Journey B Chronic Illness
25%
Journey C Dementia/Frailty
40%
In 2011-12 people in the last year of life consumed
nearly a million bed days in NSW- nearly 10% of all
bed days
Accounted for nearly $1Billion in inpatient costs
Forecast threefold increase in real healthcare and residential expenditure over thirty year period -
$85.06b (02/03) to $246.06b (2032/33)
2.3% of privately insured use 1/3rd of all hospital benefits
Costs in the Last Year of Life
Where do we die?
More than 50% of people will die in hospital
16% will die in a RACF
Less than 20% will be able to remain at home
70% of people when surveyed would choose to remain at home

Forty-nine per cent of patients were recognised as dying 24
hours or less before death
17% between 24 and 36 hours before death,
21% between 36 and 72 hours before death, and
13% greater than 72 hours before death Journal Clinical Medicine, 2009
Healthcare workers feel obliged to deliver care if no ACD exists
ACSQHC Consensus statement
Concerns about euthanasia
Too little - too late?

HOSPITAL
GENERAL
PRACTITIONER
REFERRING SPECIALIST
COMMUNITY NURSING/ ALLIED HEALTH
Patient Journey Last Year of Life - current
Admissions
ICU
AGED CARE
Icons © NEHTA 2013
Spec Palliative Care
EMERGENCY DEPT
• Gateways concept
• Goals of care
• Made in the context of an already experienced burden
• Ongoing assessment – preventing suffering/promoting healing
• Linked to person goals-based medical care - MOLST
A better model?

Developing a systems approach
Diagnosis
Chronic
Illness
Gateway 1
EOL
Gateway 2
Imminent Dying Death
Transition Points
Years 12 months 48-72 hours Death
Patient journey approaching the end of life
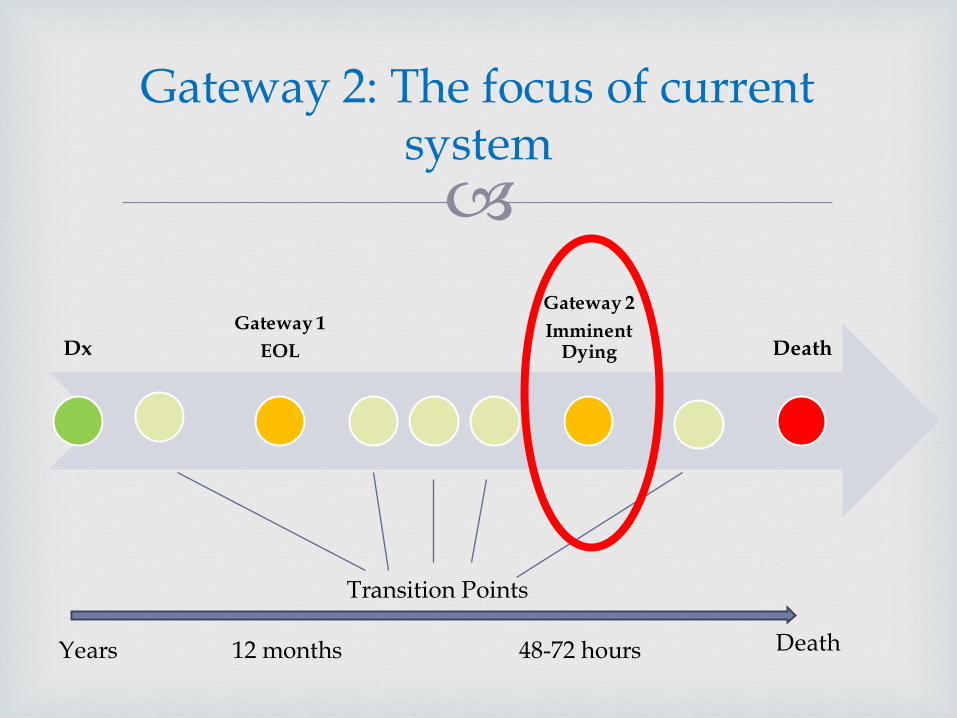
Gateway 2: The focus of current system
Dx
Gateway 1
EOL
Gateway 2
Imminent Dying Death
Transition Points
Years 12 months 48-72 hours Death
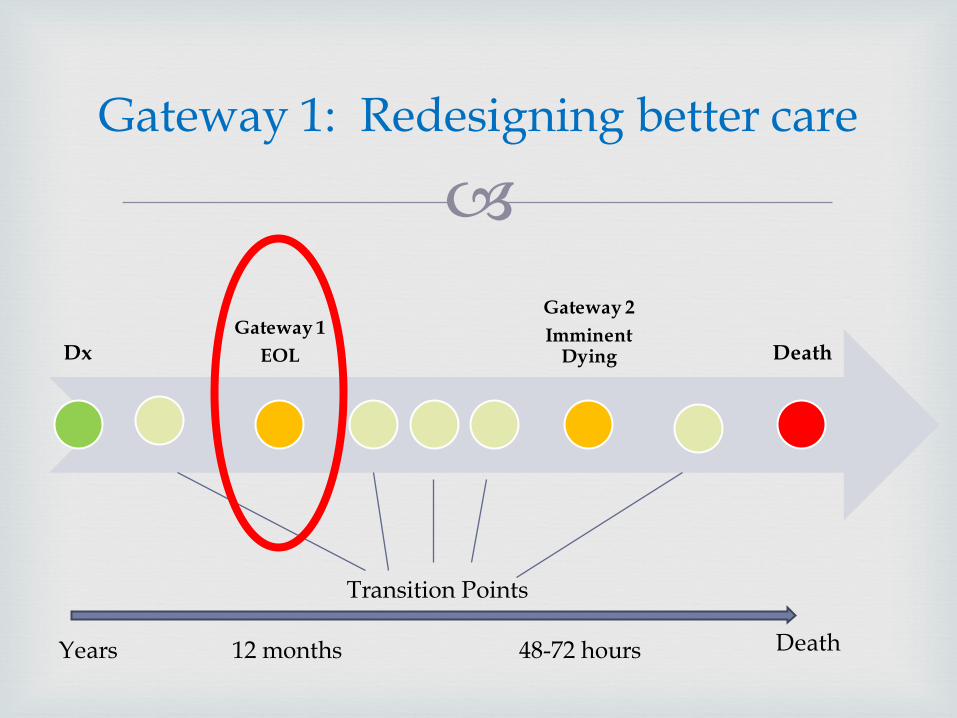
Gateway 1: Redesigning better care
Dx
Gateway 1
EOL
Gateway 2
Imminent Dying Death
Transition Points
Years 12 months 48-72 hours Death
Shift away from „hit by a bus‟ thinking
Shift from thinking about THE conversation
Shift from late to early conversations
Shift to thinking about care planning
Facilitate person-centred care
Document values, beliefs and goals
Identify substitute decision-maker for loss of decision-making capacity
Progressive, ongoing structured conversation that aligns to patient journey
Shifting our thinking

Initiate routine discussions about care
Explore understanding of disease progression
Search out values of „living well‟
Clarify statements the person makes
Discover the meaning of their experience
Explore barriers to advance care planning
Assist in selection of proxy
Advocate for and communicate persons wishes
Core ACP Skills
Initiate Routine Discussion
It‟s never too early to plant a seed
Begin discussion at regular intervals e.g. home visits, clinics, care conferences
Provide basic information first, then add more discussion over time
Incorporate as a component of good patient care (“We’re trying to begin these talks with all of our patients”)
Care in the last Year of Life
Person you would not be surprised died in the next 12 months, e.g. sentinel event, low serum albumin
Frequent hospitalizations
Declining functional status
Verbal cues e.g. “I‟m not sure all of this is worth it to me anymore”
Building new models of care that support people to have
real choices at the end of life rely on some basic principles:
Put patients, their families and carers at the centre
Including people as partners in care
Focus on quality of life and care
Deliver care as close to home as possible
Thank you
In conclusion







