1
Surgical Management of Cushing’s Disease: Recurrence After Early Remission
Baha M Arafah, MD
Case Western Reserve University
2
Diagnosis and Management of Cushing’s Syndrome
• Continues to be challenging• Can be a humbling experience• Requires integration of all available data and
great attention to details• One can not take short cuts
3
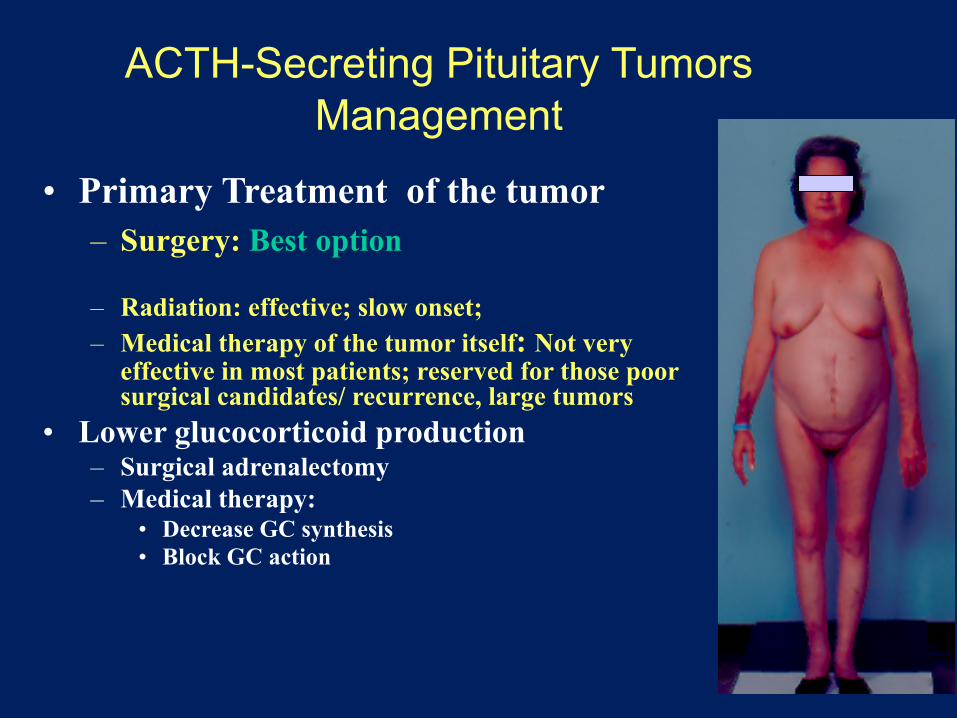
ACTH-Secreting Pituitary TumorsManagement
• Primary Treatment of the tumor– Surgery: Best option
– Radiation: effective; slow onset; – Medical therapy of the tumor itself: Not very
effective in most patients; reserved for those poor surgical candidates/ recurrence, large tumors
• Lower glucocorticoid production– Surgical adrenalectomy– Medical therapy:
• Decrease GC synthesis• Block GC action

4
ACTH-Secreting Pituitary Adenomas
Assessment of Surgical Adenomectomy Outcome• Immediate Evaluation: Development of ACTH deficiency• Subsequent assessment:
– Clinical and biochemical remission• Long-term management:
– Taper hydrocortisone gradually– Most patients stop hydrocortisone in 6-12 months– Testing after discontinuation of glucocorticoids to confirm NL
HPA function– Subsequent follow up/ testing is necessary– Possible recurrence
5
ACTH-Secreting Pituitary Adenomas
• Success of Surgical adenomectomy depends on– Correct diagnosis – Expertise / experience– Tumor size and / or extension
• Assessment of Surgical Outcome– Clinical remission: takes several months– Immediate development of ACTH deficiency
• Is this a reliable indicator? • Evaluation can be confounded by peri-operative GC use
6
Peri-Operative Management
• Literature Review• Inconsistent Approach
– Give GC peri-operatively• Change to dexamethasone, measure serum cortisol• CRH test (while on dexamethasone)• Withhold GC at 2, 6 , or 12 weeks and measure serum cortisol
– Withhold GC• Measure serum cortisol• Give GC to those whose serum cortisol levels are “low” • Give GC to patients with symptoms of AI• Is it safe?
7
Management of Patients with ACTH-Secreting Pituitary AdenomasOur Peri-operative Management
• No GC are administered before or during surgery• Cortisol & ACTH levels are measured every 4-6 hours post-operatively • Patients are monitored for signs/ symptoms of AI• GC are administered if and when either one of the following happens
• Patient has symptoms• Serum cortisol < 3 mcg/dL
• Advantages of this approach:
• Provides immediate and Long-term assessment of function
• Ability to get reliable peri-operative data that can predict future recurrence
Neurosurg Focus 2015JCEM 2013, 98: 1458-65. JCEM 2018; 103:477-485
8
0
10
20
30
40
0
20
40
60
80
100
0 1 2 3
Corti
sol (
ug/d
L)
AC
TH (n
g/L)
Days Post op
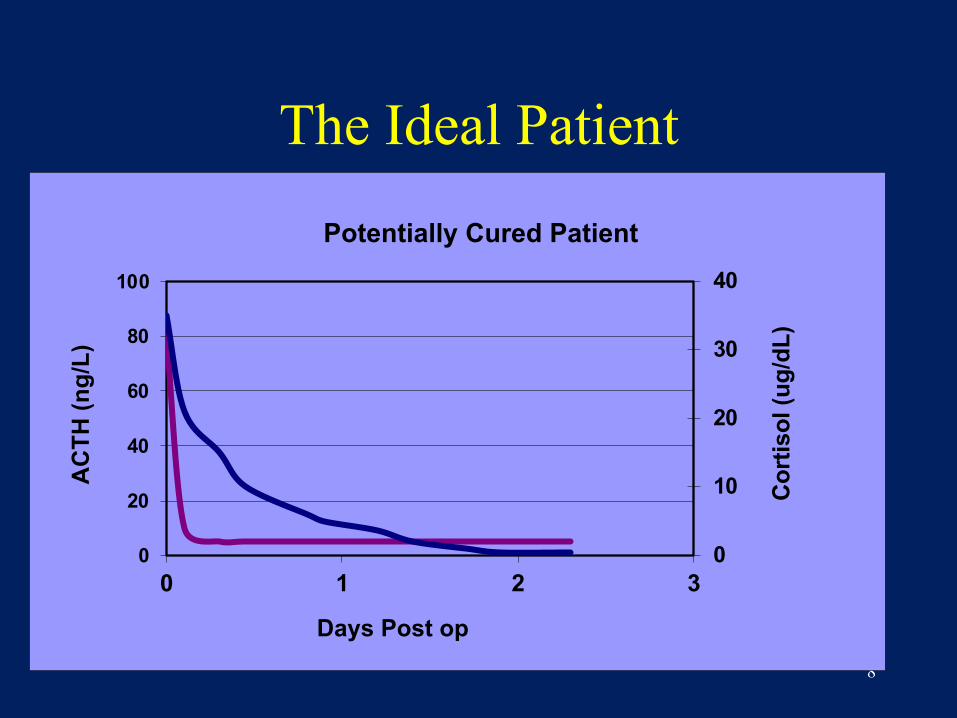
Potentially Cured Patient
The Ideal Patient
9
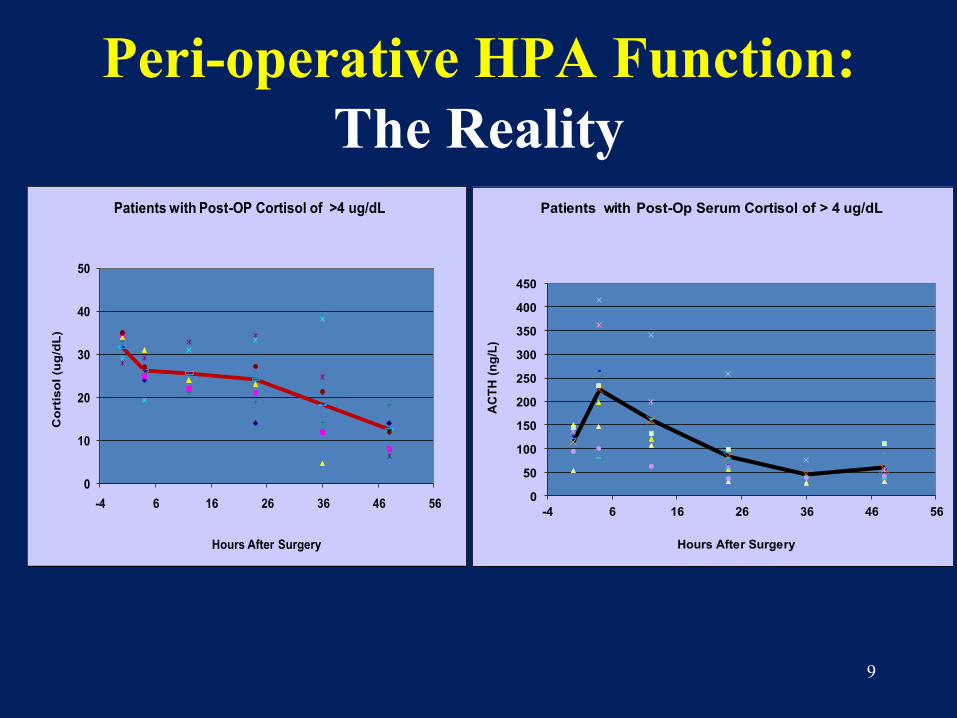
Peri-operative HPA Function: The Reality
0
50
100
150
200
250
300
350
400
450
-4 6 16 26 36 46 56A
CTH
(ng/
L)
Hours After Surgery
Patients with Post-Op Serum Cortisol of > 4 ug/dL
0
10
20
30
40
50
-4 6 16 26 36 46 56
Cor
tisol
(ug/
dL)
Hours After Surgery
Patients with Post-OP Cortisol of >4 ug/dL
10
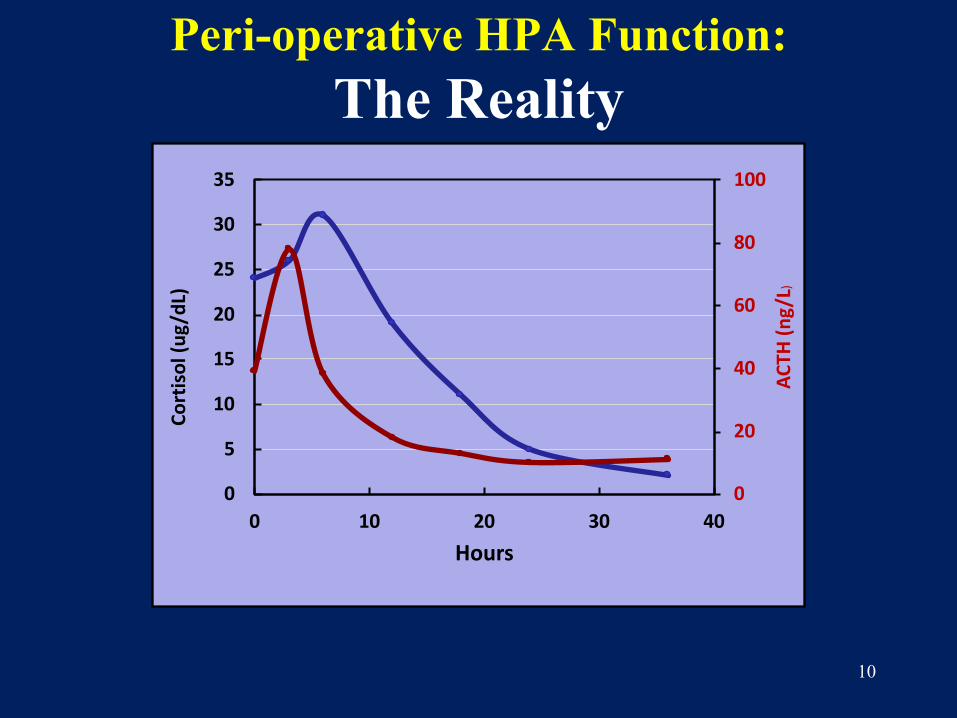
Peri-operative HPA Function: The Reality
0
20
40
60
80
100
0
5
10
15
20
25
30
35
0 10 20 30 40
ACTH
(ng/
L)
Cort
isol
(ug/
dL)
Hours
11
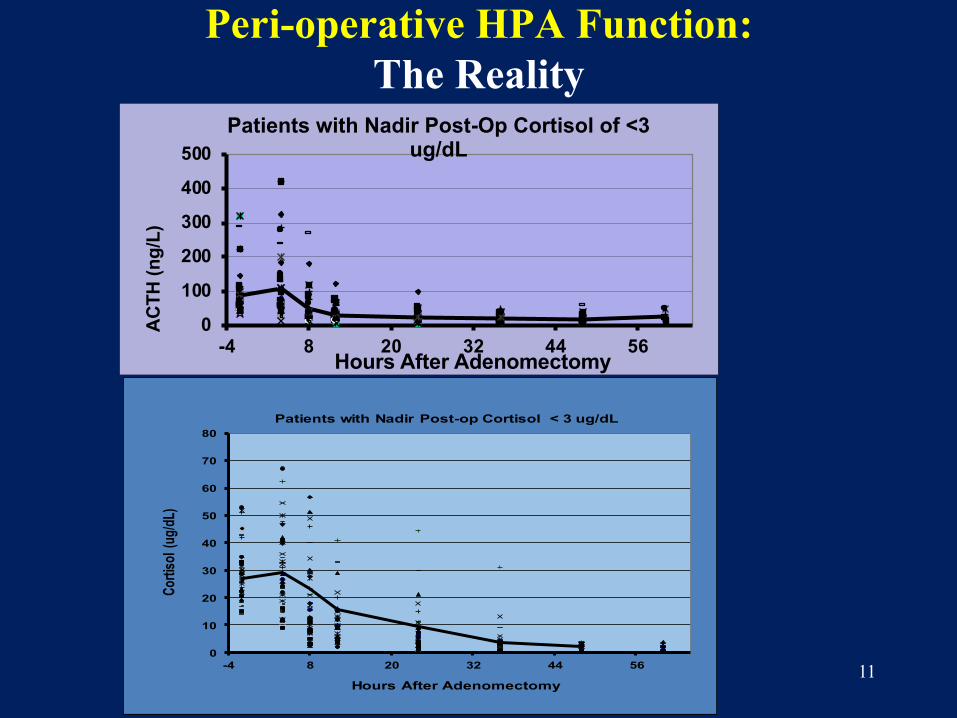
Peri-operative HPA Function: The Reality
0
10
20
30
40
50
60
70
80
-4 8 20 32 44 56
Cortis
ol (ug
/dL)
Hours After Adenomectomy
Patients with Nadir Post-op Cortisol < 3 ug/dL
0
100
200
300
400
500
-4 8 20 32 44 56
ACTH
(ng/
L)
Hours After Adenomectomy
Patients with Nadir Post-Op Cortisol of <3 ug/dL

12
Nadir Serum Cortisol of ≤ 3 ug/dL
N=66
Nadir Serum Cortisol of ≥ 4 ug/dL
N=13
P Value:
Age 39.8±12.3 39.3±8.5 0.67
Gender: Females: males 46:20 8:5 0.28
Tumor size(cm) 0.79±0.52 1.48 ± 0.72* 0.01
Pre-operative Data
ACTH (ng/L)Cortisol (ug/dL)DHEA (ng/ml)
DHEA-S (ug/dL)
80.2± 66.829.9± 12.37.7± 5.0
151.9± 57.1
89.9± 45.730.6± 6.4
9.0 4.8171.6±39.3
0.930.970.140.11
Pre- and Post-Operative Clinical and Biochemical Characteristicsin 79 Patients with Cushing’s disease stratified according
to their Nadir Postoperative Serum Cortisol Levels
JCEM 2013, 98: 1458-65.JCEM 2018; 103:477-485
13
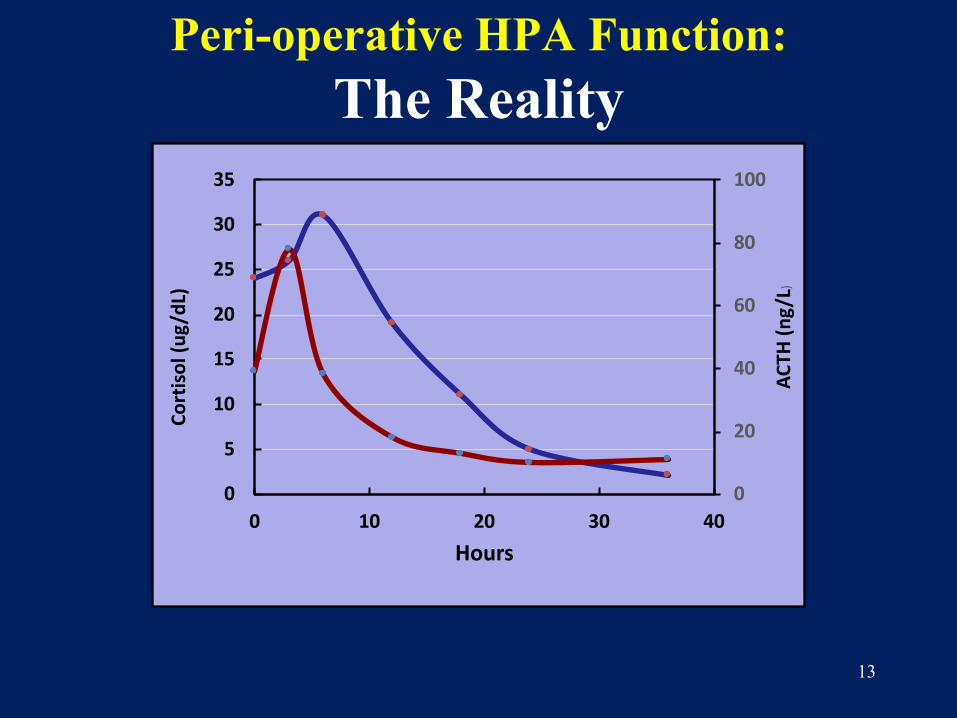
Peri-operative HPA Function: The Reality
0
20
40
60
80
100
0
5
10
15
20
25
30
35
0 10 20 30 40
ACTH
(ng/
L)
Cort
isol
(ug/
dL)
Hours
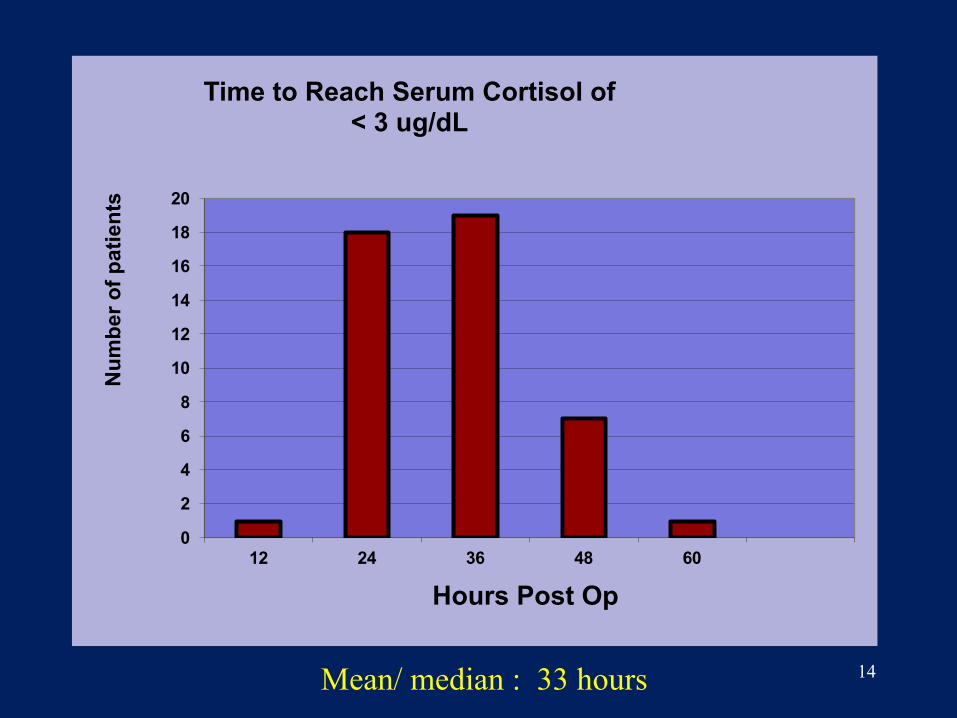
14
0
2
4
6
8
10
12
14
16
18
20
12 24 36 48 60
Num
ber o
f pat
ient
s
Hours Post Op
Time to Reach Serum Cortisol of < 3 ug/dL
Mean/ median : 33 hours
15
Recurrence of Cushing’s Disease
• Does it happen after initial remission? – Depends how remission was defined
• How often? 10-30 % • Why ?• Can we predict who will have recurrence?
16
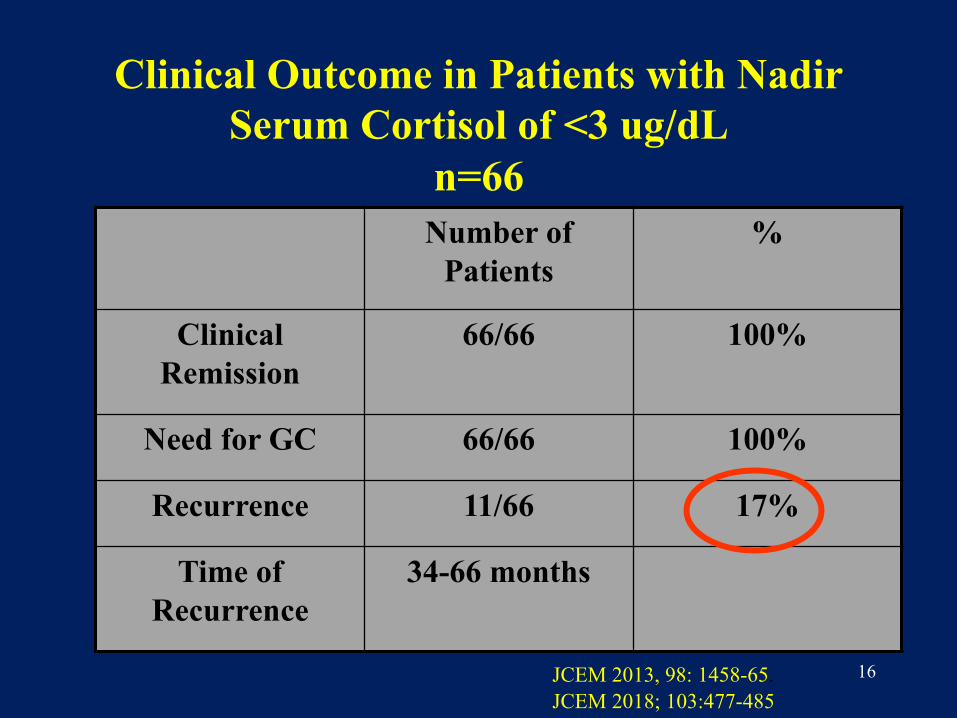
Clinical Outcome in Patients with Nadir Serum Cortisol of <3 ug/dL
n=66Number of
Patients%
Clinical Remission
66/66 100%
Need for GC 66/66 100%
Recurrence 11/66 17%
Time of Recurrence
34-66 months
JCEM 2013, 98: 1458-65.JCEM 2018; 103:477-485
17
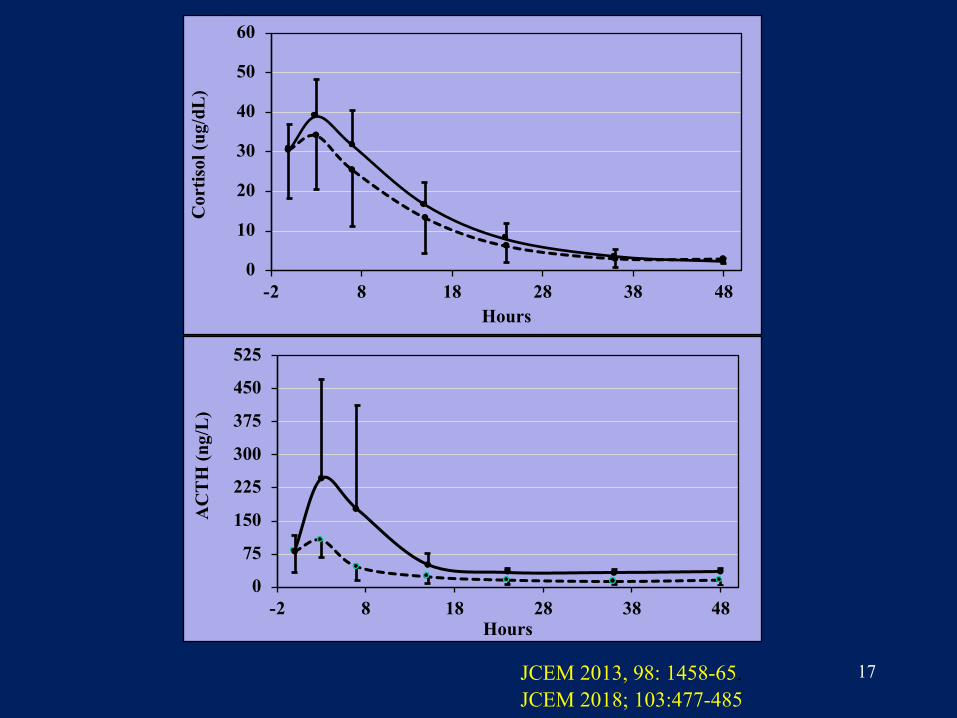
0
10
20
30
40
50
60
-2 8 18 28 38 48
Cor
tisol
(ug/
dL)
Hours
0
75
150
225
300
375
450
525
-2 8 18 28 38 48
AC
TH
(ng/
L)
Hours
JCEM 2013, 98: 1458-65.JCEM 2018; 103:477-485
18
Patients Who Had Sustained Remission
(N=55)
Patients with Recurrence
(N=11)
P Value: Sustained Remission VS Recurrence
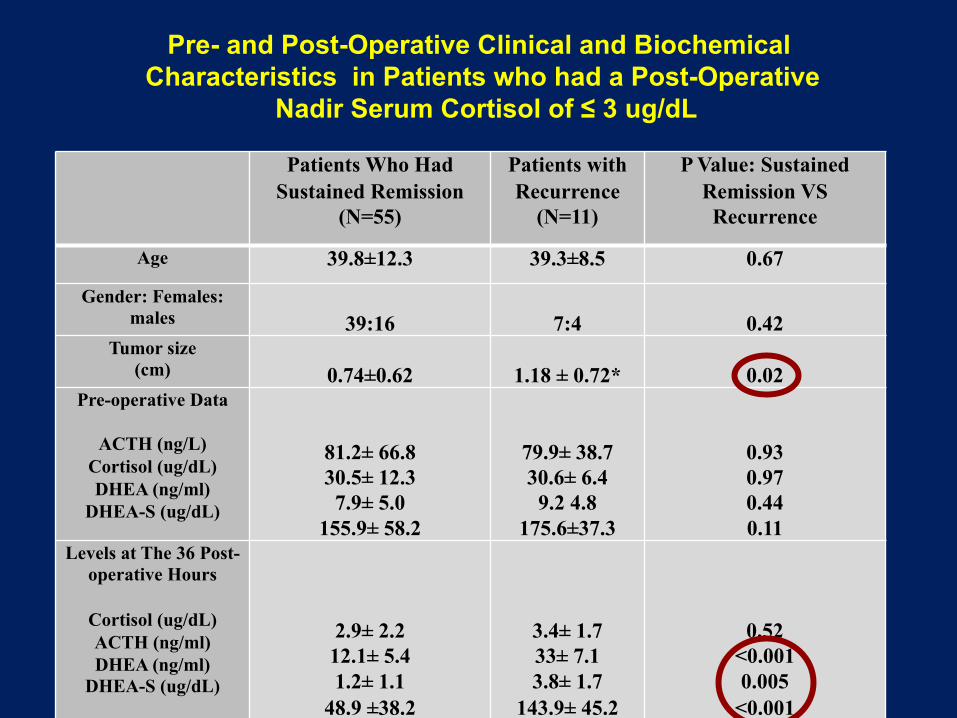
Age 39.8±12.3 39.3±8.5 0.67
Gender: Females: males 39:16 7:4 0.42
Tumor size(cm) 0.74±0.62 1.18 ± 0.72* 0.02
Pre-operative Data
ACTH (ng/L)Cortisol (ug/dL)DHEA (ng/ml)
DHEA-S (ug/dL)
81.2± 66.830.5± 12.37.9± 5.0
155.9± 58.2
79.9± 38.730.6± 6.4
9.2 4.8175.6±37.3
0.930.970.440.11
Levels at The 36 Post-operative Hours
Cortisol (ug/dL)ACTH (ng/ml)DHEA (ng/ml)
DHEA-S (ug/dL)
2.9± 2.212.1± 5.41.2± 1.1
48.9 ±38.2
3.4± 1.733± 7.13.8± 1.7
143.9± 45.2
0.52<0.0010.005
<0.001
Pre- and Post-Operative Clinical and Biochemical Characteristics in Patients who had a Post-Operative
Nadir Serum Cortisol of ≤ 3 ug/dL
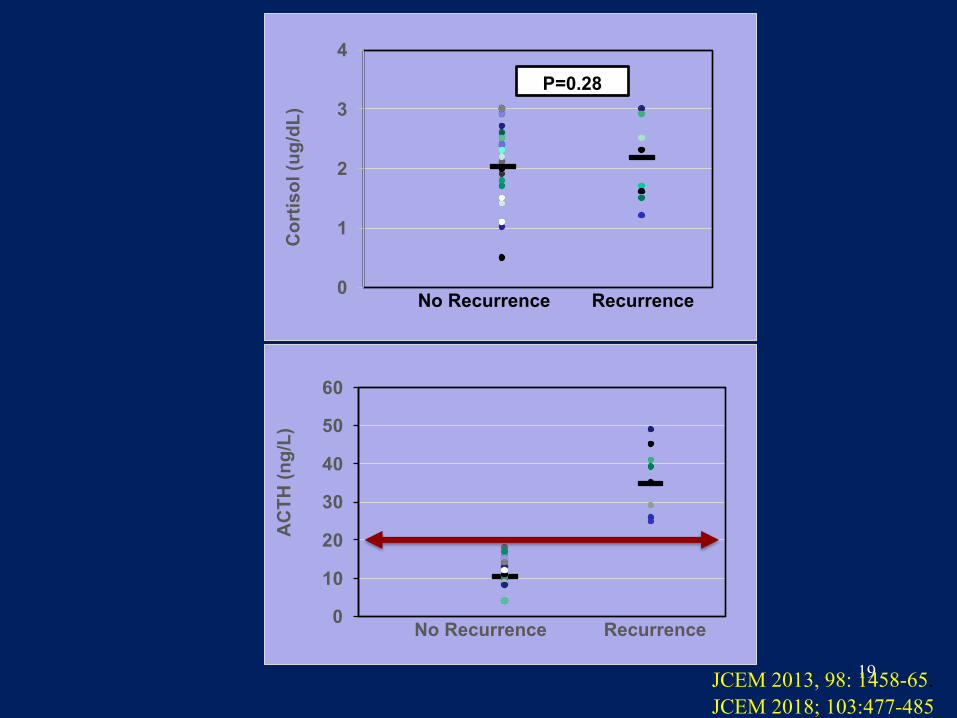
19
0
10
20
30
40
50
60
AC
TH (n
g/L)
No Recurrence Recurrence
0
1
2
3
4
Cor
tisol
(ug/
dL)
No Recurrence Recurrence
P=0.28
JCEM 2013, 98: 1458-65.JCEM 2018; 103:477-485
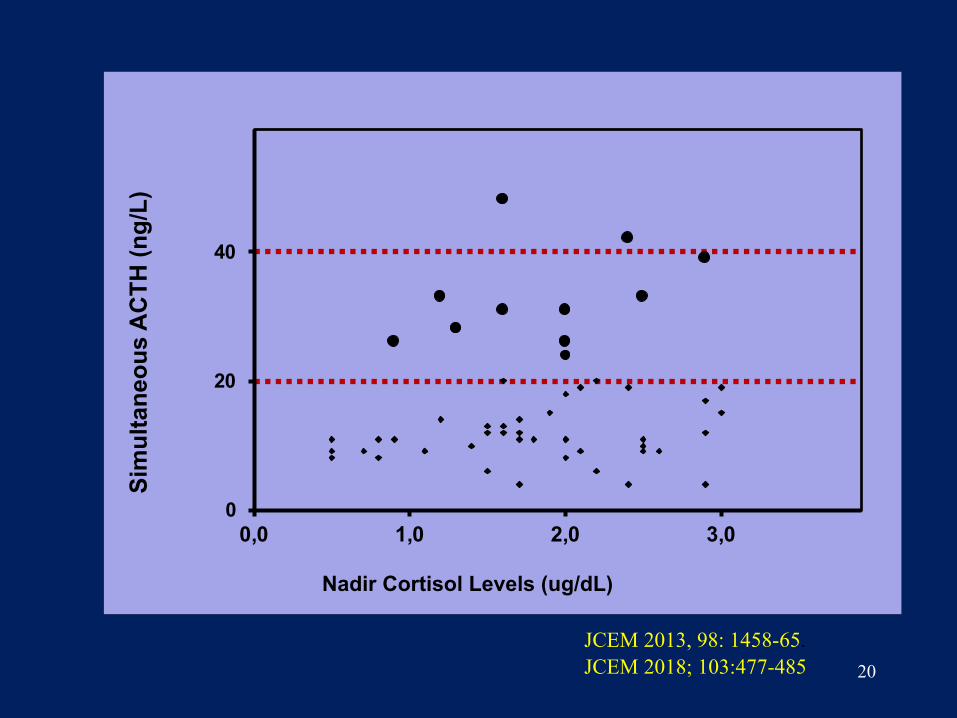
20
0
20
40
0,0 1,0 2,0 3,0
Sim
ulta
neou
s A
CTH
(ng/
L)
Nadir Cortisol Levels (ug/dL)
JCEM 2013, 98: 1458-65.JCEM 2018; 103:477-485
21
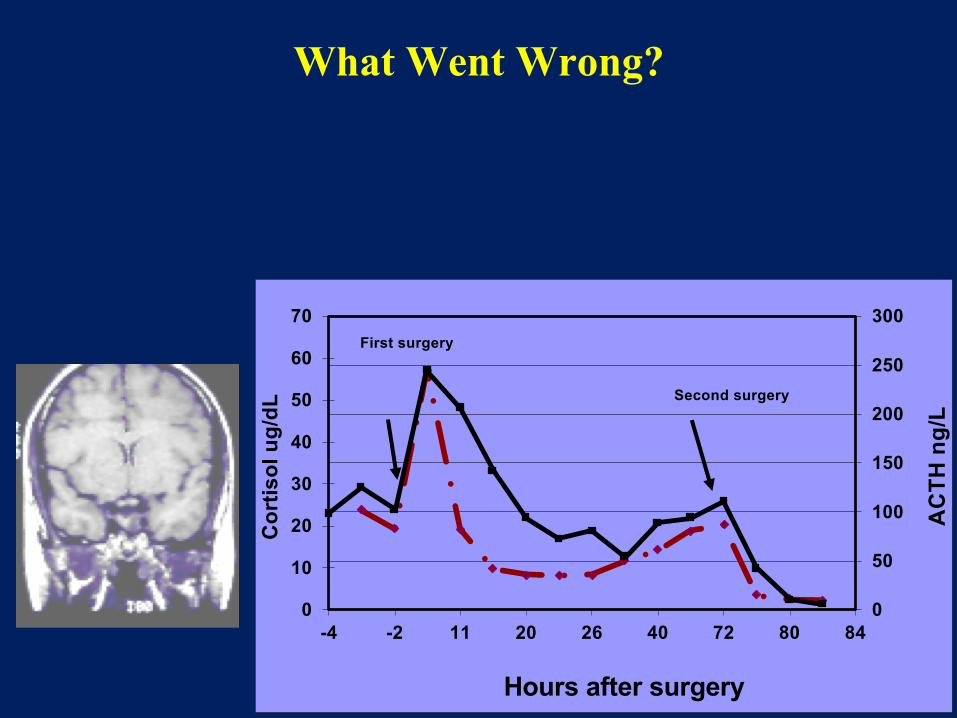
What Went Wrong?
0
10
20
30
40
50
60
70
0
50
100
150
200
250
300
-4 -2 11 20 26 40 72 80 84
Cor
tisol
ug/
dL
AC
TH n
g/L
Hours after surgery
First surgery
Second surgery

22
ACTH-Secreting Pituitary AdenomasSummary
1. Avoiding the routine use of glucocorticoids during and immediately after adenomectomy is a safe and valuable approach as it provides important clinical data that can affect immediate management as well as help predict long-term benefit
2. Despite low serum cortisol levels of < 3 ug/dl, plasma ACTH in the immediate peri-op period in patients who had recurrences were not low
3. The most likely explanation for the persistence of ACTH secretion in the peri-op period is the presence of residual tumor
4. Measurements of plasma ACTH & cortisol levels in the immediate post op period are valuable in defining immediate and long-term benefit from adenomectomy
23
Thank You







