
Disclosure
The following slides were developed for a presentation to the Kentucky Board of Pharmacy at the 2015 Board Retreat. Parts of the presentation have been edited due to usage agreements. These slides refer to some requirements of USP 797 but are not all inclusive. The slides have been made available at individual request.
T H E K E N T U C K Y B O A R D O F P H A R M A C Y S E R V E S T H E C O M M O N W E A L T H T O
P R O M O T E , P R E S E R V E , A N D P R O T E C T T H E P U B L I C H E A L T H , S A F E T Y , A N D W E L F A R E
T H R O U G H E F F E C T I V E R E G U L A T I O N O F T H E P R A C T I C E O F P H A R M A C Y .
Sterile Compounding Inspections

Objectives
Brief History of USP 797
Inspector Training and Inspection Form
Observations Facility Controls Personnel Matrix Documentation

Objectives
Clarifications Facility Controls
Design Certification and Testing Surface Sampling
Documentation Record Retention Stability References Sterility Testing Compound Record
Personnel Matrix Supervision

Objectives
Where do we go from here? Communications with pharmacists Future Board Meeting updates Future clarifications Nuclear pharmacies Regulation update Report care Out of State permits Non-sterile compounding USP 795

Brief History of USP 797
Published November 2003 Became official January 2004
First major proposed revision December 2007 Became official June 2008
Second major proposed revision September 2015 Comment period November 2, 2015 to January 31,
2016 Becomes official ???

Kentucky Statute
KRS 217.015(31) – “Official compendium” means the official United States Pharmacopoeia, official homeopathic pharmacopoeia of the United States, official national formulary, or any supplement to any of them.
July 2008 Board Meeting, the Board clarified low volume for hazardous drugs to be an average of 5 hazardous compounds/2 week period.
Inspectors Trainings
Critical Point Continuing Education Boot Camp Inspector Training

Inspection Form
Previously 10 questions on hospital, organized healthcare facility or infusion pharmacy inspection form, none on community/retail pharmacy inspection
Updated form 16 pages, universal not practice site specific
Addresses requirements of USP Chapter 797 also incorporates 201 KAR 2:076 ParenteralPharmaceutical Compounding
Divided into sections based on chapter headings and compounding types
2013 Compounding Survey
In-State Pharmacy Permit Holders Response Rate: 1306/1341 (97%) Performing Sterile Compounding: 195 (15% of responders)
High Risk: 33 (17% of sterile compounders or 3% of responders)* 1346 current in-state pharmacy permit holders (as of 8/5/15)
Out-of-State Pharmacy Permit Holders Response Rate: 451/466 (97%) Performing Sterile Compounding: 170 (38% of responders)
High Risk: 82 (48% of sterile compounders or 18% of responders) 669 current out-of-state pharmacy permit holders (as of
8/5/15)* May not be true representation some confusion with hazardous drug compounding
2013 Compounding Survey
In-State Sterile Compounders by Permit Type: Hospital and Hospital/Ambulatory: 114
High Risk: 9 Reality: 2 Community Independent: 36
High Risk: 18 Reality: 14 (5 veterinarian only) Infusion: 23
High Risk: 5 Reality: 0 Long Term Care: 16
High Risk: 1 Reality: 0 Nuclear: 6
Inspection Observations
Facility Controls Personnel Metrics Documentation

Facility Controls
Design Workflow Hazardous Rooms
Cleaning/Maintenance Documentation Environmental Services
ISO Classification Consistent certification
Environmental Sampling Re-sampling Sampling plan
Personnel Metrics
Garbing/Hand Hygiene Minor differences
Aseptic Technique Supervision
Cleaning Documentation
Equipment Training

Documentation
Policies & Procedures Formulaic
Personnel Training Observations, Written
tests, Media fill, Gloved Fingertip Sampling
Facility Conditions Temperature, Pressure
Cleaning Logs Daily, Monthly
Environmental Sampling Surface Sampling
Equipment Maintenance Calibration,
Depyrogenation
Compounding Record Sterility Results Extended BUD
Endotoxin Results

National Hospital Compliance 2015
Most compliant practice setting Home infusion 92.65% Hospital 79.9%
80% wear sterile gloves 76% on-going and annual training and competencies 28% perform sterility testing when it is required 68% daily air pressure/velocity documentation 57% line of demarcation 48% initial gloved fingertip sampling 39% on-going gloved fingertip sampling

National Hospital Compliance 2015
57% initial and on-going media fill testing 62% remedial action when action levels triggered 58% Quality Assurance program specific to CSPs 63% training and competencies in cleaning 37% written hazardous drug confirmation of risk 72% all elements of environmental sampling 31% report using 0.22 micron filter to sterilize
solution (high risk) 10% report performing high risk compounding
National Hospital Compliance 2015
Link to survey results: http://www.pppmag.com/article/1775

Points of Clarification
Facility Controls Facility Design ISO Certification – Non-viable air sampling Viable Air Sampling Surface Sampling
Documentation Record Retention Stability References Sterility Testing Compound Record
Personnel Metrics Supervision

Current Areas of Concern Proposed Clarifications(USP 797 proposed revision published 9/2015)
Lack of ante room or ante room not properly used
Incomplete segregation of compounding rooms
Wood/laminate shelving, doors and accessories
[ENVIRONMENTAL QUALITY AND CONTROL: Facility Design and Environmental Controls]
Creates 2 categories of compounding dependent on room design Segregated area, restricted
BUD Distinct rooms, longer BUD
[4. BUILDINGS AND FACILITIES: 4.2 Facility Design and Environmental Controls]
Facility Design

Current Concern: Hazardous Drugs
Proposed Clarification: USP 800 – Hazardous Drugs
Lack of negative pressure compounding room
[HAZARDOUS DRUGS AS CSPs]
Hazardous compounding must be done under negative pressure
[Chapter 800 – HAZARDOUS DRUGS - HANDLING IN HEALTHCARE SETTINGS: 5.3 Compounding]
Facility Design
Current Areas of ConcernProposed Clarifications(USP 797 proposed revision published 9/2015)
ISO Classified Areas: Certification performed every 6 months and when PECs relocated or rooms altered ISO Classification below
standard ACPH below standard Required pressure
differential not met[ENVIRONMENTAL QUALITY AND
CONTROL]
PEC not at ISO 5 cannot be used for compounding
Ante/buffer rooms not at appropriate ISO level, BUD is limited to Category 1 CSP (12 hr room/24 hr refrigerated)
[5. ENVIRONMENTAL MONITORING: 5.2 Monitoring Air Quality for Nonviable Airborne Particles: DATA EVALUATION AND ACTION LEVELS]
ISO Certification – Nonviable Air Sampling
Current Areas of ConcernProposed Clarifications(USP 797 proposed revision published 9/2015)
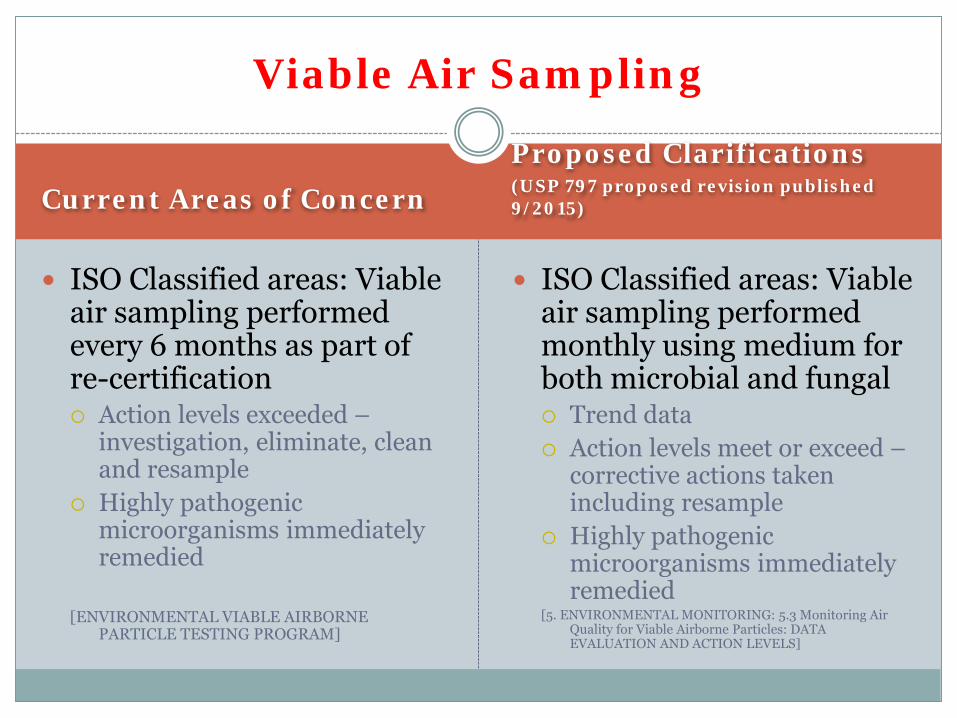
ISO Classified areas: Viable air sampling performed every 6 months as part of re-certification Action levels exceeded –
investigation, eliminate, clean and resample
Highly pathogenic microorganisms immediately remedied
[ENVIRONMENTAL VIABLE AIRBORNE PARTICLE TESTING PROGRAM]
ISO Classified areas: Viable air sampling performed monthly using medium for both microbial and fungal Trend data Action levels meet or exceed –
corrective actions taken including resample
Highly pathogenic microorganisms immediately remedied
[5. ENVIRONMENTAL MONITORING: 5.3 Monitoring Air Quality for Viable Airborne Particles: DATA EVALUATION AND ACTION LEVELS]
Viable Air Sampling
Current Areas of ConcernProposed Clarifications(USP 797 proposed revision published 9/2015)
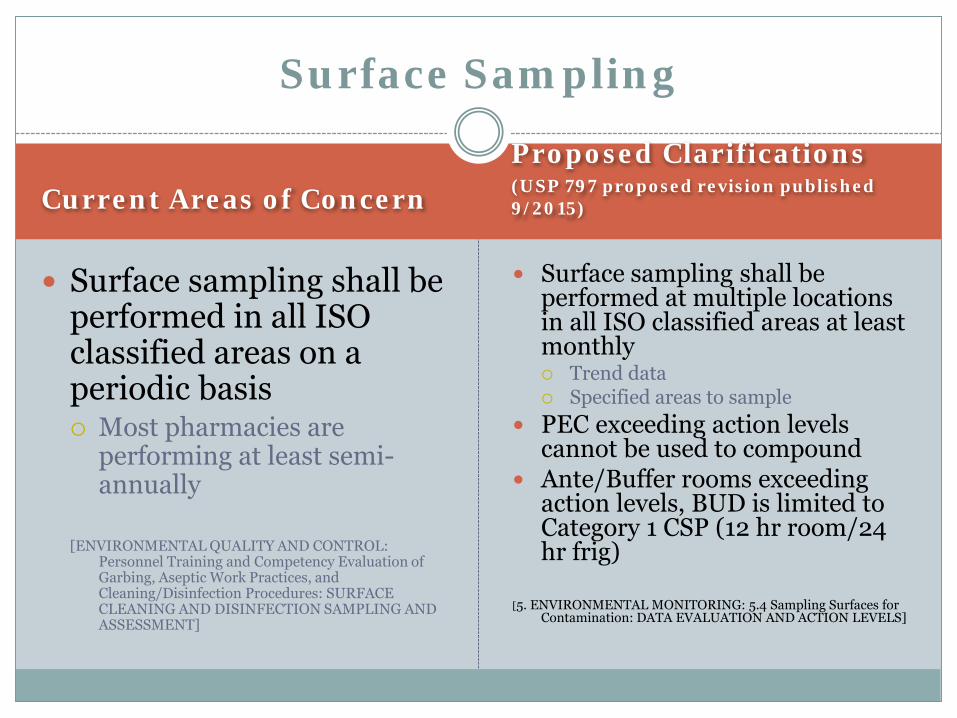
Surface sampling shall be performed in all ISO classified areas on a periodic basis Most pharmacies are
performing at least semi-annually
[ENVIRONMENTAL QUALITY AND CONTROL: Personnel Training and Competency Evaluation of Garbing, Aseptic Work Practices, and Cleaning/Disinfection Procedures: SURFACE CLEANING AND DISINFECTION SAMPLING AND ASSESSMENT]
Surface sampling shall be performed at multiple locations in all ISO classified areas at least monthly Trend data Specified areas to sample
PEC exceeding action levels cannot be used to compound
Ante/Buffer rooms exceeding action levels, BUD is limited to Category 1 CSP (12 hr room/24 hr frig)
[5. ENVIRONMENTAL MONITORING: 5.4 Sampling Surfaces for Contamination: DATA EVALUATION AND ACTION LEVELS]
Surface Sampling

Proposed Clarifications(USP 797 proposed revision published 9/2015)
Retained for as long as compounded personnel employed
Silent on how long to retain if personnel no longer employed
Maintained to provided a permanent record and long-term assessment of competency
At least 3 years or as required by state laws
[2.2. Competency Testing in Garbing and Hand Hygiene, 2.3 Competency Testing in Aseptic Technique and 16. DOCUMENTATION]
Record Retention: Personnel Training
Current USP 797

Current USP 797Proposed Clarifications(USP 797 proposed revision published 9/2015)
Silent on: Cleaning Equipment Maintenance Temperature Pressure Room/Hood Certifications Environmental Sampling Compounding Records
Batch and Compounding Records
Sterility and Endotoxintesting
Facility Design and initial qualifications – for as long as facility operational
All other records – at least 3 years or as required by state law[16. DOCUMENTATION]
Kentucky typically 5 years on record retention when addressed
Record Retention – Other Issues

Current Areas of ConcernProposed Clarification(USP 797 proposed revision published 9/2015)
BUD based on chemical and physical stability and sterility: seeing 180 days on high risk preparations
Stability data obtained from: Manufacturer Published literature Stability indicating tests Formulas from API
distributor (PCCA, Medisca)
BUD is capped Stability of all
components and devices must be considered when assigning BUD
[12. ESTABLISHING BEYOND-USE DATES AND IN-USE TIMES: 12.2 Critical Parameters to Be Considered in Establishing a BUD and 12.3 Establishing a BUD for a CSP]
CSP Stability

Current USP 797Proposed Clarifications(USP 797 proposed revision published 9/2015)
Required for: All extended BUDs
regardless of risk level High risk CSPs prepared
in groups ≥25 single dose or multi-dose vials for multiple patients
High risk CSPs exposed to warm temperature for extended period of time
[FINISHED PREPARATION RELEASE CHECKS AND TESTS: Sterility Testing]
Sterility testing of Category 2 CSPs will allow for a longer BUD
[12. ESTABLISHING BEYOND-USE DATES AND IN-
USE TIMES: 12.3 Establishing a BUD for a CSP]
Sterility Testing

Current USP 797Proposed Clarification(USP 797 proposed revision published 9/2015)
Shall meet USP Chapter 71 Sterility Test or a method not described in USP may be used if verification results demonstrate that the alternative is at least as effective and reliable as USP 71 USP 71 - 14 days Rapid Scan – 3 days (non USP) Bioluminescence – 7 days (non
USP)
[FINISHED PREPARATION RELEASE CHECKS AND TESTS: Sterility Testing]
Must be performed in a manner consistent with USP 71, with the exception to batch size requirements in USP 71
[10. RELEASE TESTING: 10.2 Sterility Testing]
Sterility Test
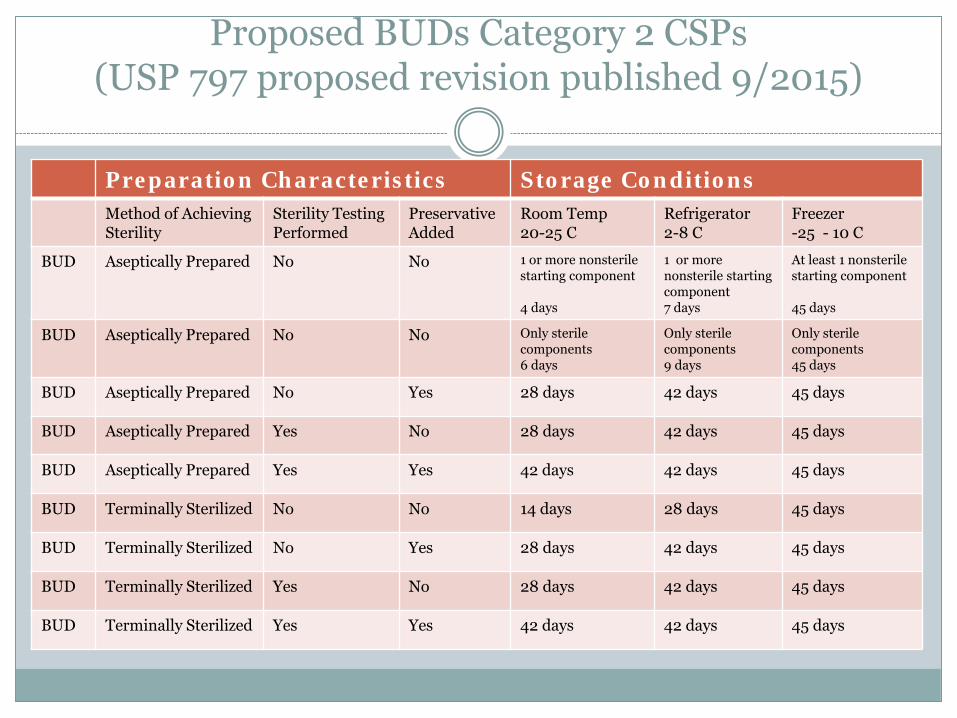
Proposed BUDs Category 2 CSPs(USP 797 proposed revision published 9/2015)
Preparation Characteristics Storage ConditionsMethod of Achieving Sterility
Sterility Testing Performed
PreservativeAdded
Room Temp20-25 C
Refrigerator2-8 C
Freezer-25 - 10 C
BUD Aseptically Prepared No No 1 or more nonsterilestarting component
4 days
1 or more nonsterile starting component7 days
At least 1 nonsterilestarting component
45 days
BUD Aseptically Prepared No No Only sterilecomponents 6 days
Only sterile components9 days
Only sterilecomponents45 days
BUD Aseptically Prepared No Yes 28 days 42 days 45 days
BUD Aseptically Prepared Yes No 28 days 42 days 45 days
BUD Aseptically Prepared Yes Yes 42 days 42 days 45 days
BUD Terminally Sterilized No No 14 days 28 days 45 days
BUD Terminally Sterilized No Yes 28 days 42 days 45 days
BUD Terminally Sterilized Yes No 28 days 42 days 45 days
BUD Terminally Sterilized Yes Yes 42 days 42 days 45 days

Current USP 797Proposed Clarification(USP 797 proposed revision published 9/2015)
Referenced multiple times but not defined
Current practice: Infusion and Community –
have compound record Hospital
Batch Records Certain preparations (TPN,
Chemotherapy)[FINISHED PREPARATION RELEASE
CHECKS AND TESTS: Inspection of Solution Dosage Forms and Review of Compounding Procedures]
Master Formula for CSPs batched or prepared from nonsterile ingredients
Compound Record required for every CSP prepared
[9. SOPs AND MASTER FORMULATION AND COMPOUNDING RECORDS]
Compounding Record

Proposed Master Formulation Record Requirements(USP 797 proposed revision published 9/2015)
Name, strength, and dosage form of the CSP Physical description of the final preparation Identities and amounts of all ingredients and appropriate container-
closure systems Complete instructions for preparing the CSP, including equipment,
supplies, and a description of the compounding steps BUD and storage requirements Quality control procedures (e.g., pH, filter integrity, and visual
inspection) Sterilization method, if applicable (e.g., filter, steam or dry heat) Any other information needed to describe the operation and ensure
its repeatability (e.g., adjusting pH and tonicity and temperature)
[9. SOPs AND MASTER FORMULATION AND COMPOUNDING RECORDS: 9.2 Creating Mater Formulation Records]
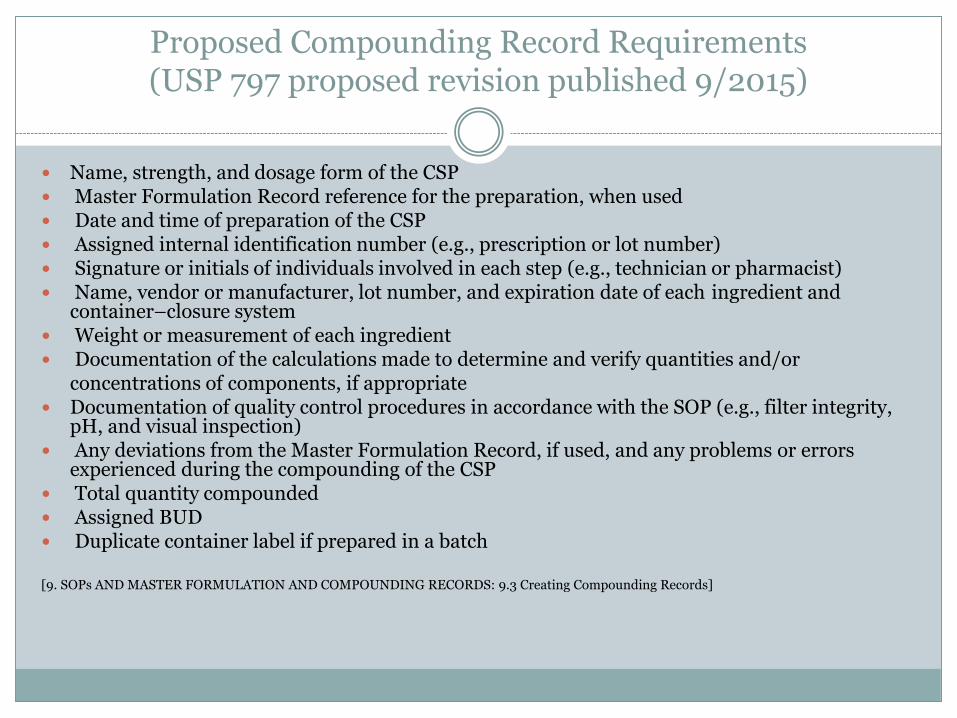
Proposed Compounding Record Requirements(USP 797 proposed revision published 9/2015)
Name, strength, and dosage form of the CSP Master Formulation Record reference for the preparation, when used Date and time of preparation of the CSP Assigned internal identification number (e.g., prescription or lot number) Signature or initials of individuals involved in each step (e.g., technician or pharmacist) Name, vendor or manufacturer, lot number, and expiration date of each ingredient and
container–closure system Weight or measurement of each ingredient Documentation of the calculations made to determine and verify quantities and/or
concentrations of components, if appropriate Documentation of quality control procedures in accordance with the SOP (e.g., filter integrity,
pH, and visual inspection) Any deviations from the Master Formulation Record, if used, and any problems or errors
experienced during the compounding of the CSP Total quantity compounded Assigned BUD Duplicate container label if prepared in a batch
[9. SOPs AND MASTER FORMULATION AND COMPOUNDING RECORDS: 9.3 Creating Compounding Records]
Current ChapterProposed Revision(USP 797 proposed revision published 9/2015)
Pharmacy Bulk Package –bear a statement limiting the time frame in which the container may be used once it has been entered
Single-Dose Container – no preservative; vials exposed to ISO Class 5 air may be used up to 6 hours after initial needle puncture
[DEFINITIONS and SINGLE-DOSE AND MULTIPLE-DOSE CONTAINERS]
In-Use Time – the time before which a conventionally manufacturer product or a CSP must be used after it has been opened or needle punctured (e.g., after a container closure of a vial has been penetrated)
Compounded stock solution – in-use time is 6 hours
[12.4 Establishing In-Use Times]
Stock Solution/Pharmacy Bulk Package
Supervision
KRS 315.020(1) No owner of a pharmacy who is not a pharmacist shall fail to place a pharmacist in charge of his pharmacy or shall permit any person to compound or dispense prescriptions, drugs, medicines, or pharmaceuticals, in his place of business except in the presence and under the immediate supervision of a pharmacist
KRS 315.010(11) “Immediate Supervision” means under the physical and visual supervision of a pharmacist
KRS 315.010(25) “Supervision” means the presence of a pharmacist on the premises to which a pharmacy permit is issued, who is responsible, in whole or in part, for the professional activities occurring in the pharmacy
Supervision
Proposed revision: Supervisors of compounding personnel should observe compounding activities on a daily basis [2. PERSONNEL QUALIFICATIONS – TRAINING, EVALUATION AND REQUALFICATION]
Training of compounding personnel Some facilities have technicians training compounding
personnel Some facilities do not have any training on pharmacists
Will perform compounding Will check/supervise compounding

Future Meetings
Communication with sterile compounders Updates to Board Further areas requiring clarification Nuclear pharmacies Regulation update Require continuing education Report cards Out of state permits Non-sterile compounding USP 795

Requested Guidance
Cessation of compounding Retesting of room Compound record







