Download - The ABCs of BPH
Interventional Radiologist
Northwell Health Physician Partners
Vice Chairman- Department of Radiology
Long Island Jewish Medical Center
Associate Professor
Hofstra Northwell School of Medicine
Attending Physician
Departments of Radiology, Surgery and Urology
The ABCs of BPH

David Siegel, M.D., FSIR
• Speakers Bureau: St. Jude Medical
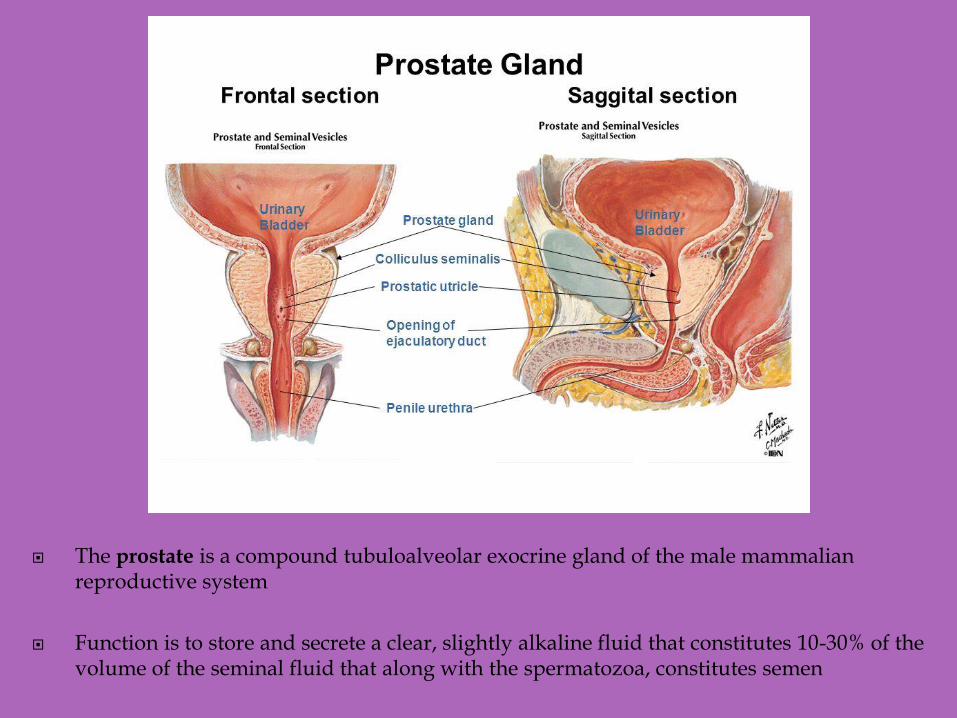
The prostate is a compound tubuloalveolar exocrine gland of the male mammalian reproductive system
Function is to store and secrete a clear, slightly alkaline fluid that constitutes 10-30% of the volume of the seminal fluid that along with the spermatozoa, constitutes semen

Benign Prostatic Hyperplasia
is a nonmalignant enlargement
of the prostate gland caused by
cellular hyperplasia of both
glandular and stromal
elements that leads to
troublesome lower urinary
tract symptoms (LUTS) in
some men

• Nearly 20 million US men have BPH
• 12 million require therapy
• Annual US cost is > 3 billion dollars
• >40% of men over 50 have the condition >80% after 80

columnar arrangement of cells
corpora amylacea in gland lumens

BPH= “nodular prostatic hyperplasia”
nodule filled with enlarged glands

Cause not completely understood
Reawakening of the urogenital sinus to proliferate
Change in hormonal milieu with alterations in the testosterone/estrogen balance.
Induction of prostatic growth factors
Increased stem cells/decreased stromal cell death
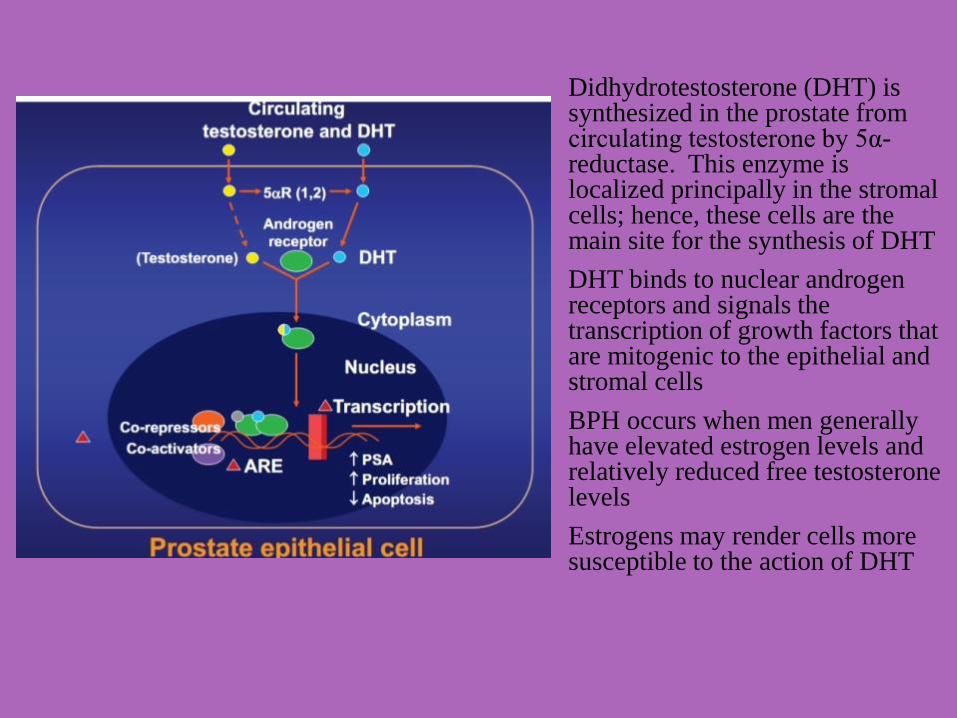
Didhydrotestosterone (DHT) is synthesized in the prostate from circulating testosterone by 5α-reductase. This enzyme is localized principally in the stromal cells; hence, these cells are the main site for the synthesis of DHT
DHT binds to nuclear androgen receptors and signals the transcription of growth factors that are mitogenic to the epithelial and stromal cells
BPH occurs when men generally have elevated estrogen levels and relatively reduced free testosterone levels
Estrogens may render cells more susceptible to the action of DHT

Age
Hereditary(genetic)/Race
Blacks
Hispanics
Lifestyle
Obesity
No Association with Smoking or Exercise
Kristal, Alan R., Kathryn B. Arnold, Jeannette M. Schenk, Marian L. Neuhouser, Noel Weiss, Phyllis Goodman, Colleen M. Antvelink, David F. Penson, and Ian M. Thompson. “Race/Ethnicity, Obesity, Health Related Behaviors and the Risk of Symptomatic Benign Prostatic Hyperplasia: Results From the Prostate Cancer Prevention Trial.” The Journal of Urology 177, no. 4 (April 2007): 1395–1400. doi:10.1016/j.juro.2006.11.065.
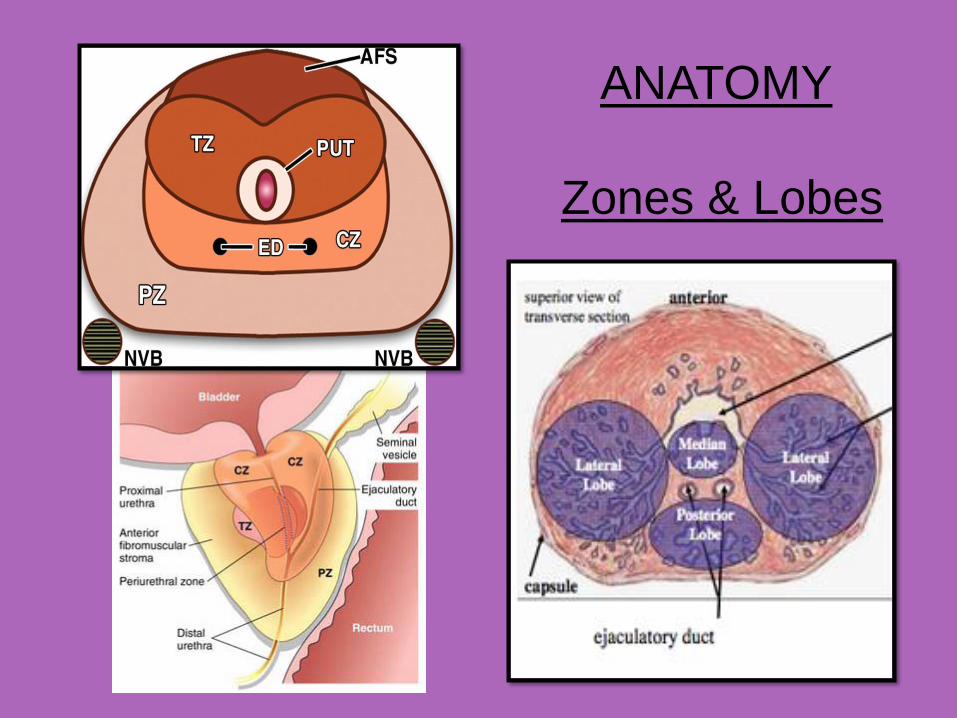
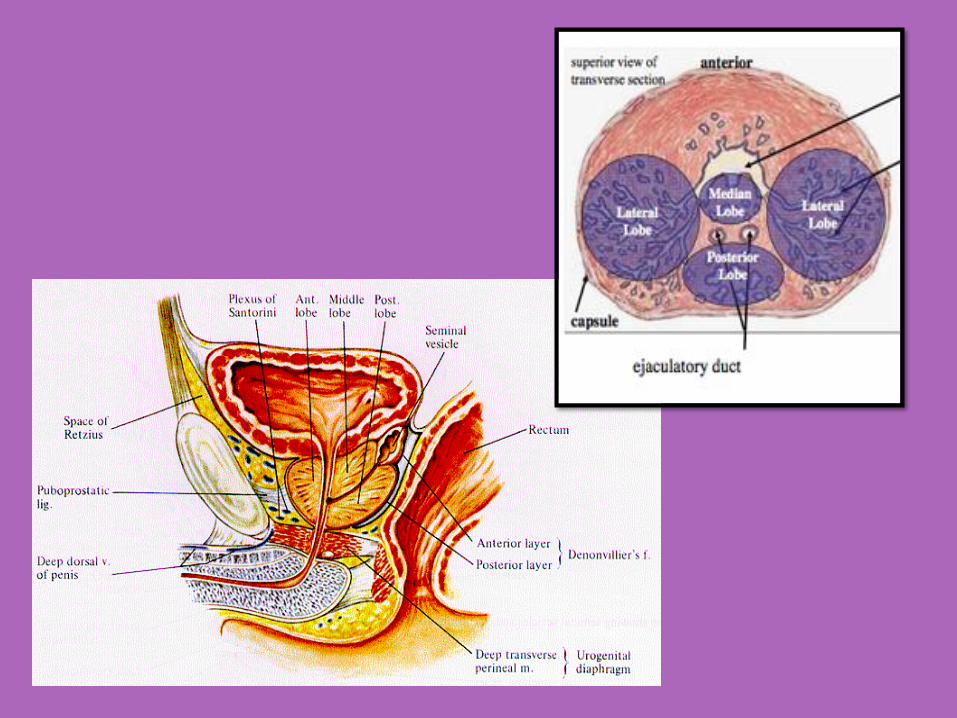
ANATOMY
Zones & Lobes

Normal BPH
Hypertrophied
detrusor muscle
Obstructed
urinary flow
PROSTATE
BLADDER
URETHRA
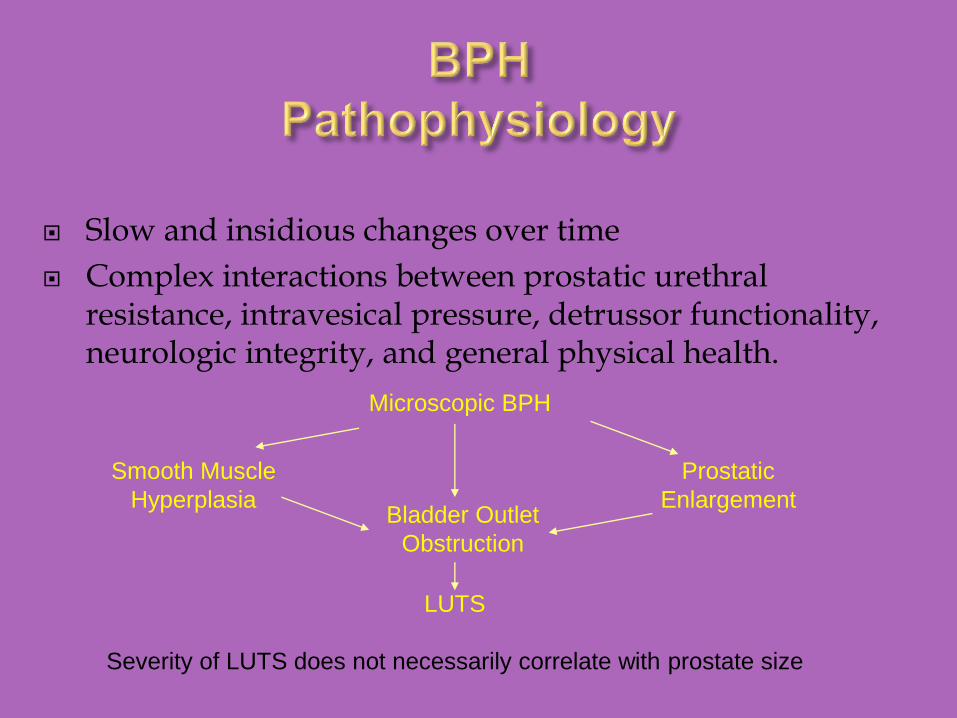
Slow and insidious changes over time
Complex interactions between prostatic urethral resistance, intravesical pressure, detrussor functionality, neurologic integrity, and general physical health.
Microscopic BPH
Smooth Muscle
Hyperplasia
Prostatic
EnlargementBladder Outlet
Obstruction
LUTS
Severity of LUTS does not necessarily correlate with prostate size

15
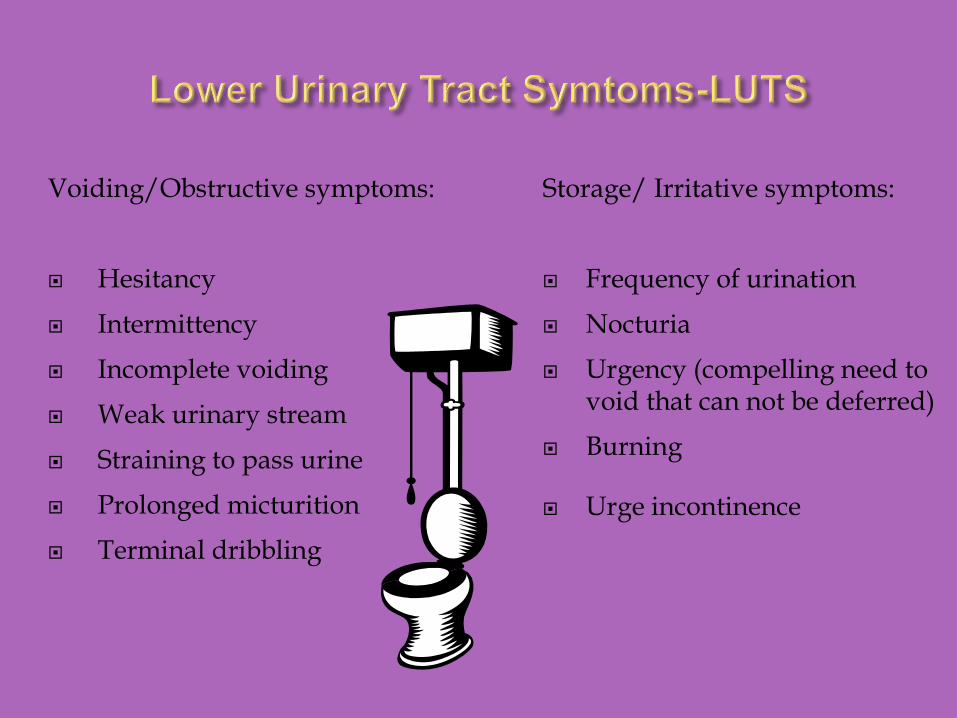
Voiding/Obstructive symptoms:
Hesitancy
Intermittency
Incomplete voiding
Weak urinary stream
Straining to pass urine
Prolonged micturition
Terminal dribbling
Storage/ Irritative symptoms:
Frequency of urination
Nocturia
Urgency (compelling need to void that can not be deferred)
Burning
Urge incontinence

Prostatitis
Neurogenic bladder
Drugs
Polyuria
Dietary
Constipation
Psychological
Urethral stricture
Bladder neck contracture
Carcinoma of the prostate
Carcinoma of the bladder
Bladder calculi
Urinary tract infection

18
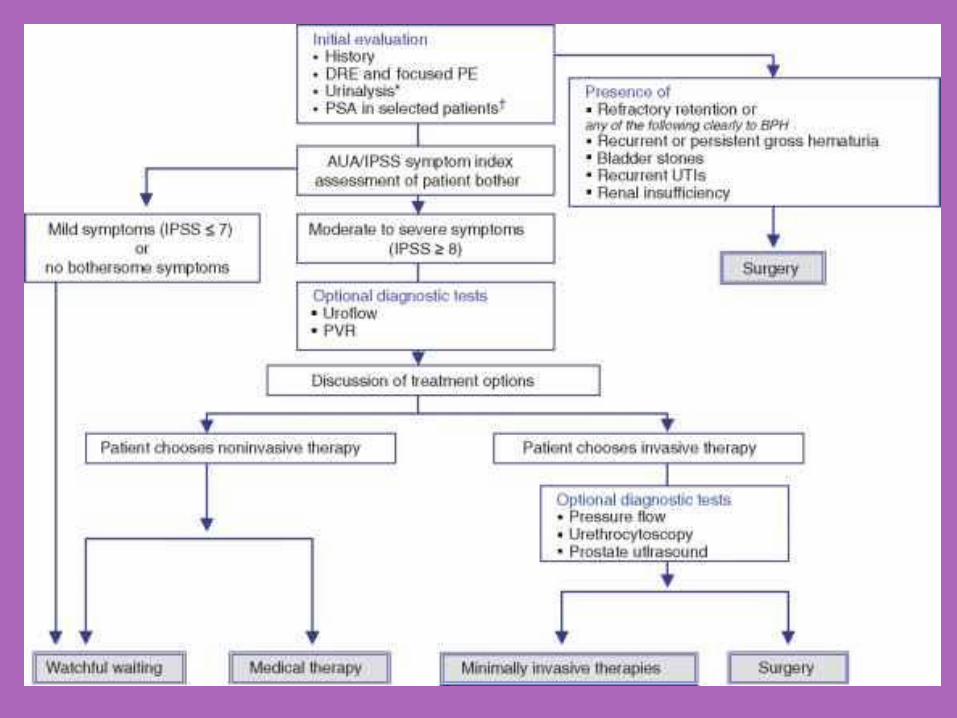
History & Examination Abdominal/GU exam
Focused neuro exam
Digital rectal exam (DRE)
Validated symptom questionnaire
Urinalysis
Urine culture
BUN, Cr
Prostate specific antigen (PSA)
Uroflometry
Prostate MRI
_________________
Post-void residual
Urodynamics
Transrectal ultrasound
Prostate Biopsy
Elevated levels of PSA
0 – 4 ng/ml (? 2.5 or 3ng/ml)
Prostatic pathology
Some men with prostate cancer have normal PSA levels

Firm to hard nodules
Irregularities
Unequal lobes
Induration
Stony hard prostate
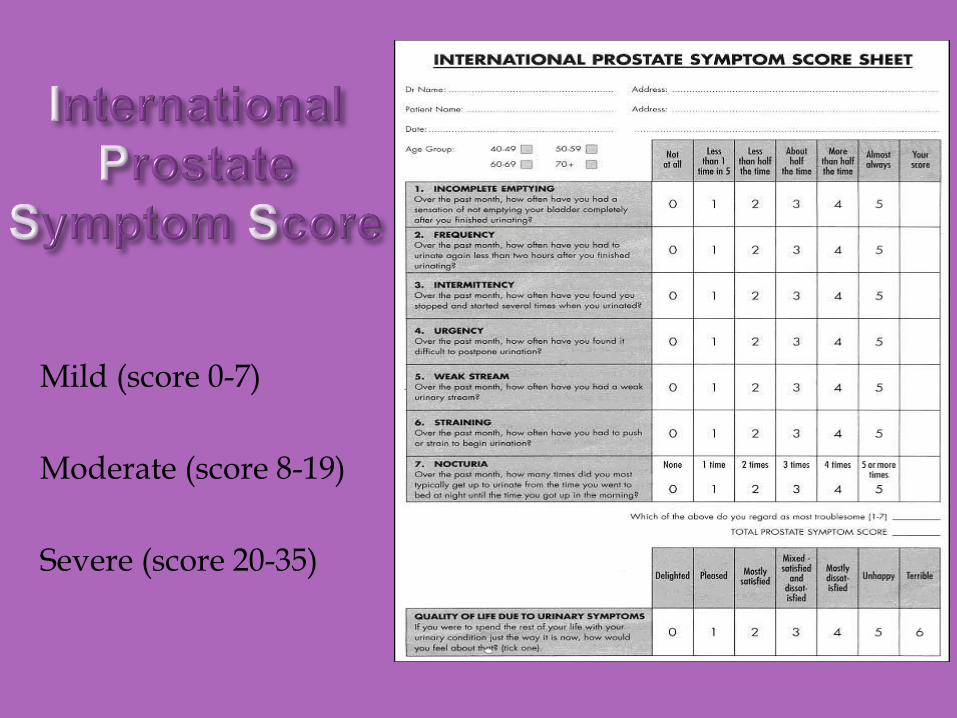
Mild (score 0-7)
Moderate (score 8-19)
Severe (score 20-35)
Interventional Radiologist
Northwell Health Physician Partners
Vice Chairman- Department of Radiology
Long Island Jewish Medical Center
Associate Professor
Hofstra Northwell School of Medicine
Attending Physician
Departments of Radiology, Surgery and Urology
The ABCs of BPH







